All published articles of this journal are available on ScienceDirect.

Knowledge of Children’s Caregivers Regarding Malaria within Vhembe District of Limpopo Province: A Cross-Sectional Study
Authors Info & Affiliations
Abstract
Background:
The high rate of malaria in the province has negatively impacted the department financially since medicines for malaria treatment are scarce and expensive. Many of the families live near the streams, and they are uninformed about malaria’s clinical manifestations and preventive measures.
Aims:
This study aimed to assess caregivers’ knowledge about malaria in children of selected villages within the Limpopo province of South Africa.
Methods:
Using a cross-sectional study design, this study was conducted in villages surrounding the Vhembe district of Limpopo province. A structured self-administered questionnaire was used to collect data. The data were analysed using descriptive statistics. This study included 80 caregivers of children under 12 years of age.
Results:
It was found that approximately 85% of caregivers knew about malaria’s clinical manifestations and prevention measures.
Conclusion:
Community health care workers can improve the knowledge of caregivers by strengthening health education and preventive campaigns.
1. INTRODUCTION
Malaria is a life-threatening disease caused by parasites transmitted to humans through the bite of the Anopheles mosquito, a female mosquito. Malaria is a common communicable infection in hot tropical areas and rarely occurs in areas of moderate temperature [1]. The disease is associated with fever, headache, chills, shivering and loss of appetite, general body weakness, and joint pains [2]. Once an infected mosquito bites a human being and transmits the parasite, it multiplies in the host liver and destroys red blood cells.
Malaria is a very serious disease that can be cured if an individual is tested, diagnosed, and treated immediately. Malaria can be suspected based on the individual travel history, symptoms, and the physical findings at examination [3]. However, for a definitive diagnosis to be made, laboratory tests must demonstrate the malaria parasites or their components [3]. World health officials are trying to reduce the incidence by distributing bed nets to help protect people from mosquito bites. In certain countries, malaria control teams conduct house to house spraying once a year in areas prone to malaria with chemicals that kill mosquitoes; however, in some countries, this preventive measure is not taken [4].
Reducing malaria morbidity and mortality in children greatly depends on the caregiver’s knowledge about malaria regarding causes, symptoms, prevention, and management [5]. Adequate knowledge of caregivers regarding the symptoms of malaria has implications for prompt seeking and preventions of progression of uncomplicated malaria to severe morbidity and mortality [6]. In some areas, caregivers lack knowledge about malaria. Therefore, caregivers require adequate education about malaria symptoms, prevention, and management to prevent high death rates, especially in children [4].
Nearly half of the world’s population is at risk of malaria, and in 2015, roughly 212 million malaria cases and an estimated 429 000 malaria deaths were reported [7]. According to WHO [1], increased prevention and control measures have led to a 29% reduction in malaria mortality rates globally since 2010. Sub-Saharan Africa (SSA) continues to carry a disproportionately high share of the global malaria burden. In 2016, there were 90% of malaria cases, 92% of malaria deaths, and 91 countries and areas had ongoing malaria transmission [1].
In all malaria-indigenous countries in Africa, 25–40% of all outpatient clinic visits and hospital admissions are for Malaria [1]. According to Greenwood et al. [8], late presentation results in high case-fatality rates, inadequate management, and unavailability or stock-outs of effective drugs. Malaria is also a significant contributor to deaths among hospital inpatients.
Malaria is a major killer disease of children, especially in sub-tropical areas; it is one of the leading causes of avoidable deaths, especially in children and pregnant women [1]. It is an acute tropical protozoa disease that is a major health hazard in developing countries [2]. Knowledge thereof is regarded as the multidimensional phenomenon determined by the interplay of five factors: causes, diagnosis, transmission, effective prevention, and curative aspects [2].
WHO [1] indicated that in Africa, around 40% of malaria deaths occur in just two countries which are Nigeria and the Democratic Republic of the Congo (DRC). Malaria is the leading cause of morbidity and death in children in DRC, accounting for an estimated 40% of outpatient visits and 40% of overall mortality. However, in Nigeria, it contributes an estimated 11% of mortality [1]. There are an estimated 100 million malaria cases, with over 300,000 deaths per year in Nigeria [9]. Similarly, in Mozambique, the statistics showed approximately 45% of cases in outpatient visits, 56% of inpatient at pediatric clinics, and 26% of all hospital deaths [9]. According to Teklemariam [10], the prevalence of malaria among children is 46.3% in rural areas compared to 16.8% in urban areas. Out of a population of 17 million, the country recorded almost 7 million cases of malaria in 2013, especially in the rainy season from August to November [9]. In the neighboring countries, malaria cases are recorded in Mozambique, Malawi, Botswana, Namibia, Zambia, and Zimbabwe, including Victoria Falls, Harare, and Gweru, as indicated by Chukwuocha et al. [11].
South Africa is no exception; there is a high rate of malaria transmission, especially in the north-eastern parts of Limpopo (along with the borders with Mozambique and Zimbabwe), the low-lying areas of Mpumalanga (including the Kruger National Park), Nelspruit and Mbombela, and the far northern parts of KwaZulu-Natal province [12]. Most malaria cases treated in South Africa have a history of travel to Mozambique, so preventative measures should include preventing mosquito bites and preventative medication.
The Mopani District in Limpopo province is also an area known to be at high risk regarding malaria infection and experiences abrupt malaria cases, but the number of cases has now decreased as the weather temperatures reduce [13]. According to the statistics of the hospitals in Mopani and Vhembe District, it was reported that most people suffer from malaria. The Limpopo Department of Health [14] statistics reported 4092 malaria cases and 33 deaths from these districts.
According to WHO [15], currently, there is an outbreak of malaria in South Africa, especially in Limpopo Province, due to the long-term heavy rain in the past few months. The Limpopo Department of Health confirmed an increase in the number of malaria cases and deaths, with 4 092 cases and 33 deaths reported by March 2017 compared to 1 543 cases and 18 deaths in the 2015/16 season. Earlier in 2017, the department also recorded 43 cases in the Waterberg region, and more than 600 malaria cases were reported around the province the same year [15]. The alarming statistics prompted the researchers to assess whether caregivers of villages around the Vhembe District have adequate knowledge regarding malaria amongst their children.
Therefore, there is a concern about the high rate of malaria infections in the province, which has financially affected the department as malaria treatment medication is scarce and expensive [13]. Limpopo MEC of health confirmed that about 624 malaria patients were admitted to hospitals around the province, and amongst these patients, the majority of them were children. Hospitals reported most malaria cases included Siloam near Makhado, Donald Fraser in Thohoyandou, Malamulele in Vhembe, and Nkhensani hospital in Giyani [13].
The study was conceptualized after the malaria outbreak in Limpopo province due to the recent heavy rainfall in areas around the Vhembe district, which also affected most of the villages in this vicinity [13]. Twenty-six (26) malaria cases in 2017 were documented, as reported in a study [11]. Children suffering from malaria are usually observed playing outdoors till late, wearing short clothes [12]. Anecdotally, areas, such as dumping sites, lakes, and ponds, where animals drink water are found to be the breeding places for mosquitoes. Most of the families around the villages are located near the streams, and most of them lack knowledge regarding malaria. Therefore, this study aimed to assess the knowledge of caregivers of children regarding malaria in children at selected villages within the Vhembe district of Limpopo province, South Africa.
2. RESEARCH DESIGN AND METHODS
The study adopted the quantitative research approach, and the cross-sectional descriptive survey was used for this study. A cross-sectional survey refers to a study conducted at one point in time. The study design was found to be appropriate given that the study sought to determine the level of knowledge regarding malaria in children.
2.1. Study Setting
This study was conducted in villages around the Vhembe district of Limpopo province. The villages were selected considering the hot and rainy seasons favourable for malaria and the exposure of individuals to a high risk of malaria. Consequently, in these villages, there are a variety of ponds where animals drink water. These ponds are made because of heavy rainfall experienced by these villages during summer, resulting in stagnant water, which is a favourable breeding area for mosquitoes.
2.2. Study Population and Sample
The population consisted of all the caregivers who lived in villages around the Vhembe district in Limpopo Province, South Africa, while the sample of this study consisted of caregivers of children under 12 years residing within the same district. Cluster sampling was used to select three villages within one municipality of the Vhembe district that was randomly selected using simple random sampling. The total population of identified caregivers was 100, and the sample size was 80 caregivers calculated using the Raosoft sample size calculator.
2.3. Research Instrument
A structured self-administered questionnaire was used to collect data. The questionnaire incorporated sections A and B. Section A sought the respondent’s demographic information. Section B consisted of questions related to knowledge regarding malaria clinical manifestations and preventive measures. The instrument was prepared in English and translated into TshiVenda and XiTsonga, the local languages used in villages around the Vhembe district, and later back-translated into English.
2.4. Data Collection
The researchers visited the household of selected caregivers for data collection. A researcher-administered questionnaire was used to assess the knowledge of caregivers regarding malaria in children. The researchers administered questionnaires at the homes of the selected respondents who gave consent to participate in the study, and the process took about 30 minutes for each respondent. Data were collected from May 2017 to July 2017.
2.5. Data Analysis
Descriptive statistics were used to analyse data through frequencies and percentages. Responses were presented through tables and pie charts using SPSS version 25.0.
2.6. Ethical Consideration
Ethical clearance was granted by the University of Venda Health Clinical Trial Research Ethics Committee (PROJECT NO: SHS/17/PDC/29/3108), and permission to conduct the study was also sought from and granted by the Vhembe district Department of Health. The researcher also ensured anonymity and confidentiality while protecting human rights
3. RESULTS
3.1. Socio-Demographic Characteristics of the Caregivers
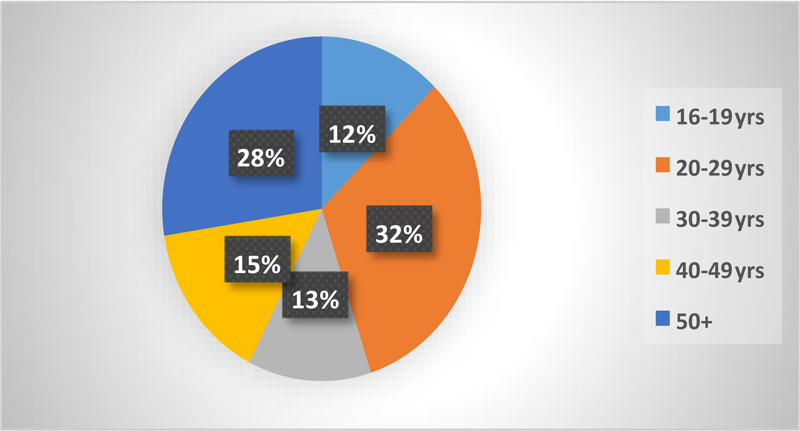
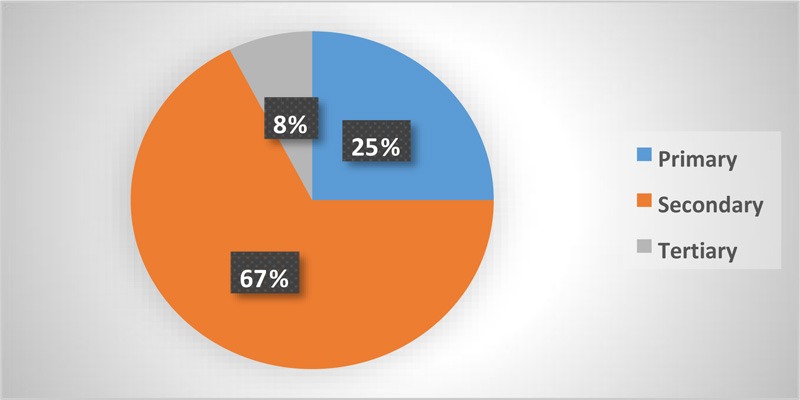
Figs. (1 and 2) present the caregivers’ demographic characteristics, including age and level of education, respectively. About 32% (n=26) of caregivers were aged 20-29 years, 28% (n=22) aged 50 years and above, and 15% (n=12) aged 40-49 years. Most of the caregivers (67%, n=54) had secondary level of education followed by primary level (25%, n=20), with the minority of the caregivers having studied up to tertiary education (8%, n= 6).
3.2. Knowledge of Caregivers Regarding Malaria and its Preventive Measures
It is evident from Table 1 that 85% (n=68) of caregivers know about malaria. This implies that the majority of caregivers have heard about malaria. The main source of information was found to be mainly from media (radio/TV) (62.5%, n=50) followed by health care providers (30.0%, n=24). Caregivers (77.5%, n=62) also reported knowing about the causes of malaria, and about 85% (n=70) acknowledged the seriousness of malaria. Mosquitos as the primary mode of transmission of malaria were recognized by 87.5% (n=70).
The findings revealed that about 80% (n=64) of caregivers knew the clinical manifestations of malaria, and the most endorsed clinical manifestations included fever and headache (84.4%, n=54) followed by vomiting (46.9, n=30). Most caregivers indicated that the step taken after noticing the above indicated clinical manifestations was to visit the hospital for treatment (62.5%, n=50) followed by visiting the hospital after the failure of self-medication (22.5%, n=18). About 92.5% (n=74) of caregivers reported that they knew about the preventive measures of malaria.
| Items | Frequency | ||
|---|---|---|---|
| Knowledge about Malaria | Yes | 68 (85) | |
| No | 12 (15) | ||
| Source of Information | From a friend | 6 (7.5) | |
| From health worker | 24(30.0) | ||
| From media (radio/TV) | 50(62.5) | ||
| Knowledge Regarding the Causes of Malaria | Yes | 62 (77.5) | |
| No | 18 (22.5) | ||
| Knowledge about Seriousness of Malaria | Yes | 70 (87.5) | |
| No | 10 (12.5) | ||
| Transmission of Malaria | Mosquitoes | 70 (87.5) | |
| other | 8 (12.5) | ||
| Knowledge about Clinical Manifestations of Malaria | Yes | 64 (80.0) | |
| No | 16 (20.0) | ||
| Clinical Manifestations of Malaria | Fever | 54 (84.4) | |
| Feeling chills | 10 (15.6) | ||
| Vomiting | 30 (46.9) | ||
| Lack of appetite | 11 (17.2) | ||
| Headache | 54 (84.4) | ||
| Steps Taken after Noticing Clinical Manifestations | Self-medication | 12 (15) | |
| Visit hospital after the failure of self-medication | 18 (22.5) | ||
| Visit hospital for treatment | 50 (62.5) | ||
| Most Frequent Mosquito Biting Time | Morning | 2 (2.5) | |
| Sunset/dusk | 22 (27.5) | ||
| Sunrise/dawn | 4 (5.0) | ||
| Night | 52 (65.0) | ||
| Knowledge about Prevention of Malaria | Yes | 74 (92.5) | |
| No | 6 (7.5) | ||
| Preventive Measures of Malaria | Mosquito coil | 8 (10) | |
| Apply mosquito repellent | 8 (10) | ||
| Wearing long protective clothing | 20 (25) | ||
| Use of fan | 4 (5) | ||
| Closing of the window during the sunset | 8 (10) | ||
| Using mosquito net | 12 (15) | ||
| Burning tissue and cow dung | 6 (7.5) | ||
| Traditional herbs (Musudzungwane) | 14 (17.5) | ||
4. DISCUSSION
Many studies have been conducted regarding malaria; however, this was the first study to be conducted on the knowledge of caregivers of children regarding malaria within the Vhembe district of Limpopo province. The knowledge of caregivers regarding malaria is of paramount importance because malaria is one of the leading causes of death in South Africa, especially in children, and these children are being taken care of by the caregivers [1].
Caregivers of children in the selected villages of the Vhembe district demonstrated adequate knowledge regarding malaria and its clinical manifestation. However, some caregivers exhibited a lack of knowledge on the studied phenomenon. The majority of caregivers who were knowledgeable about malaria were younger and educated. In contrast with the findings of the study conducted by Karascony [16], which revealed that older people have more experience regarding a phenomenon, and hence the knowledge, this study revealed that young people are the ones that have more knowledge regarding malaria regardless of the less experience of life.
Caregivers of children in the Vhembe district reported that the sources of their knowledge are mainly the radio, health care workers, and a friend. This agreed with a study conducted by Singh [17], which reported similar sources of knowledge regarding malaria from a different context.
More than half of the caregivers in the Vhembe district could identify common clinical manifestations of malaria, including fever, chills, vomiting, and lack of appetite. Knowledge of clinical manifestations has been reported as an important possession, especially to the caregivers of children, as they are the first line of care providers to children and can act immediately on the realization of these clinical manifestations. Furthermore, knowledge is regarded as pivotal because it assists in the global technical strategies for malaria elimination by 2030 [18]. This was also supported by a study conducted in the same context among community members’ knowledge on symptoms of malaria [19]. Most of the caregivers who were knowledgeable about common clinical manifestations reported that they visit health care facilities once they notice them. However, others reported visiting the health care facilities after the failure of home remedies to cure the symptoms [20-24]. This highlights that even though most caregivers possess knowledge regarding relevant actions to be taken, others still lack awareness regarding positive health-seeking behaviours appropriate for malaria, which still requires attention.
The caregivers of children in the Vhembe district demonstrated knowledge regarding preventive measures of malaria. About 25% of caregivers reported that wearing protective clothes at night, especially long-sleeved clothes, is better to prevent mosquito bites. In contrast, others reported using mosquito net at night, burning mosquito coil, using a fan at night, closing windows during sunset, using traditional herbs (Musudzungwane), and burning cow dung. Similarly, a couple of studies highlighted an increased knowledge regarding the preventive measures, including western and indigenous repellents of malaria and health-seeking behaviours in different contexts [22, 25-29]. In addition to malaria repellents, this study also revealed traditional means of preventing malaria through traditional practices that scare mosquitos away. Some caregivers in Vhembe were found to be unaware of malaria clinical manifestations and preventive measures. Therefore, health care providers and community health workers in the Vhembe district should provide relevant health education regarding malaria clinical manifestations and preventative measures.
CONCLUSION
Caregivers of children in villages around the Vhembe district were found to have basic knowledge regarding malaria even though some of them were unaware of preventive measures and clinical manifestations of malaria. The knowledge of caregivers can be improved by strengthening health education, preventive campaigns, and training of health care personnel [30, 31]. Further studies need to be conducted on knowledge, practices, and attitudes towards malaria in all tropical areas where malaria is prevalent. This study cannot be generalized to other villages of other provinces in South Africa due to the small sample size and different cultures. Although the latter limitations are marked, this study has some strengths as the study area and participants were selected via random cluster and simple sampling [32, 33].
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was provided by the Human and Clinical Trial Research Ethics Committee (HCTREC) of the University of Venda (SHS/17/PDC/29/3108).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated or analysed during the current study are not publicly available due to the type of ethical clearance approved. Data would not be shared publicly. Instead, data will only be shared in the form of a published article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the selected villages in the Vhembe district and respondents who participated in this study.

