All published articles of this journal are available on ScienceDirect.

Determinants of First Aid Knowledge and Basic Practice Among Elementary School Teachers in Debre Tabor Town, Northcentral Ethiopia
Abstract
Background:
Pre-hospital school-based Emergency Medical Service (EMS) at school by school personnel is mandatory for saving the pupils from disability and death attributed to injury-related problems. Therefore, this study aimed to assess the determinant factors of first aid knowledge and basic practice among elementary school teachers in Debre Tabor, Ethiopia.
Methods:
Institution based cross-sectional study was employed in Debre Tabor among 216 elementary school teachers. A simple random sampling technique with proportional allocation was applied for the selection of the study participants. Data entry was done by Epi data version 3.1 and exported to SPSS version 21 for cleaning and analysis. Descriptive statistics was performed by using frequency, percentage, and table. Bivariable and multivariable logistic regressions were performed to determine the significance and strength of association at a 95% confidence interval. P-value <0.05 was considered as statistically significant.
Results and Discussion:
Our study revealed that 45.8% of study subjects were knowledgeable on first aid. More than 75% of study participants reported that they have encountered a child who needs first aid. Among these, 64% of them provide first aid. The multivariable analysis revealed that service year (AOR=3.51, 95%CI: (1.06, 11.59)), educational status (AOR=12.15, 95%CI: (3.17, 46.67)), previous first aid training (AOR=0.43, 95%CI: (0.21, 0.87)) and information about first aid (AOR=0.12, 95%CI ;(0.03, 0.48)) were found to be significantly associated with having knowledge on first aid.
Conclusion:
School teachers have low knowledge of first aid. Educational status, service year, previous first aid training and information on first aid were the predictors of first aid knowledge. Introducing essential first aid training in the curriculum during teachers’ training shall be considered.
1. INTRODUCTION
First-aid is commonly defined as the “immediate assistance given at the time of injury or sudden illness by a stander or other layperson before the arrival of expert medical aid” [1]. First aid is by no means a replacement for emergency services; it is a vital initial step for providing effective and immediate action that helps to reduce serious injuries and improve the chances of survival. Emergency services’ response time is very important since the likelihood of an injured person living or dying depends on the timeliness of life-saving measures [2].
Injuries are the major causes of morbidity and mortality in the world, especially in middle and low-income countries [3, 4]. Globally, in 2013, there were 973 million people who had sustained injuries, of which 77.9% had unintentional injuries that warranted some types of care [4]. Injuries among school-age children are common in developing countries, which account for 13% of all diseases pattern and disability [5]. Unintentional injuries are the leading causes of morbidity and mortality in pediatrics children [5, 6]. Childhood DALY (Disability Adjusted Life Year), attributed to injuries was higher in sub-Saharan African countries [5]. In Ethiopia, injuries caused 25 thousand deaths among 0-14-year olds and unintentional injuries accounted for the majority. The country longitudinal projection survey suggests that there will be 27,807 and 30,364 deaths due to injuries by the year 2020 and 2030, respectively [7].
School-age children are more likely to experience unintentional injuries in the school, while they are playing [8]. School teachers are the primarily responsible body for keeping the welfare of the pupils and oversee their activities. They are the first contact and responsible person when children face injuries [8]. However, studies showed that the level of knowledge and basic practice of first aid among school teachers were found to be poor [9-13]. Different studies were conducted among primary school teachers on first aid level of knowledge in Turkey, India, Bagdad, China, and Ethiopia, which showed that 55%, 74%, 77%, 96.3% and 60% respectively had poor knowledge of first aid management [9-12, 14]. Previous studies indicated that factors affecting the level of knowledge of first aid among elementary school teachers were: age of the participant, year of experience, having previous training on first aid, exposure to children in need for first aid, and level of education [9, 13, 15].
A study conducted in Ethiopia among kindergarten teachers, 80% of participants were encountered a child in need for first aid, but only 89.7% were given first aid [14]. In the country, schools have no nurses or physicians who will give first aid. However, pre-hospital school-based EMS at school by school personnel is mandatory for saving the pupils from disability and death attributed to injury-related problems [16]. Therefore, addressing knowledge and basic practice gaps of a school teacher on first aid is vital, especially at the elementary school level. To the best of researchers’ knowledge, school teachers’ knowledge and basic practice of first aid in Ethiopia, is not clearly known. Thus, this study is the first study in Ethiopia, which assesses the teachers’ knowledge and basic practice of first aid in elementary schools.
2. METHODS
2.1. Study Design and Study Population
An institution-based cross-sectional study design was employed in Debre Tabor Town elementary school teachers from April/2018-June/2018. Debre Tabor town is located 667 km from Addis Ababa (the capital city of Ethiopia) and 98 km far away from Bahir Dar (the capital city of Amhara regional state). Debre Tabor Town is the place where the first industrial village in Africa established with king Tewodros second at Gaffat. In the town, there are six government and six private elementary schools with a total of 422 teachers.
The source population was all elementary school teachers who are teaching in Debre Tabor Town. Whereas, randomly selected elementary school teachers were taken as the study population. A total of 216 elementary school teachers were selected by a simple random sampling method among the selected government and private schools proportionally.
2.2. Sample Size Determination and Data Collection Method
The sample size was performed by using a single population proportion formula by considering the following assumptions, Zα/2=1.96, p=0.4 (a study conducted in Addis Ababa among kindergarten teachers [14], d (margin of error) =5%. Moreover, a finite population correction formula was applied since the source population is < 10,000. Thus, the final sample size becomes 216 after adding a 10% non-response rate.
The data were collected by using pretested, structured, self-administer questionnaires, which were adapted from different literatures [9, 12, 14]. The questionnaire contains information about socio-demographic characteristics of the study participant, and first aid knowledge and basic practice assessment variables like; bleeding, fracture, epilepsy, human/animal bite, burning, epistaxis’s, choking, neck and back injury, fainting, swallowed poison, and breathing difficulties.
The questionnaire was prepared in English, then translated into Amharic (local language) and then back to English for consistency by the language experts. The hard copies of the questionnaire were distributed to the study participants to put their responses in a private setting after taking orientation and consent. Four facilitators and three supervisors were recruited for the data collection process. Facilitators were health officers, while supervisors were master holders public health experts.
2.3. Measurement
Knowledge of first aid was assessed by using 20 knowledge assessment questionnaires. The questions were yes/no questions which were designed to address emergency cases. The mean score of knowledge assessment questions was 11.6, with a minimum and maximum score of 0 and 20 points, respectively. The knowledge of the study participants was dichotomized as knowledgeable and not knowledgeable. Those who scored below the mean of the sum of knowledge questions were considered as not knowledgeable. Whereas, those who scored
2.4. Data Analysis and Processing
The data were coded and entered in a template prepared in Epi-data Version 3.1. Data cleaning and editing were performed by SPSS by running frequencies and cross-tabulations. Descriptive statistics were performed by using frequencies and percentages in a table. Bivariable and multivariable logistic regressions were done to identify the determinant factors of knowledge such as age, sex, types of school, educational status, service year, previous first aid training and information about first aid. Hosmer-Leme goodness of fit test was used to test the fitness of the model. Variables with a p-value of < 0.2 in the binary logistic regression were included in the multivariable model to single out the independent predictors of knowledge. The statistical significance declared at p< 0.05 with a 95% confidence level.
2.5. Ethical Approval
Ethical clearance was obtained from the Research Review Committee (REC) of the College of Health Sciences, Debre Tabor University. An official letter was written to the South Gondar education department. Written and verbal informed consent was obtained from all respondents who were participated in the study. The autonomy of the participants and the confidentiality of the information were maintained.
3. RESULTS
3.1. Socio-demographic Characteristics of the Study Participants
With regards to age distribution, 71 (32.9%) and 29 (13.4%), of the study participants were found between the ages of 25-29 and 30-34 years, respectively. The sex distribution of the study participants was almost proportional to 107(49.5%) and 109(50.5%) for males and females, respectively. More than half (137 (63.4%)) of the elementary school teachers were diploma holders. Only a third of the respondents, 76 (35.2%), were trained on first aid. With regard to information about first aid, 175 (81%) had heard about first aid. As per participants' self-report, health personnel was mentioned as a main source of information by, 121 (69.1%), the participants (Table 1).
3.2. Knowledge of Elementary School Teachers on First Aid
In this study, 35.2%(76), and 81%(175) of the participants took training on first aid and had information about first aid, respectively. Regarding first aid information sources, 21 (12%), 50 (28.6%)), 38 (21.7%), 121 (69.1%), and 82 (46.9%) were obtained from family, books, mass media, health personnel, and health facilities, respectively. Of the total study participants, 99 (45.8%) scored above the mean value of knowledge questions, which implies more than half of the study participants, 117 (54.2%) had no knowledge about first aid.
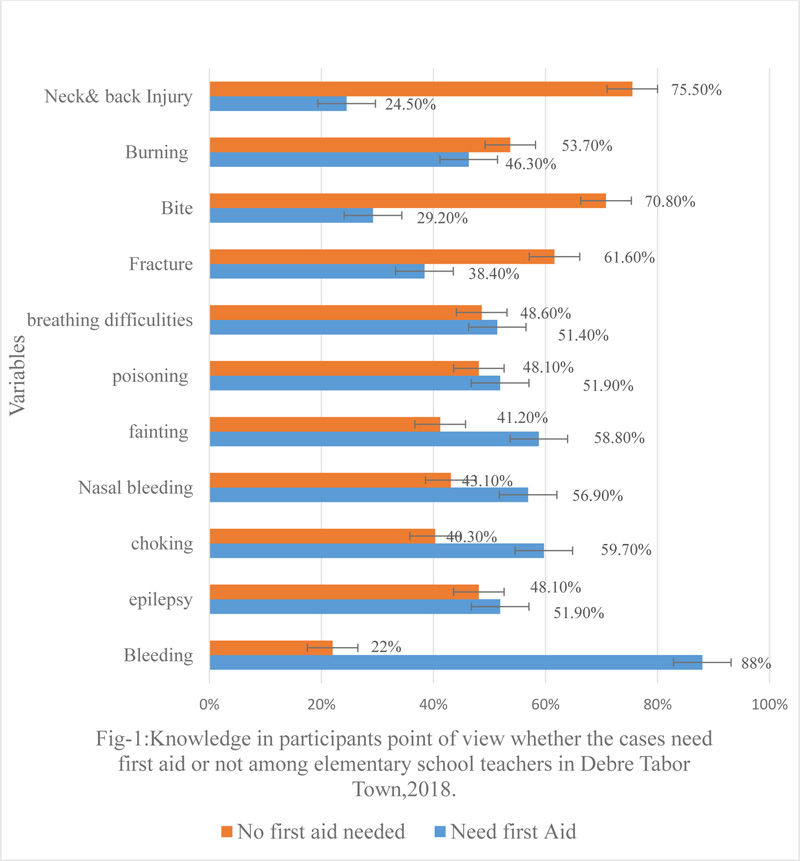
Based on the respondents' point of view, whether the cases need first aid or not, most of the respondents, 190 (88%), agreed on the needs for first aid in bleeding. Whereas, more than three fourth of the participants did not agree with the need for first aid for human/animal bite (Fig. 1).
Most of the respondents knew the correct measures against stopping bleeding 186(86.1%), followed by choking 147 (68.1%), epilepsy 133(61.6%), epistaxis/nose bleeding 154(71.3%), and breathing difficulty 145(67.1%).
| Variable | Frequency | Percent (n=216) (%) |
|---|---|---|
|
Age in years: 20-24 25-29 30-34 >34 |
47 71 29 69 |
21.8 32.9 13.4 31.9 |
|
Sex: Male Female |
107 109 |
49.5 50.5 |
|
Marital status: In union Not in union |
119 97 |
55.1 44.9 |
|
Education: Certificate Diploma Degree & above |
34 137 45 |
15.7 63.4 20.8 |
|
Service year: <5 5-10 >10 |
97 37 82 |
44.9 17.1 37.9 |
|
Type of school: Government Private |
133 83 |
61.6 38.4 |
3.3. Practices of Elementary School Teachers on First Aid
Table 2 reveals the practice of elementary school teachers on first aid. About seventy-five percent of teachers faced a child who needs first aid, among them, 158 (96.9%) of teachers tookan action. Of 158 teachers who took an action, 5 (3.1%), 52 (34.2%), and 101 (64%), calling ambulance, transfer the victim to a nearby health institution, and give an appropriate first aid, respectively. Seventy-six, (35.2%) of the study participants faced a child with the difficulty of breathing. Of whom the majority encouraged the victim to sit quietly 60 (79%), and breathe slowly and deeply, 49 (64.5%). With regard to fainting, more than one-third of the respondents, 84 (39.4%), had faced a child with fainting. The majority of the respondents, 64 (76.2%), reported as they put the victim on a flat surface. Epistaxis was another emergency case which was faced by 145 (67.1%) study participants. Of whom, 115 (79.3%) helped the child by encouraging them to sit comfortably with a slightly forward position as first aid measure. One hundred four, (48.1%) respondents faced body bleeding and most of them pressed firmly with a clean bandage to stop bleeding 87 (83.7%) (Table 2).
3.4. Factors Affecting Knowledge of Elementary School Teachers on First Aid
In this study, variables such as service year, previous training on first aid, education status and information about first aid were found to be significantly associated with knowledge in the multivariable model at 95% confidence interval. The odds of being knowledgeable on first aid were 3.5 times higher among elementary school teachers who had more than five years of experience compared with counterparts (AOR=3.51, 95%, CI: (1.06, 11.59)). Educational levels of the respondents were also found to affect first aid knowledge. Those degrees and above holders were 12 times more likely to be knowledgeable than those under degree levels (AOR= 12.15, 95%, CI, (3.17, 46.67)). Participants who have no previous training are less likely to be knowledgeable on first aid than those who had previous training on first aid (AOR=0.43, 95%CI: (0.21, 0.87)). The odds of being less knowledgeable on first aid found to be higher among participants who had no information about first aid (AOR=0.12, 95%CI ;(0.03, 0.48)) (Table 3).
| Variable | Frequency (No) | Percent (%) |
|---|---|---|
|
Faced a child within the need for first aid: Yes No |
163 53 |
75.5 24.5 |
|
Teacher took an action: Yes No |
158 5 |
96.7 3.3 |
|
Their first actions: Calling ambulance Transfer to the hospital Give appropriate first aid |
5 52 101 |
3.1 32.9 64.0 |
|
Breathing difficulty: Yes No |
76 140 |
35.2 64.8 |
|
Measure for Breathing difficulty: Call ambulance Help to sit quietly Breath slowly/deeply Contact authority |
19 60 49 35 |
25.0 78.9 64.5 46.1 |
|
Child with fainting: Yes No |
85 131 |
39.4 60.6 |
|
Measures for fainting: Call ambulance Help to sit quietly Loosen clothes around Clear airway offer nothing per mouth Contact authority |
19 64 38 43 25 25 |
22.6 76.2 45.2 51.2 29.8 29.8 |
|
Epistaxis: Yes No |
145 71 |
67.1 32.9 |
|
Measures for epistaxis: Call ambulance Help to Sit slightly forward Laid on the side by a pillow Apply pressure on a nostril Apply ice on the nose |
22 115 59 68 64 |
15.2 79.3 40.7 46.9 44.1 |
|
Body Bleeding: Yes No |
104 112 |
48.1 51.9 |
|
Bleeding management: Call ambulance Bandage bleeding site Elevate bleeding part Bandage with no pressure with circulation Cover child with a blanket Contact school authority |
15 87 35 69 21 38 |
14.4 83.7 33.7 66.3 20.2 36.5 |
|
Epilepsy: Yes No |
94 122 |
43.5 56.5 |
|
Measures for Epilepsy mgt: Call ambulance Help to sleep on the floor Left free epileptic movement Move nearby objects to avoid injury Hold any drink/food per mouth Clear airway and placing the child on the side Report to parents/school authority |
17 61 56 59 50 37 29 |
18.1 64.9 59.6 62.8 53.2 39.4 30.9 |
|
Choking: Yes No |
100 116 |
46.3 53.7 |
|
Management of choking: Call ambulance Squeeze the child chest turning back chest compression until expel Contact responsible body |
18 79 76 24 |
18.4 80.6 77.6 24.5 |
| Variable | Knowledgeable No (%) |
Not knowledgeable No (%) |
COR (95% CI) | AOR (95% CI) |
|---|---|---|---|---|
|
Age in years: 20-24 25-29 30-34 >35 |
16 (16.2) 27 (27.3) 18 (18.2) 38 (38.4) |
31 (26.5) 44 (37.6) 11 (9.4) 31 (26.5) |
ref 1.19 (0.55, 2.57) 3.17 (1.21, 8.30) 2.38 (1.10, 5.12)* |
ref 0.64 (0.22, 1.81) 0.34 (0.07, 1.62) 0.41 (0.07, 2.45) |
|
Sex: Male Female |
55 (55.6) 44 (44.4) |
52 (44.4) 65 (55.6) |
ref 0.64 (0.37, 1.10) |
ref 0.83 (0.43, 1.62) |
|
Education: Certificate Diploma Degree & above |
5 (5.1) 60 (60.6) 34 (34.3) |
29 (24.8) 77 (65.8) 11 (9.4) |
ref 4.52 (1.65, 12.38) 17.93 (5.58,57.62)* |
ref 4.77 (1.42, 15.98) 12.15 (3.17,46.67)** |
|
Service year: <5 5-10 >10 |
27 (27.3) 24 (24.2) 48 (48.5) |
70 (59.8) 13 (11.1) 34 (29.1) |
ref 4.79 (2.13, 10.74) 3.66 (1.96, 684)* |
ref 3.51 (1.06,11.59)** 3.65 (0.76, 17.67) |
|
School ownership: Government Private |
56 (56.6) 43 (43.4) |
88 (75.2) 29 (24.8) |
ref 2.33 (1.31, 4.15)* |
ref 1.97 (0.92, 4.24) |
|
Previous training: Yes No |
50 (50.6) 49 (49.5) |
26 (22.2) 91 (77.8) |
ref 0.28 (0.16, 0.50)* |
ref 0.43 (0.21, 0.87)** |
|
Information about first aid: Yes No |
96 (97.0) 3 (3.0) |
79 (67.5) 38 (32.5) |
ref 0.07 (0.02, 0.22)* |
ref 0.12 (0.03, 0.48)** |
4. DISCUSSION
In the present study, less than half (n=99, 45.8%) of the study participants were knowledgeable about first aid. However, 64% (117) reported as they provide first aid at least once. Our finding indicated that study participants provide first aid measures without having detailed knowledge about the problem. The finding of our study is consistent with a study conducted among kindergarten teachers in Addis Ababa, Ethiopia [14], and a sample of elementary school teachers in Kayseri, Turkey [11]. Our finding was higher than a study conducted in Isparta, Turkey, among preschool teachers, which found only 15.5% of participants to have good knowledge of first aid [13]. The variations could be explained by variations in sample size in which the aforementioned studies were conducted among 110 teachers, unlike our study. Variation in measurement could also explain the discrepancy. The finding of our study is also higher than a study conducted in Baghdad, Iraq, among primary school teachers with regards to external bleeding and fracture [10]. This difference might be due to the variation of the number of trained staff on first aid, the accessibility of information, and variation in a school setup.
In this study, those participants who did not take any training on first aid were found to be less knowledgeable compared with those who had training on first aid. The finding suggests that training is an important strategy to increase the knowledge of school teachers on first aid. The finding of our study is consistent with previous studies conducted in Addis Ababa, Ethiopia [14], Shanghai, China [9], and Mangalore, South India [12]. Thus, basic and refreshment training on first aid shall be conducted to increase the knowledge of elementary school teachers on first aid.
With regards to information about first aid, eighty percent of the respondents have information about first aid in this study. The finding is in line with a study conducted in Mangalore, South India (74%) [12] but lower than the finding in Addis Ababa, which was 100%. The variation might be explained by variation in the level of awareness between study participants and the setting in which Addis Ababa is a more urbanized place than Debre Tabor [14]. Unlike the previous studies [11, 13, 18], our study participants’ main sources of information were health personnel and health facilities. In this study, those participants who did not have previous information about first aid were less likely to be knowledgeable than counterparts. A similar finding was reported in the study in Addis Ababa, Ethiopia, in which participants whose sources of information were a health professional or health institution were more likely knowledgeable than others [14].
Service year was found to be significantly associated with the level of knowledge about first aid. Consistent with a previous study [14], the multivariable logistic regression analysis revealed that the odds of being knowledgeable were found to be 3.5 times higher among teachers who had more than five years of experience compared to counterparts. This implies that people can learn from experience in addition to the chance of getting training on first aid and emergency medical care through time. The finding of our study revealed that special emphasis shall be given to newly employed teachers since experience plays its role in the acquisition of knowledge of first aid.
Our study showed that there is a significant association between educational status and their knowledge of first aid. Those diploma holder elementary school teachers were found to be more likely to be knowledgeable compared to certificates. Similarly, those who were degree and above were twelve times more likely to be knowledgeable than counterparts. The finding implies that, the higher the education level, the more likely to be knowledgeable of first aid. A similar finding was reported in the study conducted in Shanghai, China, among preschool teachers which found high knowledge about first aid among teachers who had attended college or more level of education [9]. This implies that educational status affects the level of understanding.
Regarding the basic practice, 163 (75.5%) of the study participants encountered a child who needs first aid, of whom only 64% (n=101) had provided emergency medical aid, 52 (34.2%), and 5 (3.1%) take measure by transferring the injured child to the hospital and calling ambulance respectively. The finding of our study showed that a third of elementary school teacher could not provide appropriate emergency first aid at a school level. Thus, special attention shall be given for improving the practice of elementary school teacher on first aid since unintentional injuries are common in a school setting. The finding of our study is consistent with the study in South India, which found 36.8% did not provide first aid for those in need, and the study in Mysore, India, reported 45.4% poor first aid practice among school teachers [19]. The finding of our study is not supported by the study in Addis Ababa, which found 89.7% of kindergarten teachers provide first aid for children in need [14]. Similarly, our finding is inconsistent with other studies in India, which reported 72%-84% of school teachers provided first aid [12, 20]. The discrepancy may be explained by the difference in availability of first aid room, first aid kit, and emergency drugs in a school setting.
This study shall be seen in consideration of the following limitations. Firstly, the study was conducted in one town, which might affect the generalizability and representativeness of the finding. Secondly, the cross-sectional study design was used, which may affect causal inference. Thirdly, there is a limited number of published papers in Ethiopia and developing countries, so only available literature were used.
CONCLUSION AND RECOMMENDATION
More than half of elementary school teachers did not have knowledge of first aid. Those with an education level of degree and above, having previous training on first aid, availability of information on first aid and work experience of 5 years and more were found to be more knowledgeable than counterparts. School administrators shall give due emphasis for the training of staff on first aid. Integrating first aid in teachers' training curricula shall be considered by the ministry of education.
LIST OF ABBREVIATIONS
| AOR | = Adjusted Odds Ratio |
| COR | = Crude Odds Ratio |
| EMS | = Emergency Medical Service |
| SPSS | = Statistical Package for Social Science |
| DALY | = Disability-Adjusted Life Year |
AUTHORS’ CONTRIBUTIONS
WT, MM, and CY have contributed to the design, data entry, thesis write-up, manuscript development, and edition. The final manuscript is reviewed and approved by all the authors.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the research ethics committee of the College of Health Sciences, Debre Tabor University, Ethiopia Reference No.: CHS/2553/2018.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written and verbal informed consent was obtained from all respondents who were participated in the study. The autonomy of the participants and the confidentiality of the information were maintained.
AVAILABILITY OF DATA AND MATERIALS
The datasets used in this study are available from the corresponding author and can be accessible through reasonable requests.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the College of Health Science, Debre Tabor University for securing the ethical review process. The authors also want to express the deepest gratitude to supervisors, data collectors, and study participants.

