All published articles of this journal are available on ScienceDirect.

Evaluation of CA-125 Biomarker in Acute Appendicitis Patients: Correlation with Clinical Symptoms and Lab Results
Authors Info & Affiliations
Abstract
Objectives:
The aim of this study is to evaluate the diagnostic significance of CA 125 in Acute Appendicitis (AA) along with the changes in its levels about clinical symptoms and lab findings.
Methods:
Patients referred at the emergency department of Madani hospital with the suspicion of AA and right iliac fossa pain were enrolled in this study. Preoperative CA 125 levels along with C-reactive Protein (CRP) and complete blood count were obtained. Lab findings, signs and symptoms were recorded for all the patients. Statistical analysis was conducted based on CA 125 < 16.4 U/mL and ≥ 16.4 U/mL using the logistic regression model, where variables such as fever, anorexia, CRP and Erythrocyte Sedimentation Rate (ESR) were added to the model.
Results:
Of 207 patients with the mean age of 26.55 ± 0.967 years, 48.8% of them were males and 51.20% were females. 122 of the total patients had CA 125 ≥ 16.4 U/mL. Anorexia was significantly associated with increased levels of CA 125. CA 125 was 2.14 times higher in patients presenting anorexia. However, ESR, CRP and fever were not associated with the elevation of CA 125. Based on the contour plot, it was deduced that leukocytosis at its lowest and erythrocyte sedimentation rate at its highest levels is associated with the maximum concentration of serum CA 125.
Conclusion:
Based on the findings from this study, CA 125 cannot be considered as a reliable diagnostic variable for acute appendicitis. Levels of CA 125 may vary with the severity of AA.
1. INTRODUCTION
Acute Appendicitis (AA), inflammation of the appendix, is one of the most reported pathologies of the abdomen that requires emergency surgery, appendectomy. If left untreated, inflammation can lead to the perforation or rupture of the appendix that can cause the spread of the content into the abdominal cavity, causing infection and inflammation of the peritoneum, peritonitis. However, the abscessed appendix is known to be less urgent yet can only be identified surgically. Blockade by feces or foreign material, cancer and infection are commonly known causes of AA. Diagnosis of AA can be challenging and is likely to be presented with signs and symptoms of other ailments such as gall bladder obstruction, gastrointestinal and urinary tract disorders, Crohn’s disease and ovary dysfunction. Alvarado scoring system, comprising of eight predictors based on the sign, symptoms and lab findings, is used for the diagnosis, in addition to the imaging techniques, physical examination and patients’ history [1]. Classically, AA is characterized by abdominal pain, nausea/vomiting, anorexia and fever. Nonetheless, nonclassical signs and symptoms, prevalent in 55% of the patients, make the diagnosis challenging [2].
Studies have been focusing on the determination of biomarkers that can aid the diagnosis of AA with greater sensitivity and specificity. These include inflammatory markers, increased urinary bilirubin [3], pro-calcitonin and 5-hydroxyindole acetic acid, a metabolite of serotonin [4]. MUC16, also referred as CA 125 (carcinogen antigen), is a membrane glycoprotein that is encoded by MUC16 gene. Alterations in the protein are associated with carcinogenic conditions, including ovarian cancer [5] and breast cancer [6], endometriosis and cirrhosis. Researches have also revealed that levels of CA 125 increase in response to peritoneal inflammation. Furthermore, its association with surgical intra-abdominal conditions is also well established. Nonetheless, its role in AA is not yet proven significantly [7]. Therefore, the aim of this study is to evaluate the levels of CA 125 in acute appendicitis patients.
2. METHODS
This prospective study was conducted at the emergency department of Madani hospital from January 2019 - June 2019. Patients presenting right iliac fossa pain and those suspected of having AA were included in the study. Patients aged < 18 years and > 50 years, along with clinical conditions that increase CA 125, such as heart and lung diseases, inflammatory bowel disease, malignancy, pregnancy and endometriosis and ones with recent abdominal surgery, were excluded from our study.
CA 125 levels were measured, preoperatively, using Electrochemiluminescence machine and kits provided by Germany Roche Company. Other blood tests included C-reactive Protein (CRP) and complete blood count. Sonography was also performed for the diagnosis of AA. Patients were evaluated for the signs and symptoms and ones with the Alvarado score of 7 and above underwent an appendectomy.
Categorical parameters were reported using standard deviation, median, relative frequency. The CA 125 variable was then divided into two groups: “less than 16.4 U/mL” and “16.4 U/mL or more”, based on the previous reports [8]. The logistic regression model with the forward method was used to investigate the relationship between underlying and clinical factors with CA125. In this model, at each step, a variable is added to the model. If the p-value of the variable is lesser than 0.25, the variable will stay in the pool, otherwise, it will be excluded. Variables studied were leukocytosis, Erythrocyte Sedimentation Rate (ESR), gender and CRP. Pearson's and Hosmer Lemeshow tests were used for a goodness-of-fit analysis for logistic regression. Statistical significance level was considered at p-value < 0.05. All the analysis was conducted using Minitab v16 software. This study was approved by the Research Ethics Board of Alborz University of Medical Sciences.
3. RESULTS
Of 207 patients evaluated for the study, 101 (48.8%) were males and 206 (51.20%) were females. Descriptive statistics of quantitative and qualitative variables are reported in Tables 1 and 2. The mean age of the patients was 26.55 ± 0.967 years.
CA 125 levels were lower than 16.4 U/mL in 41% of the patients whereas, 58.9% of the patients had CA 125 ≥ 16.4 U/mL.
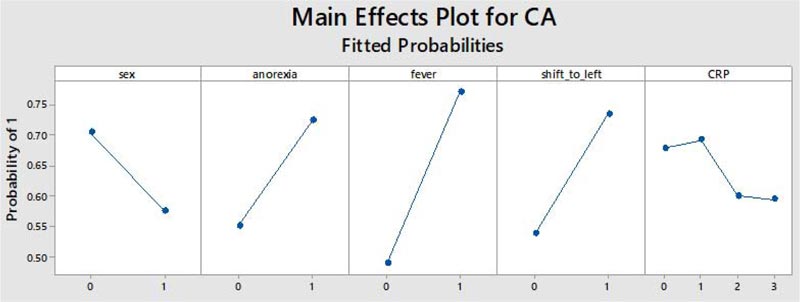
Results from the forward regression model showed that anorexia had a significant impact on the levels of CA 125, p= 0.034 (Fig. 1). Therefore, the chance of CA 125, being greater than 16.4 U/mL for patients with anorexia, was approximately 2.14 times higher than patients without anorexia. The detailed findings from the logistic regression model are shown in Tables 3 and 4.
According to Table 3, with 5 units increase in leukocytosis and ESR, no significant change was observed in CA 125 variable. Furthermore, the odds of high CA 125 for women were 43% lesser than men, however, the difference was not statistically significant. CA125 was 53.3% higher in patients presenting fever, compared to those without fever. Similarly, the value was not statistically significant. Similar results were obtained for CRP.
Pearson and Hosmer Lemeshow were used to examine the goodness-of-fit for logistic regression model. No significant statistical findings were reported for this analysis.
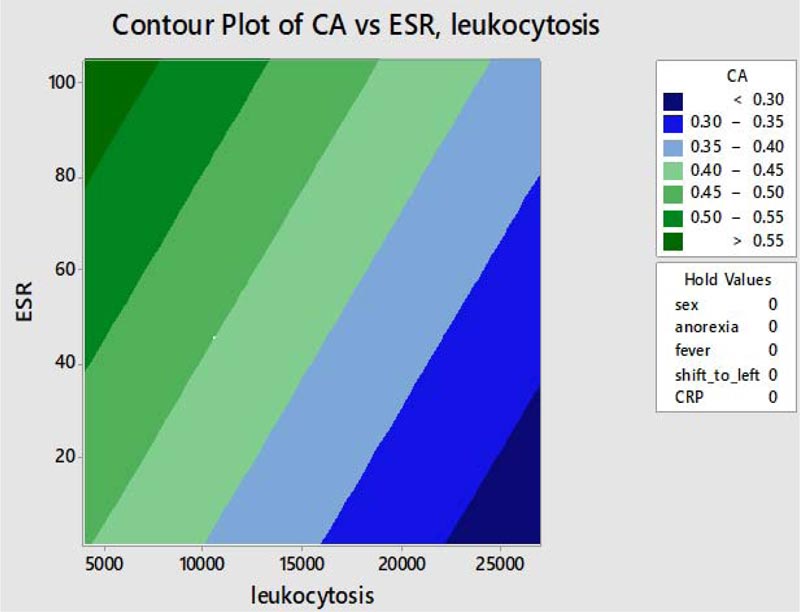
To understand the effect of simultaneous changes in ESR and leukocytosis in regard to CA 125, the counter (Fig. 2) was used. In this chart, the probability that CA 125 above 16.4 U/mL is indicated with a blue (lowest) to green (most) color spectrum. As it can be seen, when the value of leukocytosis is the lowest and that of ESR is highest, the probability of elevated levels of CA 125 is maximum. CA 125 is less likely to be below 16.4 U/mL in patients with elevated leukocytosis and normal ESR.
4. DISCUSSION
Inflammation is the primary underlying pathogenesis of appendicitis [9]. Studies have shown that elevated levels of CA 125 are associated with the progression of the disease and corresponding inflammatory response [10].
The tumor antigen, CA 125 is expressed in mesothelial cells, lungs, amniotic cells, endometrial cells and conjunctiva. Its expression in peritoneal cells is characterized by peritonitis, where IL-1 is one of the effective triggers of its secretion. Furthermore, it is also seen that the elevation of CA 125 usually occurs 6 hours following the stimulation of mesothelial cells [11].
Our study reports the relationship between the increased levels of CA 125 in acute appendicitis patients and the relationship with the classical symptoms and findings of AA. Based on the previous reports, our study evaluated the cut-off of 16.4 U/mL from the receiver operator curve. In a recent study, Pouraghaei, M et al. [8] reported that among 95 AA patients, CA 125 levels are significantly higher in female and AA patients than non-AA patients. However, the severity of appendicitis was insignificantly associated with CA 125 levels. In a study by Cetinkaya, E et al. [12], CA 125 levels were reported to be significantly higher in patients with perforated or gangrenous appendix as compared to uncomplicated ones, showing that the severity of AA is linearly associated with the levels of CA 125.
| - | Age | ESR | Shift_Left_Higher_85pr | Leukocytosis | Onset | Admitted_days |
|---|---|---|---|---|---|---|
| Mean | 26.55 | 21.46 | .7935 | 12924.12 | 1.08 | 3.88 |
| Std. Error of Mean | .769 | 1.154 | .00742 | 287.389 | .090 | .139 |
| Median | 25.00 | 17.00 | .8200 | 13000.00 | 1.00 | 3.00 |
| Std. Deviation | 11.068 | 16.560 | .10472 | 4054.119 | 1.273 | 1.995 |
| Variables | Count | Column N % | |
|---|---|---|---|
| CA125 | less than 16.4 U/mL | 85 | 41.1% |
| 16.4 U/mL or more | 122 | 58.9% | |
| Sex | 0 | 126 | 60.9% |
| 1 | 81 | 39.1% | |
| Pain_location | 0 | 187 | 91.2% |
| 1 | 18 | 8.8% | |
| Shifting_pain | 0 | 24 | 11.8% |
| 1 | 179 | 88.2% | |
| Anorexia | 0 | 76 | 37.1% |
| 1 | 129 | 62.9% | |
| Naseua_vomiting | 0 | 53 | 25.9% |
| 1 | 152 | 74.1% | |
| Fever | 0 | 198 | 95.7% |
| 1 | 9 | 4.3% | |
| Lecositoz_above_16000 | 0 | 155 | 78.7% |
| 1 | 42 | 21.3% | |
| Shift_to_left | 0 | 33 | 16.6% |
| 1 | 166 | 83.4% | |
| U_A_pos_edrar | 0 | 176 | 88.0% |
| 1 | 24 | 12.0% | |
| CRP | 0 | 56 | 27.7% |
| 1 | 43 | 21.3% | |
| 2 | 38 | 18.8% | |
| 3 | 65 | 32.2% | |
| Sonography | 0 | 55 | 27.4% |
| 1 | 146 | 72.6% | |
| Sppendix_location_during_surgery | 1 | 175 | 84.5% |
| 2 | 32 | 15.5% | |
| Appendix_status_during_surgery | 1 | 49 | 23.7% |
| 4 | 110 | 53.1% | |
| 5 | 48 | 23.2% | |
| Pathology_status | 0 | 29 | 14.0% |
| 1 | 178 | 86.0% | |
| Complication | 0 | 171 | 96.1% |
| 1 | 7 | 3.9% | |
| Exp | 1 | 34 | 16.4% |
| 2 | 61 | 29.5% | |
| 3 | 112 | 54.1% | |
| - | Unit of Change | Odds Ratio | 95% CI |
|---|---|---|---|
| Leukocytosis | 5 | 0.9998 | (0.9994, 1.0003) |
| ESR | 5 | 1.0256 | (0.9190, 1.1446) |
| Level A | Level B* | Odds Ratio | 95% CI |
|---|---|---|---|
| Sex(ref:male) | - | - | - |
| 1 | 0 | 0.5691 | (0.2764, 1.1716) |
| Anorexia | - | - | - |
| 1 | 0 | 2.1402 | (1.1184, 4.0954) |
| Fever | - | - | - |
| 1 | 0 | 3.5327 | (0.4066, 30.6940) |
| Shift_to_left | - | - | - |
| 1 | 0 | 2.3825 | (0.8000, 7.0952) |
| CRP | - | - | - |
| 1 | 0 | 1.0673 | (0.3980, 2.8623) |
| 2 | 0 | 0.7101 | (0.2500, 2.0173) |
| 3 | 0 | 0.6941 | (0.2823, 1.7071) |
| 2 | 1 | 0.6654 | (0.2438, 1.8158) |
| 3 | 1 | 0.6504 | (0.2642, 1.6011) |
| 3 | 2 | 0.9775 | (0.3994, 2.3924) |
To our knowledge, this is the first study to evaluate the symptoms and clinical presentation of AA with elevated levels CA 125. Herein, we found that elevation of CA 125 is greater in AA patients presetting fever, anorexia, leukocytosis, CRP and increased ESR. An exception to anorexia, these variables were not associated significantly. A study has shown that increased leukocytes are correlated with the increased levels of CA 125 [10]. Berger, Y et al. [7], reported no significant differences in the level of CA 125 among AA and non-AA patients and the cut-off was set at 8.75 U/mL. They also showed that CA 125 was significantly associated with severity of AA in males and with white blood cells levels where neutrophil percentage and CRP were insignificant.
Our study does not include gender-based comparison, whereas studies have reported that the levels CA 125 may vary in males and females [7, 8]. Furthermore, postoperative levels of CA 125 are also not recorded in this study. In order to conclude findings related to new biomarkers, studies enrolling larger sample sizes are required, which is also one of the limitations of this study.
CONCLUSION
From our findings, despite CA 125 levels, that may vary with the severity of the symptoms and lab findings, CA 125 is not significantly associated with acute appendicitis and associated presentations.
AUTHORS' CONTRIBUTION
Dr. Mojtaba Ahmadinejad and Dr.Mahla Alizadeh: conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript.
Dr. Seyed Ali Hashemi and Dr.Alireza Shirzadi:Designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the manuscript.
Dr. Ali Soltanian and and Dr. Jafar Ashrafi and Dr.Kourosh Kabir: Coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Research Ethics Board of Alborz University of Medical Sciences, Iran (Approval No. IR.ABZUMS.REC.1398).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 1983.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

