All published articles of this journal are available on ScienceDirect.

The Development of a New Understanding of Symptom Cluster During Pregnancy Using the Mediation Model
Abstract
Background:
Fatigue, depression and sleep disturbance are regarded as a symptom cluster associated with pregnancy. The mediation effect of sleep disturbance on the relationship between depression on fatigue is still unclear.
Objective:
To assess the mediation effect of sleep disturbance on the established relationship between depression and fatigue among pregnant women.
Methods:
This study used a cross-sectional design. Pregnant women (n = 130) at a private gynecology and obstetrics outpatient clinic in Amman, Jordan. Participants were recruited to complete the Brief Fatigue Inventory, the Insomnia Severity Index, and the Zung depression scale, in addition to the demographic questionnaire. The mediation effect was examined through a Hierarchal Multiple Regression model.
Results:
A total of 130 pregnant women participated (mean of ages= 27.3). Of those, 41.5% were in the first trimester, while the rest were in their second and the third trimesters (27.7%, and 30.8%, respectively). Regression analysis indicated that about 23% of the variation of fatigue was explained by depression. Nonetheless, 47% of the variance of fatigue was explained by depression after identifying the mediation effect of sleep disturbance.
Conclusion:
The mediation role of sleep disturbance between depression and fatigue added a new approach to the assessment and prognosis of fatigue during pregnancy.
1. INTRODUCTION AND BACKGROUND
A number of symptoms experienced by pregnant women affect their quality of life including their energy, appetite, and weight balance [1-3]. Fatigue scored the highest incidence among pregnant women of more than 90% [2, 4, 5]. Studies that examined symptoms experienced by pregnant women reported that fatigue is often associated with other symptoms such as sleep disturbances and depression [6-8]. The latter symptoms have recently gained greater popularity during pregnancy. Studies found that more than 75% of pregnant women complained of sleep disturbances [9-13]. Other studies revealed that more than 57% of pregnant women reported depression during pregnancy and in the postpartum period [5, 14]. In Jordan, minimal research attention has been given to the study of symptoms among Jordanian pregnant women. A previous study, nonetheless, reported that Jordanian pregnant women experience low social support and symptoms such as depression that interfere with life satisfaction [14].
The existence of these symptoms may warrant symptom cluster [5, 15-18]. Because the majority of the previous studies examined the incidence of each symptom individually, the association between these symptoms is still controversial. However, the relationship between fatigue, depression and sleep disturbances was identified in some other studies. For instance, a significant negative correlation was found between fatigue and sleep hours in which less sleeping hours were correlated with more fatigue [15, 17, 19-22]. Sleep disturbance was also correlated with depression across the three pregnancy trimesters [17, 23, 24]. However, inconsistent relationship was suggested between fatigue and depression among pregnant women, as one study confirmed this significant correlation (r=0.24, p=0.01) [22], while another rejected this supposition in late pregnancy and postpartum period [6]. Despite the existence of these associations, understanding the extent of how depression may influence fatigue, excluding the effect of sleep disturbances, is still not clear. The need for understanding these relationships within a conceptual model becomes a necessity.
The mediation model developed by Baron and Kenny [23] was previously used to explain the relationship between fatigue, depression, and sleep disturbance in cancer patients [24, 25]. Huang and Lin [25] found a complete mediated effect of depression between sleep disturbances and fatigue, as depression led to sleep disturbances which, in turn, led to fatigue. Similarly, Beck et al. [24] showed a partially mediated effect of sleep disturbances between pain and fatigue in which pain led to sleep disturbances that, in turn, led to fatigue. Thus, the mediation model can be employed to enhance a better understanding of how this symptom cluster interacts with each other and its impact on pregnant women.
The study aims to achieve the following objectives:
1. To examine the relationship between fatigue, depression, and sleep disturbance, on pregnant women in Jordan.
2. To explain the mediation effect of sleep disturbance on depression that induces fatigue in pregnancy.
2. METHODS
This study employed a cross-sectional correlational design through recruiting pregnant women from a private gynecology and obstetrics outpatient clinic located in Amman, Jordan. A non-probability convenient sampling technique was used to recruit the study sample. A pregnant woman was eligible to participate in the study if she was pregnant regardless of her trimester and able to read and write in Arabic. Women were excluded if they suffered from any comorbid disease such as diabetes mellitus, hypertension, heart failure, chronic kidney diseases, chronic obstructive pulmonary disease, asthma and migraine. Women who had the psychiatric disease were also excluded from the study. All previous illnesses had to be declared in the informed consents and the researchers had to be assured that none of the participants had a disease that may induce fatigue or sleep disturbances. The preliminary sample size calculation revealed the need for at least 120 participants. However, 150 questionnaires were distributed.
2.1. Instruments
A self-administered questionnaire was used in this study and included a demographic sheet and four self-report instruments to assess the symptoms. Although the instruments are self-reported tools, they are valid and reliable tools that have been used widely in the literature to assess the symptoms in different clinical populations.
2.2. Demographic Part
This section contains questions about age, trimester, number of children, educational level, any health problems, and employment status.
2.3. The Brief Fatigue Inventory (BFI)
The BFI [26] is a self-report questionnaire that assesses the severity of fatigue and its interference with life in 9 items. The total BFI score ranges from 0 to 10, with a higher score indicating more fatigue and more fatigue interference with life [26]. The severity of fatigue can be obtained from the average of the first three items, while the interference with participants’ life is obtained from other items such as general activity, mood, walking ability, and relationships with others. Mendoza et al. [26] set up cut-off points for fatigue severity in two categories: a score of 0-6 indicating non-severe fatigue, and a score >7 indicating severe fatigue. The BFI demonstrated high internal consistency coefficient of 0.96, and good validity as supported by significant correlations with both the Functional Assessment of Cancer Therapy-Fatigue scale (r= -0.88, p<.001) and the Profile of Mood States-Vigor (r= -0.84, p<.001) [26]. Suleiman et al. [27] reported high internal consistency (α= 0.93) of the Arabic version of the BFI.
2.4. The Insomnia Severity Index (ISI)
The ISI [28] is a self-report questionnaire that assesses the severity of insomnia for the preceding two weeks. It consists of 9 items rated from 0 (not at all severe) to 4 (very severe) with the total score ranges from 0 to 28. Higher scores indicate greater insomnia severity. Morin [28] defined four categories of insomnia scores as follows: 0 to 7 indicating no clinically significant insomnia, 8 to 14 indicating subthreshold insomnia, 15 to 21 indicating moderate clinical insomnia, and 22 to 28 indicating severe clinical insomnia. Morin [28] reported that ISI had a high internal consistency of 0.88. The convergent validity of the ISI with sleep diary indicated significant correlations (0.32-0.91, p<.05) [29]. Good internal consistency (α=0.84) was also demonstrated in the Arabic version of the ISI [30].
2.5. The Zung Depression Scale (ZDS)
The ZDS [31] is a self-report tool that assesses depression for the previous week. This 20-item scale has a rating system of 5-point (0-4) and its total scores ranged from 0 to 80. A cut-off point for depression was established by the original authors as follows: 20-49 indicating a normal range, 50-59 indicating mild depression, 60-69 indicating moderate depression, and 70 and above indicating severe depression. The validity and reliability of the scale have been established [32]. Regarding the Arabic version of the ZDS, Kirkby et al. [33] reported a higher agreement with the original English versions as indicated by the kappa K measurement (0.65, CI: 0.57-0.73).
2.6. Procedure
Approval to conduct the study was granted by the manager of the clinic where the study was conducted. An IRB approval was obtained from Al-Zaytoonah University of Jordan. At the clinic waiting room, participants were invited directly by the researchers to participate in the study. Invitation to the study included a verbal description of the study's purpose, benefits, and participants’ rights. Participants were assured that their contribution was totally anonymous, voluntary, and confidential, in addition to the right to withdraw or participate. Eligible participants were informed to complete the questionnaires with signed consent. They were given a choice to complete the questionnaire during their current visit or take it home and return it back in their next visit. In the latter case, participants' contact information (i.e., telephone number) was required to allow for follow-up. The estimated time to complete the whole questionnaire was 15-30 minutes.
2.7. Data Analysis
The collected data were entered into the Statistical Package for Social Sciences software (SPSS) version 23. It was checked for missing and outliers through visualizing the frequency distributions of each variable and treated by re-checking the original papers. Descriptive statistics included frequencies, percentages, means, and standard deviations. Bivariate correlation coefficient was used to evaluate the relationship between symptoms. The mediation model developed as proposed by Baron and Kenny [23] was implemented to examine the effect of sleep disturbances on fatigue and depression using the Hierarchical Multiple Regression as follows:
1. Sleep disturbances (the mediator) is regressed on depression (the independent variable).
2. Fatigue (the dependent variable) is regressed on depression (the independent variable).
3. Fatigue (the dependent variable) is regressed on sleep disturbances (the mediator) and depression (the independent variable).
It was assumed that significant mediation occurs if depression (independent variable) has no effect (not significant) when the mediator (sleep disturbances) is controlled.
3. RESULTS
3.1. Participants Characteristics
Of the 150 questionnaires distributed, 130 returned their forms representing 86% response rate. Table 1 shows the demographic characteristics of the participants. The participants' average age was 27.33 years. Most of the participants (70.3%) held high school degrees, unemployed (86.2%), had kids (73.8%). While 41.5% of the participants were in their first trimester, the rest were in their second and third trimester (27.7% and 30.8%, respectively) (Table 1).
3.2. Fatigue, Depression and Sleep Disturbance Among Pregnant Women
Descriptive statistics of the three symptoms (fatigue, depression, and sleep disturbance) are as follows. The pregnant women reported an average BFI of 5.43 (SD= 1.92), indicating non-severe fatigue. The majority of the women (67.7%) had non-severe fatigue. The BFI severity mean score was 5.23, while the BFI interference mean score was 5.61 (SD= 2.44). The mean of the total ISI scores was 13.41 indicating sub-threshold insomnia. The mean of the total ZDS scores was 50.09 indicating mild depression (Table 2).
| Variable | Total (N= 130) | |
|---|---|---|
| Mean | SD | |
| Age | 27.33 | 5.93 |
| Number of kids | 2.64 | 0.97 |
| - | - | - |
| - | n | % |
| Have kids | - | - |
| Yes | 96 | 73.8 |
| No | 34 | 26.2 |
| Education | - | - |
| Secondary School | 90 | 70.3 |
| Primary education | 38 | 29.7 |
| Employment | - | - |
| Employed | 18 | 13.8 |
| Unemployed | 112 | 86.2 |
| Trimester | - | - |
| First | 54 | 41.5 |
| Second | 36 | 27.7 |
| Third | 40 | 30.8 |
3.3. Associations Between Symptoms
The Pearson correlations coefficient was used to evaluate the relationships between fatigue, depression, and sleep disturbance as shown in Table 2. A significant positive correlation was found between fatigue and depression, fatigue and sleep disturbances, and between depression and sleep disturbances. All correlations were statically significant at α: 0.01 and ranged from 0.48 to 0.68. (Table 3).
| Symptom | Mean | SD |
|---|---|---|
| Total BFI | 5.43 | 1.9 |
| Fatigue severity items total | 5.61 | 2.44 |
| Fatigue interference items total | 5.2 | 2.21 |
| Total ISI | 13.41 | 5.3 |
| Total ZDS | 50.09 | 7.3 |
| Symptom | BFI | ISI | ZDS |
|---|---|---|---|
| BFI | 1 | 0.68** | 0.48** |
| ISI | - | 1 | 0.59** |
| ZDS | - | - | 1 |
**p<0.01
3.4. The Mediation Effect of Sleep Disturbances
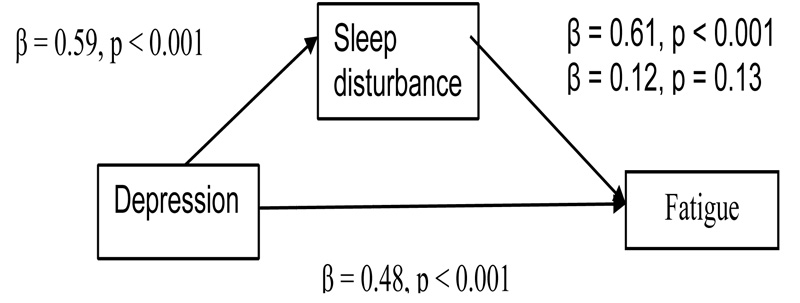
Based on the mediation steps mentioned earlier, the regression model is presented in Table 4. The first step was regressing sleep disturbances (the mediator) on depression (the independent variable). Results revealed a significant association between depression and sleep disturbances (β= 0.59, p< 0.001). The second step was regressing fatigue (the outcome variable) on sleep disturbances (the mediator). Results revealed a significant association between fatigue and sleep disturbances (β = 0.68, p< 0.001). The third step was regressing fatigue (the outcome variable) on depression (the independent variable). Results revealed a significant association between fatigue and depression (β = 0.48, p< 0.001). The final step was regressing fatigue on both depression (the independent variable) and sleep disturbances (the mediator). When sleep disturbance was controlled, this association between the dependent and the independent variable became no longer significant (β = 0.12, p= 0.13). Fig. (1) shows the mediation model of all symptoms based on the regression results. The results indicated that sleep disturbance completely mediated the effect of depression on fatigue. In other words, concurrent experience of depression, fatigue and sleep disturbances by pregnant women can be attributed to the effect of sleep disturbances that induce depression, which in turn, induces fatigue.
| Model | Variables | Adjusted R Square | SE | t test value | Standardized Coefficient | Sig* |
|---|---|---|---|---|---|---|
| Bata | ||||||
| Model 1 | Depression | 0.23 | 0.020 | 6.33 | 0.48 | <0.001 |
| Model 2 | Depression | 0.47 | 0.021 | 1.51 | 0.12 | 0.13 |
| Sleep disturbance | 0.29 | 7.71 | 0.61 | <0.001 |
*Significant value was drawn from the coefficients table indicating that the two models were statistically significant (Sig<0.001) in F change and ANOVA results.
4. DISCUSSION
Pregnancy induces many bothersome symptoms as experienced by pregnant women. Fatigue, depression and sleep disturbance are commonly reported symptoms associated with pregnancy. The experience of pregnant women of more than one symptom together may be explained by the sickness behavior model which suggests that the difference in symptom experiences by pregnant women may result from the woman ability to respond to physical and psychological stressors exhibited as symptoms through changes in pro-and-anti-inflammatory cytokines during pregnancy period [34]. The results of this study can also be explained by the idea that getting married and pregnant may induce a big change in the social class of the woman. Specifically, the pregnant woman transitioning from one social class to another is likely to generate status-based identity uncertainty, helplessness, and lack of freedom. This uncertainty increases the woman’s allostatic load and induces a range of negative physical health outcomes [35]. Allostatic load theory may explain the stressors that pregnant women may experience and how to accommodate them [36]. Symptom cluster experience during pregnancy may be examined as a stressor that affects the women’s social life. During marriage, women may move from one social class to another which may induce stressors that are exhibited as a cluster of symptoms affecting their quality of life [37].
The current study investigated three common symptoms of pregnancy (fatigue, depression and sleep disturbances altogether) from within the Jordanian context. The study supports previous evidence about the influence of one symptom on the others. However, integrating these three symptoms has not been studied before in pregnant women, especially when the implementation of a mediation model is integrated. The results found strong correlations between fatigue, depression and sleep disturbances and confirmed that sleep disturbances had a significant mediation effect on depression which, in turn, induces fatigue.
In the current study, the pregnant women in all pregnancy trimesters revealed a significant relationship between fatigue and depression. Although a previous study found a weak relationship between fatigue and depression in 113 pregnant women in the early pregnancy period [22], pregnant women in the majority of studies experience more fatigue and depression levels while advancing in the pregnancy trimesters [6]. The current study also reported a strong correlation between fatigue and sleep disturbances. This conforms to a previous study conducted on 650 pregnant women and indicated a significant negative relationship between sleeping hours and fatigue [19]. Another study by Tsai et al. [7] found that naps were significantly associated with fatigue, suggesting that longer sleeping was associated with less fatigue. It was evident that depression in the current study was strongly correlated with sleep disturbance. This result is consistent with Reshadat et al. [16], who also suggested a higher correlation (r=0.48). Similarly, Shariat et al. [17] who used Cramer's correlation coefficient to examine the relationship between sleep disturbance and depression, found that depression was significantly correlated with sleep quality in all pregnancy trimesters. Further, another study by Nylen et al. [38] confirmed the relationship between depression and sleep disturbances among pregnant women which are in line with the findings of the current study.
The mediation effect of sleep disturbance indicated that depression could directly affect fatigue, but its impact can be influenced by sleep disturbances. The direct effect of depression on fatigue, however, became insignificant when the role of sleep disturbance was added to the model. Thus, the effect of depression on fatigue should not be justified without understanding the effect of sleep disturbances. This suggests that both depression and sleep disturbances can affect each other and trigger fatigue. Therefore, sleep disturbance plays a pivotal role in both depression and fatigue among pregnant women. The results of this mediation model are consistent with previous studies that reported a positive relationship between the three symptoms of which sleep disturbance had the most substantial contribution to fatigue development [25]. Since the three symptoms may need to be managed simultaneously, discovering the impact of one symptom on the others may expedite the effectiveness of the therapeutic management and mitigate the complexity resulting from using various modalities in those delicate individuals.
4.1. Application to Nursing
Symptom cluster indicates that symptoms may occur simultaneously with other symptoms and consequently interact with each other; that is, two or more symptoms may occur at the same time and serve as catalysts for each other. Pregnant women experience more than one symptom, such as fatigue, depression and sleep disturbances. For example, fatigue seems considerably worse when pregnant women also have depression or sleep disturbances.
The results of this study provide basic information for nurses and midwives regarding symptom experience among pregnant women in Jordan. Hence, nurses and midwives should monitor pregnant women who demonstrate fatigue and depression which may affect the women's quality of life. Nurses may adopt standard assessment tools to assess the symptoms and reduce the women's symptoms experience by implementing counseling or strategies such as sole reflexology [3]. Nursing administrators could also develop and implement continuing education programs about symptom management to improve sleep quality and decrease fatigue and depression levels to improve the quality of life among pregnant women.
Understanding the relationship among these symptoms will provide direction to future intervention studies to know which symptom to focus on specifically in a symptom-management intervention. According to the results of this study, a complete mediation relationship of sleep disturbances on the relationship between fatigue and depression is shown to exist. In Jordan, there is a lack of research related to symptoms management among pregnant women. More research is needed to fill this gap. The current study may serve as a baseline for further studies in the Jordanian context. Given the centrality of pregnant women, as well as the role of sleep effect on fatigue and depression relationship in the management of symptoms among pregnant women in Jordan, future researchers may conduct interventional studies using behavioral therapies to reduce sleep disturbances and consequently reduce fatigue and depression levels.
5. LIMITATIONS
*The current study implemented a cross-sectional design which is carried out at a one-time point and does not allow for inferences over time, so the results cannot be generalized unlike that of a longitudinal design. With cross-sectional design, it is not possible to establish a true cause and effect relationship in longitudinal studies considering several demographic and sociocultural variations.
*The current study implemented a non-probability convenience sample. The sample was pulled out from pregnant women who were willing to participate in the study. Voluntary participation meant that it was possible that pregnant women who did not choose to participate differed from those who did participate. The voluntary sampling methodology may limit the generalizability of the findings.
*The important role of hormones on pregnant women and the influence of hormones such as HCG, E2, PRL on depression and fatigue was not assessed through this study as thus, the current study recommends examining these important variables in the future research.
*Further, this study has been conducted in a single setting with minimal variation with respect to socioeconomic and cultural properties. Future research is encouraged to evaluate the impact of other important factors such as women’s husbands, family members, economical situation, hygiene factors, and security on symptom experience among pregnant women.
*Future studies should also develop a unique framework of symptom cluster for each individual trimester rather than generating inferences to the whole pregnancy period.
CONCLUSION
Symptom cluster is an imminent phenomenon experienced by pregnant women. Fatigue, depression and sleep disturbances are common symptoms that should not be understood or treated as discrete, individual, separate symptoms. Rather, each individual symptom has a unique contribution to the other symptoms, something that should be clinically undertaken. The mediation role of sleep disturbance between depression and fatigue added a new approach to the assessment and prognosis of fatigue during pregnancy. Depression, which is viewed as one of the main precursors for fatigue, can be heavily influenced by sleep disturbance. Therefore, surveying sleep disturbances can be an integral part of the routine pregnancy follow-ups, and its impact should be investigated further in future prospective studies.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
An IRB approval was obtained from Al-Zaytoonah University of Jordan (IRB approval number is 2017-2016/602/11).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All patients participated on a voluntary basis and gave their informed consent.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
None
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge Dr Mustafa Harb for his guidance and advice.

