All published articles of this journal are available on ScienceDirect.

Resuming Elective Ophthalmic Surgery during COVID-19 Pandemic
Abstract
Background:
The Coronavirus (COVID-19) pandemic has become a global health problem.
Purpose:
This paper aims to describe the practical experience of resuming elective ophthalmic surgery during the COVID-19 pandemic in a specialized eye hospital.
Methods:
A descriptive design was conducted in Middle East Eye Hospital, Ammann, Jordan. The current practices were observed to be conducted according to many evidence-based measures, including mainly the American Academy of Ophthalmology guidelines to safely resume ophthalmology service during the COVID-19 pandemic.
Results:
The main strategies that were adopted were related to patient and employee awareness and education, infection control measures, medical instruments, clinical environment, administrative control, patient screening and workflow, and quality control.
Conclusion:
We expect that these strategies could help ophthalmologists globally to resume elective ophthalmic surgery.
1. INTRODUCTION
Since the first Coronavirus disease 2019 (COVID-19) case was reported in Wuhan on December 31st, 2019, about 213 countries and territories have been affected by this virus. For this reason, the World Health Organization (WHO) has announced COVID-19 as a public health emergency of international concern and as a pandemic on January 30th and March 11th, 2020, respectively. The incidence and mortality rates of COVID-19 in September 2020 have been estimated as 3,412 cases and 112.3 deaths per one million population, subsequently. The highest number of cases were reported in the United States of America (USA), India, Brazil, Russia, and Peru [1].
COVID-19, which is also called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a new infection that affects human airways and lungs. It could be fatal when it advances to Severe Acute Respiratory Syndrome (SARS). COVID-19 spreads essentially through discharge from the nose and droplets of saliva when an infected person talks, coughs, or sneezes. It is highly transmitted from one person to another when they are in close contact (within about 1.8 meters). Moreover, it could be transmitted by touching an object or a surface that has been contaminated, and then touching the eyes, mouth, or nose. Moreover, COVID-19 may be transmitted by asymptomatic patients, which makes the control more difficult [2].
In addition to human health, COVID-19 has a significant negative impact on health services [3-5]. In many countries, the health services are partially or completely disrupted, such as with respect to cancer (49%), diabetes (49%), hypertension (53% of countries), and cardiovascular (31%) diseases [4]. Ophthalmology service is also partially or completely affected due to restrictive governmental measures [3].
The CDC advises social distancing at least 2 meters apart and short contact to avoid transmission of the virus. However, the distance between the patient and the health care professionals in ophthalmic related examination and treatment is close to 20 cm in most circumstances, and the contact duration for taking a history, measuring intraocular pressure, checking visual acuity, and waiting for pupil dilation, is more than 30 minutes [2,3,6,7].
Moreover, it is thought that the ocular surface may play a role in transmission. A prospective interventional study showed that 1 of 30 patients with COVID-19 had conjunctivitis, and RT-PCR for the tears and conjunctival secretions showed positive results [8]. Another study showed that 9 of 1099 patients with COVID-19 had conjunctival congestion [9]. A case series study showed that 12 of 38 patients with COVID-19 had ocular signs that appeared in advanced cases, such as epiphora and conjunctival congestion. These results may play an important role in increasing patient visits [10]. In spite of a low possibility of COVID-19 transmission through tears, it is still possible due to the long contact duration and close distance in the eye clinic between the patient and the healthcare professional [3,11].
For this reason, many health professional organizations, such as the American Academy of Ophthalmology (AAO), developed a comprehensive recommendation regarding how to safely resume ophthalmology service during this pandemic. These recommendations were developed for outpatient clinics and elective surgery, resuming elective ophthalmic care, scheduling or seeing patients, triage of ophthalmology patients, and environmental cleaning and disinfection [12,13]. Moreover, many studies confirmed that the ophthalmic protocol during the COVID-19 pandemic should cover patient screening and triaging, remote examination, technology adoption, personal protective equipment (PPE), clinic patient flow, and safe medical equipment [5-7,11,14-16].
Jordan is one of the developing countries in the Middle East region. The population is around 10 million. The first case of COVID-19 was registered on March 1st, 2020. In spite of restrictive governmental measures to combat COVID-19, including lockdown, technology adoption, ensuring social distancing, and mandatory screening, the number of registered cases increased to 2301 cases with an average of 225 cases and two deaths per million until September 5th, 2020 [1].
Our hospital, Middle East Eye Hospital, is a specialized eye hospital located in Amman with 15 beds. The average number of ophthalmic surgeries is 4000. Around 90% of them are elective. No elective surgeries were done during the first two months as per the health authority in Jordan.
This paper describes the practical experience of resuming elective ophthalmic surgery during the COVID-19 pandemic in a specialized eye hospital. We expect that these strategies could help ophthalmologists globally to resume elective ophthalmo- logic surgery.
2. METHODS
A descriptive design was conducted in Middle East Eye Hospital, Ammann, Jordan. The current practice was observed to be conducted according to many evidence-based measures that protect our patients, health professional, and the community in order to organize our work. These measures were developed based on health professional organizations’ recommendations, studies, policies, and procedures such as AAO [3,5,7,11-16]. It addressed hand hygiene, PPE, medical instruments, the clinical environment, patient and employee awareness and education, administrative control, and patient screening and triaging themes. However, these measures need active participation from both patients and employees.
3. RESULTS
3.1. Patient and Employee Awareness and Education
Proper awareness and education were given to our patients and employees. For our employees, a well-structured educational material was prepared and sent by email to all employees regarding the safety measures and how to screen patients. Moreover, many online courses, studies, and websites regarding reducing the risk of COVID-19 infection were sent to them and encouraged to be taken by the employees.
For our patients, adequate education and instructions were given to them by phone before coming to the hospital, including the mandatory mask-wearing, frequently performing hygiene measures, and limiting the number of companions. All patients who had appointments received an SMS message on their cell phones to ensure proper compliance with our measures. The required instructions and education will be determined based on the results of the screening that is described below.
Many posters and reminders were prepared and distributed in all areas aiming at increasing employees' and patients’ awareness and reminding them to perform the developed measures related to ensuring social distancing, as indicated in Fig. (1).
3.2. Hand Hygiene and PPE
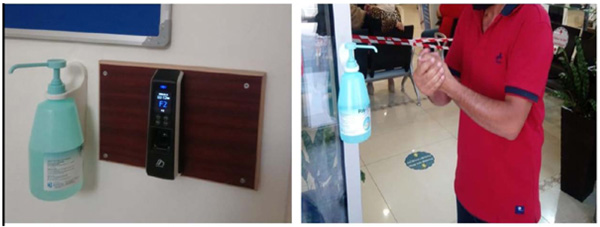
Based on many published recommendations, hand hygiene measures have been encouraged to be performed frequently: before entering the hospital, before and after patient contact, and after touching an object or a surface. In compliance with this goal, hand hygiene gels were distributed in different areas, as shown in Fig. (2).
Moreover, close monitoring of both employees and patients was conducted to ensure their compliance. Hand hygiene was considered mandatory for all patients and employees who entered the hospitals. In compliance with this, an ultraviolet (UV) Light-Emitting Diode (LED) machine was used in the hospital entrance to detect the effectiveness of hand hygiene. All patients and employees have shown their interest in seeing the result of this machine before and after hand-hygiene. Accordingly, they confirmed that hand hygiene was properly conducted.
Moreover, all patients and employees were instructed to wear a surgical mask during their stay in the hospital, while gloves, N95 masks, goggles, caps, and gowns were instructed to be used according to working areas or care steps. Table 1 summarizes the use of hand hygiene and PPE in our center.

| Health Care Professionals | Patient Protection | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Masks | Caps | Gloves | Goggles/ N95 |
Gown | H.H | Masks | Caps | Gloves | Gown | |
| Outpatient Patient Transfer During operation Clinical round Before or after examination During examination |
√ √ √ √ √ √ |
√ √ √ √ √ |
√ √ √ √ √ √ |
√ √ √ √ |
√ √ √ √ √ |
√ √ √ √ √ √ |
√ √ √ √ √ √ |
√ √ √ |
√ √ √ |
√ √ |

3.3. Medical Instruments and the Clinical Environment
Placing a protective plastic shield on slit lamps was recommended in order to decrease the risk of infection transmission between ophthalmologists and patients. For this reason, a large protective plastic shield was placed on all slit lamps in our clinic, as shown in Fig. (3). A non-contact tonometer was utilized to measure the intraocular pressure.
The distance between the patient and the health care professionals in the ophthalmic-related examination is close to 20 cm in most circumstances. For this reason, we utilized a clock to aware the ophthalmologists and patients about the duration of being in close contact. This clock has been activated immediately before giving an alarm every 30 seconds. This process may help in decreasing the contact duration and/or make the duration more separated, which may decrease the risk of being infected with COVID-19.
Moreover, the disinfection of instruments such as tonometer tip and breath shields as well as of chairs and door handles, keyboards, and desks, has been regularly performed after each patient visit. Strict sterilization was performed for contact lenses and B-scan probe. This process was performed with alcohol solutions with at least 70% alcohol. Proper ventilation has been ensured in the examination room and waiting areas.
3.4. Administrative Control
Our employees, including health care professionals such as nurses and doctors, have been distributed into small fixed teams aiming to reduce any risk of cross-contamination by working in fixed areas and/or shifts, as we can. The patient visits were scheduled in a way that prevented any crowding in the hospital.
A phone consultation or teleconsultation of another physician was encouraged if possible. If not possible, the physician examined the patient alone without any contact with the previous physician. The public cafeteria has been closed. All meetings and training courses were canceled and replaced with online meetings and training courses using many software applications, such as ZOOM Video, Inc, San Jose, CA, USA.
Moreover, all employees and patients were instructed to download the AMAN application according to the health authority’s instructions. This application shows the history of exposure and contact with any confirmed cases and the risk of this exposure.
Many isolation rooms have been prepared for any urgency, such as the development of any signs and symptoms related to COVID-19 and waiting of employees and patients with suspected COVID-19 before further management. Quarantine for 14 days has been implemented for any employee who has been in contact with a confirmed case. PCR tests have been performed within 48 hours before returning to the hospital.
3.5. Patient Screening
3.5.1. Phone Screening
All patients who had an appointment in our hospitals, including patients who required elective surgery, were screened 24 hours before coming to hospitals. The screening was performed using an evidence-based tool. Table 2 presents the main questions that have been asked in phone screening.
| S. No. | Questions |
|---|---|
| 1. | Did you download the AMAN application on your phone? If no, go to question 3 |
| 2. | Did you receive any alarms during the last 14 days? (if no, answer the other questions) |
| 3. | Did you have contact with any confirmed cases of COVID-19 during the last 14 days? |
| 4. | Did you have contact with relatives and family with confirmed COVID-19 infection during the last 14 days? |
| 5. | Do you have any of the following symptoms recently? Fever or chills, cough, loss of taste or smell, muscle or body aches, congestion or runny nose, difficulty in breathing or shortness of breath, fatigue, nausea or vomiting, sore throat, headache, and diarrhea. |
If the patients answered “Yes” to the 2nd,3rd, 4th, and 5th questions, the appointment was rescheduled after 14 days, and the phone screening has been done again. If patients answered “No” to the questions, they were instructed to come to the hospital at a predetermined time. Phone Screening is popular in many services due to its role in the early detection of patients with COVID-19. However, limited ophthalmology hospitals and clinics utilized this type of screening in our country.
3.5.2. Onsite Patient Screening
A screening area has been prepared in every hospital entrance to perform patient screening and ensure wearing the mask. The screening performed on the phone has been repeated. Moreover, the temperature was tested using an electronic thermometer that measures the temperature remotely (Fig. 4). All patients and their companions were instructed to wear surgical masks in addition to a general instruction regarding social distancing and standard precautions.
If the screening showed any remarkable results, the patients were discharged home, and the appointment has been rescheduled after 14 days.
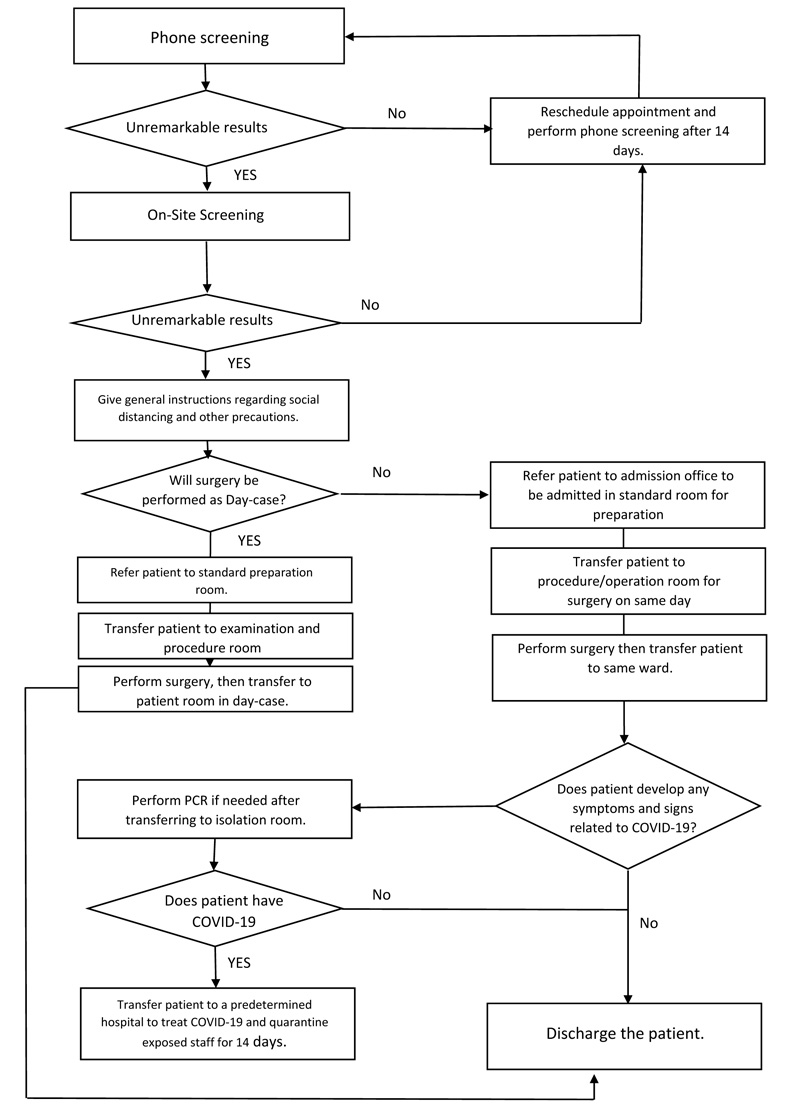
3.6. Workflow
In order to make our practice clear, a workflow was developed. This workflow describes our procedures for patients who need elective surgery during the pandemic, as shown in Fig. (5). All patients in need to be admitted into the hospital were prepared for the surgery on the same day to decrease the risk of cross-contamination.

3.7. Quality Control
The compliance with all approved measures was monitored by the quality control team and leaders through conducting regular rounds to all hospital areas, identifying gaps and challenges, preparing regular quality reports to be discussed in the online administrative meeting. These rounds play an important role in improving patient and employee safety and enhancing the patient’s experience.
4. DISCUSSION
This paper describes the practical experience of resuming elective ophthalmic surgery during the COVID-19 pandemic in a specialized eye hospital. It addressed hand hygiene, PPE, medical instruments, the clinical environment, administrative control, and patient screening and triaging, active participation from both patients and employees.
Remote awareness and education for patients and employees is considered the main strategy to combat the outbreak since COVID-19 is a new virus, and there is a lack of previous information regarding how to deal with it. It affects the compliance of patients and employees with precaution protocol, including hand hygiene and social distancing. This strategy has been implemented in many areas in health sectors, as described in the literature [3,5,7,11-16]. The remote training could be conducted via video conferences, telephone, and other e-collaborative tools. Many studies indicate that the proper education and awareness for both patients and employees play an important role in increasing their commitment to the organization and enhancing their outcomes and satisfaction [17-19].
Safe medical instruments and healthy clinical environment are also one of the main strategies to combat the outbreak since the distance between the patients and the health care professionals is very close [12,13,16]. The use of the clock in addition to a protective plastic shield on slit lamps may help to minimize the close contact duration and/or make the length of the contact more separate, which helps lower the chance of getting infected with COVID-19. However, the measurement of its impact is very difficult.
The use of a standardized screening tool and workflow is important to enhance the compliance and quality of care during this outbreak [3,5,7,11-16]. Many studies have shown the adoption of a structured tool to follow and screen the patients, increasing the patients’ centered care and reducing missed care and malpractice, as well as decreasing the staff’s workload, thus enhancing the satisfaction [20-22].
This paper shows the important role played by health managers and quality team in care coordination, staffing, ensuring a safe environment, utilization of resources, and following the staff and patients' compliance and engagement [23]. For this reason, each hospital management has to make sure that all managers and quality teams have high qualifications and awareness regarding crisis and risk management. Finally, the paper has shown how the adoption of e-health strategies is a main factor to decreasing social distancing and improving patients' and employees' awareness and quality of care, which has also been supported by many previous studies [5,24].
However, the adoption of technology and e-health applications, such as telemedicine, teleconsultation, and e-learning, is not well implemented due to the absence of required infrastructure and lack of acceptance from both employees and patients. COVID-19 is a new virus, and there is a lack of previous information regarding how to deal with it. So, the continuous updates from health organizations and health authorities in Jordan regarding safety measures make the implementation of measures more difficult.
Many recommendations could be concluded, such as the following:
- Adoption of lean and supply chain thinking for disaster management.
- Proper education and training of health care providers and patients regarding how to utilize the e-health application in control and management of e-health.
- There is a need to include e-health applications within national and international disaster plans.
- Sufficient funding to improve the infrastructure of health organizations toward medical equipment and e-health, as well as provision of related training and education.
- Supporting effective collaboration between all stakeholders to increase the flexibility of strategies.
CONCLUSION
In the context of the COVID-19 pandemic, we have discussed important strategies for healthcare administrators in ophthalmology and how these strategies have been or must be implemented. The primary emphasis is absolutely on restricted infection measures and ensuring proper participation from both patients and employees. Moreover, many strategies have been developed to safely conduct elective ophthalmic surgery, thereby maintaining public confidence and implementing safe practice in elective surgery through balancing the required measures in this pandemic.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval is not applicable as this is a discussion paper.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants for publishing the images in the study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank the staff in Middle East Eye Hospital, Amman, Jordan, for their help and cooperation. The authors present their special gratitude to Dr. Mousa Bydoon, General Manager and Consultant Ophthalmologist at Middle East Eye Hospital, for his endless support and help.

