All published articles of this journal are available on ScienceDirect.

Factors Influencing Patient Satisfaction with Healthcare Services Offered in Selected Public Hospitals in Bulawayo, Zimbabwe
Authors Info & Affiliations
Abstract
Introduction:
Patient satisfaction with health care services is vital in establishing gaps to be improved, notably in public health facilities utilised by the majority in Low and Middle-Income Countries. This study assessed factors that influenced patient satisfaction with United Bulawayo Hospitals and Mpilo Hospital services in Bulawayo in Zimbabwe.
Methods:
A cross-sectional survey was conducted on 99 randomly selected respondents in two tertiary hospitals in Bulawayo. Chi-squared tests were employed to determine associations between different demographic characteristics and patient satisfaction with various services they received. Multiple Stepwise Linear regression was conducted to assess the strength of the association between different variables.
Results:
Most of the participants who took part in the study were males in both selected hospitals. It was generally observed that patients were satisfied with these facilities' services, symbolised by over 50% satisfaction. However, patients at Mpilo were overall more satisfied than those at United Bulawayo Hospitals. Variables “received speciality services,” “average waiting times,” and “drugs being issued on time” were significant contributors to different levels of satisfaction observed between Mpilo and United Bulawayo Hospitals.
Conclusion:
Generally, patients are satisfied with the services and interactions with the health service providers at United Bulawayo Hospitals and Mpilo Hospitals. However, patients at Mpilo were more satisfied than those at United Bulawayo Hospitals. There is generally a need to improve pharmaceutical services, outpatient services, and interaction with health service provider services to attain the highest levels of patient satisfaction.
1. INTRODUCTION
Patient satisfaction surveys have gained momentum in the past two decades [1, 2]. There has been a significant shift towards providing patient-centred care to attain high standards as far as the quality of care is concerned [1, 2]. There is an agreement by different scholars that satisfied patients are more willing to seek medical advice, abide by treatment regimens, and encourage their peers to utilise health services [1, 3-5].
Different health facilities that provide similar services may differ in service quality levels [6]. Various contextual factors could influence the nature and manner in which the health services are rendered to recipients, stimulating varied satisfaction levels [6]. In developed countries such as Germany and France, public health facilities are expected to conduct patient satisfaction surveys regarding the quality of care and services offered to patients [1, 7].
In developing countries such as Zimbabwe, most public health care facilities are run by nurses due to high staff turnover [8]. The nurse to patient ratio in both facilities is well above the recommended by the World Health Organization of a minimum health worker density of 2.3 skilled health workers (physicians and nurses/ midwives) per 1000 population [8, 9]. Public hospitals are the most utilised by the general populace as services are usually cheaper than private facilities, which results in health service workers to population ratios of less than 1 per 1000 population in developing countries with high migration of workers Zimbabwe [8, 9]. There is usually a trade-off in quality of services rendered in these institutions as most public facilities have long waiting times, shortage of drugs, and staff shortages [10, 11].
Reviewed patient exit interviews in public health hospitals in Bulawayo indicate that at least 60% of patients are dissatisfied with the services they receive in these institutions. Researchers did not find any research documenting patient satisfaction and associated factors in patients attending public health institutions in Bulawayo. Therefore, this study sought to assess factors that influence patient satisfaction with services offered at United Bulawayo Hospitals and Mpilo Hospital in Bulawayo, Zimbabwe.
2. METHODS
2.1. Study Area
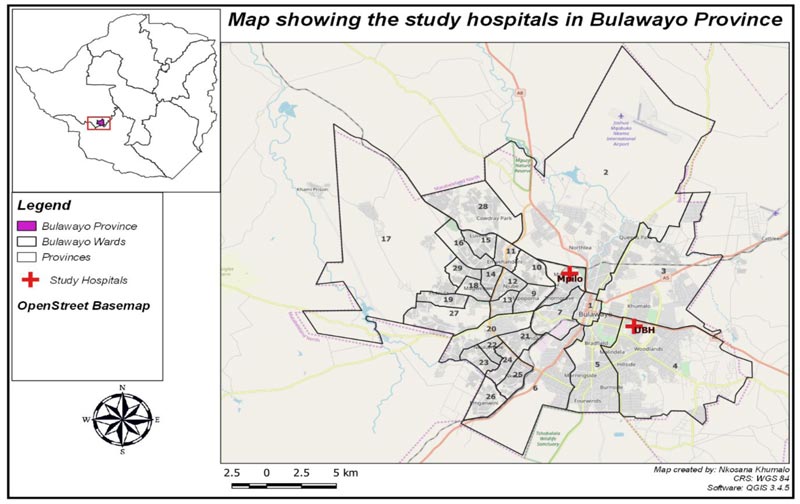
The study was conducted at United Bulawayo Hospital and Mpilo Hospital in Bulawayo. The two hospitals are tertiary referral hospitals that are found in Bulawayo Metropolitan Province. Mpilo Hospital is the second-largest hospital in Zimbabwe after Parirenyatwa hospital in Harare [12]. It is a referral centre for all western suburbs of Bulawayo and Matabeleland North, Matabeleland South, and Midlands Provinces of Zimbabwe [12, 13]. The hospital has a Renal Unit, Main Hospital with outpatients and admission services, Maternity Unit, Pediatric Unit, Opportunistic Infection Clinic, and a Nurse Training School [13]. The hospital is not described as a group of hospitals though it offers varied specialist services. This hospital caters to most people living in this catchment area, most of whom are unemployed, and those who are employed live well below the poverty datum line [14]. On the other hand, United Bulawayo Hospital (UBH) is a hospital offering varied services to patients [15]. The group of hospitals is made up of Richard Morris (that offers eye services), Lady Rodwell Maternity Hospital (which offers maternal services), the Main Hospital (which offers inpatients casualty, surgical, theatre, and intensive care unit), surgical and medical care, Opportunistic Infections Clinic (for HIV and Aids and other Opportunistic infections), Training Hospital (for General Nurses, Orthopedic Nurses, and Ophthalmology Nurses) and a family planning walk-in clinic [15]. The hospital is located in the eastern part of the city of Bulawayo [13]. It serves as a referral centre for the eastern suburbs of Bulawayo, part of Matabeleland South and North and Masvingo provinces [13, 15]. The majority of the people in this catchment are from Low to Medium socioeconomic status [13]. The facility is recognised as a group of hospitals. Fig. (1) presents the study area map.
2.2. Study Design
A cross-sectional survey was conducted on selected patients who attended outpatient departments, those who received services from the pharmacy, and those admitted in the wards at Mpilo and UBH. This design enabled researchers to identify factors that influenced patient satisfaction and, at the same time, determining levels of patient satisfaction with the services they received in these selected hospitals [16].
2.3. Study Population
This study targeted all patients aged 18 years and above who received or attended outpatients, pharmacy, and those admitted at the wards at UBH and Mpilo Hospitals during data collection. The total number of those that met this inclusion criterion during data collection was approximately 2500 for both hospitals. Only patients deemed competent were included in the study such as mentally ill patients, and patients in intensive care units and other specialised wards were excluded from this research.
2.4. Sampling and Sample Size
A sample size calculator on EPI INFO was used to estimate the minimum sample size needed to make meaningful inferences. The estimated 2500 patients met the inclusion criteria, a Confidence Level of 95%, Width of Confidence of 10%, and the expected value of an attribute of 50% gave a sample size of 92 respondents. The samples were divided equally for the two hospitals, which gave a 46 per hospital sample size. A non-response rate of 10% was factored in, resulting in a sample size of 50 per hospital, giving a total number of respondents of 100. The systematic random sampling technique was then utilised to select patients from outpatients, pharmacies, and wards. The total number of available patients who met the inclusion criteria was ascertained. That number was divided by a certain interval that would enable the sample size of 50 to be attained in each hospital. The patients were assigned random numbers and if not consenting to take part in the study the next available was recruited until the targeted sample size was attained. Selected patients had at least received one of these services at outpatient, pharmacy, and wards.
2.5. Data Collection Tool
A pre-tested self-administered semi-structured question- naire developed and adapted from different authors was used to collect data from respondents [1, 17, 18]. The questionnaire comprised four sections: Section A, addressing sociodemo- graphic characteristics of respondents, Section B, addressing satisfaction with services offered at outpatients, Section C, addressing patient satisfaction with services provided at the pharmacy and Section D satisfaction with services provided at the wards. The tool was translated into IsiNdebele to cater to a majority of the patients at the aforementioned Bulawayo hospitals. The tool took, on average, 15-20 minutes to administer.
2.6. Data Analysis
2.6.1. Data Management
Data was captured in excel then imported into STATA Version 13 SE for cleaning, coding, and analysis.
2.6.2. Data Management and Analysis
Patients were asked some binary questions to probe their satisfaction with different services they received in the health facility. After all these questions, they were asked to rate the services they received on a scale of 1-10 with zero being dissatisfied and ten being highly satisfied. The respondents who chose five and above were deemed satisfied with the services in question, while those choosing four and below were dissatisfied. The sample of the questionnaire is attached as a supplementary file to this manuscript. The Chi-squared tests were then conducted to test for the association between demographic characteristics and satisfaction levels with different services received. Furthermore, Multiple Stepwise Linear Regression (MSLR) was also conducted to determine the strength of observed associations between the two hospitals' different variables and comparisons.
3. RESULTS
The study had a 99% response rate resulting in the completion of 99 questionnaires.
3.1. Socio-demographic Characteristics of Respondents
Most of the respondents in both facilities were males (54% for UBH and 57% for Mpilo). Over 40% of respondents in both facilities had a secondary level of education. Most respondents (92%) in both facilities were living well below the Poverty Datum Line. These findings are presented in Table 1.
| Socio-demographic Characteristic | UBH | Mpilo | Total | (%) | ||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Sex | ||||||
| Male | 27 | 54.0 | 28 | 57.1 | 55 | 55.6 |
| Female | 23 | 46.0 | 21 | 42.9 | 44 | 44.4 |
| Marital Status | ||||||
| Single | 15 | 30.0 | 17 | 34.7 | 32 | 32.3 |
| Married | 24 | 48.0 | 27 | 55.1 | 51 | 51.5 |
| Divorced | 5 | 10.0 | 1 | 2.0 | 6 | 6.1 |
| Widowed | 6 | 12.0 | 4 | 8.2 | 10 | 10.1 |
| Age (in years) | ||||||
| 18-19 | 1 | 2.0 | 1 | 2.0 | 2 | 2.02 |
| 20-64 | 46 | 92.0 | 46 | 94.0 | 92 | 92.9 |
| 65+ | 3 | 6.0 | 2 | 4.1 | 5 | 5.1 |
| Education | ||||||
| Primary | 10 | 20.0 | 14 | 28.6 | 24 | 24.2 |
| Secondary | 22 | 44.0 | 18 | 36.7 | 40 | 40.4 |
| Tertiary | 18 | 36.0 | 17 | 34.7 | 35 | 35.4 |
| Occupation | ||||||
| Unemployed | 12 | 24.0 | 16 | 32.7 | 28 | 28.3 |
| Employed | 22 | 44.0 | 14 | 28.6 | 36 | 36.4 |
| Self-employment | 16 | 32.0 | 19 | 38.8 | 35 | 35.4 |
| Income | ||||||
| Below poverty datum line | 46 | 92.0 | 46 | 94.0 | 92.0 | 92.9 |
| Above poverty datum line | 4 | 8 | 3 | 6.12 | 7 | 7.1 |
3.2. Patients Satisfaction with Different Services Received and Interactions with Health Service Providers
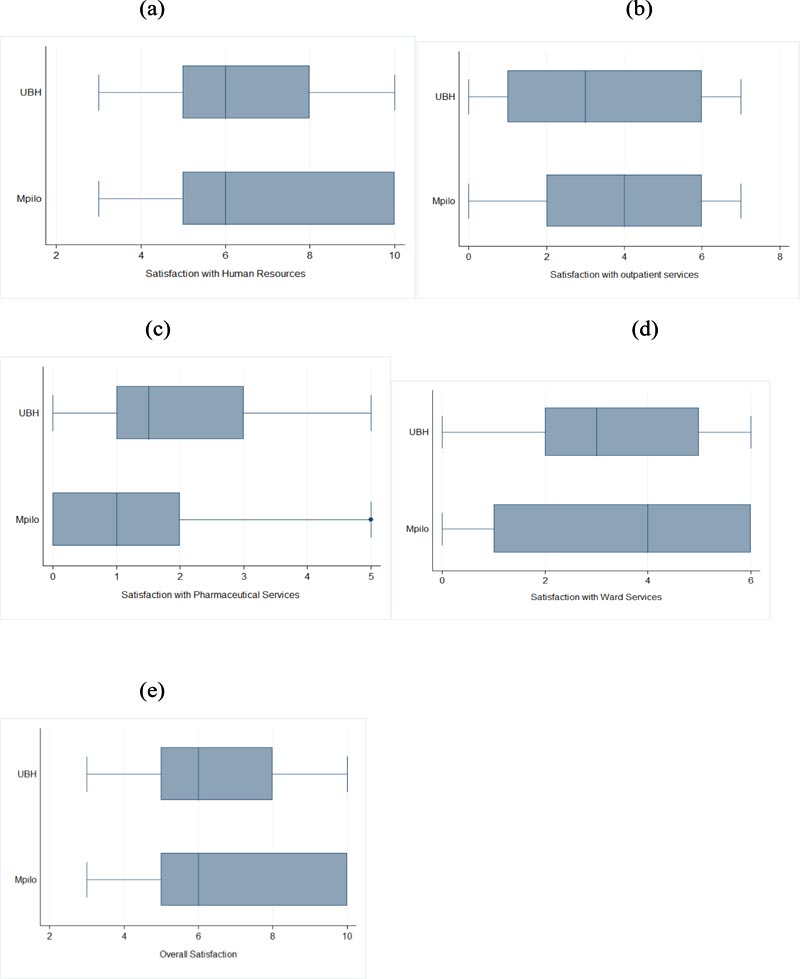
Generally, patients were satisfied with services received or interactions they had with health service providing staff members. However, patients receiving services at Mpilo were generally satisfied than those at UBH except for the pharmacy services. These findings are presented in Table 2 and Fig. (2a-e), and they depict medians of greater than five on a satisfaction scale of 1-10 symbolising that the patients were generally satisfied.
3.3. Satisfaction with Outpatient Services at Mpilo and UBH.
The differences in satisfaction levels on services offered at the outpatient department in these institutions were not significant except for the variables “received speciality services” and “average waiting time.” These variables were found to be predictors of patient satisfaction influencing overall satisfaction. These findings are presented in Table 3.
3.4. Satisfaction with Pharmaceutical Services in these Selected Hospitals
Drugs being issued on time were a significant contributor to patient satisfaction through other variables that were not contributors to satisfaction. However, values obtained for satisfaction with the cost of medication were similar in the two hospitals. These findings are presented in Table 4.
3.5. Satisfaction with Services Offered in the Wards in these Selected Hospitals
The differences in satisfaction with the wards' services were not significantly different between the two public health facilities. These findings are presented in Table 5. A multi-linear regression model depicts that overall patient satisfaction can be explained by general satisfaction in the ward, satisfaction in interaction with the health workers, and the amount of time the patient spends at the outpatient department.
| Variable | *MSLR Coef. | p-value |
95% Conf. Interval |
|---|---|---|---|
| Ward Satisfaction | 0.31 | 0.00 | 0.16-0.46 |
| Satisfaction with Human Resources | 0.61 | 0.00 | 0.49-0.74 |
| Satisfaction with time spent in Outpatients | -0.01 | 0.003 | -0.02-0.00 |
| Residual | 1.97 | 0.00 | 1.17-2.77 |
| Outpatient Care | UBH | Mpilo | Total | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | χ2p-value | |
| Treated in a friendly manner | 30 | 60.0 | 32 | 65.3 | 62 | 62.6 | 0.59 |
| Adequate ventilation in waiting areas | 23 | 46.0 | 26 | 53.1 | 49 | 49.9 | 0.48 |
| Examined with respect and care | 32 | 64.0 | 34 | 69.4 | 66 | 66.7 | 0.57 |
| Expensive Consultation fee | 14 | 28.0 | 16 | 32.7 | 30 | 30.3 | 0.61 |
| Adequate consultation time with Doctor | 30 | 60.0 | 28 | 57.1 | 58 | 58.6 | 0.77 |
| Condition was explained fully by medical practitioner | 14 | 28.0 | 15 | 31.2 | 29 | 29.6 | 0.73 |
| Received specialty services | 14 | 30.4 | 6 | 13.0 | 20 | 21.7 | 0.04* |
| Average waiting time in Minutes (Interval) | 35 (30-60) | 45 (30-60) | 40 (30-60) | 0.02* | |||
| Pharmaceutical Services | UBH | Mpilo | Total | - | |||
|---|---|---|---|---|---|---|---|
| - | n | % | n | % | n | % | χ2 p-value |
| Drugs issued on time | 14 | 30.4 | 6 | 13.0 | 20 | 21.7 | 0.04* |
| Received all prescribed medication | 13 | 28.3 | 8 | 17.4 | 21 | 22.8 | 0.21 |
| Pharmacy staff friendly and helpful | 17 | 37.0 | 16 | 34.8 | 33 | 35.9 | 0.83 |
| Queries on medication clarified | 20 | 43.5 | 13 | 28.3 | 33 | 35.9 | 0.13 |
| Cost of medication fair | 22 | 47.8 | 22 | 47.8 | 44 | 47.8 | *** |
| Ward Services | UBH | Mpilo | Total | - | |||
|---|---|---|---|---|---|---|---|
| - | n | % | n | % | n | % | χ2 P-value |
| Nurses are friendly and helpful | 34 | 69.3 | 37 | 80.4 | 71 | 74.7 | 0.22 |
| Provides good quality food | 12 | 25.5 | 12 | 26.1 | 24 | 25.3 | 0.86 |
| Ablution facilities are easily accessible | 31 | 63.3 | 26 | 56.5 | 57 | 60.0 | 0.5 |
| Wards are clean | 33 | 67.4 | 32 | 69.6 | 65 | 68.4 | 0.82 |
| Bed Linen Clean | 21 | 42.9 | 25 | 54.4 | 46 | 48.4 | 0.26 |
| Would you refer a relative | 27 | 55.1 | 31 | 67.4 | 58 | 61.1 | 0.22 |
4. DISCUSSION
It was observed in the study that most of the respondents were male's contrary to what other scholars report. It has alluded that women are the ones that have good health-seeking behaviours as compared to males [4, 19]. However, our finding is supported by a study conducted by Syed et al. (2017), which found that ill women would less often seek health services than males [20, 21]. This is further explained by Johansson et al. (year), who reported that women usually shun away from health facilities in fear of stigmatisation and being separated from their families [22]. Furthermore, it has been noted that males seek treatment late and are more likely to report to tertiary institutions for care than females.
It was reported in the study that the majority of respondents (over 90%) lived well below the Poverty Datum Line. Different authors report that the Poverty datum line ranges between 170-400 United States Dollars or equivalent for an average family of five [23-25]. Most public facilities in Zimbabwe cater to all classes' patients through being frequented by people of low economic quintile. Those who are of medium to high socioeconomic quintile can afford private institutions with a better quality of services than public institutions [26]. Public facilities are lenient and flexible in affording patients' payment plans [27, 28]. Children under the age of five and the elderly (65+) are exempted from paying hospital fees in public institutions [17].
Our study reported that most patients are satisfied with health care services in these two public health facilities. Patients are deemed to be satisfied by different authors if their overall assessed satisfaction levels are greater than 50% [1, 29, 30]. These findings are supported by a study by Shamu et al. (2017), who report that most bigger referral facilities in Zimbabwe are well equipped as compared to smaller ones [31]. This ensures that most of the patients' expectations are usually met as they would tend to compare services received with the facilities where they would have been referred from [31].
Predictors of patient satisfaction were average waiting times, availability of speciality services, and being given drugs on time. These findings are also well explained by the study conducted by Shamu et al. (2017), who pointed out that higher hierarchy health facilities are usually well funded and equipped to deal even with complications that lower-level facilities cannot deal with [31]. Therefore, patients attending these facilities are bound to be satisfied. Other scholars have also reported waiting times to be critical in influencing patient satisfaction [1, 32].
5. LIMITATIONS
It should be noted that patient satisfaction is highly subjective, depending on some factors on a particular day. Therefore responses given in a specific day may depend on the patients' mood or how they have been treated for a particular issue and might sometimes differ from what a person would have experienced over a more extended period. Therefore, there is a need for a cautious interpretation of the findings as these might differ from individual's participants.
CONCLUSION
Generally, patients are satisfied with the services and interactions with the health service providers both at UBH and Mpilo Hospitals. However, patients at Mpilo were more satisfied than those at UBH. Predictors of satisfaction that led to differences between the two selected facilities were the availability of specialised services, average waiting times, and being given drugs on time. There is generally a need to improve pharmaceutical services, outpatient services, and interaction with health service provider services to attain the highest patient satisfaction levels as the observed were not near 100%.
AUTHOR'S CONTRIBUTIONS
CPN crafted objectives and developed the methodology and data collection tools. The author further went on to collect the data together with NM. WNN, together with NM conceptualised the research idea. The author also coordinated the research process and drafted the first manuscript. NM translated the data collection tools into Local Language (Isi Ndebele) and captured the data into excel and cleaned it in preparation for analysis. NS coded the data and performed data analysis. All the authors read and approved the final manuscript.
AUTHOR'S INFORMATION
CPN is a BSc student at the National University of Science and Technology. WNN is a Lecturer in the Department of Environmental Science and Health at the National University of Science and Technology in Bulawayo in Zimbabwe. The author is also a Ph.D. student in the Department of Public Health in the School of Health Sciences at the University of Venda in South Africa. NM is a Lecturer in the Department of Environmental Science and Health at the National University of Science and Technology. NS is a Research Fellow in the Department of Environmental Science and Health at the National University of Science and Technology in Bulawayo, Zimbabwe.
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
Written permission to carry out this study was sought from the Department of Environmental Science and Health at the National University of Science and Technology and the Ministry of Health and Child Care.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was obtained from parents of adolescents, and the adolescents accented to participate. All respondents were made aware that their participation was voluntary, and they could opt out of the study at any given time without any explanation. Participants were not coerced or given tokens of appreciation for being part of the study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publisher's website along with the published article.

