All published articles of this journal are available on ScienceDirect.

Knowledge and Practices of Triage Amongst Nurses Working in the Emergency Departments of Rural Hospitals in Limpopo Province
Abstract
Background:
Many deaths in hospitals occur within 24 hours of admission. Some of these deaths could be prevented if the patients were effectively triaged, identified quickly, and treatment initiated without delay. Triage and emergency care have always been weak and under-emphasized components of healthcare systems in rural areas of Limpopo Province, and yet, if well organised, it could lead to saving many lives and reducing the ultimate costs of care. There have been few studies, and there is little information focusing on nurses’ knowledge about triage in rural hospitals.
Objective:
This study aims to assess the knowledge and practices of triage amongst nurses working in the Emergency Departments (ED) of the Sekhukhune District, Limpopo Province, South Africa.
Methods:
By employing a quantitative, non-experimental research method, 84 nurses working in the Emergency Departments, completed and submitted structured questionnaires. The validity and reliability were ensured by pre-testing the data collection instrument on respondents who were not part of the main study. Data were analyzed by using the SPSS version 25, Excel computer programs and score methods.
Results:
The findings indicate that there is a correlation between triage knowledge and job title (p-value = 0.046). Registered nurses, specialty nurses, and enrolled nurses, were found to know more than auxiliary nurses. However, the study discovered that, among the nurses with knowledge, 61% exercised poor triage practice, while only 30% showed evidence of good practice.
Conclusion:
The study aims at defining triage knowledge and practice amongst nurses in the Emergency Departments. The results indicate that nurses have knowledge regarding triage but have difficulty in converting their factual knowledge into practice, as they scored poorly on questions about the practice. In addition, there emerged a significantly positive relationship between triage knowledge and job titles. The study recommends the development of strategies to enhance the conversion of factual knowledge into practice regarding triage in the ED. This could be implemented through sustainable training courses regarding triage for all the categories of nurses.
1. INTRODUCTION AND BACKGROUND
The triage of patients in the Emergency Departments (ED) is a worldwide healthcare problem. Triage is commonly defined as an essential procedure in ED that involves sorting patients according to priorities [1], thereby reducing patients’ waiting time and improving the quality of patient care [2-4]. Afaya et al. [5] indicate that an unfair allocation of patients in the triage room can have adverse outcomes for patients. Such outcomes according to Ali et al. [6] include compromised patient care and escalated death rates in ED [7]. However, the outcomes are influenced by various factors, such as the type of triage system, the effectiveness of the system and the knowledge and skills of emergency staff in ED.
The triage systems date back to World War 1 when military surgeons developed and implemented triage rules to promptly evaluate and categorize wounded soldiers [8]. The Emergency Departments around the world use different triage systems to assess the severity and urgency of incoming patients’ conditions and to assign treatment. Triage instruments include the Australian Triage Scale (ATS), the Canadian Triage and Acuity Scale (CTAS), the Manchester Triage System (MTS), the Emergency Severity Index (ESI) [9]. The CTAS, MTS and ATS, although used widely in European countries, all require extensive training to implement, making their widespread adoption in African settings challenging [10].
Although many developing countries in Africa did not have any formal triage system to categorise incoming patients in their ED, many countries have adopted a particular system for improving the quality of patient care. For instance, South Africa [11], has developed and validated a triage scale known as the South African Triage Scale (SATS) which is effective in sorting and categorizing patients in the ED. Other African countries, like Botswana, and also some Asian countries (Pakistan) have adopted the system [12]. According to Twomey et al. [13], the reasons for using the SATS are that it is simple and easy to use in low-resource clinical settings and is effective in ED. Although the system is easy to use, Soogun et al. [14] indicate that the benefits of the system, such as reducing the waiting period for patients and improving patient flow [8, 12, 15], depending on the correct implementation of the tool in hospitals in both urban and rural areas. SATS involves asking for the complaints, looking for clinical signs and measuring vital signs. These results are then used in calculating the Triage Early Warning Score (TEWS) [13, 14].
Unfortunately, in the South African healthcare environment, human resource constraints do not readily allow for a physician-led triage system or the most-qualified nurses always to be available to perform triage. This is because of a lack of skills and knowledge of specialized healthcare providers in the ED - [15] which is a serious concern. A high staff turnover often results in expertise being lost, which according to Mirhagi et al. [16] affects the effective implementation of the Triage system in ED. According to Goldstein et al. [17], the effectiveness of triage is embedded in the knowledge and skills of the emergency staff. The emergency staff in ED comprises medical doctors, professional nurses, and allied staff members, such as radiographers. This manuscript focuses on nurses. According to Kenneth et al. [18] and Ali et al. [6], the skills and knowledge of nurses are critical for effective triaging and are a key element for the provision and improvement of quality patient care in ED. However, there is continued concern about the knowledge of triage amongst nurses working in ED. These concerns extend beyond South Africa, to include Pakistan, Dar es Salaam and Ghana [5, 6, 18, 19].
In Limpopo Province of South Africa, a study conducted by Cimona-Malua [20] in the Sekhukhune District found that the triage system was inefficient and needed improvement. The study found that patients waited too long to be triaged. To the author’s knowledge, there has been no study focusing on the knowledge of triage amongst nurses working in ED in hospitals of rural areas. The ED staff in rural hospitals receive little training regarding triage of patients. The triage system has always been weak and an under-emphasized component of the health care system in rural areas and yet, if well organised, it could lead to saving many lives and reducing the patient waiting period and the ultimate cost of care. The hospitals in rural areas face serious over crowding in the ED. For this reason, they need an effective triage system with highly skilled and knowledgeable staff. The current authors believe that assessing nurses’ triage knowledge will improve triage practices and the quality of patient care in the ED. Therefore, this paper describes the knowledge and practices of triage amongst nurses working in the ED of the Sekhukhune District hospitals.
2. MATERIALS AND METHODS
The study used a quantitative approach, utilizing a cross-sectional design that takes place at a specific point in time [21]. The design was appropriate for achieving the research objective. The design was selected based on the fact that most of the South African studies, such as [14, 22, 23] conducted on triage, used a retrospective design. The current authors wanted to describe the knowledge of triage amongst nurses working in ED using a different design.
2.1. Study Site
According to the National Government of South Africa [24], Limpopo Province has five districts: Sekhukhune, Capricorn, Vhembe, Mopane and Waterberg District. The districts are further divided into local municipalities. The study was conducted in Sekhukhune District, which has five district hospitals, all of which provide 24-hour emergency services to patients in rural areas. Table 1 below shows the total number of hospitals, according to the municipalities of the Sekhukhune District:
| Hospital | Municipality | Total Number of Nurses |
|---|---|---|
| Dilokong Hospital | Greater Tubatse Municipality | 18 |
| Mecklenburg | Greater Tubatse Municipality | 21 |
| Jane Furse Hospital | Makhuduthamaga Municipality | 25 |
| Groblersdal Hospital | Elias Motswaledi Municipality | 19 |
| Matlala Hospital | Greater Marble Hall Municipality | 22 |
2.2. Population
A total number of 105 nurses (this includes all categories, such as registered/professional nurses, staff nurses and auxiliary nurses) working in the Emergency Departments of the Sekhukhune District Hospitals in Limpopo Province South Africa, constitute the population of the study.
2.3. Sample, Sampling Technique and Sample Size
A simple random sampling was supported by a table from Krejcie & Morgan [25] to determine a sample size of 85 from the total population of 105 nurses in this study. The sample size (85) was then divided by five, the total number of all district hospitals of Sekhukhune as they all had an almost equal number of staff members in their Emergency Departments. The fishbowl technique was used to select respondents randomly. Each number assigned to a respondent was written on a piece of paper and then placed in a container. The researcher then drew a piece of paper, noted the number and replaced the piece of paper to shake again and selected the second and third and so on, until the required number of 17 respondents per hospital was met.
2.4. Data Collection
Turfloop Research Ethics Committee (TREC) gave ethical clearance for the study to be conducted (TREC/372/207: PG). Permission to conduct the study in the hospitals was granted by the Limpopo Department of Health. The Sekhukhune District office gave permission to conduct the study within the district hospitals. The Chief Executive Officers (CEO’s) of the five hospitals granted permission to approach nurses working in the ED. The Deputy Nurse Managers and Operational Managers of the ED assisted in arranging dates and a quiet area for the distribution of questionnaires. Data collection dates were arranged at a time when most nurses would be available on duty. For example, ward meeting dates and changing of shift dates, to avoid disturbing the nursing care activities. At the time of data collection, the researcher gave instructions to respondents and informed them the reason for the research and explained the ethics, anonymity and confidentiality of the study. This was repeated in a consent form that the respondents signed before partaking in the study. Data were collected from nurses working in the Emergency Departments of the five hospitals of the Sekhukhune District through structured questionnaires. The researcher took a month to collect data, from 23 July to 24 August 2018. The duration for completion of the questionnaire ranged from 45 to 60 minutes in the private rooms of the five ED of Sekhukhune District Hospitals.
2.5. Data Collection Instrument - Questionnaire
The questionnaire consisted of 3 sections: Section A - Demographic data, B - Triage knowledge and C - Triage practice and waiting-time. The questionnaire was only available in English. The instrument was developed from the literature review, as published and tested instruments on the topic were not available for this study.
2.6. Reliability and Validity of the Research Instrument
The validity was safeguarded by grounding the questionnaire in existing scientific knowledge obtained from the literature. A panel of experts in the field were consulted to validate the appropriateness and accuracy of the questionnaire. Face validity was ensured by giving the questionnaire to the researcher’s supervisor and co-supervisor. The content validity of the questionnaire was ensured through an extensive review of the literature to check that the content of the instrument would achieve the objectives of the study. The supervisor and co-supervisor in the Nursing Department, Senior Degrees’ Committee members of the University, and the Turfloop Research Ethics Committee (TREC) reviewed the questionnaire to ensure content validity and changes were made in line with their recommendations. Reliability was enhanced by checking and testing the questionnaires during pre-testing. The main drive of the pilot study was to allow the researcher to amend or correct the research instrument tool before the actual data collection process. Pre-testing was done in the Emergency Department of a hospital that was not part of the main study.
3. ANALYSIS
Data were analysed using the IBM Computer program Statistical Package for the Social Sciences (SPSS version 25) and the Microsoft Excel programme with the help of the University of Limpopo statistician. The descriptive and inferential statistics were used to correlate the variables. The descriptive variables are often used to describe the average of a variable in a population [26]. The Chi-square and crosstab analyses were carried out to calculate the relationship between the demographic factors and the knowledge and practices of triage amongst nurses in the Emergency Departments. A mark sheet was used to analyze questions relating to the knowledge and practices of triage amongst nurses working in the ED of the Sekhukhune District hospitals.
4. PRESENTATION OF RESULTS
As the data collection instrument was divided into 3 sections, the presentation of the results followed the format of the instrument, that is, Section A shows findings on the demographic variables of the respondents, while sections B and C describe the knowledge and practices of triage amongst nurses in the Emergency Departments.
4.1. Demographic Profile of the Participants
The demographic information and their relevance to the studied problem are charted below:
4.1.1. Gender Distribution
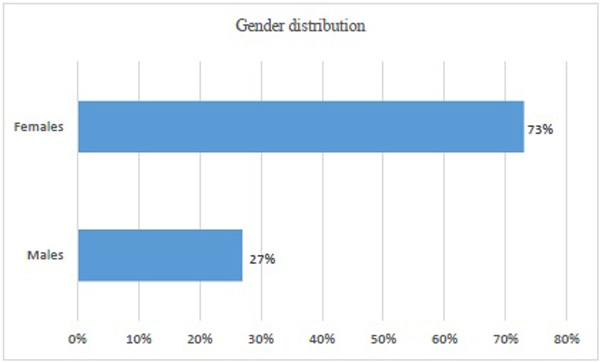
Fig. (1) presents the gender of the participants. The study indicates that most of the participants in this study are female, 73%, and 27% males. This indicates that the Emergency Departments where data was collected were dominated by females, which might be because the nursing profession is predominantly female.
4.1.2. Age Distribution
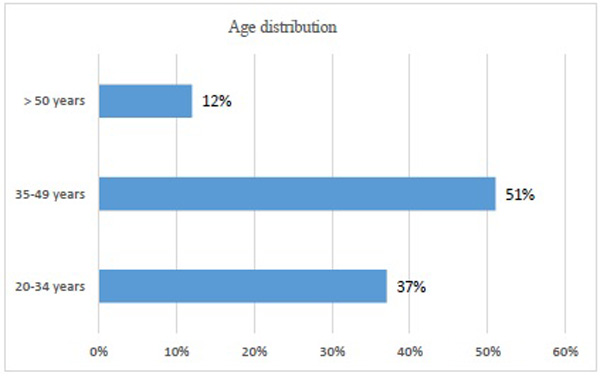
Most of the respondents in this study (51%) were between the ages of 35 and 49, followed by those in the age group of 20-35 (37%). This indicates that nurses in the Emergency Departments represent the most active working age group, as the oldest were the fewest with 12% (Fig. 2).
4.1.3. Job Titles of Nurses
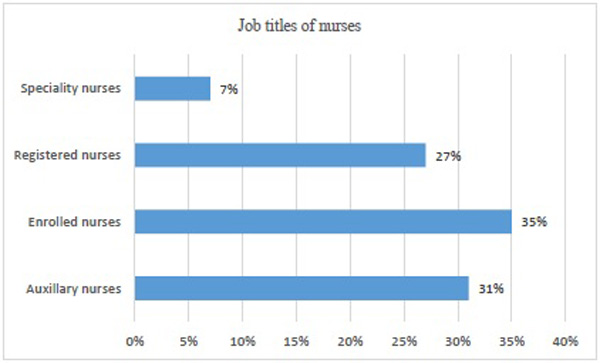
Enrolled nurses formed the largest category of participants with 29 (35%), followed by auxiliary nurses with 26 (31%). This indicates that there is a shortage of registered nurses (27%) and specialty nurses (7%) in the Emergency Departments. These categories are the ones most needed in the Emergency Departments because of their knowledge, the scope of practice and triage, as physician-led triage is difficult in South Africa because of the shortage of physicians.
All nursing personnel are eligible to triage in the Emergency Departments despite their job titles, but in this study, auxiliary nurses are the second largest population with 31%, after enrolled nurses with 35%. This is a concern as the auxiliary nurses are the group that is mostly delegated to triage due to a shortage of registered and specialist nurses, meanwhile they have been shown in this study to be the group with deficient triage knowledge and practice (Fig. 3).
4.1.4. Qualifications of Nurses
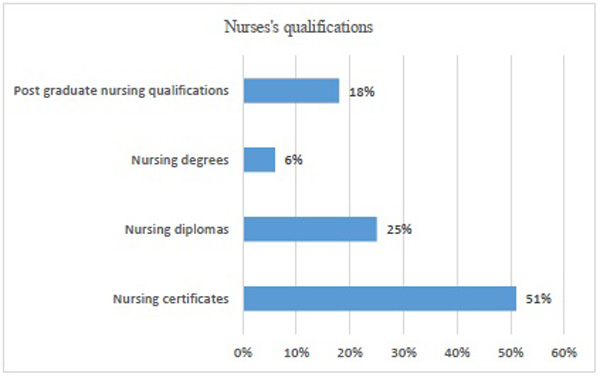
Most of the participants in this study have certificates (51%). This is because the majority of the respondents in this study were enrolled nurses (35%) and auxiliary nurses (31%), and these groups have one-year and two-year nursing certificates. Nurses with diplomas made up 25% compared with 6% of those possessing degrees. This might be because nursing colleges have a greater intake and output of nursing graduates than universities do (Fig. 4).
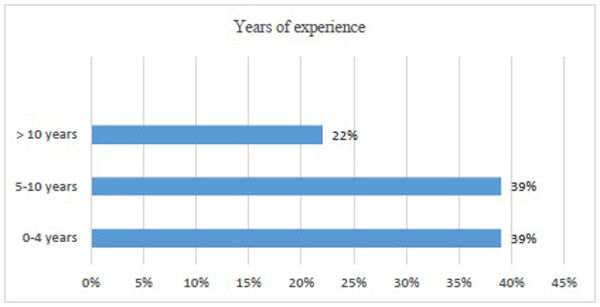
4.1.5. Years of Experience
With years of experience, the most experienced nurses, with more than 10 years of working experience, were the fewest at 22% followed by the experience of 0 - 4 years and 5 -10 years, each scoring 39% (Fig. 5).
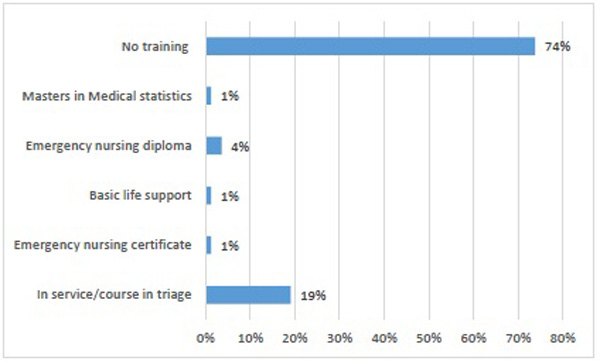
4.1.6. Triage Training
The study reveals that most participants (74%) had neither formal nor in-service training in triage as compared with 19% with triage training. Only 1% had basic life support training, and 5% had attended emergency nursing courses, necessary for quality emergency care. One percent (1%) had a Masters’ in Medical Statistics, which is irrelevant for emergency patient care (Fig. 6).
The demographic results indicate that most of the respondents in this study were female, 73%, with males making up only 27% of the gender variable. Most of the respondents in this study (52%) were between the ages of 35 and 49, followed by those in the age group of 20-35 (39%). This indicates that nurses in the Emergency Departments were mostly part of the active working-age group, as the oldest were the fewest with 8%. Enrolled nurses form the largest category of the respondents with 29 (35%), followed by auxiliary nurses with 26 (31%). This indicates that there is a shortage of registered nurses (27%) and specialty nurses (7%) in the Emergency Departments. These categories are the ones most needed in the Emergency Departments because of their knowledge and scope of practice in triage, particularly because physician-led triage is difficult to implement in South Africa because of the shortage of physicians. Most of the respondents in this study have certificates (52%), other than a degree certificate in nursing. This is because the majority of the respondents in this study were enrolled nurses (35%) and auxiliary nurses (31%) and these groups have one-year and two-year nursing certificates. Nurses with diplomas were 18% compared with 5% of those possessing degrees. This might be because nursing colleges have a greater intake and output of nursing graduates than universities do. The majority of the respondents (40%) had less than five years of experience in the Emergency Departments, those with 5-10years of experience make up 38%, and the most experienced were the fewest, with only 18%. In this study, most of the participants (74%) had neither formal nor in-service training in triage.
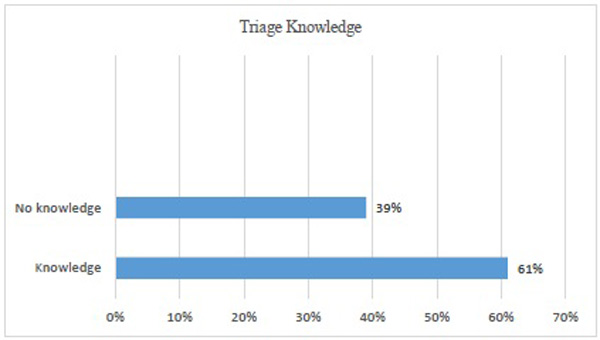
4.2. Triage Knowledge
Fig. (7) indicates that 61% of the respondents were knowledgeable about triage, whereas 39% demonstrated insufficient knowledge.
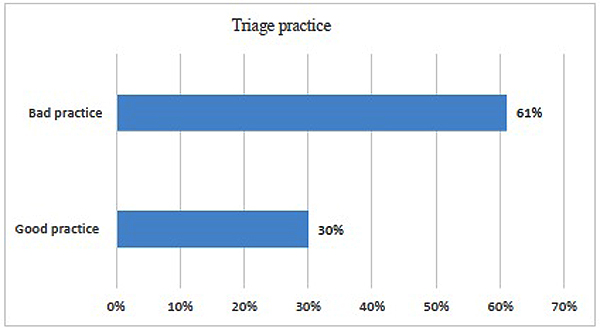
4.3. Triage Practices
Fig. (8) below demonstrates the results of the practices of triage related to the study objective.
Sixty-one percent of the respondents demonstrated to bad triage practice despite showing greater knowledge of triage. This might be because 39% of respondents had less than 4 years of working experience in the Emergency Department and 74% were not trained in triage. 9% of respondents did not have a triage system hence they did not answer the section about triage practice
5. DISCUSSION OF RESEARCH RESULTS
5.1. Gender and Age Distribution
This study reveals that 73% of the nurses were female compared with only 27% of males. This could be because the nursing profession is primarily dominated by the female gender. There was no statistical association between the variables, gender and age, on triage knowledge. The p-values were 0.128 and 0.213 respectively. This means that both males and females had the same triage knowledge, regardless of their gender or age. This is consistent with the study by Manoharan et al. [27], where the gender and age variables had no statistical significance
Most of the nurses in this study (51%) were between the ages of 35 and 49, followed by 37% between the ages of 20 and 34 years and, lastly, 12% were older than 50 years. These indicate that most of the participants in this study were of the active-working age group, less than 50 years of age. This is the age group that is expected to perform better in the Emergency Departments.
5.2. Job Titles
Enrolled nurses made up the largest category with 29 (35%), followed by auxiliary nurses, with 26 (31%). This indicates that there is a shortage of registered nurses (27%) and specialty nurses (7%), not only within the Emergency Departments but in the nursing fraternity as a whole. Registered and specialist nurses are urgently needed in the Emergency Departments because of their knowledge and the scope of practice of triage. Physician-led triage is a challenge in South Africa because of human resource constraints. According to Goldstein et al. [17], to compensate for the lack of highly qualified and experienced nurse practitioners in triage, SATS was designed to be used by auxiliary and enrolled nurses as well. All nurses are eligible for triage in the Emergency Departments, regardless of their job titles. In this study, auxiliary nurses are the second largest population with 31%, after enrolled nurses with 35%. Auxiliary nurses are mostly delegated to triage rooms and this is a cause of concern as this study has shown that they have poor triage knowledge and can’t practice efficiently. There is a positive association between triage knowledge and job titles. Enrolled nurses, registered nurses, and specialty nurses know more than auxiliary nurses, p-value (P =0.046). According to SATS, an auxiliary nurse must seek the advice of an experienced registered nurse in triage. For example, when triaging babies and other complicated cases.
5.3. Nurses’ Qualifications
Most of the participants in this study had certificates (51%). This is because the majority of the participants were enrolled nurses and auxiliary nurses . These categories of nurses have one-year and two-year nursing certificates. Twenty-five percent (25%) of the nurses had diplomas, compared with the 6% possessing degrees and 18% with post-graduate nursing qualifications. This could be because nursing colleges have a greater intake and output of nursing graduates than universities in South Africa.
5.4. Years of Experience
The most experienced nurses, with more than 10 years of experience, were the fewest with 22%, while those with less than five years and 5-10 years were equal, both scoring 39%. Thirty-nine percent (39%) of the participants had less than 5 years and 5-10 years of working experience respectively, yet their triage knowledge was good (61%). Despite that, only 30% of participants in this study demonstrated good triage practice and 30% of the participants with good triage practice came from the 22% of the most experienced nurses with more than 10 years of working experience in the Emergency Departments. According to Benner’s [28] theory on the five stages of skill acquisition, one needs to have at least three years or more of working experience in the same job environment to be competent. The job titles of nurses in this study indicate that the lower category of nurses including auxiliary nurses, scored poorly on triage knowledge and practice. They make up 31% of the participants. According to Kerie et al. [29], in the study assessing levels of triage skills and associated factors among emergency nurses in Addis Ababa, Ethiopia; nurses demonstrated moderate triage skills (52.9%). Triage training, knowledge about triage and educational levels reflected a significant relationship with triage practice (p=.002). This is consistent with the findings of this study, where only enrolled nurses, registered nurses and specialty nurses demonstrated better triage knowledge than auxiliary nurses whose level of education is the lowest of the three nursing categories.
5.5. Triage Knowledge, Experience, and Practice
Sixty-one percent (61%) of participants in this study demonstrated good triage knowledge which is consistent with the study conducted by Afaya et al. and Ali et al. [5, 6], where the studies revealed that 62.6% of the respondents were knowledgeable about triage because they correctly answered more than 50% of the questions in the self-administered questionnaires in the Emergency Departments of hospitals in Tamale, Metropolis, Ghana. In the study of Ali et al. [6] 69% of the participants in Pakistan had poor triage knowledge. This is consistent with the study conducted by Kenneth et al. [18] on the assessment of knowledge of triage amongst nurses working in the Emergency Departments of Dar es Salaam, Tanzania, where only 33% of the participants were not knowledgeable about triage. In addition, 13% of the participants reported that although they had attended workshops, there had been a lack of information and protocols on how to triage patients. Fifty-two percent (52%) demonstrated poor triage practice as they could not allocate appropriate triage categories. These results are congruent with the results of the present study, where 61% of the participants demonstrated poor triage practice.
Interestingly, although most of the participants in this study (61%) had good triage knowledge, they scored poorly in the practice of triage skills as they failed to follow the first three steps in triaging a patient in the Emergency Departments, according to the South African Triage Scale (SATS). These findings contradict the findings of Duko et al. [30] where triage skills were better while triage knowledge was of a low level. The study by Kerie et al. [29], and many previous studies reveal that there is a strong positive relationship between triage knowledge and practice. However, according to Considine et al. [4], having only knowledge about triage does not always yield good triage practice or skills because knowledge is factual, and the acquisition of factual knowledge is not necessarily associated with behaviour change in terms of practice and clinical decisions. This was evident in this study.
This study found that 74% of the participants had not attended triage training or in-service workshops while 19% had received triage training. These findings are consistent with the study by Mucktar & Fadlallah [30]. In their study, They assessed nurses’ knowledge of triage systems in the emergency departments in a public hospital in Khartoum and found that only 17% of the participants had received triage training.
According to Duko et al. [31], training on triage has a significant correlation with triage skill and practice. Their study found that triage knowledge and practice were further affected by the working experience of nurses, their educational status, triage training, and triage experience. In the current study, nurses’ triage skills or practices were poor which could be attributed to the fact that nurses were not trained in triage, the majority had less than 5 years of working experience and little education Most of them were auxiliary nurses and enrolled nurses whose educational qualifications were low. However, the results showed no significance except for job titles which are related to educational status as registered and specialist nurses have higher qualifications. A study conducted by Hammad et al. [32] reveals that just over half (50.8%) of the participants from 13 tertiary hospitals in Changsha, China, reported receiving dedicated triage training provided by their employers (38.6%), an education organization (30.7%) or a conference (26.1%). Approximately, half of them (53.2%) reported using formal triage scales. It is a huge concern within the nursing profession that the level of care in the Emergency Departments is deteriorating due to ineffective triaging.
Formal training in triage improves the effectiveness of triage nurses and, with improved confidence, nurses are more prepared to triage effectively (Rahmati et al). [33]. Another strategy is to train nurses in the field of triage on a continuous basis. The study by Rahmati et al. [33] on the knowledge of triage indicates that most nurses scored poor marks on triage knowledge but that their marks improved after triage training. However, they scored poor marks again after six weeks. This indicates that continued education on triage is necessary to maintain efficient and up-to-date triage skills. Findings by Tilahun [34] on the knowledge and triaging among nurses working in the emergency department of a government hospital in Addis Ababa, Ethiopia, suggest that there training is inadequate and nurses working in the emergency department have little knowledge. Hence, they need continuuous education and training in order to improve their triage skills and practices. Nine percent of the participants did not respond to questions on triage practices, they did not practice it within their Emergency Department. Further studies could be conducted to explore the reasons behind the challenges of practicing triage.
The study conducted by Naidoo [35] on the evaluation of the emergency care training workshops in the province of KwaZulu-Natal, South Africa, has revealed that participants felt that their knowledge and skills improved significantly across all modules (p < 0.001). The mean difference across all modules; pre-workshop compared with post-workshop was -1.22 (95% confidence interval: -1.45; -0.99), which is statistically significant. Knowledge significantly improved post- triage workshops for both doctors and nurses, the nurses’ mean scores were higher than the doctors’. Many of the participants suggested that simulations and workshops should be conducted at each hospital more often to enhance triage knowledge and practice (Naidoo [35]). The results of the study conducted by Asgari et al. [36] showed no significant relationship between work experience, gender and age with the level of knowledge and the practice of triage. However, there was a significant relationship between knowledge and the practice of triage in nurses with nursing education. In the current study, nurses with the lowest qualifications; auxiliary nurses were found to have little knowledge of triage and did not practice it in the Emergency Departments. Furthermore, Asgari et al. [36] added that nurses’ knowledge of triage was greater than the level of practice. This indicates that their theoretical knowledge is greater than their practical knowledge. This finding coincides with the finding in the current study where nurses were found to be knowledgeable about triage (61%) but poor in its practice. Only 30% demonstrated good triage practice.
Findings by Fathoni et al. [2] support the findings of this study. Knowledge, experience, or training alone are not enough to yield accurate clinical decisions. Due to which, 61% of the participants scored poorly on triage practice: they had not received training and 40% had less than 4 years of working experience in the Emergency Departments. According to Benner‘s [28] theory of five stages of skill acquisition, most of the nurses in this study (40%) were at a competent level of skill acquisition, in terms of years of experience. More proficient and expert nurses are needed for triage. The integration of different types of knowledge results in knowledge that is applicable to a range of clinical situations and practice. A proficient nurse, according to Benner’s theory, perceives the situation as a whole, not in parts, whereas an expert nurse has a deep connection and understanding of the situation. Only one study disputes the notion that factual knowledge improves triage practice or decision-making [2].
CONCLUSION
This study aims to define triage knowledge and practice of nurses in the Emergency Departments. The results indicate that nurses know about triage but have difficulty in converting factual knowledge into practice, as they scored poorly in practice. The authors recommend the development of strategies to enhance the conversion of factual knowledge into practice regarding triage in ED. In addition, there was a significantly positive relationship between triage knowledge and job titles, with auxiliary nurses having less knowledge. The study recommends a sustainable training programme to enhance both knowledge and practice for all categories of nurses.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance to conduct the study was given by the University of Limpopo Turfloop Research Ethics Committee, (TREC/372/2017: PG). The permission to conduct the study in hospitals was granted by the Limpopo Province, Department of Health Research Ethics Committee, and the Sekhukhune District office.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The participants were informed about the topic, purpose, and objectives of the study and their rights to participate and/or withdraw from the study should they wish to do so without being victimized. They were also informed about the risks and the benefits of the study. All participants were made aware that if any emotional or psychological distress was caused as a result of the study, they would be referred to a counselor since all the hospitals have registered counselors. The respondents received all the information before they voluntarily signed a consent form. The study was explained to the respondents briefly and their permission was taken to administer the questionnaire. The questionnaires were only given to those who agreed to participate and no one was pressurized to participate. The anonymity of the respondents was ensured by not including the respondents’ names on the questionnaires. This was done to ensure that the responses could not be linked with the identity of the participants. The confidentiality of the respondents was further ensured by not divulging information about the study to anyone who was not directly linked with the study. The participants completed the questionnaire in a private room and signed consent forms which were kept under lock in a safe place and are supposed to be destroyed five years after the completion of the study.
AVAILABILITY OF DATA AND MATERIALS
Due to confidentiality issues, it is not permitted to share the data.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
To the University of Limpopo Nursing Department staff, your energy and commitment to developing students in research gave me the courage and drove me to accomplish my goal.
To the Department of Health, Limpopo Province and Sekhukhune District, thank you for granting me permission to conduct the research study at your healthcare institutions.
To all the nurses working in the Emergency Departments of Mecklenburg Hospital, Dilokong Hospital, Fane Furse Hospital, Matlala Hospital and Groblersdal Hospital, who participated in this study, thank you for your co-operation and willingness to offer data by completing the questionnaires.
To the statisticians, Mr. Peter Letsoalo and Mr. Peter Mphekgwana, thank you for your assistance and direction with data analysis.
To the editor, Sue Matthis, thank you for providing editorial assistance.

