All published articles of this journal are available on ScienceDirect.

Doctoral Theses as a Source of Knowledge Production for IPV Prevention: A Literature Review of Doctoral Theses at a Swedish University
Abstract
Background:
Intimate Partner Violence (IPV) is a pervasive form of Violence Against Women (VAW). IPV has been acknowledged as a human rights violation and a public health problem. Years of research and advocacy have led to a better understanding of the problem including the development of the ecological model for explaining IPV. Although diverse international policies and global advances in women’s rights have contributed to addressing IPV, the problem still persists. IPV is associated with adverse health outcomes, therefore, its prevention is an important aspect of population health promotion.
Objective:
Considering that doctoral research and theses form an integral aspect of knowledge production, the present study aims to provide a review of doctoral theses on IPV at a Swedish university in order to identify areas of unmet need for future IPV prevention studies.
Methods:
A search was conducted to identify IPV related thesis stored in the Karolinska Institutet (KI), which is a database where all publications produced at KI are stored. A total of thirteen PhD theses (the earliest published in 2004 and the latest in 2017) met the inclusion criteria and were reviewed.
Results:
Through their wide range of contexts and contents, these theses provide a global insight into IPV. Findings show that prevalence estimates and risk factors at the individual and relationship levels are well researched. Potential areas of unmet needs include the under-researched nature of risk factors and interventions at the community and societal level as well as underlying issues preventing the healthcare sector from actively playing its role in addressing IPV.
Conclusion:
Capacity building for the health sector and addressing community and societal level risk factors of IPV are modifiable factors to address IPV and improve population health.
1. INTRODUCTION
There is an increasing global effort to address Intimate Partner Violence (IPV) which is one of the most pervasive forms of Violence Against Women (VAW). IPV is described as any behaviour (including controlling behaviours), within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship [1, 2]. The global life-time prevalence of IPV among ever partnered women is about 30% [3]. IPV is associated with adverse health outcomes such as injury, physical and mental health problems and a range of diseases [4]. Research and advocacy through the years have contributed to knowledge production [5]. Diverse international declarations and policies continue to contribute to advances in women’s rights globally [6-10], yet the problem persists. Currently, elimination of all forms of VAW including IPV is part of the Sustainable Development Goals, SDGs [11] and is considered central to achieving the SDGs [10].
Understanding the determinants of IPV is the bedrock of prevention. The ecological model for explaining IPV presents factors associated with IPV at four distinct levels, i.e. individual, relationship, community and societal levels [12-14]. The ecological model provides an important framework for understanding interactions between different factors that can result in IPV as well as specific points in the model at which prevention strategies can be introduced. While primary prevention focuses on measures to stop the prevalence of IPV [15], the focus of secondary and tertiary prevention is to identify cases and manage the health outcomes of IPV, respectively. Continuous knowledge production to identify determinants in different population groups is thus an essential aspect of prevention.
Doctoral (PhD) research constitutes an important source of knowledge production in every discipline [16, 17]. Doctoral theses are often executed within knowledge environments characterised by creativity, application and flexibility [16, 17]. They are designed to be original and closely aligned with current global needs [18]. The elimination of all forms of VAW including IPV and generation of evidence have been major global goals in recent times [13, 15]. While acknowledging the importance of scientific utility for a doctoral thesis, Lafont (2014) highlights the importance of social utility of doctoral theses to account for societal issues and aid decision-makers [19].
This paper is intended to provide a review of IPV related thesis at a Swedish university and to ïdentify likely areas of unmet need for IPV intervention.
1.1. Context
Karolinska Institutet (KI), is a leading medical university [20]. Research at the department of public health sciences focuses on identifying public health problems and designing population-level interventions [21]. PhD theses at the department provide a global perspective since almost two-thirds of them are based on non-Swedish populations [21].
2. MATERIALS AND METHODS
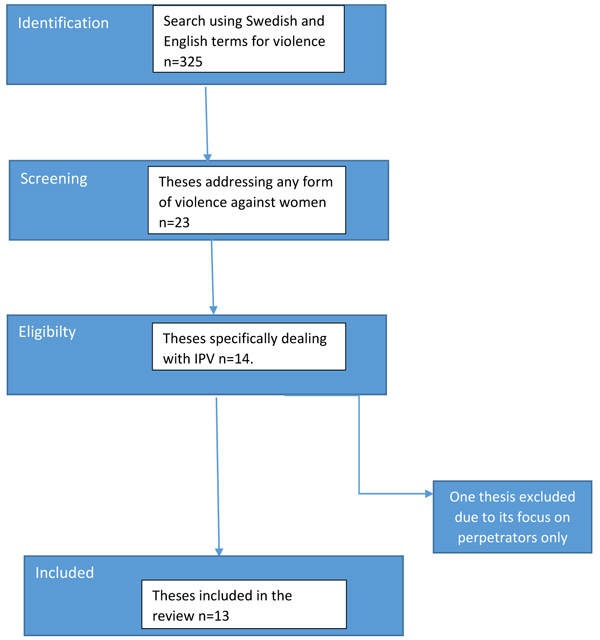
KI has had an open access policy since 2011, and therefore, maintains a database known as the KI open archive. The foregoing is an electronic archive where all publications produced at KI are stored. The thesis section of the database was searched between April and May 2018; the search was not limited by the publication year. A singular search term ”Violence” was first applied and resulted in 325 hits. It is important to note that theses written in Swedish also had an abstract in the English Language. The 325 hits were then individually examined to identify those dealing with VAW. This screening further resulted in a total of 23 theses. In the final step, IPV was used as the inclusion criteria yielding a total of 14 PhD theses. Only thirteen theses were included in the current study due to the exclusion of one thesis which focused on only perpetrators (Fig. 1).
3. RESULTS
A total of thirteen theses met the set inclusion criteria, the earliest was published in 2004 and the latest published in 2017. The theses covered twenty-four different countries, a majority of them were low and middle-income countries (Table 1). The theses explored prevalence estimates and determinants (including IPV in pregnancy), diverse health-related outcomes, attitudes, disclosure and help-seeking behaviour (Table 2). Only two theses in total had intervention components i.e. one with the intervention to improve screening skills among nurses [22], and another which conducted a mapping of possible aspects to include in a planned intervention [23]. Findings of this review are presented in two broad categories i.e. background information in the theses and the result findings.
| References | Reference list Number | Study Context | Data Source | Sample Characteristics | Key Findings | |
|---|---|---|---|---|---|---|
| 1. | Caman, S (2017) | 32 | Sweden | European Homicide Monitor National homicide dataset Forensic Homicide Database |
All solved homicides (N = 1,725) in Sweden between 1990 and 2013. All male-perpetrated homicides (N = 211) in Sweden between 2007 and 2009 All female-perpetrated (n = 9) and stratified male-perpetrated (n = 36) between 2007 and 2009 |
-Decline in male-perpetrated Intimate Partner Homicides (IPH), compared to female-perpetrated IPH -Female-perpetrators likely unemployed, has history of substance use and been victimized by the male victim -Male IPH perpetrators are older, employed, less likely previously convicted and have less persistent criminal histories -Perpetrators of IPH likely to commit suicide |
| 2. | Dufort, M (2015) | 33 | Sweden | Swedish National Public Health Survey, 2004 to 2009, Three separate cohorts of women exposed to IPV: help seekers recruited from women’s shelters and social services; non-help seekers |
Men and women aged 16-84 (2005-2007) and 18-84 years (2004). (n=50,350). |
-Prevalence of physical IPV 0.7% women; 0.4% men -Risk factors were being foreign born, lack of social support, psychological distress and hazardous drinking and financial problems -Increased risk of suicidal thoughts and attempts among male victims -Increased psychological and psychosocial impairments among women seeking help for IPV -Help seeking women were younger, had lower education, still in a relationship with and had children together with the perpetrator. |
| 3. | Sundborg, E (2015) | 22 | Sweden | Nurses and district nurses | Nurses and district nurses working at health centers in two different counties. Nurses and district nurses n=192 11 district nurses for interview District nurses n=304 |
-Nurses lack knowledge and preparedness IPV response -Many had preconceived notions about victims -Nurses screen depending on interest -Nurses commonly referred abused women to doctors. -Intervention to improve IPV response showed positive potentials |
| 4. | Zacarias, A (2012) | 26 | Mozambique | Women visiting Forensic Services | 1442 women aged 15-49 years-old | -Past year prevalence of IPV was 70% -Risk factors were middle/high educational, divorce/separation, children at home, controlling behaviors, being a perpetrator; childhood abuse -About 69% of the women were IPV perpetrators -Mental health symptoms |
| 5. | Okenwa, L (2011) | 24 | Nigeria | women visiting a healthcare facility 2008 Nigeria DHS |
934 Women 15-49 years old 33,385 women and 15,486 men |
-Past year prevalence of IPV 23% psychological, 9% physical and 8% sexual -Risk factors were lack of access to information, women’s autonomy in decision making and contribution to household expenses -54% not willing to disclose IPV -Disclose mostly to only friends, relatives or religious leaders -Only 1% willing to disclose to police - IPV significantly associated with using modern forms of contraception; miscarriages, induced abortions, stillbirths and having many children. -More women than men justified IPV -Access to radio/tv was associated with increased justification of abuse. |
| 6. | Uthman, O (2011) | 35 | Benin, Burkina Faso, Ethiopia, Ghana, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mozambique, Namibia, Nigeria, Rwanda, Swaziland, Tanzania, Uganda, Zimbabwe. | DHS data from 17 subsaharan African countries between 2003-2007 | Women 15-49 years old 165,983 women; 68,501 men |
-More women than men justify IPV -Gender disparity in attitudes - Education, access to information and joint decision making were associated with decreased tolerance of IPV -Neighbourhood and contextual factors influenced levels of IPV tolerance -Risk factors for justifying IPV were living in disadvantaged communities, husband having higher education and polygamy -Tolerant attitudes to and witnessing IPV was significantly associated with disclosing IPV. |
| 7. | Ali, TS (2011) | 29 | Pakistan, health outcomes | Household surveys of 759 living in two different towns Five FGDs with women with diverse sociodemographic background |
Married women aged 25–60 years | -Life time IPV prevalence 57.6% -Past year prevalence 56.3% -Risk factors low education, illiteracy, large family size -Tolerant attitudes to protect family honor - Suicidal thoughts and feelings of worthlessness common among victims. |
| 8. | John, IA (2010) | 30 | Nigeria | Healthcare providers (HCP) and women visiting a teaching hospital in northern Nigeria | Healthcare providers (HCP) comprising of nurses, midwives, doctors and social workers 507 Women visiting the healthcare facility |
-74% Healthcare providers (HCP) did not inquire about IPV -HCP scored low on readiness to screen -Social workers had higher efficacy and network to screen and refer. |
| 9. | Hamzeh, B (2009) | 23 | Iran | Potential victims and perpetrators; stakeholders | 435 Women, 447 Men; 23 key informants from healthcare, religious, judicial etc. sectors 9 males and 13 women attending mandatory premarital education center, 4 female gate keepers, i.e. facilitators at center; |
-Causes of IPV identified by men and women were partner’s addiction, mental disorder, unemployment, unsuitable clothes etc. -Victim blaming among key informants -Participants suggest familiarity with women’s rights according to Islamic laws as solution -Observed gender differences in participants suggestions for interventions. |
| 10. | Dalal, K (2008) | 31 | India | Multi source | married women between aged 14-49yr 719 boys; 681 girls in India 4411 Household surveys in two sub-districts in rural Bangladesh 14016 women from 2005 DHS Egypt 5878 women from Kenyan DHS 2003 |
-Mothers’ exposure and IPV tolerance were determinants of child abuse -Religion, illiteracy, suspected husband’s infidelilty, large age difference between partners, dowry are risk factors for IPV -In Bangladesh 41% physical abuse; 5% sustenance abuse -In Kenya 11% emotional, 11% sexual and 25% physical IPV. -The economic burden of violence arising from injury, death, deprivation and others are enormous especially on families. |
| 11. | Vung N (2008) | 28 | Vietnam | 5 FGDs Household surveys |
883 married/partnered women aged 17-60 years | -30.9% lifetime and 8.3% past year IPV -Psychological IPV most prevalent; 33% past year and 54.4% lifetime -Risk factors, low education, polygamy, women witnessing IPV between parents, low household income, low occupational status. -Health consequences were depression, chronic pains and suicidal thoughts. |
| 12. | Kaye, D (2006) | 25 | Uganda | Women visiting antenatal and post natal clinics | - 379 women attending antenatal clinic -16 in depth interviews with pregnant adolescents -Case control study of 942 women seeking post-abortion care -Prospective cohort of women with low birth weight babies and antepartum hospitalisation |
-57% moderate to severe IPV associated with being adolescent, abuse in childhood and first pregnancy. -Risk factors are bride price, modernisation, urban migration, men’s unemployment, misconceptions about pregnancy changes, household division of labour, negotiating for sex. -Women seeking induced abortion were 18 times likely to be experiencing IPV. -19% of low birth weight and 74% antepartum hospitalisations were attributable to IPV. |
| 13. | Rubertsson, C (2004) | 34 | Sweden | National cohort of 4600 Swedish-speaking women | women in antenatal and postnatal care | - IPV prevalence first post partum year was 2% i.e. 52 women -Only 3 women reported to police. -IPV determinants were age 24 years or younger, country of birth outside Europe, having a partner born outside Europe, being single and being unemployed. |
3.1. Background Information
3.1.1. Definitions and Typologies of IPV
Various definitions were adopted by authors, some definitions almost exhaustively describe what constitutes IPV and who the potential victims are, examples included definitions by the World Health Organisation, WHO and Center for Disease Control, CDC [24-26]. The Center for Disease Control (CDC), defines IPV as any ”physical, sexual, or psychological harm by a current or former partner or a spouse. This type of violence can occur among heterosexual or same-sex couples and does not require sexual intimacy. IPV can vary in frequency and severity. It occurs on a continuum, ranging from one hit that may or may not impact the victim to chronic, severe battering” [27]. Various terms were used to describe IPV e.g. domestic violence, men’s violence against women and sometimes VAW. Some authors [22, 28] discussed this tendency to use terms interchangeably and made attempts to clarify each term. The United Nations’ (UN) definition of VAW was commonly referred [22-24, 28].
3.1.2. International Documents Cited
Global health policies and strategies are instrumental in shaping health promotion strategies at national and local level. Some authors [22, 28-30] approached IPV from human and women’s rights perspectives. More commonly cited were UN’s convention on the elimination of all discrimination and violence against women (CEDAW) and UN’s 1993 Declaration on the Elimination of Violence against Women.
| Variables | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Prevalence and Determinants | Associated Consequences | Attitudes | Disclosure/ Help-seeking |
Health Care Response | Women’s Perpetration | Economic Burden | IPV in Pregnancy or First Post Partum Year | |||
| Mental Health | Reproduc- tive Health |
Homicide | Others | ||||||||
| Caman, S (2017) | x | ||||||||||
| Dufort, M (2015) | x | x | |||||||||
| Sundborg, E (2015) | x | ||||||||||
| Zacarias, A (2012) | x | x | x | ||||||||
| Okenwa, L (2011) | x | x | x | x | |||||||
| Uthman, O (2011) | x | x | |||||||||
| Ali, T (2011) | x | x | x | x | |||||||
| John, I (2010) | x | ||||||||||
| Hamzeh, B (2009) | x | x | |||||||||
| Dalal, K (2008) | x | x | |||||||||
| Vung N (2008) | x | x | x | ||||||||
| Kaye, D (2006) | x | x | x | ||||||||
| Rubertsson, C (2004) | x | x | x | x | x | ||||||
3.1.3. Theses Methodologies
3.1.3.1. Design, Study Context, Setting and Participants
A total of five theses [22, 23, 25, 28, 29] used mixed methods incorporating qualitative (i.e. deep interviews and focus group discussions, FGD) and quantitative approaches. About six theses [24, 26, 30-34] were quantitative of mainly cross-sectional design; Kaye (2006) combined cross-sectional, case control, and prospective cohort [25]. Quantitative data source was either through a larger research project [34], active data collection [22, 23, 25, 26, 28-30, 33], registers [32, 35] or a combination of active data collection and registers/database (24, 28, 31, 33). Three Swedish registers were used i.e. National Public Health Survey conducted between 2004 and 2009 [33], national homicide dataset and the Forensic Homicide Database [32]. Demographic and Health Surveys (DHS) is an international database for monitoring demographic and health situations in developing countries, DHS was used by three authors [24, 31, 35]. The populations included in the theses are presented in Table 1. Some studies were conducted in clinical settings [22, 24-26, 30], others were household surveys or a combination of both (Table 1). Many of the theses based on DHS data focused on women of reproductive age (i.e. 15-49 years) while others chose a wider age range i.e. 16 – 84 years [33].
3.1.3.2. Instruments Used in the Quantitative Studies
Operationalisation of IPV was majorly based on the Conflict Tactic Scales (CTS and CTS2) [36, 37] which are well established self-report measure of IPV [36, 38]. Some theses authors adapted and used the WHO questionnaires for some or all aspects of their studies [24, 28, 29]. CTS was used to measure chronicity and severity of IPV [25, 26]. Other IPV related instruments used were Controlling Behaviors Scale-Revised (CBS-R) [26, 39, 40]; attitudes towards IPV [24, 28, 35]; Decision Making In Abuse Relationships Interview, DIARI [33]; Domestic Violence Healthcare Provider Survey scales and Violence against Women Health Care Provider Survey [22, 30].
3.2. Theses Findings
3.2.1. Prevalence and Determinants of IPV
Lifetime prevalence ranged from 30.9% to 57.6% (29, 30), past year prevalence was between 8.3% in Vietnam to 56.3% in Pakistan [24, 25, 28, 29, 31]. Psychological IPV appeared to be the most common of IPV. In one study, 69% of the women reported having perpetrated IPV in the past year [26]. Women’s use of controlling behaviors over partners predisposed them to psychological and sexual IPV [26], while partners’ use of controlling behaviors was positively associated with physical IPV and injury but negatively associated with psychological IPV [26].
Determinants of IPV include woman’s or partner’s low education, illiteracy [28, 29, 31]; large family size [29]; being foreign-born, lack of social support, psychological distress, hazardous drinking and financial problems [33], having children [24, 26], controlling behaviors, being a perpetrator and history of abuse in childhood [26], low education, polygamy, having witnessed IPV between parents, low household income, low occupational status [28, 31] etc. Others include religion, suspected husband’s infidelity, dowry issues, alcohol problems [31], large age difference between partners, polygamy [31], lack of access to information, women’s lack of autonomy in decision making, [24, 31], and being in the age group 15-24yrs [24].
Whereas financial problems such as difficulty managing monthly expenditure and contribution to household expenses were risk factors in studies in Nigeria and Sweden, financial strain was a protective factor for IPV in Mozambique [24, 26, 33]. In Kenya, high educational level was a protective factor for IPV, however high educational level combined with being employed and high occupational status were risk factors for IPV. Risk factors for IPV in pregnancy were adolescent pregnancy, abuse in childhood and first pregnancy. The study from Iran [23] showed gender differences regarding what men and women considered causes and triggers of IPV. While 90% of women ranked the three top causes of IPV as partner’s addiction, mental disorder, husband’s unemployment, 70-75% men ranked it as not obeying husband, unpleasant comment in the presence of other people and wearing unsuitable clothes.
3.3. Associated Consequences of IPV
IPV was significantly associated with adverse reproductive health outcomes such as miscarriages, stillbirths, having many children and increased used of modern forms of contraception [24], induced abortions [24, 25], depressive mood during pregnancy [34], antepartum hospitalisations [25], suicide, suicidal thoughts and homicide [28, 29, 33]. One study showed that female perpetrated intimate partner homicides are few and have remained relatively unchanged during the period studied [32]. Female perpetrators of intimate partner homicide are likely to have a history of substance abuse or prior victimization by the male victim [32]. Mental health outcomes include depression and worthlessness even in cases where women were perpetrators [26, 28, 29]. Other outcomes associated with IPV were chronic pains [28] and economic burden especially on families due to injury, death, deprivation etc. [31].
3.4. Attitudes, Disclosure and Help-Seeking
3.4.1. Attitudes
More women than men justified IPV [24, 35]; the determinants of justifying IPV include living in disadvantaged communities, husbands having higher education, polygamy, lack of autonomy in decision making and being young [24, 35]. Living in urban areas, certain ethnicity and a rich wealth index were factors associated with the non-justification of IPV [24]. The likelihood of justifying abuse was lower among women with frequent access to newspapers compared to access to radio and television [24]. Protection of family honour was central to why women tolerated IPV, however, having an educated extended family and being younger reduced tolerant attitudes [29]. This finding is in contrast to one of the studies from Nigeria where tolerant attitudes to IPV were more among younger woman [24]. In Vietnam, witnessing IPV during childhood was associated with justifying IPV [28]
3.4.2. Disclosure and Help-seeking
Five studies [24, 29, 33-35] examined disclosure and help-seeking. About 54% of women were not willing to disclose abuse, only 1% of those willing to disclose will report to the police while the majority preferred to disclose to friends, relatives or religious leaders [24]. Ali (2011), approached disclosure as a coping strategy and found that only 177 of the 646 women subjected to IPV actually disclosed abuse [29]. A majority disclosed to their parents, friends and in-laws, however, only 1.5% sought formal help e.g. from healthcare services, judiciary or religious leaders [29]. Whereas one thesis [35] found that tolerant attitudes to IPV were significantly associated with disclosing IPV, another study [24] found that women with tolerant attitudes did not differ from those with non-tolerant attitudes in their willingness to disclose.
In one study from Sweden, only about 5% of women exposed to IPV after childbirth reported to the police [34]. Compared to non-help seeking women, women who seek help for IPV were likely to be younger, less educated and still in a relationship and have children together with the perpetrator; they also had more psychological and psychosocial impairments [33].
3.5. Health Sector Response
Two theses [22, 30], examined IPV screening practices among health care providers (HCPs) and found that victim blaming [30] and preconceived notions about victims were common [22]. HCPs (comprising doctors, midwives, nurses and social workers) scored low on readiness to screen [30]. Social workers had higher self-efficacy and a network to screen and refer victims of IPV. Other factors associated with increased likelihood of screening for IPV were being male, victim blaming and increased self-efficacy. Screening for IPV was associated with women’s satisfaction with nursing care. Sundborg’s thesis [22] investigated Swedish nurses knowledge and readiness to inquire about IPV. Nurses lacked knowledge and skills for IPV screening, nurses who inquired about IPV had most likely acquired knowledge on their own. Furthermore, nurses commonly referred abused women to doctors.
3.6. Interventions
One thesis from Iran [23] found that a majority of the participants believed that education based prevention is a good approach. Suggestions of important components of such education include improving knowledge of women’s rights according to Islamic laws, knowledge about women’s rights, sexual education, consequences of VAW and coping strategies with legal action as the last alternative. Participants’ suggestions for intervention revealed gender differences. Another thesis [22] developed an education-based intervention to equip nursing staff with the necessary knowledge and readiness for identifying victims of violence and offer them adequate care. Post-test after one year showed significant improvements in knowledge and readiness to screen among participants. Part of this thesis was developing and testing a Swedish version of the Violence Against Women Health Care Provider Survey.
4. DISCUSSION
Using doctoral research theses produced at a Swedish university, this study sought to review the contribution of doctoral studies to knowledge production for IPV and IPV prevention. Another goal of this review was to identify areas of unmet need for IPV intervention studies. Only two of the theses had elements of intervention [22, 23] further confirming the current concern about the dearth of IPV intervention studies [13, 15]. The only thesis which conducted an actual intervention did so within the healthcare setting and is from Sweden, a high-income country [22]. According to the WHO (2010), the need to refine and adapt the few available evidence-based interventions emanating from high-income countries for use in low-resource settings is a challenge [13]. The existence of very little intervention studies especially from low-resource settings is an area of unmet need for IPV prevention.
The wide range of countries covered and the diverse nationally representative data materials in this review provide a range of important findings for future practice. Despite the potential problem of underreporting, the prevalence estimates, determinants and associated consequences of IPV found in these theses provide relevant information for planning interventions in different population groups. Moreover, the observation of the inverted U phenomenon (i.e. varying directions of association observed in different contexts for certain demographic and socioeconomic factors), provides a much-needed input for designing appropriate context-specific interventions. Using the widely accepted ecological model as a point of departure [12, 13], it appears that factors at the proximal end of the model (i.e. individual and relationship levels) are more well-researched than factors at the distal end (community and societal levels). This tendency probably explains why many of the evidence-based interventions and those for which evidence is emerging, are majorly based on addressing factors at the individual and relationship levels [13]. While these are crucial aspects for prevention, the need for a holistic approach which takes community and societal level factors into consideration can not be overemphasised.
A relevant example for the foregoing is the finding that tolerant attitudes to and justification of IPV are common in many patriarchal, low-income contexts as well as in disadvantaged communities [24, 29, 35]. IPV and justification of IPV are rooted in social norms which reinforce gender inequality and perpetuate IPV [6, 7, 10]. Despite evidence that tolerant attitudes are known predictors of IPV victimization and perpetration, many interventions have only targeted women through economic empowerment and equipping them with skills related to gender equality [41]. Interventions to address harmful norms and values must target the wider society in order to alter beliefs and practices which perpetuate IPV. Furthermore, the finding that women who frequently watched television were more likely to have tolerant attitudes to IPV compared to those who read newspapers frequently [24, 42], may have implications for the use of access to information as a measure of women’s empowerment in research. Indeed, concerns regarding contents that seem to promote gender inequality in African movies and television programmes have previously been raised [42, 43]. Access to tv and radio as parameters for women’s empowerment may have to be specified in terms of what content has been accessed.
While primary prevention is important for preventing the occurrence of IPV, secondary and tertiary prevention helps to identify and manage cases, disclosure is therefore important. The finding that women are more willing to disclose IPV (or the fear of it) to informal resources such as family, friends or religious leaders, than to formal sources, e.g. police, healthcare is an important one. Informal resources provide social support and collaborate effectively with formal resources (e.g. counselors, doctors, law enforcement etc.) in providing safety and help to victims. Future research may aim at providing evidence for best practices regarding how to effectively engage informal resources. Women’s willingness to disclose is the bedrock of screening practices commonly found in healthcare settings. The health care sector has long been identified as an important arena for addressing IPV. While existing guidelines and standard routines in the sector may serve as good frameworks for responding to IPV, findings from this review further confirm that they do not provide the fundamental knowledge and competence for identifying IPV and responding accordingly [22, 44]. More studies on capacity building strategies for the general public health workforce (including healthcare) will help generate evidence for IPV prevention [45].
4.1. Strengths and Weakness
The national representative data used in most of the theses, the methodological rigor of databases used (e.g. DHS) and the various methodologies employed in the studies etc., all contribute to the strength of this review. Some weaknesses are however worthy of note. Firstly is that this review is based on doctoral theses from one university in Sweden and does not cover other contexts. Secondly, some of the theses are based on populations recruited within clinical settings. Although clinical populations provide quick access to participants, it is often criticised due to the risk of overrepresentation of IPV victims.
CONCLUSION
IPV research and advocacy have come a long way, however, the dearth of IPV intervention studies is an area of unmet need. Also, unlike factors at community and societal level, many of the determinants of IPV at individual and relationship level are well research and have provided vital information for interventions. The need to address community and societal levels factors that perpetuate IPV, e.g. attitudes towards IPV, can however not be overemphasised. Addressing community and societal level factors is important in order to have a holistic approach to IPV prevention. More studies on capacity building for the public health workforce (including the healthcare sector) will contribute to generating much-needed evidence for effective response to IPV. Doctoral theses research provide vast opportunities for knowledge production in addressing IPV and VAW in general.
AUTHORS' CONTRIBUTIONS
Dr. Emegwa-Okenwa Leah, PhD is the only author of this manuscript
SIGNIFICANCE FOR PUBLIC HEALTH
The findings from this review raise awareness for the need for more intervention studies on intimate partner violence in order to generate more evidence. Capacity building for public health workforce and addressing community and societal level determinants of IPV are discussed here as modifiable factors to address IPV and improve population health.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
PRISMA guidelines and methodology were followed.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author wishes to thank Professor Bjarne Jansson, Department of Public Health Sciences, Karolinska Institutet, for the invitation to do this overview.

