All published articles of this journal are available on ScienceDirect.

Nutrition-related Knowledge and Behaviour and Financial Difficulties during the COVID-19 Quarantine in Saudi Arabia
Authors Info & Affiliations
Abstract
Background:
Coronavirus disease 2019 (COVID-19) is a severe global public health issue. Evaluating clinical readiness during a pandemic requires substantial awareness of public knowledge and the ability to predict behaviour when working with a highly pathogenic virus.
Objective:
This study examined nutrition-related knowledge and behaviours and financial difficulties related to COVID-19 among adults in Saudi Arabia.
Methods:
A cross-sectional study was conducted among 968 participants via an online questionnaire focusing on demographics, nutrition-related knowledge regarding COVID-19, nutrition-related behaviours, and financial difficulties under COVID-19 quarantine.
Results:
Female participants showed higher scores in knowledge (3.15 ± 0.87) and nutrition-related behaviour (5.49 ± 1.2) during COVID-19. Those aged 40 to 49 years had the highest knowledge score, while older participants (>50) showed more adherence to positive nutrition-related behaviour (P < 0.0001 for both). Higher education indicated higher knowledge scores (3.4 2 ± 0.86; P = 0.001) but not behaviour scores. High-income participants had the highest knowledge score (3.29 ± 0.96; P = 0.001), while middle income participants had the highest behaviour scores (5.52 ± 1.23; P = 0.01). Low-income participants faced more difficulties with food source availability, compared to high-income participants.
Conclusion:
This study’s results help in providing guidelines for planning and designing health education programmes for vulnerable groups.
1. INTRODUCTION
The novel coronavirus disease 2019 (COVID-19) is the latest disease outbreak to gain global attention. COVID-19 has been identified by the United States Centers for Disease Control and Prevention (CDC) as a significant threat to public health [1]. The first case was identified in Wuhan City, Hubei Province, China, and the disease has since spread rapidly [1]. Additionally, the World Health Organization (WHO) announced on February 28, 2020, that the COVID-19 outbreak is a Public Health Emergency of International Concern [2], with numerous cases attributed to human-to-human interaction [1]. Thus, governments worldwide have implemented lockdowns and quarantines to help in decreasing the rate of infection.
In managing infectious diseases, public awareness is critical; individual behaviours, such as increased hygienic care and social distancing, may reduce the spread of the disease. Moreover, the public’s response can be evaluated by the extent of their awareness and knowledge during an outbreak, especially regarding disease transmission, vaccine availability, and successful medical care [3]. Health nutrition awareness also plays a key role in reducing infection and related problems by promoting good health, increasing care outcomes, and avoiding future health issues. Additionally, higher nutritional awareness is related to healthier eating habits and stronger nutritional status [4].
The WHO and the Ministry of Health of Saudi Arabia provided various food and nutritional tips during quarantines [5]. Notably, previous studies have reported that knowledge of infectious diseases allows individuals to act appropriately to prevent infection [6-8]. However, quarantines result in negative dietary behaviours by restricting an individual’s daily routine [5]. Thus, to achieve ultimate success against COVID-19 and contain the transmission of the virus, public awareness, healthy practices, and positive commitment are necessary [9, 10].
Saudi Arabia has devoted many resources to successfully control the COVID-19 outbreak. Moreover, the economic strength of Saudi Arabia has allowed it to import food to meet its needs and to achieve financial stability that allows individuals to follow a regular diet that is dependent on trade [11]. However, there is limited research on the nutrition behaviours and difficulties in following a regular diet among adults in Saudi Arabia [12]. Hence, in the current study, nutrition-related knowledge and behaviours, as well as the financial difficulties related to the COVID-19 pandemic, were assessed among adults in Saudi Arabia. This information is essential to strengthening the coordination of efforts between public health officials and clinicians for the at-risk population [13].
2. MATERIALS AND METHODS
2.1. Participants
A cross-sectional survey was conducted between 1 April and 15 May 2020, during the early stages of the pandemic in Saudi Arabia. The participants were under a 13-hour quarantine on 23 March, followed by a 24-hour quarantine on 13 April when learning institutions, malls, and restaurants were closed [14]. Participants were recruited from all Western regions of Saudi Arabia and comprised both men and women within the age range of 18–60 years. According to the Unified National Platform GOV.SA, the total population of Saudi Arabia in 2019 was 34,218,169 [15]; given this number, the sample size calculator indicated that the sample size needed to achieve sufficient statistical power is 664, allowing for a 5% margin error, with a 99% confidence level, and a response distribution of 50% [16]. The study design was reviewed and approved by the Unit of Biomedical Ethics Research Committee at King Abdulaziz University (Reference No 216-20).
2.2. Study Design
The study used a self-administered questionnaire that included 21 closed-ended questions in Arabic, and which took less than 10 minutes to complete. It was distributed online through a web link shared over email and social media like Facebook, Twitter, and WhatsApp. The questionnaire consisted of four parts: sociodemographic information, nutrition-related knowledge about COVID-19, nutrition-related behaviours during the period of quarantine during COVID-19, and financial difficulty in following a regular diet. The first page of the survey explained the purpose of the study, the target population, that participation in the study was voluntary, and that all information would be kept confidential. Online informed consent was obtained before participants started the questionnaire.
2.3. Sociodemographic Characteristics
Sociodemographic characteristics included questions on age, sex, nationality, marital status, occupation, monthly income, and education level.
2.4. Nutrition-Related Knowledge Regarding COVID-19
This section consisted of six questions adapted from the CDC and WHO [1]: (1) ‘Do you have knowledge about the emerging coronavirus (COVID-19)?’ (2) ‘What is your source of information about COVID-19?’ (3) ‘Is COVID-19 transmitted through food?’ (4) ‘Do you think that cooking food well eliminates COVID-19?’ (5) ‘Do you think that eating healthy food and drinking water increase the body’s immunity and resistance to COVID-19?’ (6) ‘Do you think that COVID-19 is transmitted through food if the person preparing it is infected with the virus?’ The responses to Questions 1, 3, 4, 5, and 6 were ‘Yes’, ‘No’, and ‘Do not know’, while Question 2 included five checkbox options: (1) ‘Saudi Ministry of Health’, (2) ‘World Health Organization’, (3) ‘television’, (4) ‘social media accounts’, and (5) ‘Family or friends’. The total score for nutrition-related knowledge regarding COVID-19 ranged from 0 to 5, with a higher score indicating better knowledge. Incorrect and ‘Do not know’ answers were given a score of 0.
2.5. Nutrition-Related Behaviours During Quarantine
This section contained eight questions that were developed by the authors, as follows: (1) ‘Did you change your eating habits during quarantine?’ (2) ‘Has your consumption of fruits in general and citrus fruits in particular increased, especially after the spread of COVID-19, because you think it strengthens immunity?’ 3) ‘Have you reduced your intake of fresh food (vegetables, fruits, and fresh milk, among others) due to the quarantine?’ (4) ‘Did you eat more homemade meals during the quarantine period?’ (5) ‘Have you stopped eating from outside the home (from restaurants in general, fast food restaurants, or others) due to the spread of COVID-19?’ (6) ‘Did your dependence on canned and frozen foods increase (due to their long shelf life) during the quarantine period as compared to before quarantine?’ (7) ‘Has your food intake increased due to the quarantine?’ (8) ‘Did you buy more food and store it at home due to the quarantine?’ The choice of responses was ‘yes’, ‘no’, or ‘do not know’. A score of 1 was given for answers that indicated good behaviour, while a score of 0 was given for responses indicating bad behaviour and responses of ‘do not know’. The total score ranged from 0 to 8, with high scores indicating good behaviour.
2.6. Financial Difficulties to Follow a Regular Diet
This section consisted of four questions, which were developed by the authors, as follows: (1) ‘During the COVID-19 quarantine, did you eat fewer meals per day (fewer than three) due to food shortage at home?’ (2) ‘During the COVID-19 lockdown, did you find it difficult to eat the foods you prefer due to food shortage at home?’ (3) ‘During the COVID-19 quarantine, did you have to eat smaller meals due to food shortage at home?’ (4) ‘During the COVID-19 quarantine, did you have to eat foods that were not your favourite due to food shortage at home?’ The responses were ‘Never’, ‘Rarely’, ‘Sometimes’, and ‘Often’. The questionnaire was validated by 10 expert researchers from the Faculty of Human Sciences and Design at King Abdulaziz University.
2.7. Statistical Analysis
The data were analysed using SPSS Inc., version 26, Chicago, IL, USA. Descriptive analysis was conducted, including frequency, percentages, means, and standard deviations. Categorical data were compared using a non-parametric Chi-square test. Spearman’s correlation test was used to examine the differences between characterisations of participants and knowledge and behaviour scores. Income was divided into three groups based on a monthly salary: low (3,000–7,000), medium (7,001–20,000), and high (>20,000), to test the difficulties related to following a regular diet. To the best of our knowledge and according to the latest available data, the poverty line in Saudi Arabia is 5,000–6,000 Saudi riyals and the maximum sufficient living amount required to meet individual or household needs is 7,000 Saudi riyals [17]. All differences were considered significant if P-values were < 0.05. Cronbach’s alpha was calculated to measure the internal reliability of the questionnaire.
3. RESULTS
A total of 968 individuals completed the survey, most were aged between 18 and 49 years (84%), female (67.5%), married (65.3%), from Saudi (87.6%), and employed (48.2%). Approximately 30% of participants had secondary education or lower, 58.2% had completed their college education, and 11.8% had a postgraduate degree. Participants’ responses regarding monthly income revealed that 56.8% earned a monthly salary between 3,000–7,000, 33.7% earned between 7,001–20,000, and 9.5% earned more than 20,000 Saudi riyals (Table 1).
Table 1.
| Characteristics | n (%) |
|---|---|
| Sex | - |
| Male | 314 (32.4) |
| Female | 654 (67.5) |
| Age group | - |
| 18–29 | 276 (28.5) |
| 30–39 | 267 (27.6) |
| 40–49 | 269 (27.8) |
| 50–59 | 126 (13) |
| >60 | 30 (3.1) |
| Marital status | - |
| Single | 288 (29.8) |
| Married | 632 (65.3) |
| Divorced/Widowed | 48 (4.9) |
| Education level | - |
| High school or below | 291 (30) |
| Bachelor/diploma | 563 (58.2) |
| Postgraduate | 114 (11.8) |
| Nationality | - |
| Saudi | 848 (87.6) |
| Non-Saudi | 120 (12.4) |
| Employment | - |
| Student/unemployed | 411 (42.5) |
| Employed | 467 (48.2) |
| Self employed | 41 (4.2) |
| Retired | 49 (5.1) |
| Monthly income (RS)* | - |
| 3000–7000 | 549 (56.7) |
| 7001–<20000 | 327 (33.7) |
| >20000 | 92 (9.5) |
Nutrition-related knowledge about COVID-19 was widely spread among the choices provided; the Ministry of Health of Saudi Arabia was the major source of information, followed by television and social media accounts (Fig. 1). Table 2 presents the average scores for nutrition-related knowledge and behaviour during the COVID-19 quarantine based on participants’ age, sex, marital status, nationality, educational level, employment, and monthly income. Statistically significant differences were found among all characterisations except for nationality in relation to knowledge scores (P = 0.02; Table 2). Female participants showed a higher level of knowledge (3.15 ± 0.87) than male participants (3.02 ± 1.02; P = 0.02). Participants aged between 40–49 years had the highest knowledge scores (3.31± 0.86), while those aged 18–29 years had the lowest (2.79 ± 0.92). The average knowledge scores of divorced or widowed participants were higher than those who were single or married. These scores were significantly associated with increased levels of education and salary earned (P < 0.001 for both): participants with higher education scored 3.42 ± 0.86, while those who earned more than 20,000 Saudi riyals scored 3.29 ± 0.96.
Regarding nutrition behaviour score, statistically, significant differences were found among sex, age, marital status, nationality, employment, and income in relation to behaviour scores (P < 0.01). Female and divorced or widowed participants showed higher adherence to acceptable nutrition behaviours during the COVID-19 quarantine. Participants aged 50 years and above, as well as those who were retired (usually aged above 60 years) had higher behaviour scores than younger participants (P = 0.000002) and those who were employed (P = 0.02), respectively. The average behaviour scores of participants with a middle-level income (5.52 ± 1.23) were significantly higher than those with high- (5.43± 1.21) and low-level (5.31 ± 1.23) incomes. Among the behaviours, approximately 60% of participants reported increased fruit consumption, especially citrus fruits; 94% reported eating more homemade meals, and 82% reported no decrease in their consumption of fresh food during the COVID-19 quarantine in Saudi Arabia.
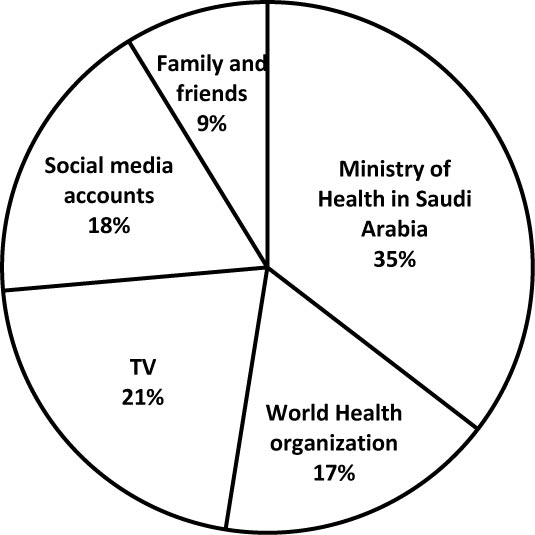
Table 3 presents participants’ responses to the four questions measuring food difficulties during the COVID-19 quarantine. Among all three levels of income, the highest percentage of participants responded ‘never’ to all four questions measuring food difficulties. However, there were statistically significant differences among the three levels of income for the following questions: ‘I ate smaller meals’, ‘I ate foods that were not my favourite’, and ‘I ate fewer than three meals’ (P = 0.01, 0.03, 0., and 0.005, respectively); however, there were no differences across income groups for ‘I did not eat my preferred food’. The results show that participants in the low-income group faced more difficulties with the availability of food sources than those with high income, since a significant number of participants in the low-income group responded with ‘sometimes or often’ to these three questions (8.9%, 9.6%, and 7.7%, respectively).
| Characteristics | Knowledge Score | P Value | Behaviour Score | P Value |
|---|---|---|---|---|
| Sex | - | - | - | - |
| Male | 3.02±1.02 | 0.02 | 5.19±1.28 | 0.0003 |
| Female | 3.15±0.87 | - | 5.49±1.2 | - |
| Age group | - | - | - | - |
| 18–29 | 2.79±0.92 | < 0.0001 | 5.11±1.30 | < 0.0001 |
| 30–39 | 3.19±0.92 | - | 5.43±1.16 | - |
| 40–49 | 3.31±0.86 | - | 5.45±1.26 | - |
| 50–59 | 3.15±0.88 | - | 5.69±1.07 | - |
| >60 | 3.30±0.87 | - | 5.86±1.07 | - |
| Marital status | - | - | - | - |
| Single | 2.78±0.97 | < 0.0001 | 5.09±1.29 | < 0.0001 |
| Married | 3.24±0.85 | - | 5.51±1.19 | - |
| Divorced/Widowed | 3.37±1 | - | 5.62±1.16 | - |
| Education level | - | - | - | - |
| High school or below | 3.01±0.94 | 0.001 | 5.41±1.21 | 0.43 |
| Bachelor/diploma | 3.10±0.91 | - | 5.41±1.26 | - |
| Postgraduate | 3.42±0.86 | - | 5.28±1.15 | - |
| Nationality | - | - | - | - |
| Saudi | 3.12±0.91 | 0.38 | 5.43±1.23 | 0.01 |
| Non-Saudi | 3.04±1.01 | - | 5.12±1.22 | - |
| Employment | - | - | - | - |
| Student/unemployed | 2.98±0.94 | 0.001 | 5.30±1.21 | 0.02 |
| Employed | 3.22±0.90 | - | 5.41±1.24 | - |
| Self employed | 3.29±0.98 | - | 5.53±1.32 | - |
| Retired | 3.08±0.86 | - | 5.85±1.06 | - |
| Monthly income (RS)* | - | - | - | - |
| 3000–7000 | 3.02±0.94 | 0.001 | 5.31±1.23 | 0.01 |
| 7001–<20000 | 3.21±0.87 | - | 5.52±1.23 | - |
| >20000 | 3.29±0.96 | - | 5.43±1.21 | - |
| - | Low (n=549) |
Medium (n=327) | High (n=92) |
P value |
|---|---|---|---|---|
| During the COVID-19 quarantine period. Did you find it difficult to eat the foods you prefer due to food shortage at home? |
- | - | - | - |
| Never | 359 (65.4) | 236 (72.2) | 71 (77.2) | 0.09 |
| Rarely | 117 (21.3) | 58 (17.7) | 14 (15.2) | - |
| Sometimes | 64 (11.7) | 31 (9.5) | 7 (7.6) | - |
| Often | 9 (1.6) | 2 (0.6) | 0 | - |
| Did you have to eat smaller meals due to food shortage at home | - | - | - | - |
| Never | 441 (80.3) | 287 (87.8) | 80 (87) | 0.01 |
| Rarely | 59 (10.7) | 29 (8.9) | 6 (6.5) | - |
| Sometimes | 44 (8) | 11 (3.4) | 6 (6.5) | - |
| Often | 5 (0.9) | 0 | 0 | - |
| Did you have to eat foods that were not your favourite due to food shortage at home | - | - | - | - |
| Never | 426 (77.6) | 275 (84.1) | 77 (83.7) | 0.03 |
| Rarely | 70 (12.8) | 36 (11) | 7 (7.6) | - |
| Sometimes | 44 (8) | 15 (4.6) | 8 (8.7) | - |
| Often | 9 (1.6) | 1 (0.3) | 0 | - |
| Did you eat fewer meals per day (fewer than three) due to food shortage at home? | - | - | - | - |
| Never | 446 (81.2) | 286 (87.5) | 84 (91.3) | 0.005 |
| Rarely | 61 (11.1) | 25 (7.6) | 8 (8.7) | - |
| Sometimes | 30 (5.5) | 10 (3.1) | 0 | - |
| Often | 12 (2.2) | 6 (1.8) | 0 | - |
4. DISCUSSION
The current study aimed to examine nutrition-related knowledge and behaviours, as well as financial difficulties among adults in Saudi Arabia during the COVID-19 pandemic. Our findings indicate that the participants have a high level of nutrition-related knowledge regarding COVID-19, which is higher among participants who were female, divorced, or widowed, and who had higher education and income levels. Moreover, the nutrition behaviour score regarding COVID-19 was higher among participants who were female, older, Saudis, retirees, divorced, or widowed, and with middle-level income. While the majority of participants across all income groups reported no difficulties in accessing food resources during the COVID-19 pandemic, low-income groups faced greater difficulties with the availability of food sources during the COVID-19 pandemic than the high-income group.
The level of nutrition-related knowledge regarding COVID-19 was widely spread among the study participants. According to a previous study, China has a high level of knowledge regarding COVID-19 transmission, prevention, and control, as evidenced by almost 90% correct responses on the knowledge survey conducted [18]. Likewise, female participants aged between 30 and 49 years, as well as those with high levels of education (master’s degree and above) were significantly associated with higher knowledge scores [18]. Additionally, Al-Hanawi et al. (2020) showed an overall high knowledge score about COVID-19 in Saudi Arabia, which included modes of transmission, clinical symptoms, treatment, risk groups, isolation, prevention, and control. Older participants, those with higher education (postgraduates) and income levels, and retirees were associated with higher knowledge scores [19]. In Jordan, a high level of knowledge about the symptoms, mortality rate, incubation period, and complications regarding COVID-19 were also reported, and the Internet and social media were reported as the main sources of information about the disease [20]. The average knowledge score about the characteristics, symptoms, prevention, and control of COVID-19 in Iran was 90%, which is also considered high [21]. Furthermore, our results showed that the Ministry of Health in Saudi Arabia was the major source for information about COVID-19 among study participants, followed by television and social media. A comprehensive campaign has been conducted by the Ministry of Health in Saudi Arabia to increase public awareness about COVID-19 and to communicate with the public via different channels, such as television. It has also aimed to provide the population with scientific information in many languages and to curb rumours that spread in the media during the pandemic. Therefore, the relatively high knowledge score among the study participants might be due to their high dependence on the Ministry of Health for information about COVID-19. Likewise, the high knowledge score in the present study might also be due to the features of the study sample as almost 70% of the sample holds a bachelor’s or diploma degree or above, which may explain the significant association between education level and knowledge score.
Regarding nutrition-related behaviours, the results of the current study showed that more than half of the study participants increased their fruit consumption, especially citrus fruits, and that almost 95% indicated eating homemade food during the COVID-19 pandemic, which is possibly due to the lockdown and closure of restaurants. Likewise, a study conducted in Indonesia showed that the majority of the study sample prepared food at home, while only 5% bought food online and 17% ate food outside their homes, even though eating out was a part of their lifestyle [22]. Previous studies in Saudi Arabia demonstrated that a high percentage of Saudis ate food outside of their homes, including restaurants and fast-food establishments, before the pandemic [23]. For instance, a study conducted in Riyadh reported that 94% of its study sample ate in restaurants, while 79% ate fast food at least once a week before the COVID-19 outbreak [23]. Previous studies conducted in Europe and Asia confirmed that eating out was positively associated with increased energy intake and consumption of fat, carbohydrates, and protein [24, 25]. Additionally, home-cooked meals were shown to be high in nutrients and fibre and lower in energy than out-of-home meals [26, 27]. Since January 2019, the Saudi Food and Drug Authority has implemented a policy to ensure that all restaurants display the calorie content of their meals on the menu [28]. Moreover, our results showed that the majority of participants believed that COVID-19 cannot be transmitted through food. This belief is in line with the reports of the U.S. Department of Agriculture and the CDC website, which state that there is no evidence confirming that COVID-19 can be transmitted through food, yet it is important to maintain a high level of food hygiene practices while handling or preparing food, including washing hands and surfaces, cooking food at the correct temperature, and freezing food immediately [29].
In the present study, we found that women had higher knowledge scores regarding COVID-19 and higher adherence to preferable nutrition behaviours during the COVID-19 quarantine period than men. This can be attributed to the high health consciousness among women, as reported by numerous studies that show sex differences in health behaviours [30]. A study involving a Finnish sample showed that women sought health-related information from various sources, such as family and co-workers, as compared to men. Additionally, women were more conscientious in buying goods and of how their choices may affect their health [31]. Furthermore, divorced and widowed participants showed a higher knowledge and behaviour score than those who were married or single, which is likely attributable to the fact that they were single parents; thus, they were more attentive to protect their families during the pandemic.
Saudi Arabia is ranked as the fifth most food secure country in the Arab countries and the 32nd most food secure country globally in the Global Food Security Index 2018 [32]. It also ranked as the 30th most food secure country in the world in 2019 [33]. The government of Saudi Arabia has applied regulations to supply food chains across the country with sufficient products. For instance, the Saudi Grains Organization stores approximately 2 million bags of wheat flour and 30% of its needs to maintain self-sufficiency in red meat [34]. Furthermore, the Saudi government imposed agricultural expertise programmes, including responsive plans for farmers, free agricultural land distribution, and intensive extension programmes, resulting in the maintenance of substantial crops of fruits, vegetables, and cereals, as well as a host of veterinary products [35]. Indeed, countries like Saudi Arabia have not experienced any food shortages during the COVID-19 crisis due to certain regulation and the support given to food supply chains across the country, which eased the process of food supplies reaching the consumer, including plans to secure food supplies quickly and reliably in case of an emergency shortage [11]. However, Saudi Arabia is highly dependent on food imports, which means food security might become a challenge in the future, especially during a pandemic such as coronavirus [32]. The findings of the present study revealed that the majority of participants indicated not having any difficulties with the availability of food sources; however, a small percentage of low-income participants faced some difficulties with the availability of food sources compared to those in the high-income group, which resulted in eating less or undesired food, as well as eating fewer than three meals a day because of the lack of food resources. Similarly, a national study reported that overall food insecurity in Saudi Arabia was 28.4% during the COVID-19 quarantine and it determined that food insecurity negatively influenced the eating habits of study participants for several reasons, including a rise in food prices, absence of grocery stores in the neighbourhood, and food unavailability in the neighbouring grocery stores and supermarkets [36]. Another study reported that the level of food insecurity in the country was 37.7% during the quarantine and concluded that food access by food-insecure participants was not affected by the quarantine [37]. Moreover, previous studies showed that lack of money was an essential indicator of the inability to eat healthy and nutritious foods [38, 39]. Additionally, in a study conducted in Vermont, 52% of the study sample indicated that they were eating less food during COVID-19, while the majority stated that having extra money (almost $106 per week) might help them to obtain their food requirements [40]. Therefore, the coronavirus quarantine might have produced some difficulties with the availability of food sources for the low-income population in Saudi Arabia.
This study has several limitations that should be taken into consideration. First, the data collection took place only in the Western region of the kingdom; however, the sample size was relatively large. Second, the survey period was early during the outbreak and lasted only six weeks, which may limit the generalizability of the results. Finally, using an online survey to collect data might introduce some bias as some people may have limited or no access to the Internet. A contribution of this study is that we used a self-reported questionnaire that focused on nutrition-related knowledge and behaviours, whereas the majority of studies regarding knowledge and behaviours regarding COVID-19 focused on the disease itself and not on its relationship with food and nutrition.
CONCLUSION
In conclusion, the current study revealed that the participants have a high level of nutrition-related knowledge about COVID-19. Additionally, sex, marital status, education level, and income level were significant predictors of knowledge level. Moreover, participants who were female, older in age, Saudis, retirees, and divorced or widowed showed higher adherence to optimal nutrition-related behaviours during the COVID-19 quarantine period. Furthermore, participants in the low- and middle-income groups faced some difficulties with the availability of food sources during the COVID-19 quarantine period, compared to those in the high-income group. These findings are beneficial for policymakers and healthcare professionals to target demographic factors such as being male, as well as having low education and income levels when designing health education programmes to enhance public knowledge regarding the COVID-19 pandemic and its prevention.
LIST OF ABBREVIATIONS
| COVID-19 | = Coronavirus Disease 2019 |
| CDC | = Centers for Disease Control and Prevention |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study design was reviewed and approved by the Unit of Biomedical Ethics Research Committee at King Abdulaziz University, Saudi Arabia (Reference No 216-20).
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Online informed consent was obtained before participants started the questionnaire.
AVAILIBILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGMENTS
We sincerely thank all participants in this study for their collaboration.

