All published articles of this journal are available on ScienceDirect.

Educating to Say ‘no’ to Reject High-Risk Suggestions Through Roleplaying Model Among Middle School Students
Abstract
Background:
As the adolescents lack necessary social and communicational skills, the present study aimed to educate to say ‘no’ to reject high-risk suggestions through the use of role play model.
Methods:
In a field trial, 145 female students using randomized sampling were selected in Arak. The checklist made for saying ‘no’ was completed before, immediately and two months after the intervention for students. The study was conducted based on the skill of saying ‘no’ through role-play training method. Data were analyzed by descriptive and inferential statistical tests through SPSS.
Results:
The mean scores of skills of saying ‘no’ to reject high risk suggestions showed a significant difference among the subjects before, immediately and two months after intervention (respectively p=0.000, p=0.009)
Conclusion:
The results indicate that the educational interventions of preventive behaviors are necessary for students to improve their skill of saying ‘no’.
1. INTRODUCTION
Investigations show that nearly half of the world's population is composed of teenagers. About 1.5 billion people in the world were in the age range of 10-25 years by 2009 [1]. In Iran, 27% of the population, i.e., about 16 million, are adolescents. When people reach puberty, essential and important changes emerge in their appearance, social behaviors, and psychosocial status, with many healthy habits and behaviors forming at this stage of life and having a significant impact on adult health behaviors [2]. Unsuccessful marriages, high-risk pregnancies, deaths, unhealthy habits and behaviors are rooted in this period. In the world, adolescents are not adequately protected against AIDS, sexually transmitted diseases and pregnancy, and are exposed to unhealthy and unprotected sexual relationships, drug abuse, sex without responsibility, early pregnancy, violence, failure in the course and school and so forth. In Iran, most cases of high-risk sexual behavior (55.6%) occur at the age of 16-21. The average age for starting to smoke in Iran is 16.6 years, and the highest proportion of drug addicts (45.7%) begins from the age of 17-22 years old [3]. Moreover, the average age of the first sexual contact is 14 years, as quoted by Rahmani from Mohammadi, and Soleimani Nia reported a 44.7% prevalence of high-risk behaviors [4]. The vulnerability of females, however, makes this period more sensitive for females [5]. In many countries, pregnancy during adolescence is considered as a risk factor with high rates of embryonic and maternal complications [6]. Every year, an estimated 21 million girls aged 15-19 years and 2 million girls aged under 15 years become pregnant in developing regions. Approximately 16 million girls aged 15- 19 years and 2.5 million girls under the age of 16 years give birth in developing regions. Complications during pregnancy and childbirth are the leading cause of death for 15 to 19-year-old girls in the world. Every year, some 3.9 million females aged 15-19 years undergo unsafe abortions. Adolescent mothers (ages 10 to 19 years) face higher risks of eclampsia, puerperal endometritis, and systemic infections than women aged 20 to 24 years [7]. Another challenge that adolescents face is risky behaviors and a lack of life skills. In this regard, various studies show that there is a relationship between lack of social skills with behavioral disorders and risky behaviors in the future such as delinquency, defect in academic and cognitive function, escape from school in childhood and alcoholism, anti-social behaviors and mental disorders. The absence of social skills causes several problems for children and adolescents and leads to the lack of reconciliation and compromise in interpersonal relationships, behavioral problems and disorders, which negatively affects the development of personality and adaptation to the environment [8]. A deficit in social skills leads to high-risk behaviors. Based on the results, there was a moderate inverse relationship between social skills and high-risk behaviors. People who have social skills are able to present appropriate and rational reactions in different situations, avoiding behaviors that are dangerous with harmful consequences. Education of social skills helps at-risk youth to develop techniques for creating or maintaining positive social relationships with family members, peers, and teachers. Social skills training can have long-term effects associated with preventing anti-social behaviors among young people. Thus, considering this category of skills can be effective in reducing high-risk behaviors [2]. Therefore, adolescents need to be trained before and during puberty [9].Vorobjov showed that students’ social skill levels were related to their licit and illicit drug use. A low level of social skills can increase adolescents’ vulnerability to drug abuse. Vorobjov suggested that gender-related risk prevention programs of social skills training could be beneficial in preventing drug use [10]. Bagheri showed that training programs which make people aware of drug abuse complications would reduce the demand and inclination for drugs, especially among the youth [11]. Babazadeh showed that after the training, significant changes in the mean scores of knowledge, attitude and behavior were observed in the intervention group. Knowledge and attitude were able to predict 41% of changes in behavioral intention and concluded that education could be effective in interventions to increase knowledge, improving attitude and behavioral intention about HIV preventive behaviors [12]. Studies show that life skills training has a satisfactory effect on the prevention and treatment of health problems and that social skills training affects all components of psychological capital (resilience, hope, optimism and self-efficacy), which improves students' psychological capital [13]. According to the results of these studies, teaching life skills to adolescents increases their personal and social adequacy, and the possibility of prevention is provided by social skills training to reduce the vulnerability of social interactions and cause resistance against group pressures so that saying ‘no’ is possible when necessary and adolescents are able to identify and withstand risky situations [14]. Hence, the acquisition of venture, which is characterized by autonomy, self-orientation, the tendency to peers, as well as relieving the stresses of growth that make teenagers more vulnerable to health-threatening factors, is of vital importance. This skill gives them the feeling of self-efficacy so that trust is made in their relationships with others. The adolescent who has learned to say ‘no’ or has acquired venture would more probably make positive choices and avoid engaging in high-risk behaviors [15]. Therefore, the most effective training programs should be applied to express this venture and reject risky suggestions in adolescents [16, 17]. Role-playing is a training method of expressing existence and a venture [18], which is known as one of the approaches for group therapy. Nowadays, role-playing has found various applications such as being a tool for emotional evacuation, a way to change attitudes, an approach to create insight into references and to teach new behaviors [19]. Role-playing is an approach through which the therapist asks the patient to behave in a situation within a treatment or practice room that is simulated with a real-life situation. In this simulated situation, the client and the therapist perform interpersonal interaction related to the problem of the patient [20]. In this regard, the results of the study by Bahri showed that training venture with group counseling (role-playing) method was effective on the self-esteem of female students compared to the non-trained control group [21]. On the other hand, according to studies conducted by many countries in the world, adolescent girls do not receive timely official education on health issues [22-24]. According to the fact that adolescents do not have the necessary social-relationship skills, they tend to be independent, have an inclination toward friends, and are exposed to risky behaviors and situations in their socialization and identification, and scholars have attempted to conduct a research aimed to educate the skill of saying “"no"” to reject risky suggestions using role-playing in students. It is hoped that this is a step to furnish students with preventive behaviors.
2. METHODS
This is a field trial study with pre-test and post-test, which was conducted in three stages on two groups (intervention and control) of female secondary school students living in Arak (Markazi Province of Iran). The research samples (63 per group) were systematically and randomly selected, and given the loss of samples, 10 individuals were added. The inclusion criteria were as follows: secondary female students, studying in state-run schools, having a willingness to participate in the research, signing the consent form by both students and their parents, enjoying physical and mental health based on the records available at the school. Exclusion criteria included the reluctance to continue participating in the project, absence in more than one session of training sessions, transfer to other schools and any incidents increasing student’s stress. The data collection tool was a demographic questionnaire for research units (with such items as number of children, parental occupation, family income level, parent’s education, the death of a parent, having a stepparent, and parent’s divorce), and a checklist was developed for the skill of saying "no". This checklist included four questions with multiple-choice scale having two options (no/yes), in which 0 and 1 were assigned for "no" and yes, respectively. The checklist was designed to evaluate the role-playing of the student in three stages. The score range of saying "no" was 0-4.01 (0-1.33, weak; 1.34-2.67, middle; 2.68-4.01, good). The research method was as follows. Firstly, one district was randomly selected from the two education districts of Arak (by drawing lots). Out of 13 state-run schools for females, two schools were randomly selected (by drawing lots). After the presence of the researcher in the schools, students were systematically and randomly sampled from the school office. Subsequently, after explaining the objectives of research to students and filling the consent form for participation in the study by the students and their parents, the demographic information questionnaire was filled by them. Then, the harmful behaviors were introduced to each student by the researcher in one of the classrooms, and their verbal and non-verbal reactions were observed and scored by the researcher according to the saying "no" checklist. The same scenario with harmful behaviors was again conducted in the post-test and the two schools were randomly assigned to the intervention and control groups. Subsequently, the training was conducted by the researcher in the form of seven sessions of 1.5 hours and a maximum of three sessions per week at the praying room of the school. In the first session, the researcher explained the research goals to subjects. The contents of the training materials in this session were as follows: definition and concept of assertiveness, the necessity and importance of assertiveness skills in life, the description of ordinary and high-risk situations, explanation of the concept of assertive behavior, the difference of assertiveness with aggression and embarrassment, characteristics of the aggressive, shy, and assertive people. There are three types of assertive behaviors: 1) Assertive rejection (saying "no"); 2) Assertive statement; 3) Assertive suggestion. The advantages of assertive behaviors were discussed in the second session; the barrels to reject risky suggestions and associated solutions were dealt in the third session; and a quick review of the third session materials was conducted by the researcher in the fourth session. Subsequently, other barriers to the rejection of risky suggestions were summarized, and after removing probable mistakes and receiving feedback, the definition of self-awareness and its concept, the necessity and importance of self-awareness for self-confidence were described and adequate explanations were given in this regard. Then, for the more active intervention of the self-awareness form, a few students in each educational group (due to lack of time) were asked to answer the questions with the hot seat method and their feedbacks were evaluated using Q&A at the end of the session. The students were also requested to write questions about self-awareness and to think more about them at home, so that each student could better understand oneself (including abilities, disadvantages, feelings, values, responsibilities, needs, desires, goals, etc.). In the fifth session, the definition of self-confidence, its importance and necessity in life, the need for self-confidence, the relationship of self-confidence and assertiveness, ways to increase self-confidence, relationship between self-confidence and the skill of rejecting risky suggestions, benefits of having confidence and the disadvantages of lacking it, characteristics of individuals with confidence in high-risk situations, etc., were actively discussed with students. All training materials were provided using the lecture method, group discussion, question and answer, and brainstorming. In the sixth training session, besides receiving feedback and probable errors, the skill of saying "no" with its four components (saying “no”, saying “no” by sign language and physical movements, saying “no” by appropriate voice tone, repeating the message “no”) followed by the components of assertive behaviors including non-verbal factors, the way of expression, verbal factors and the word content, interacting factors, cognitive factors (thinking, beliefs, and subjectivities) were discussed in detail. The skill of saying "no" in this session was trained with the help of the school counselor who actively participated in all the sessions in the form of different scenarios for various situations with “role-playing and performing methods. Executed scenarios for the skill of saying "no" in ordinary situations included situations such as asking for renting a book by a friend from another friend on the test night when the owner of the book needed it himself, stimulating the student to a friend to mock their new colleague and so on. The high-risk scenario also included the stimulation of a student to another student for friendship with a boy (opposite sex), the suggestion of a friend to board an unknown person's car, the offer of invitation to an inappropriate party, suggesting the immoral internet sites, recommendation to go to quiet and strange places with strangers, accepting to eat something from an unknown person and so on. Afterward, according to the remaining time, students were requested to practice this skill in role-playing style in groups of 2, 3 or 4 individuals. In addition, in all scenarios, other students had to evaluate the performed scenario in terms of the four components of saying "no". They were also asked to practice this skill at least 20 times in reality or virtually at home until the next session, and if not, the researcher was not responsible. In the seventh session, the students executed the skill of saying "no" fully and effectively with all the four components using the role-playing method in groups of 2, 3 or 4 students. The rest of the students were asked to evaluate what they were seeing, strengthen their weaknesses and encourage their strengths so as to use the skills fully and effectively. Each student at least fulfilled the skill once at this session and was asked to run the skill in different situations of life as an assignment. Immediately and two months after the training, after fully reassuring the student, the researcher assuming to be a close friend of the student suggested a high-risk offer and requested the students to show her reaction for the rejection of high-risk offer, and the checklist of “saying "no" was filled by observing this skill that was performed as role-playing. The validity and reliability of the skill checklist of “saying "no" were previously evaluated by Ghaffari et al. through agreement method and Kappa statistical test, where the Kappa coefficient of the first component (saying the word "no") obtained the score 1; the second component (saying "no" by sign language and physical movements) 0.73; the third component (saying "no" with the appropriate voice tone) 0.81; and the fourth component (repeating "no"” message) scored 1, thus ensuring its reliability. In agreement method of Kappa, a number of students were asked to have role-playing and were scored by two previously trained observers, each separately scoring the role played by the students. The scores of the two observers were then compared and the Kappa coefficients implied the high reliability of the saying "no" checklist [14]. Data analysis was done using SPSS software by descriptive statistics (mean and standard deviation) as well as inferential statistics (ANOVA with repeated observations and independent t-test).
3. RESULTS
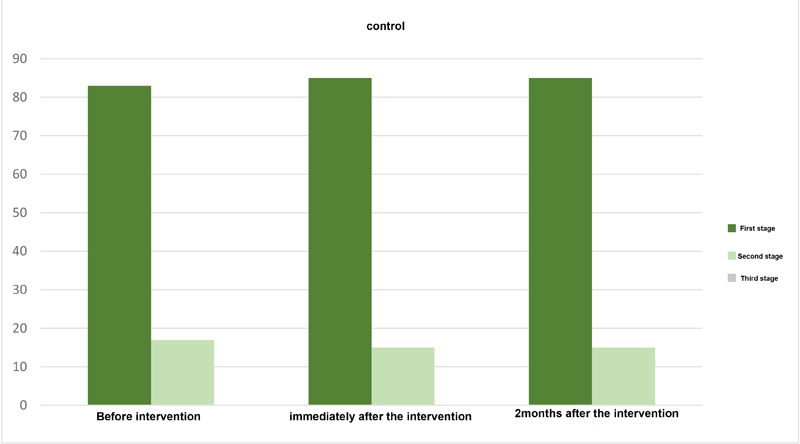
The results showed that the majority of families had two children. There were 24 students (33.3%) in the intervention group and 23 (43.8%) in the control group. In addition, the highest frequency of birth is the first child of the family, including 31 (43.1%) in the intervention group and 29 (39.7%) in the control group. In terms of family characteristics, the findings indicated that the father's job of most students in both groups was self-employed, including 43 (59.7%) in the intervention group and 32 (43.8%) in the control group. With regard to the mothers’ occupation, most of them were housewives who were 68 (94.4%) in the intervention group and 93 (93.2%) in the control group. Furthermore, the highest frequency of fathers' and mothers’ education was an elementary school (51.4% and 44.4%, respectively). In relation to the main goal of the study, the t-test between two independent groups showed that the mean score of saying ‘no’ in the pre-intervention stage showed no significant difference between the intervention and control group. Based on the mean of each one, there was a higher score for saying ‘no’ in the control group (0.06), but immediately and two months after the intervention, there was a significant difference between the groups (0.000) (Table 1). Furthermore, the ANOVA test with repeated values showed a statistically significant difference between the skill score of saying "no" in the intervention and control groups after the intervention compared to before it (Table 2). Based on the classification of saying ‘no’ scores (0-1.33, weak; 1.34-2.67, moderate; 2.68-4.01, good), it has been observed that the mean scores of the intervention group in the pre-training stage were in the moderate class. In the stage immediately and two months after the intervention, they were in a good class and the control group, the scores were assigned to the moderate class in all three stages (before, immediately, and two months after). According to the repeated variance analysis, the mean of saying "no" skill score increased significantly (p=0.000). Given that the saying no skill checklist was designed with four-components to evaluate students' role-playing in the first, second, and third times, if the researcher failed to evaluate four-skill components at the first time, then the assessment was completed the second and third times, and the frequency distribution of the role-playing of research units is shown in all the three stages of both intervention and control groups in Figs. (1 and 2). The assessment was mainly done in the first time of the role-play and none of the research units was evaluated for the third time.
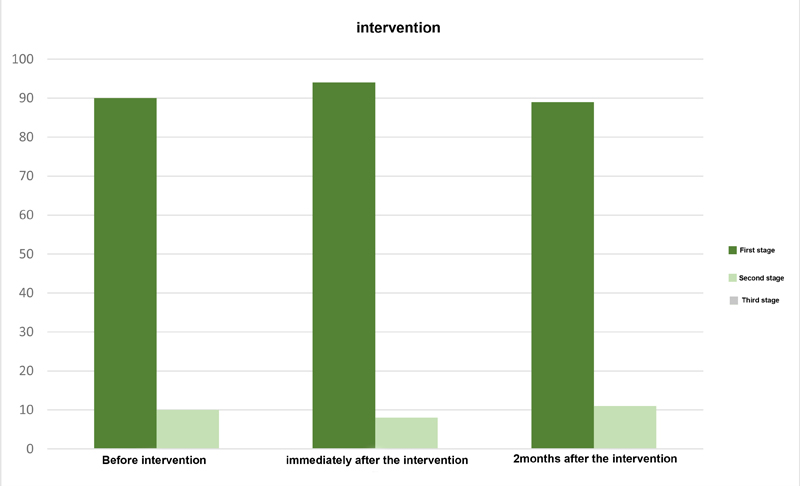
Table 1.
| Stage | Group | Number | Mean | Standard deviation | T value |
Degree of freedom |
p-value |
| Before intervention | control | 73 | 2.0685 | 1.05842 | 1.835 | 143 | 0.06 |
| intervention | 72 | 1.7500 | 1.03120 | ||||
| Immediately after the intervention | control | 73 | 1.7534 | 0.98292 | -14.996 | 143 | 0.000 |
| intervention | 72 | 3.6944 | 0.49330 | ||||
| Two months after the intervention | control | 73 | 2.0822 | 0.95384 | -10.776 | 143 | 0.000 |
| intervention | 72 | 3.5139 | 0.60498 |
| Score of saying no skill | Intervention | Control | ||
| Mean | Standard deviation | Mean | Standard deviation | |
| Before intervention | 1.7500 | 1.03120 | 2.0685 | 1.05842 |
| immediately after the intervention | 3.6944 | 0.49330 | 1.7534 | 0.98292 |
| Two months after the intervention | 3.5139 | 0.60498 | 2.0822 | 0.95384 |
| p-value | 0.000 | 0.009 | ||
4. DISCUSSION
The results of this study showed that the mean score of saying ‘no’ was significantly increased in the intervention group after the intervention and was placed in the good class, while the control group was placed in the moderate class in the three stages. Marsigelia et al., in a study entitled “Culturally specific youth substance abuse resistance skills: applicability across the US-Mexico border” investigated the application ability of REAL (Rejection, Explanation, Avoidance, Leaving) among the youth for resistance against drug abuse. Based on the results of this study, most of the young people in the training group used one of these methods in response to the suggestion of cigarette smoking, alcohol and marijuana, while there was no significant difference between the education and control groups in terms of age, socioeconomic status and training [25]. In addition, Rahimi conducted a research with the aim of assessing the effectiveness of life skill training on the reduction of high-risk behaviors among male students who were at risk. The results of this study showed that the training of life skills resulted in a change in at-risk students’ attitude to drug abuse and a significant decrease in the rate of depression, as well as the students’ problems related to assertiveness, self-control and sensation seeking [26]. Dortaj in a study entitled “The effect of group discussion and role-playing on assertive skills in students” showed that both methods of group discussion and role-playing affected the venture skills [27]. Findings of Sohrabi's study entitled “Determining the effectiveness of life skills training on coping styles of girl Adolescents” indicated that life skills training had an impact on the problem-centered style [28]. Moreover, training in other groups is effective, as Ahmadi et al. in their research on the effectiveness of group education on social anxiety among adolescents with hearing impairment revealed that education in this group of adolescents was also effective and recommended that group training of assertiveness should be considered in educational programs for adolescents with hearing impairment [29]. Dorke in 2013, in the study entitled “Determining the effectiveness of life skills training in reducing the tendency toward drug use among workers” also showed that the tendency of drug abuse of the experimental group in the post-test stage was significantly less than the control group. The results of an investigation by Ezat Aghajari et al. entitled “The effect of school-based interventions on “saying no” in junior high school students showed that there was a significant increase in the scores of “saying no” in the experimental group, which were decreased in the control group [30]. Bahrami in a study with the aim of assessing the effectiveness of life skills training on reducing the tendency toward high-risk behaviors in high school adolescents confirmed that the effect of life skills training on the tendency towards high-risk behaviors (drug abuse, alcohol and smoking) was significant and that the mean scores of high-risk behaviors of the experimental group in the pre-test (76.46) as well as post-test (67.46) indicated a decrease in the inclination to high-risk behaviors as a result of life skills training [31].
Moreover, the results of Nichols et al. with the aim of determining the ability to reject, showed that providing logical and detailed discussions for the rejection strategy was effective. The results of the above studies are consistent with ours in relation to the lack of ability to say "no" because the training led to the increased skill of saying "no" in the mentioned researches and the present research [32]. The above studies were consistent with the results of the present study. It seems that due to the fact that the skills of saying "no" were trained in detail with the participation of students in the present study and that the students learned the skill to say "no" fully and effectively with all the four components using the role-playing method in groups of 2, 3 or 4, the role-play of each student was discussed by the group and its strengths were enhanced to fully and effectively utilize the skills, leading to an increase in this skill in the case group. In the control group, this skill has increased, which seems to be due to various reasons, including the use of mass media particularly radio and television, family and school education, personal experiences, students' curiosity and exchange of views with each other. Besides, despite the fact that the case and control groups were randomly selected from two schools in one area similar in terms of cultural, economic, and social context without significant difference in demographic information, the parents’ level of education in the control group was higher than the case group and the number of children in the case group was more than the control group. Considering the random sampling method, the existence of a significant difference between the parents' education and the number of children in families of research units in the case group was out of control of the researcher. The results of this study also showed that there was no significant intergroup difference in pretest between case and control groups in terms of saying "no" skill and that the score of saying "no" was higher in the control group. In the stage immediately and two months after the intervention, the score of saying "no" skill in the case group had a higher score, which implies the effectiveness of the training. Another case is that to reduce the observation error by the researcher, the role-playing assessment was performed in three stages. Based on the results presented in Figs. (1 and 2), the majority of students have done role-playing in the first performance. This possibility of evaluation during the three steps eliminates the error of the evaluator, which emphasizes the accuracy of information obtained.
CONCLUSION
When a person is worth by oneself, can take on an active role in the social group more than others to freely and effectively express what they want and they resist the belief pressure of others, using training methods such as role-playing where a new behavior is expected, this active role is likely to be provided and will affect the skill of rejecting risky suggestions among students, and this educational method can be easily implemented and applied as a preventive and therapeutic strategy in educational centers for children and adolescents. Considering that the follow-up period of the effect of this intervention method is short, it is suggested that the present study be pursued with more sessions and that the continuation of training, i.e., the repetition of education be done in different intervals as a supportive step for more efficiency.
ETHICS APPROVAL AND CONSORT TO PARTICIPATE
The study was approved by the ethical committee of Isfahan University of Medical Sciences, Iran with approval No. 328960.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from all individual participants included in the study.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from [Isfahan University of Medical Sciences]. Restrictions apply to the availability of these data,.
FUNDING
This article is part of a research project number 389260 of Isfahan University of Medical Sciences that supported this project.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This article has been taken from a part of the thesis approved by the Deputy Minister for Research and Technology, Isfahan University of Medical Sciences whose sampling was conducted in Arak.

