All published articles of this journal are available on ScienceDirect.

Determinants of Overweight and Underweight among Children under 5 in Kazakhstan
Authors Info & Affiliations
Abstract
Background:
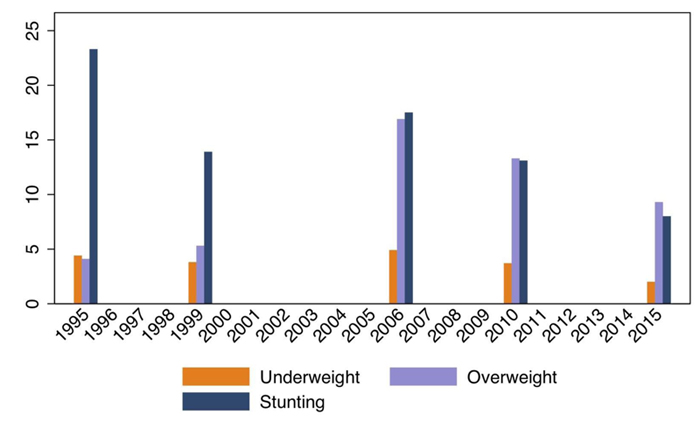
During the last 10 years, the prevalence of underweight has decreased considerably in Kazakhstan and, nowadays, it is set under 3% for children under 5 years old. However, the prevalence of overweight, which was not important at all in the 90s, is reaching 10% for children under 5 nowadays. This means that there is a co-existence between being underweight and overweight in the same country and, in some cases, within the same region. In order to design policies addressing both problems and avoiding policies, which may solve underweight but worsening overweight, and vice versa, the aim of this paper is to analyse the socioeconomic determinants of the two problems.
Methods:
We estimate the probability of occurrence using the Multiple Indicator Cluster Survey (MICS) collected by the United Nations Children’s Fund (UNICEF) and Agency of Statistics of the Republic of Kazakhstan for the years 2006, 2010-2011 and 2015. This survey includes a questionnaire for children younger than 5 years old containing information on maternal and child health. We consider that a child is overweight if she/he falls over two standard deviations of the World Health Organization standards (WHO) for her/his age. Similarly, we consider that a child is underweight if she/he falls below the two standard deviations of the WHO standards.
Results:
Children of mothers with higher education have a higher probability of being overweight (6,8%) and less probability of being underweight (-5,5%). This effect disappears for children older than 2 years old. Children of Russian origin and other ethnic groups show a lower probability of being overweight in comparison with their Kazakh peers. Being born in the highest wealth quintile reduces the risk of a child under 2 years old being underweight (-2,9%). On the other side, children in rich families at age 2-4 years old have a higher probability of being overweight (3,7%).
Conclusion:
Health policy aimed to improve family and institution´s knowledge on child nutrition could be effective measures to reduce infant overweight.
1. BACKGROUND
During the last 10 years, the prevalence of underweight has decreased considerably in Kazakhstan and, nowadays, it is set under 3% for children under 5 years old. However, the prevalence of overweight, which was not important at all in the 90s, is reaching 10% for children under 5, nowadays (Fig. 1). This means that there is a co-existence between being underweight and overweight in the same country and, in some cases, within the same region.
In order to assess if the determinants behind the reduction of underweight are the same as those behind the increase of overweight, this paper aims to analyse the socio-economic determinants of the two problems. The results of the paper will allow us to design policies addressing both problems, which may only resolve problems related to being underweight but worsen those regarding overweight, and vice versa.
In order to assess the factor behind underweight and overweight, first, we review the literature analysing each of the problems. Subsequently, we present the methodology and database. Results are analysed and we draw some conclusions in the last section.
2. LITERATURE REVIEW
Although overweight and underweight keep coexisting in many middle- and low-income countries, the determinants behind each of the problems may be different [1]. Early-life determinants of overweight and underweight among children can be grouped into three types of factors: individual, household-family and environmental (society).
Individual explanatory variables of child overweight include birth weight, height, growth and infant feeding. Most of the studies confirm the positive association between birth weight, size and infant growth and the risk of having an infant and child obesity among children from Hong Kong [2] and Mexico [3]. However, the low weight at birth can have the opposite effect. The article of Ibáñez et al. [4] revealed that children with low birth weight then tend to gain weight more rapidly, which may later lead to more abdominal fat and body adiposity. The evolution of the first month's weight can depend on the children's nutrition. Actually, breastfed children have less probability of being overweight in comparison to their peers exclusively formula-fed [5, 6].
The family unit and parents provide a physically protective environment for children and it affects their healthy or unhealthy lifestyle. Eating behaviour and habits, active lifestyle, and sleeping patterns are developed and shaped mainly by parents. Education influences the decisions of the main caregiver regarding diet, lifestyle problem-solving capacity and values of the child. In this line, maternal education is considered as one of the most relevant explanatory indicators from a public policy perspective because of the major influence of maternal health and behaviours on child health [7]. To have a mother with higher education has been linked with a reduced likelihood of being overweight among children during early childhood in some European populations [8]. Maternal education reduces obesity and overweight by approximately 3% for children 4-6 years old in Sweden and the UK but increases them by 0.3% in China. Results demonstrated a positive, although small, relationship between mother’s education and child obesity and overweight for rural areas of China. However, being underweight was strongly associated with maternal education in the same study, reducing the prevalence of those underweight almost by 20%. Maternal education reduces stunting and underweight of 4-year-old to 6-year-old children in rural areas of different countries [9].
Mother’s education can be correlated with the risk of her child being overweight and underweight throughout the period of her employment. The study of McDonnell and Doyle [10] suggests that maternal employment of highly-educated mothers and formal and informal child care may increase the probability of a child to be overweight almost to 8%. This effect is insignificant for low-educated mothers. The authors argue that the lack of high-quality child care and favourable labour and social policies might affect the weight of children for households with high socioeconomic status. Another reason for the negative impact of maternal employment on child weight is the traditional gender role implying that child care and meal preparation are solely the women's responsibilities [11]. Moreover, less time devoted to child care by working women usually is a little offset by the husband or partner [12]. Mindlin, Jenkins, and Law [13] analysed major studies from developed countries and concluded that maternal employment increased the risk of being overweight for children with a bigger impact on children from high income groups. The reason may be the higher use of informal child care and the unavailability of good quality formal child care. Lin et al. [14] in Hong Kong study revealed that informal child care led to higher levels of childhood obesity. The article by Maher et al. [15] also found the negative impact of informal child care on children’s health, especially on the risk of being overweight. Moreover, children under the care of grandparents [16]; and three-generation families [17] are more likely to contribute to childhood overweight.
Family lifestyle and parents’ behaviour may have an important effect on the risk of being overweight [18]. The study of Greek pre-schoolers demonstrated that the 3-5 years old children have a 1.79 times higher risk of being overweight if their mothers were active or passive smokers during the pregnancy. Additionally, father’s obesity increases the risk of child overweight significantly [6]. Wake et al. [19], in the study of Australian children, observed that fathers' but not mothers' permissive and disengaged parenting styles were associated with increased risks of pre-schoolers being overweight and having obesity. Hence, nutrition, physical activity, and parental behaviour play an important role in the risks of being overweight and underweight for children.
Children of some ethnicities have a higher prevalence of being overweight. Early maternal age, maternal pre-pregnancy body mass index, BMI [20], and parental feeding styles [21] of different ethnic groups can be among the explanatory factors contributing to ethnic differences of child overweight. For example, European American parents pressurize their children to eat, which tends to cause the child to be overweight compared with Hispanic and African American families [22]. As well, the perception of normal BMI can vary among different ethnic groups and in some cases, it may be associated with family’s wealth [23].
On the other hand, the main determinants of underweight children under 5 years old are socioeconomic status, low birth weight, mothers’ age at marriage and family size. Family income is also a especially important variable when we analyse overweight. The risk of being underweight is four times higher for children under 5 years old from poor socioeconomic status in comparison with their peers from wealthier socioeconomic status in Nepal. The socioeconomic status was measured by the proxy of food self-sufficiency, land holding of family and housing standard [24]. The study of children aged 5 in Kenya revealed that underweight were detected among children introduced to foods at an early stage (before 6 months) or who had an illness in the past month [25].
Various studies have discovered the array of factors for the risks of being underweight for children aged 5 years or below. Yet, the most common factor found by scholars is household wealth and/or income. Chalasani and Rutstein [26], in their study of Indian children, found that the relationship between household wealth and malnutrition became stronger over time for boys and particularly for girls in urban and (especially) rural areas. The study conducted by Guyatt et al. [27] also revealed that being in a poor household was an important factor leading to underweight and stunting among children under 2 years of age in Kenya. Guyatt et al.’s [27] research highlighted that the low birth weight significantly affected the risks of being underweight for children. Overall, socio-economic status had an impact on household food security and, subsequently, the health of children.
However, there are other factors other than household wealth that affect the risk of being underweight. The investigation of Pakistani children found that BMI of mother, mothers’ age at marriage, child’s size at birth and antenatal clinic visits also were also important predictors [28]. Additionally, there are studies that argue that family size has an important effect on children being underweight. Wu and Li [29], in their study, found the impact of one-child-policy in China that families with one child had a lower probability of being underweight. The strictly imposed one-child policy in China decreased competition for food in families. However, Wu and Li [29] observed that the increased access to food led to the increased problem of obesity and being overweight. Similarly, the study conducted in India by Rana et al. [30] found that women with a higher number of births and among those with first-order births with fewer than 2 years between marriage and first birth, the risk of being underweight and having anemia were significantly higher compared with their counterparts. Hence, the literature shows the importance of health-demographic factors, such as BMI of mother, family size and mother’s age for the risk of being underweight.
3. METHODS
We will consider that a child is overweight if she/he falls over two standard deviations of the World Health Organization standards (WHO) for her/his age. Similarly, we consider that a child is underweight if she/he falls below the two standard deviations of the WHO standards. Assuming a logistic functional form:

We estimate two different models: (a) yi takes the value 1 if the child is overweight with the probability p and 0 otherwise with the probability (1 - p), and (b) yi takes the value 1 if the child is underweight with the probability p and 0 otherwise. We will consider the same factors (X) in both models in order to identify if they have the same or opposite effects in overweight and underweight children.
We estimate the probability of occurrence using the Multiple Indicator Cluster Survey (MICS) collected by the United Nations Children’s Fund (UNICEF) and Agency of Statistics of the Republic of Kazakhstan for the years 2006, 2010-2011 and 2015.1 The sample is designed to be represented from Kazakhstan's population by region, putting special effort to make rural areas representative. From this household sample, women aged 15-49 years and children under 5 years old were eligible to respond to extra questionnaires containing information about maternal and child health. Our sample consists of the pool of all eligible children under 5 years all from the 2006, 2010-2011 and 2015 surveys, using the sample weight adjusted for kids under 5 weights (provided by MICS) to make them representative. Once we had the pool of kids to be analysed, we classified them as overweight, underweight, or to be under standard parameters using the WHO tables for each age as mentioned at the beginning of the section.
In Table 1, we show the main descriptive statistics of our database. On average, 13.4% of children suffer overweight, whereas the percentage of underweight children under five years old is much lower, around 3% of total observations. The mean age of the children analysed is 1.96, living in households with 5.66 people on average. The observed households showed a higher percentage of mothers with education than the household head, especially when referring to higher education (33.8% vs 23.8%).
1 This survey is part of a UNICEF programme that has been done for different countries in collaboration with the national governments. The program is currently operating in about 90 developing countries.
Ethnic diversity is also important in Kazakhstan. Although Kazakhs are the major ethnic group with 73% of the population, Russians still keep an important share of 14%. Other ethnicities, such as Ukrainian, Uzbek, German, Tatar, and Uygur, represent more than 12%. On average, the population lived slightly more in urban areas than rural during the period, although the population in rural areas decreased during the whole period. The MICS database calculates a wealth index and provides an criterion indicating to which wealth quintile the household belongs to. However, our sample includes just the households that have children younger than 5 years old, and descriptive statistics show that richer families have less children, 18.2% of families being with children under 5 relative to 22.9% families with low income.
4. RESULTS
Estimation of the marginal effects, i.e. the probability that a child under five is overweight or underweight in Kazakhstan, is shown in Table 2. Since determinants of overweight and underweight may be different depending on the age of the child, we also made separate estimations for children younger than 2 years old and children aged between 2 and 4 years old. Actually, some variables seem to act in opposite directions depending on the age, such as the age of the child has a positive effect on the probability of being overweight for children under 2, however, it turns out to be negative for children aged between 2 and 4 years old. Moreover, it is negative for underweight children under 2 years of age.
| - | Observations | Mean | SD | Min | Max |
|---|---|---|---|---|---|
| Overweight | 14,463 | 0.134 | 0.340 | 0 | 1 |
| Underweight | 14,463 | 0.033 | 0.180 | 0 | 1 |
| Age | 14,463 | 1.964 | 1.395 | 0 | 4 |
| Household size | 14,463 | 5.660 | 2.119 | 2 | 19 |
| Househouls head level of education | - | - | - | - | |
| Lower Secondary and primary | 14,463 | 0.113 | 0.315 | 0 | 1 |
| Upper Sec | 14,463 | 0.376 | 0.484 | 0 | 1 |
| Technical | 14,463 | 0.273 | 0.446 | 0 | 1 |
| Higher | 14,463 | 0.238 | 0.426 | 0 | 1 |
| Mother level of education | - | - | - | - | - |
| Lower Secondary and primary | 14,463 | 0.044 | 0.208 | 0 | 1 |
| Upper Sec | 14,463 | 0.336 | 0.472 | 0 | 1 |
| Technical | 14,463 | 0.282 | 0.450 | 0 | 1 |
| Higher | 14,463 | 0.338 | 0.473 | 0 | 1 |
| Wealth index quintil | - | - | - | - | - |
| Poorest | 14,463 | 0.229 | 0.420 | 0 | 1 |
| Second | 14,463 | 0.209 | 0.407 | 0 | 1 |
| Middle | 14,463 | 0.209 | 0.407 | 0 | 1 |
| Fourth | 14,463 | 0.171 | 0.377 | 0 | 1 |
| Richest | 14,463 | 0.182 | 0.386 | 0 | 1 |
| Ethnicity | - | - | - | - | - |
| Kazakh | 14,463 | 0.737 | 0.440 | 0 | 1 |
| Russian | 14,463 | 0.143 | 0.350 | 0 | 1 |
| Other eth. | 14,463 | 0.120 | 0.325 | 0 | 1 |
| Urban | 14,463 | 0.502 | 0.500 | 0 | 1 |
| Rural | 14,463 | 0.498 | 0.500 | 0 | 1 |
| - | Overweight | Underweight | |||||
|---|---|---|---|---|---|---|---|
| - | Younger than 5 | Younger than 2 | 2-4 year old | Younger than 5 | Younger than 2 | 2-4 year old | |
| Age of child (months) | -0.001*** | 0.004*** | -0.002*** | -0.000*** | -0.003*** | 0,000 | |
| Number of HH members | 0.000 | 0.004 | -0.003 | 0.000 | -0.001 | 0.001 | |
| Mother level of education | - | - | - | - | - | - | |
| Primary/Not Completed Secondary | Reference | Reference | Reference | Reference | Reference | Reference | |
| Completed Secondary | 0.019 | 0.016 | 0.025 | -0.014 | -0.038 | 0.001 | |
| Secondary specialized | 0.029* | 0.049** | 0.015 | -0.022* | -0.039* | -0.012 | |
| High | 0.029* | 0.068*** | 0.006 | -0.026** | -0.055** | -0.008 | |
| Head of the household level of education | - | - | - | - | - | - | |
| None/Primary/Some Secondary | Reference | Reference | Reference | Reference | Reference | Reference | |
| Completed Secondary | -0.021* | 0.010 | -0.038*** | 0.011** | 0.014 | 0.008 | |
| Secondary specialized | -0.020 | -0.009 | -0.023 | 0.004 | 0.004 | 0.003 | |
| High | -0.022* | -0.015 | -0.023 | 0.009 | -0.002 | 0.014* | |
| Wealth quintile | - | - | - | - | - | - | |
| Poorest | Reference | Reference | Reference | Reference | Reference | Reference | |
| Second | -0.013 | -0.022 | -0.010 | -0.006 | -0.005 | -0.007 | |
| Middle | -0.010 | -0.039** | 0.009 | -0.010 | -0.011 | -0.007 | |
| Fourth | 0.018 | 0.015 | 0.020 | -0.007 | -0.021* | 0.005 | |
| Richest | 0.018 | -0.014 | 0.037** | -0.014** | -0.029*** | -0.003 | |
| Ethnicity | - | - | - | - | - | - | |
| Kazakh | Reference | Reference | Reference | Reference | Reference | Reference | |
| Russian | -0.028*** | -0.010 | -0.038*** | -0.001 | 0.000 | -0.001 | |
| Other Ethnic | -0.022** | -0.002 | -0.035*** | -0.003 | -0.005 | -0.003 | |
| Rural/Urban | - | - | - | - | - | - | |
| Urban | Reference | Reference | Reference | Reference | Reference | Reference | |
| Rural | 0.010 | 0.005 | 0.012 | -0.003 | -0.006 | 0.001 | |
| Psedo R2 | 0.031 | 0.037 | 0.038 | 0.044 | 0.080 | 0.048 | |
| Observations | 14318 | 5750 | 8568 | 14617 | 5852 | 8765 | |
| Notes: Coefficient estimates. Significance levels: *** p<0.01 ** p<0.05 * p<0.10. Year and regional dummies included. | |||||||
Mother’s education appears to be more relevant than the educational level of the household head. However, head of households with upper secondary education decreases the risk of children being overweight by 3.8% relative to lower levels of education for children aged 2-4 years old. Instead, maternal education affects both overweight and underweight, in particular, for children younger than 2 years old, although in opposite directions: children of mothers with higher education have a higher probability of being overweight (6,8%) and less probability to be underweight (-5,5%).
Wealth index shows a similar effect than maternal education, increasing the probability of being overweight (3,7%) and decreasing the probability of being underweight (-2,9%) for children living in the richest households. Nevertheless, the wealth effect on overweight is significant in the case of children aged between 2 and 4 years old. The wealth index is inversely associated with underweight for children under 2 years old.
Household behaviour, habits and lifestyle are also important for explaining overweight and underweight. We attempt to approximate this effect through ethnicity. Children of Russian origin and other ethnic groups show a lower probability of being overweight in comparison with Kazakh peers.
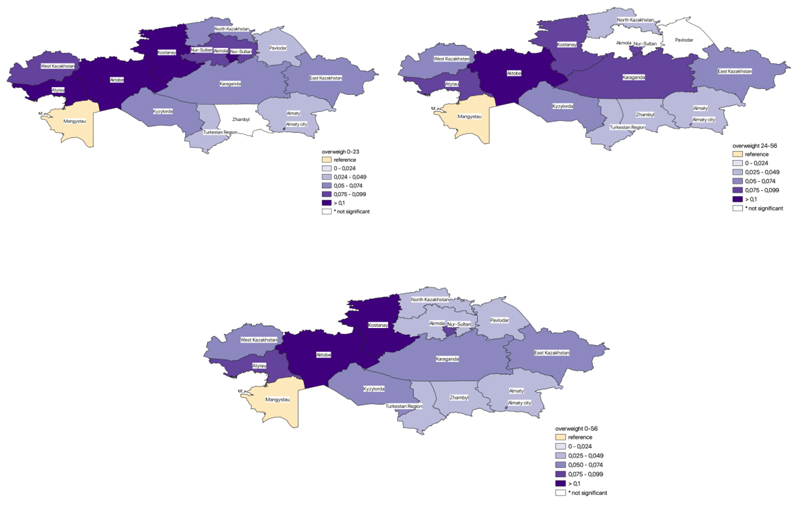
The numbers of household members, breastfeeding and rural/urban variables are not significant in prediction of being overweight or underweight. Regional disparities analysis discovered the prevalence of overweight in the West of Kazakhstan (Fig. 2). Interestingly, Aktobe region has more than 10% higher probability of being overweight for children 2-4 years old in comparison with the lowest overweight region (Mangistau). There are more regions with significant overweight among children until 2 years old than from 2 to 4 years old.
Children with the highest risk of underweight from 0 to 2 years old are located in Almaty oblast. The region of Almaty is characterized by a high pollution level. Despite its economic value for the country, the health expenditure for Almaty oblast is among the lowest in Kazakhstan. Aktobe also has a high risk of children underweight from 2 to 4 years old. Actually, Aktobe is the region with the highest risk of both, overweight and underweight, which is remarkable in a sense. To get a full credible explanation of the obtained results, further research should be carried out with similar estimates at the oblast level with the following comparison between regions (Fig. 3).

CONCLUSION
During the last 10 years, the prevalence of underweight has decreased considerably in Kazakhstan and, nowadays, it is set under 3% for children under 5 years old. However, the prevalence of overweight was not important at all in the 90s, reaching 10% of children under 5 nowadays. This means that there is a co-existence between underweight and overweight in the same country and, in some cases, within the same region.
Maternal education is inversely associated with being underweight, thereby reducing the risk of being underweight for children under 2 years old. At the same time, the higher education of mothers increases the risk of being overweight for children before 2 years old. Results suggest that higher education might affect infant diet leading to excessive weight gain. Further research is needed to find a casual relation between mother’s education and overweight and underweight.
The probability of being overweight also increases for the wealthiest quintile 5th. It seems that richer families give larger quantities or food with more sugar and fat to the children.
Ethnicity can reflect family lifestyle, eating habits and behaviours, which shape the child's diet. Study findings suggest that children of Kazakh families are more likely overweight.
The study suggests a considerable geographical variability of underweight and overweight prevalence in Kazakhstan. Aktobe is the region with the highest prevalence of overweight and underweight at the same time. The Mangistau region has the lowest risk of child overweight which can be explained by the fish-rich diet.
NOTES
1 This survey is part of a UNICEF programme that has been done for different countries in collaboration with the national governments. The program is currently operating in about 90 developing countries.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the UNICEF-MICS at: https://mics.unicef.org/surveys, reference numbers Kazakhstan-MICS3, Kazakhstan-MICS4, Kazakhstan-MICS.
FUNDING
This study was supported by the Science Committee of the Ministry of Education and Science of the Republic of Kazakhstan throughout the project “Healthy Childhood and Socio-Economic Status in Kazakhstan” for 2018-2020 (AP05135896).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Authors wish to acknowledge the support of the Science Committee of the Ministry of Education and Science of the Republic of Kazakhstan.

