All published articles of this journal are available on ScienceDirect.

Assessment of High School Students’ Knowledge, Attitudes and Vaccination Status of Hepatitis B Virus in Hohoe, Ghana: A Cross-sectional Study
Abstract
Background:
Hepatitis B Virus (HBV) is a highly infectious disease and a major global public health threat. About one-third of the world’s population is estimated to be infected with Sub-Saharan Africa and East Asia, regarded as high prevalence regions of between 5-10% of the adult population chronically infected. Comprehensive knowledge of HBV in highly endemic areas like Ghana among population groups is crucial to mitigating the effects of the disease. Thus, the objective of this study was to assess the knowledge of students of two high schools on the Hepatitis B Virus (HBV) in the Hohoe Municipality of the Volta Region of Ghana to identify and describe their risk of infection, attitude, test, and vaccination status.
Methods:
A descriptive cross-sectional survey was conducted in the two Senior High Schools. The survey involved 244 students of both boys and girls from years one to three. Recruitment was through a stratified simple random sampling technique. Data was collected via respondents’ self-administered questionnaire. Data was analysed using STATA version 12.0.
Results:
The results of the study showed moderate knowledge, especially of the modes of transmission and prevention among the majority of the respondents (89.2%). Protection against the virus was a concern as about 19.5% reported receiving the HBV vaccine, with 7.2% completing all three doses. Respondents also showed a generally positive disposition towards the disease. The school and mass media were the main sources of information about HBV.
Conclusion:
The findings of the study showed that high school students (teenagers) have various misconceptions about HBV as the majority of students in the Hohoe municipality had moderate knowledge of HBV. The study also established that teenagers are at risk of contracting the virus, given the low vaccination status, as seen in the study.
1. INTRODUCTION
Hepatitis B Virus (HBV) infection is one of the commonest viral hepatitis worldwide and a major global public health problem with varied prevalence across the world [1, 2]. It is estimated that about one-third of the world’s population has been or is infected with hepatitis B virus (HBV) and around 290 million are chronic carriers [3, 4] despite the availability of effective vaccines against the virus [4, 5]. Thus, the virus is endemic in most parts of the world, with higher endemicity in Asia and sub-Saharan Africa, where seroprevalence is above 6% [1, 6].
Ghana has been grouped among the areas of the world, where the prevalence of chronic HBV infection is high (≥8 %) [7], and that of the hepatitis C virus is also high (5-10%) [8]. Therefore, Ghana is regarded as an endemic hepatitis B country, with about 8%-20% of the adult population estimated to be living with the infection [9, 10]. The long-term consequences of the infection are also reported to account for 42.9% of liver cirrhosis in the country [9, 11], resulting in the high prevalence of chronic liver disease and liver cancer [8].
Nationally, HBV prevalence is estimated at 11-12.3% of seropositivity, arrived at using prevalence among blood donors and pregnant women [8, 12]. Across the country, HBV infection is reportedly highest in persons within the age group 16-39 years [8, 12], which emphasises the importance of this study as the majority of teenagers who are in high school fall within this age bracket.
The virus has multiple modes of transmission, including contact with the blood or other body fluids of an infected person [13]. In other words, when blood, semen, or another body fluid from a person infected with the virus, enters the body of an uninfected person through sexual contact, sharing needles, syringes, or other drug-injection equipment; or from mother to baby at birth [14]. In highly endemic areas such as Ghana, hepatitis B is most commonly spread from mother to child at birth (perinatal transmission), or through horizontal transmission (exposure to infected blood), especially from an infected child to an uninfected child during the first five years of life. An additional transmission route for the rapid spread in Ghana is people with bleeding gums sharing a drink with others using the same cup [15].
In Ghana, several studies have been conducted on HBV, but they tend to focus on prevalence rates among some selected population groups or short screenings. Specifically, in the Volta Region, the setting of this study, researchers have also reported a high prevalence rate among pregnant women attending antenatal clinics with an HBsAg seroprevalence rate of 2.4% recorded [1] in one study. Another study tested socioeconomic factors, risky behaviours, knowledge and awareness of HBV infection correlated with actual HBV status among antenatal clinic attendees and concluded that age, religion, ethnicity, educational level, blood transfusion, number of blood transfusions, gravidity, parity, awareness of HBV and monthly income were associated with HBV status [16]. Few studies on HBV in Ghana have examined knowledge, attitudes and vaccination status in relation to HBV. Yet, the knowledge of HBV status enables patients to seek early treatment, facilitates referral for social support and counselling [16]. A search of the literature found no evidence of a study among the specific population group of high school students in the region and the districts. The only study assessing knowledge, vaccination status, perceptions or attitudes found in the region was conducted among nursing trainee students at the Ho Nursing Training School, where researchers reported a satisfactory knowledge and vaccination status but poor attitude among the trainee nurses towards the disease [17]. This study sought to extend the literature by assessing an urban high school students’ knowledge of the hepatitis B virus so as to determine their perceptions, attitude, risk of infection and vaccination status.
2. METHODS
2.1. Design and Setting
We adopted a descriptive, quantitative cross-sectional design, which used standardised, closed-ended questions with few open-ended respondents self-administered questionnaires to survey knowledge, attitudes as well as vaccination status of Senior High School (SHS) students regarding the HBV virus. The questionnaire captured questions on knowledge, attitude and vaccination status of the virus. Knowledge was defined to include awareness, modes and routes of transmission and spread, and information sources about the disease. The knowledge items and sources about the disease are shown in Figs. (1a and 1b), in the results section of the paper. A good attitude in this study was defined to include having a positive disposition about the disease, which are illustrated in Figs. (2a and 2b) in the results section.
The study was conducted in the Hohe Municipality-a Peri-urban area, and one of the 26 administrative districts of the Volta Region of Ghana. Hohoe Municipality has six (6) Senior High Schools-four (4) public and two (2) technical schools. Two (2) schools were randomly selected.
2.2. Sample Size Determination
The sample size was determined using the formula below.
(A). n = (Zα/2)2 P (1-P) / e2 (Degu & Tessema.,2005)
The calculation was done as follows:
*Definition of terms or parameters in the formulae;
♦ n= Sample size to be determined
♦ Zα/2 = Z score (reliability coefficient) of 1.96 at 95% Confidence level
♦ P = Proportion of students’ knowledge on HBV according to Chireh (2011), is 82.5%
♦ e = represents margin of error of 5% = 0.05
♦ A non-response rate of 10% was added
Substituting the figures above gives:
n = (Zα/2)2 P (1-P) / e2
 |
n= 221.8524 ≈ 222
Non -response rate of 10% = (10A÷100) A-222
= 22.2 ≈ 22
Therefore, 222+22 =244
Hence, a sample size of 244 students was enrolled for the study.
2.3. Sampling Method
Two schools were randomly selected from the list of senior high schools in the Hohoe municipality by writing down the names of the schools on pieces of paper in a container. The container was shaken to properly mix the pieces of paper. The stratified sampling technique was employed in grouping the students into three strata according to their year of study (1, 2 & 3). A list/roll of all the students in the selected schools was obtained, which was used as a sampling frame. Respondents were selected according to their years of study. Year one consisted of a total of 393 students out of which, 110 students were selected; year two had a total of 189 students, of which 53 were selected; and the 3rd year had a total of 315 students, of which 88 were selected all based on simple proportion. After a proportional stratification, a simple random sample was obtained by placing all the numbers, corresponding to the name list in a container and selecting the stipulated sample size from respondents who met the expressed qualification criteria, which ensured a fair distribution for all levels to participate in the study. 250 students were sampled from the two selected senior high schools in the Hohoe municipality, but 244 students were selected based on the sample size calculation we used above. Of the two schools, one was rural and the other semi-urban.
2.4. Data Collection Procedure
Data for the study were collected through a self-administered questionnaire on the school premises. The questionnaire was written in the English Language.
2.5. Data Management and Analysis
Data collected were compiled and entered into a database using Epi Data 3.1., where data cleaning and validation was done. The analysis was carried out using STATA version 12.0. In addition, collected and compiled data were tabulated using Microsoft Excel. A Chi-square test was used to find the association between sociodemographic variables and knowledge level and attitude. The simple frequency was conducted on the data to determine the knowledge on causes, signs and symptoms, attitude and vaccination status. A test of the p-value of less than 5% level of significance was considered statistically significant.
3. LIMITATIONS
The findings of the current study should be interpreted in light of the fact that only two senior high schools were included, and the study covered only one municipality in the region. Thus, the results of this study may only be generalized to similar populations of students.
4. RESULTS
The key findings of the study are presented below in eight sub-headings. These include demographic characteristics of respondents; level of respondents’ knowledge on Hepatitis B virus infection; respondents’ perception of Hepatitis B infection; respondents’ attitude towards Hepatitis B virus infection; the vaccination status of respondents; association between sociodemographic characteristics and knowledge, and attitude of respondents respectively.
4.1. Sample Characteristics
Of the 251 student participants sampled, 127 (50.6%) were males and 124 (49.4%) were females. The mean age of the study respondents was 18.20 years and the standard deviation was (SD =1.621) with a minimum age of 14 and a maximum of 25 years. Majority of respondents in the sample identified as Christians, 245 (97.6%) and slightly smaller number 6 (2.4%) identified as Muslims. Ewes presented as the predominant ethnic group in the area with 189 (75.3%), followed by Akans 24 (9.6%). This is explained by the fact that the Ewes are the indigenous ethnic group of the Volta Region. The majority of the respondents 109 (43.4%) were in their first year, followed by third-year 88 (35.1%) and the second year 53 (21.1%), respectively Table (1).
| Variables | Frequency | Percentage (%) |
|---|---|---|
| Age | - | - |
| 11-14 | 2 | 0.8 |
| 15-18 | 161 | 64.1 |
| 19-25 | 88 | 35.1 |
| Gender | - | - |
| Male | 127 | 50.6 |
| Female | 124 | 49.4 |
| Year of study | - | - |
| 1st Year | 110 | 43.8 |
| 2nd Year | 53 | 21.1 |
| 3rd Year | 88 | 35.1 |
| Religion | - | - |
| Christian | 245 | 97.6 |
| Islamic | 6 | 2.4 |
| Traditional | 0 | 0 |
| Ethnicity | - | - |
| Akan | 24 | 9.6 |
| Ewe | 189 | 75.3 |
| Guan | 19 | 7.6 |
| Ga | 7 | 2.8 |
| Others | 12 | 4.8 |
| Parent Highest Educational Level | - | - |
| Basic | 50 | 19.9 |
| Secondary | 121 | 48.2 |
| Tertiary | 58 | 23.1 |
| No education Missing values |
8 14 |
3.2 5.6 |
4.2. Level of Knowledge on Hepatitis B
When we examined our analytical sample in relation to the level of knowledge variable, which featured nine questions on the routes and modes of transmission of the HBV, we found levels of knowledge ranged from moderate to high. This was arrived on the basis of participants selecting a number of correct answers in the respondents’ self-administered questionnaire, which determined how much knowledge the participant possessed about the hepatitis B virus, as shown in Table 2.
4.3. Awareness and Perception of the Hepatitis B Virus Infection
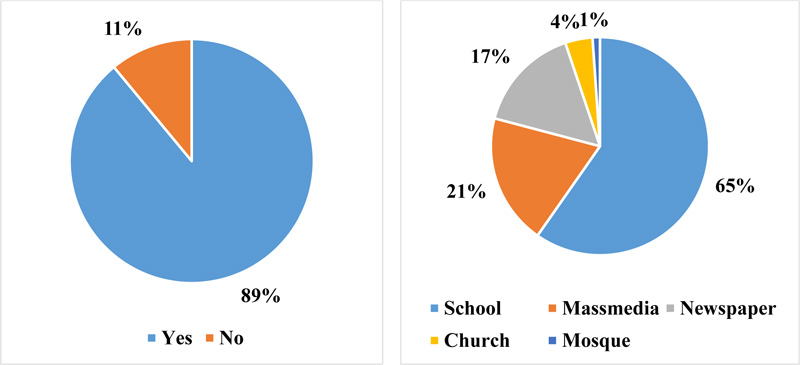
Since comprehensive knowledge is critical to mitigating the high risk of HBV infection, especially among teenagers and young adults of which students are part, we further assess respondents’ awareness and perception of the disease based on four questions, which are illustrated in Figs. (1a and 1b) and Table 3 respectively.
| Knowledge Items | Number Reporting the Correct Responses (Frequency) | Percentage (%) |
|---|---|---|
| HBV can be transmitted by sexual intercourse (Yes) | 123 | 49.0 |
| HBVcan be transmitted from mother to child (Yes) | 163 | 64.9 |
| HBV can be transmitted by sharing needle or syringe (Yes) | 123 | 49.0 |
| HBV can be transmitted by blood transfusion (Yes) | 191 | 76.1 |
| HBV can be transmitted by shaking hands (No) | 146 | 58.2 |
| HBV can be transmitted by wearing the same clothes with an HBV-positive person (Yes) | 124 | 49.4 |
| HBV can be transmitted through a mosquito bite (No) | 151 | 60.2 |
| Does HBV have signs and symptoms (Yes) | 184 | 73.3 |
| Does HBV cause liver cancer (Yes) | 129 | 51.4 |
| Can healthy-looking HBV positive person spread HBV(Yes) | 157 | 62.5 |
| Perception | Number Reporting Correct Responses (Frequency) | Percentage (%) |
|---|---|---|
| Is there effective treatment for HBV? (Yes) Can regular exercise and eating healthy food can Prevent HBV (No) |
187 163 |
74.5 64.9 |
The figures above showed a majority of respondents, 224 (89.2%) had heard of HBV infection with a slightly smaller number, 27 (10.8%) reporting of not having heard of hepatitis B before while 163 (64.9%) of the respondents mentioned schools as the main source of information.
From the table, only 35 (13.9%) of the respondents knew that there is no effective treatment of Hepatitis B Virus infection. This is of great concern as by this, the majority of the participants demonstrated a high level of misconceptions about the hepatitis B virus treatment. This has the potential of affecting screening and early diagnosis and treatment. The misconception, notwithstanding, further analysis revealed that more than half of the respondents, 163 (64.9%) answered correctly that exercising regularly and eating healthy food cannot prevent Hepatitis B Virus infection, which showed a high level of knowledge and positive perception about HBV.
4.4. Attitude and Practices towards Hepatitis B Virus Infection
A key objective of the study was to evaluate the attitude and practices of the students towards the HBV. In order to this, we designed five questions, the responses of which are presented in the Table 4.
| Attitudes and Practice Items/questions | Frequency |
Percentage (%) |
|---|---|---|
| Do you know if healthy people need vaccination? (Yes) Would you continue friendship with a person who has Hepatitis B? (Yes) Should HBV positive students be allowed in schools?(Yes) Do you need vaccination at your age? (Yes) Will you be willing to be tested for HBV infection? (Yes) |
167 124 136 167 197 |
66.5 49.4 54.2 66.5 78.5 |
The table shows that 167 (66.5%) of the respondents believe that even healthy people need vaccination against HBV, and 167 (66.5%) of them thought that people of their own age needed vaccination. Less than half of the respondents, 124 (49.4) agreed that they would continue a friendship with HBV positive friends. Slightly more than half of the respondents, 136 (54.2%) agreed to the question that HBV positive individuals should be allowed in schools, while 197 (78.5) of the respondents indicated that they were willing to be tested for Hepatitis B Virus infection.
4.5. Vaccination Status of Students
As part of the overarching goal of the study, we also sought to determine the vaccination status of the students since this is the major strategy for the prevention of the disease and mitigating the risk of infection and spread. The figures below are the responses of respondents.
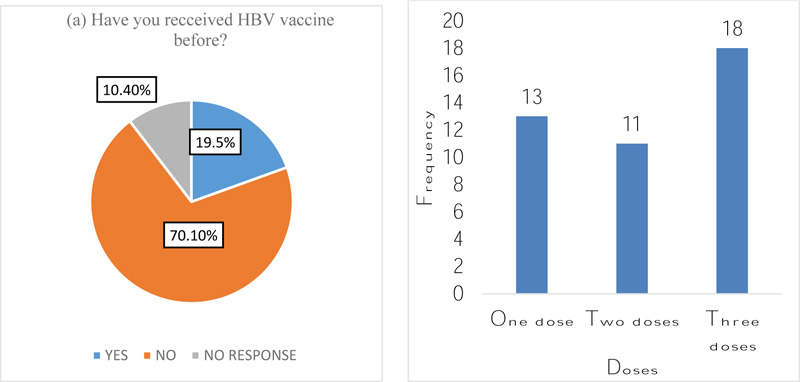
Analysis of respondent's answers revealed that 49(19.5%) had received the HBV vaccine, 176 (70.1%) answered they have never received any vaccine of HBV and 26 (10.4%) participants did not respond to the question as illustrated in Fig. (2a). Of those reporting to have received the vaccine before, 13 (5.2%) of them confirmed that they received just a dose of the vaccine, whilst 11 (4.4%) also said they received two doses of the vaccine. 18 (7.2%) showed they had received all three doses of the vaccine with the rest 13 (5.2) not responding to the question as illustrated in Fig. (2b). In our attempt to understand why they have not vaccinated, we asked further questions, as presented in the Table 5.
| Reason | Frequency |
Percentage (%) |
|---|---|---|
| I’m not at risk | 126 | 50.2 |
| I don’t believe in the vaccine | 40 | 15.9 |
| The vaccine is too costly | 57 | 22.7 |
4.6. Association between Sociodemographic Characteristics and Knowledge, and Attitude on Hepatitis B Virus Infection
We also wanted to find out if there was an association between the demographic variables and knowledge, risk of infection and attitude, the results of which are presented in the table below using Chi-square and P-Values.
Table 6 indicates that there was no association between sociodemographic characteristics and knowledge of the respondents as there were no statistical associations with P- values above (0.05). It is also apparent from the table that the majority of the sociodemographic characteristics variables had no statistical associations with the attitude and practice of students on HBV infection. The only year of study was strong enough to yield a statistically significant association with the attitude and practice of students with a chi-square value of (25.344) and P-value of (0.000).
|
Dependent variable (Level of knowledge) |
Independent Variables |
Chi- square (X2) |
P-value |
|---|---|---|---|
| Religion | 3.987 | 0.136 | |
| Year of study | 8.283 | 0.082 | |
| Ethnicity | 3.842 | 0.871 | |
| Parents’ educational level | 7.71 | 0.462 | |
| Age group Gender |
0.763 0.803 |
0.943 0.668 |
|
|
Attitude and perception of students on HBV infection |
Religion | 0.648 | 0.421 |
| Year of study | 25.344 | 0.000 | |
| Ethnicity | 3.743 | 0.442 | |
| Parents’ educational level | 6.542 | 0.162 | |
| Age group Gender |
1.085 3.089 |
0.581 0.079 |
In our attempt to further assess and determine the association between participants’ level of knowledge and attitude towards the HBV infection, we again computed the scores using Chi-square and P Values with additional variables comprising positive and negative attributes as shown in the Table 7.
| - | Attitude | |||
|---|---|---|---|---|
| Knowledge | Negative | Positive | Chi Square (X2) | P value |
| Low knowledge | 8(8.4%) | 13(10.1%) | 0.193 | 0.908 |
| Moderate knowledge | 57(60.0%) | 77(59.7%) | ||
| High/Comprehensive knowledge | 30(31.6%) | 39(30.2%) | ||
As the previous results, there was no statistical association between students’ knowledge and their attitude towards HBV infection, as this yielded a chi-square and p-value of 0.193 and 0.908, respectively.
5. DISCUSSION
Increasing knowledge about an infection can be a powerful means of fostering positive attitudes and building safe practices among populations. Exposure to body fluids such as sweat and sharing of personal belongings like clothing and other sharps objects remains a significant risk factor for contracting hepatitis B among confined populations such as students of secondary schools. It was revealed that the majority of the students 224 (89.2%) were aware of Hepatitis B infection, with major sources of information being the school, the mass media, newspapers, and religious institutions (church and mosque respectively). This is not surprising as the study participants were students of high schools. It also demonstrates that schools could be the channels for health education and promotion. On the other hand, the finding is an indication that religious institutions in Ghana need to play a more active and significant role in educating their members on emerging health issues.
Generally, 134 (53.4%) students had moderate knowledge about the infection as they scored correctly between 4 to 8 out of 10 questions presented on knowledge items. This is similar to a study conducted by Vu et al., where an average knowledge was recorded among more than half of 433 Vietnamese men in Australia [18]. Earlier studies in Ghana and other sub-Saharan African countries have reached similar conclusions. For instance, among 175 healthcare workers at Suntreso Government Hospital in the Ashanti region of Ghana, knowledge about HBV was moderate even among the healthcare workers [19]. Again, among 200 barbers in Obuasi in the Ashanti region of Ghana, 90.5% lacked knowledge about HBV [20]. In Nigeria, a study among 643 pregnant women found that 76% reported poor knowledge of HBV [21]. Studies in other parts of the world have reported a similar trend of poor to moderate knowledge [22].
Despite the general moderate knowledge exhibited about the infection, there were clear misconceptions about the HBV as 109 (43.3%) did not know the infection could be contracted through sexual intercourse; 68 (27.1%) did not also know the infection could be transmitted from mother to child. A further 107 (42.7%) did not know the infection could be transmitted through sharing needles and syringes. Even though the majority of the respondents knew the infection could be transmitted through unsafe blood transfusion, few 35 (13.9%) thought it was not possible, again highlighting the risk of infection. At the other end of the continuum, respondents had different misconceptions about the disease including that the infection could be transmitted through a handshake, 78 (31.1%); not knowing that wearing of clothing of an infected individual could foster transmission, 101 (40.2%); the belief that the infection could be transmitted through a mosquito bite 74 (29.5%); the infection not having signs and symptoms 41 (16.3%). Other misconceptions included respondents saying HBV could not cause liver cancer 96 (38.3%); and 68 (27.1%) thinking healthy-looking HBV patients could not transmit the infection. The various misconceptions and thoughts about the infection could have been because of the lack of sources to obtain knowledge about the infection that, in turn, increase their risk and exposure to infection.
In relation to treatment, 187 (74.5%) of the respondents knew that there is an efficient treatment of the Hepatitis B Virus infection. Some respondents, 145 (57.8%), also perceived that exercising regularly and eating healthy food could prevent Hepatitis B Virus infection.
The finding of the attitude towards the disease was more positive. A majority-167 (66.5%) indicated the need for healthy people to be vaccinated, with 124 (49.4%) expressing the desire to continue the friendship with a Hep B positively-diagnosed person. Again, 136 (54.2%) agreed that HBV positive students should be allowed in schools with 167 (66.5%) having the thought that people of their own age needed vaccination. Most of the students, 197 (78.5%) were also willing to be tested for Hepatitis B Virus infection. This finding agrees with results from a study, which recorded a positive attitude among the participants where more than half of them exhibited a positive attitude [23]. In this earlier study, out of the 354 participants, 309 (79.2%) were within the positive attitude range, whereas 81 (20.8%) showed a negative attitude range towards Hepatitis B [23].
Another important finding in this study related to the low vaccination coverage among this population group. Only 49 (19.5%) of the respondents reported receiving the vaccine, with less than half of the 18 (7.2) completing all 3 doses. Despite the moderate knowledge of the study participants 134 (53.4%) about the disease, and 167 (66.5%) identifying the need for healthy people to be vaccinated, the coverage was disappointingly low. This again highlights the dangers of infection as vaccination is one of the key methods of prevention. Reasons noted for not vaccinating included the belief that they were not at risk126 (50.2%); not believing in the vaccine 57 (22.7%); and cost 40 (15.9%). The significance of these is manifold. There is the need for more education and screening, and policy interventions that aim at making it more affordable or free for students in basic and secondary schools, especially those born before 2003 before hep B vaccination became part of the immunisation programme in Ghana. It must be noted, however, that similar low vaccination coverages were also recorded in studies carried out in Ethiopia and Nigeria where only 23 (9.3) participants reported being vaccinated against HBV among 246 participants [24], and only (46.6%) of participants who commenced HBV vaccine completed the 3-vaccine dose [25], respectively.
Factors that could have accounted for the low percentage of completing the HBV vaccine in the current study may probably be as a result of some respondents not due for the third HBV vaccine at the time of the study, some respondents not aware that HBV vaccine is given in three doses at given intervals of time or other circumstances.
From the results, there was no association between sociodemographic characteristics and knowledge of the respondents. Again, there was no association between sociodemographic characteristics and attitude except participants’ year of study, which was strong enough to yield an association, where good attitude and practice continuously decreased as the year of study of the participant increased. This could have happened by chance, as a good attitude is expected to be exhibited by participants as their knowledge about the infection increases. Yet, there was no association between participants’ knowledge and year of study.
CONCLUSION
The findings of the study showed that the majority of teenagers/senior high school students in the Hohoe municipality had moderate knowledge of HBV but had misconceptions about the infection that could negatively affect their attitude and perception and, in effect, impact their risk of infection and vaccination status. A clear understanding of knowledge and attitudes can be an important source of data to design intervention programmes and measures and public health policies. There is a need for further research nationally to inform policy on HBV in schools.
AUTHORS’ CONTRIBUTIONS
EKA conceptualized and designed the study, collected the data, and analysed it with JKA under the supervision of AF. EKA and JKA did the literature searches. Both EKA and JKA wrote the first draft of the manuscript. AF reviewed the first draft and offered suggestions. All authors read and approved the final manuscript.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for the study was granted by Dodowa Health Research Centre, Ghana with approval number DHRCIRB/18/05/17.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All patients participated on a voluntary basis and gave their informed consent.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We acknowledge the study participants, who agreed to take part in the study, the school authorities of the Senior High Schools selected, and the Municipal Directorate of Ghana Education Service for allowing us to undertake the study in the municipality.

