All published articles of this journal are available on ScienceDirect.

Assessment of Orthodontic Treatment Need in Kosovar Children
Abstract
Background:
To date, no survey was done in Kosovo for the identification of orthodontic treatment needs. The aim of this study is to assess the prevalence of orthodontic treatment need among Kosovar children of ages 11-13, using the DAI and the DHC-IOTN in the identification of orthodontic treatment need.
Methods:
A sample of 185 children (50.3% female, 49.7% male), aged between 11-13, was randomly selected from one elementary school in Prishtina. Orthodontic treatment need was measured using the Dental Aesthetic Index (DAI) and the dental health component of the Index of Orthodontic Treatment Need (DHC-IOTN).
Results:
Based on DAI, treatment was found as elective in 11.9 percent of the children. Treatment was found as highly desirable and mandatory in 5.9 percent and 4.3 percent of children, respectively. No gender-based significant differences were noted. According to IOTN DHC: 16.2 percent of children had borderline treatment need, while 66.5 percent had severe and extreme treatment need (grades 4 and 5). Again, no significant gender-based differences in the treatment need were found.
Conclusion:
High prevalence of orthodontic treatment need was identified in Kosovar children of ages 11-13, while no gender-based statistically significant differences were noted in the need for orthodontic treatment.
1. INTRODUCTION
Several studies show that there is an increase in the prevalence of orthodontic anomalies, leading to an increase in the need for orthodontic treatment [1-11]. Most of the orthodontic patients are children and adolescents and information on the orthodontic treatment prevalence among this category allows national budget planning in the most convenient way. Orthodontic anomalies besides functional limitation cause psychological effect too [12], thus emphasizing its importance of treatment. Information about the prevalence of malocclusion and early detection of malocclusion, as a result, early orthodontic treatment allows better national funds allocations.
Kosovo as a new state has no data about the prevalence of malocclusion or orthodontic treatment need, thus research articles on the epidemiology of malocclusion offer information on oral health anomalies among specific age population.
The need for orthodontic treatment is established using standardized indices, based on which the dental anomalies can be categorized. The index for assessing the orthodontic treatment priority was developed by Brook and Shaw and was later modified by Richmond [1, 13]. Today, this index is accepted as a standardized, valid, and reproducible index for the objective assessment of treatment need. The Index of Orthodontic Treatment Need (IOTN) has two components: Dental Health Component (DHC) and Aesthetic Concern (AC). The latter has 10 subcategories and is used only when the patient is assessed in DHC group 3.
DHC-IOTN has 5 categories, ranging from 1 (no need for treatment) to 5 (great need) and malocclusion is assessed based on the following characteristics: tooth loss, overjet, crossbite, displacement of the contact point, and overbite [13].
The dental aesthetic index (DAI) evaluates 10 occlusal characteristics: the number of missing teeth, overjet, negative overjet, diastema, anterior open bite, anterior crowding, anterior spacing, anterior irregularities (mandible and maxilla), and antero-posterior molar relationship [2]. DAI has four stages of malocclusion severity: a score lower than or equal to 25 (no or slight treatment need), a score between 26 and 30 (elective treatment need), a score between 31 and 35 (highly desirable treatment need), and a score greater than 36 (mandatory treatment) [13].
While DAI and DHC-IOTN are widely used instruments to determine malocclusion and the need for orthodontic treatment, Kosovo, to date, has not produced data to assess their validity and reproducibility in the identification of orthodontic treatment need of Kosovar children. Thus, the aim of this study is to assess the applicability of DAI and DHC-IOTN in the Kosovar context with the aim of assessing the prevalence of orthodontic treatment need among Kosovar children of ages 11-13.
2. MATERIALS AND METHODS
This study was carried out in accordance with recommendations of the Helsinki Declaration and was approved from the Research Ethics Committee of the University Dentistry Clinical Center of Kosovo (University of Prishtina) and Ministry of Education, Science and Technology of Kosovo. Written consent was taken from all subject’s parents.
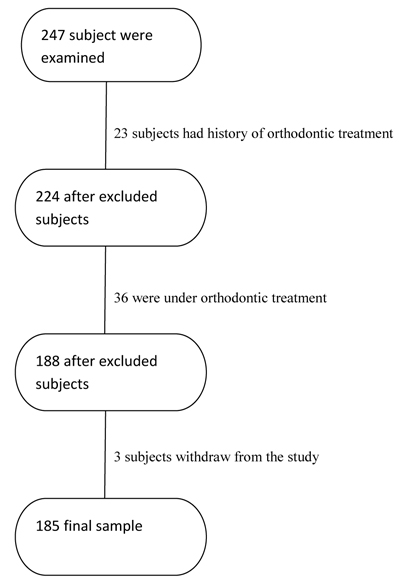
A total of 247 subjects, aged 11-13, were examined in one elementary school in Prishtina. Out of this number 23 subjects were excluded due to history of orthodontic treatment, 36 subjects were excluded because of current orthodontic treatment, and 3 subjects withdraw from the study. The final sample consisted of 185 subjects (50.3% female), aged 11-13 (Fig. 1).
The sample size calculation was performed by considering the 54.3 percent prevalence of orthodontic treatment need, as measured by the DAI, with a confidence interval of 95% and 5% of level of precision [1, 14, 15]. During sampling, the following exclusion criteria were applied: 1) No history of orthodontic treatment, 2) No ongoing orthodontic treatment.
Data on the overall oral condition were obtained for selected subjects. One researcher, an expert in orthodontics, previously trained and calibrated on the use of the index, gathered the following data for each participant: dental insufficiency, crowding, maxillary and mandibular median diastema, overjet, Angle’s classification, bite type, and other anomalies in the maxillary and mandibular anterior region. The examination was performed in natural light by means of a wood spatula, millimetric ruler, sterile gloves, and disinfectant.
For each subject, DAI and the DHC-IOTN values were classified according to the specific criteria of each index studied [2, 13, 16]. The aesthetic component of the IOTN was not assessed, as it presents poor association with the clinical condition [17]. The instruments used were those recommended for each index, namely the periodontal probe for the DAI and the proper ruler for the DHC-IOTN.
In our study, DAI scores were dichotomized as “no need for treatment” (DAI ≤ 25) and “in need of treatment” (DAI > 25). Likewise, DHC-IOTN scores were classified into “no need for treatment (grades 1 and 2) and “in need of treatment” (grades 3,4, and 5).
2.1. Statistical Analysis
Data analysis was performed using the Statistical Package for Social Sciences (version 16.0, SPSS Inc., Chicago, Illinois, USA). Descriptive statistics were compiled for all variables. Crosstables and chi-square test was used to test the distribution differences between genders.
3. RESULTS
The need for orthodontic treatment in our sample is very high, according to IOTN DHC. When presented based on our dichotomous categorization, 82.7 percent of the subjects were in need of treatment, while 17.3 percent were in no need of treatment. It is worth noting that 47.6 percent of the sample had very severe malocclusion. No significant gender-based differences were noted regarding treatment need (p=0.215). A breakdown of distribution for each category is presented in Table 1.
| IOTN DHC | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Normal or minor malocclusion | 5 | 5.43 | 12 | 12.9 | 17 | 9.2 |
| Minor malocclusion | 10 | 10.87 | 5 | 5.4 | 15 | 8.1 |
| Moderate malocclusion | 16 | 17.39 | 14 | 15.1 | 30 | 16.2 |
| Severe malocclusion | 20 | 21.74 | 15 | 16.1 | 35 | 18.9 |
| Very severe malocclusion | 41 | 44.57 | 47 | 50.5 | 88 | 47.6 |
| Total | 92 | 100 | 93 | 100 | 185 | 100 |
| Male | Female | Total | ||||
|---|---|---|---|---|---|---|
| DAI | N | % | N | % | N | % |
| No treatment need | 72 | 78.3 | 72 | 77.4 | 144 | 77.8 |
| Moderate treatment need | 8 | 8.7 | 14 | 15.1 | 22 | 11.9 |
| Treatment need | 8 | 8.7 | 3 | 3.2 | 11 | 5.9 |
| Treatment mandatory | 4 | 4.3 | 4 | 4.3 | 8 | 4.3 |
| Total | 92 | 100 | 93 | 100 | 185 | 100 |
The dichotomization of DAI scores reveals that the majority of the schoolchildren have no treatment need (77.8%), while 22.2 percent of the sample needed treatment. In subcategories, treatment was highly desirable in 5.9 percent and mandatory in 4.3 percent of children. No significant gender-based differences were noted in treatment need based on DAI index (p=0.272). A breakdown of distribution for each category is presented in Table 2.
4. DISCUSSION
The prevalence of malocclusion and orthodontic treatment need found in our study is much higher than in European countries. According to DHC IOTN as an objective method, as much as 66.5 percent had definite treatment need because they were categorized in grades 4 and 5 of treatment need. Based on our dichotomous variables, 82.7 percent of the subjects were in need of treatment.
The prevalence of orthodontic treatment need varies among different countries. It is much lower in European countries. In France, Souames et al. found 21.3 percent of children needed orthodontic treatment [4]. In Italy, Perillo et al. found similar results - the prevalence rate for (grades 4 and 5) was 27.3 percent of the total sample [5]. In Spain, Manzanera et al. found that 23.5 percent of 12-year-olds and 18.5 percent of 15- to 16-year-olds had a definite treatment need, while in the United Kingdom, Chestnut et al. in a sample of 12- to 15-year-old subjects, found 21 percent to 35 percent to have definite orthodontic treatment needs [6, 7].
However, prevalence rates of orthodontic treatment need in Asian and African countries seem to be quite high. Abdullah and Rock reported prevalence for an objective orthodontic treatment need of 47.9 percent for a Malaysian sample of 12- to 13-year-old schoolchildren [10].
Similarly, Ngom et al. found that 42.6 percent of a Senegalese sample, with 12- to 13-year-old adolescents, was categorized as grade 4 or 5 of the DHC of the IOTN [11].
Studies from the region show great differences. The study conducted in Serbia by Janošević et al. shows similar results to those of other European Counties, with 27.4 percent of children having a definite need for orthodontic treatment [8]. The study conducted in Albania by Lagana et al. found that 41.2 percent of respondents had the need for orthodontic treatment in Tirana [9]. This prevalence is quite high, but much lower then the one found in our study.
Our findings show that Kosovar children aged 11-13 years old have more malocclusion than their counterparts in neighboring countries. It is well known that causes of malocclusion are multifactorial with genetics having a key role; however, lack of preventive measures and oral health promotion programs as well as lack of systemic dental control causes premature tooth loss, this, in turn, causes malocclusion. Higher prevalence of orthodontic treatment need tells us that more children will require orthodontic therapy in the future.
The low prevalence of definite need for orthodontic treatment in developed countries can be attributed to early prevention measures [9]. On the other hand, the high prevalence of orthodontic need in developing countries, including our country, can be the result of the lack of appropriate dental health information, therefore lack of early intervention, as well as the low economic status of the majority of the population.
While our study is the first one to evaluate the orthodontic treatment need in Kosovar children of specific ages in Prishtina, the early results reveal the need for an interceptive orthodontic treatment. The assessment of orthodontic treatment needs across the population provides data that would enable policymakers to develop a national program for prevention and early orthodontic treatment. It is very important to assess orthodontic anomalies in a population so that planning of public health care expenditures and services can ensure coverage and accessibility in the most efficient way possible.
CONCLUSION
High prevalence of orthodontic treatment need was identified in Kosovar children of ages 11-13, while no gender-based statistically significant differences were noted in the need for orthodontic treatment.
This means that in the future, national budget funding for orthodontic treatment should be higher as treatment cost will burden the health budget.
More effective oral health education and promotion programs are needed in Kosovo.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved from the Research Ethics Committee of the University Dentistry Clinical Center of Kosovo (University of Prishtina) and Ministry of Education, Science and Technology of Kosovo.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was taken from all subject’s parents.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest, financial, or otherwise.
ACKNOWLEDGEMENTS
Declared none.

