All published articles of this journal are available on ScienceDirect.

Role of Knowledge, Attitude and Practice Among the General Population of Saudi Arabia in Management of Second Wave of COVID-19
Authors Info & Affiliations
Abstract
Introduction:
The highly infectious corona virus disease, described as a pandemic by the WHO, has been the focus of intense discussion world-wide due to its unpredictable nature and impact. The present study was undertaken to assess the health behavior of individuals as a result of their knowledge, attitudes and practice, which are important in containing the spread of such a pandemic in the community with anticipated future outcomes.
Methods:
This study was carried out to explore the influence of KAP of the Saudi population from Riyadh, Dammam, Jeddah, Medina, Abha, Qassim and other cities of KSA towards the second wave of the pandemic spike, and determine the acceptance of the population of changed behavioral measures.
Results:
About 90.2% of the respondents had strong knowledge and awareness about COVID-19 where as 80.7% showed positive attitudes, with a mean score of 29.52 ± 2.591 and 59.4% following good practices. About 75.5% of respondents regularly washed their hands, 73.7% used sanitizers effectively every time after touching some surface and 86.8% affirmed using masks regularly.
Conclusion:
The present data showed that irrespective of gender, age group, nationality, education level and occupation, majority of the population had adequate knowledge and positive attitude. However, it was found that good knowledge and positive attitude may not always culminate into good practice as evident from the study. This reflects that irrespective of the shortcomings, the Saudi government was successful in propagating right information across all sections of the society. The findings give valuable insight to policy makers and health officials to pinpoint gaps in these areas and bolster ongoing efforts to contain the pandemic and sustain the preventive measures implemented as part of the future strategic planning.
1. INTRODUCTION
The coronavirus pandemic witnessed certain peculiarities during the first and the second wave, with a massive spike in the COVID-19 infections during the winter season of 2020 and later in July 2021, respectively, as the contagious delta variant became dominant eventually. Despite mass vaccinations, behavior modifications, widespread education, and infection prevention policies, the second wave caught the global population by surprise, resulting in almost 6.9 million deaths till May 2021 [1]. However, there was a huge difference in the COVID-19 scenario, which was witnessed in the Western and other countries, including the subcontinent and the Middle East. This can be expressed in terms of the differences in the infection and the mortality rates of the two parts of the world, as stated.
Literature review suggests that an assessment of knowledge, attitude / awareness, and practices (KAP) is critical to understanding the reasons for the success or failure of prevention methods and support efforts to contain the spread of COVID-19 and anticipate future outcomes [2, 3]. The Saudi government initially implemented strict lockdown policies during the first wave as well as developed highly effective technological measures to monitor the situation with high vigilance in line with WHO guidelines since early March 2020, apart from the measure of aggressively vaccinating the Saudi population at large [4-6]. The present study was designed to explore the KAP of the Saudi population towards the second wave of the COVID-19 pandemic spike as well as to determine the acceptance of the general public of changed behavioral measures.
2. MATERIALS AND METHODS
2.1. Study Design
A web based cross-sectional study was conducted using the snowball sampling method. The study participants were recruited across different major regions of Saudi Arabia. The self-reported questionnaire on monkey survey link was distributed through social media platforms (Twitter, WhatsApp) from 10th to 20th April 2021 across the kingdom. The self-reported questionnaire was adapted from the study conducted by Zhang et al. [3], as well as from the guidelines recommended by the Center for Disease Control and Prevention for COVID-19 [4].
Both English and Arabic versions of the questionnaire were validated and tested for reliability as per the standard protocol. The Cronbach’s α coefficient was 0.70, indicating internal reliability from the pilot study. A small preliminary study was conducted on 15 participants to assess its feasibility. No specific exclusion criteria were used for the study, except those respondents below 18 years of age were exempted from the study. A total of 1294 people responded to the survey, out of which only 992 completed the full survey and were included in the study. As it was not feasible to conduct a systematic nationwide sampling procedure during this period, the researchers opted to use an online survey using Survey Monkey Advantage Annual. Members of the Kingdom of Saudi Arabia over the age of 18 years and currently residing in the country were eligible to participate in the survey. We utilized several strategies to reach out to as many respondents as possible all over the country within the one-week data collection period. This included relying on the professional and personal networks of the researchers, reaching out to community leaders and social media influencers to broadcast and share the survey. The structured questionnaire was divided into four parts having 30 questions; the first section contained demographic characteristics such as age, gender, occupation, marital status, education, and employment. The second section included 18 questions regarding knowledge of COVID-19, the third section included 7 questions regarding attitude towards COVID-19 and the fourth section included 12 questions to assess practice levels towards COVID-19. Each correct answer in relation to the knowledge of COVID-19 was given one point and incorrect and not sure answers were scored as zero points. Bloom's cut off point was used to characterize the overall knowledge, practice, and attitude scores [7]. If the score was less than 60%, it was regarded as bad knowledge; 60%-80% and 80% and above were classified as average and good knowledge, respectively. Similar criteria were set for both attitude and practice.
2.2. Statistical Analysis
The data were analyzed using Statistical Package for Social Services (SPSS) Version 26. Descriptive statistics and relevant tables using frequencies and percentages were used to summarize information. The knowledge, attitude, and practice scores were presented using mean and standard deviation. Descriptive statistics were used to define the socio-demographic factors as well as to represent the achieved knowledge, attitude and practice scores. Inferential statistics, correlation coefficient, and logistic regression methods were used to identify the influences, associations, and determinants of different socio-demographic factors in relation to COVID-19 knowledge, attitude, and practice. A two-tailed p value of less than 0.05 was considered statistically significant, at a 5% significance level.
2.3. Ethical Considerations
The study approval was obtained from the Institutional Research Committee of Saudi Electronic University Riyadh, Saudi Arabia, under the Deanship of Scientific Research, Ethical Clearance No. (REC Number SEUREC-CHS20100). Responses to the survey instrument were collected anonymously, and data were used for analysis and interpretation purposes only.
3. RESULTS
A total of 992 respondents from across various regions of the Kingdom completed the survey. Among the participants 65.8% of respondents were female against 34.2%, who were males. On the basis of nationality, 82% of the respondents were Saudis, in comparison to the 18% expatriates. On the basis of marital status, 51.6% were married, as against 42.4% who were single. Similarly, comparing the educational status, a majority 70.2. % of the respondents had a qualification of undergraduate degrees and above in comparison to the 15% who were diploma holders, whereas 14.4% had studied till high school or less.
On the basis of service categorization, 43.1% of respondents had government jobs as against 15.2% who were employed in the private sector. Almost 37.1% of the study samples were not working and the remainder were self-employed. On the basis of age, a majority (94.7%) were in the age bracket of 18-45 years, as compared to others (5.3%). Similarly, on the basis of geographical location, the majority of the respondents (45.86%) were from Riyadh, followed by Dammam (18.5%). The details of the demographic data are presented in Table 1.
| Variables | Numbers | Percentage |
|---|---|---|
| Age | ||
| 18-25 | 264 | (26.6) |
| 26-35 | 436 | (44.0) |
| 36-45 | 239 | (24.1) |
| 46-55 | 46 | (4.6) |
| 56-65 | 4 | (0.4) |
| 65+ | 3 | (0.3) |
| Gender | ||
| Male | 339 | (34.2) |
| Female | 653 | (65.8) |
| Nationality | ||
| Saudi | 814 | (82) |
| Non-Saudi | 178 | (18) |
| Marital status | ||
| Married | 512 | (51.6) |
| Divorced | 52 | 5.2) |
| Widowed | 7 | (0.7) |
| Single | 421 | (42.4) |
| Education | ||
| High School or Less | 143 | (14.4) |
| Diploma | 153 | (15.4) |
| Undergraduate | 497 | (50.1) |
| Postgraduate | 199 | (20.1) |
| Occupation | ||
| Private | 151 | (15.2) |
| Government | 428 | (43.1) |
| Self employed | 19 | (1.9) |
| Not working | 368 | (37.1) |
| Others | 26(2.6) | |
| City of Residence | ||
| Riyadh | 455 | (45.9) |
| Dammam | 184 | (18.5) |
| Jeddah | 119 | (12) |
| Abha | 23 | (2.3) |
| Madina | 31 | (3.1) |
| Al-Ahsa | 32 | (3.2) |
| Qassim | 11 | (1.1) |
| Jazan | 6 | (0.6) |
| Tabuk | 3 | (0.3) |
| Others | 128 | (12.9) |
3.1. Knowledge Regarding COVID-19
A majority (90.2%) responded correctly to knowledge related questions, assessed with respect to asking pertinent questions related to the spread of infection, risk groups, preventive measures, as well as awareness regarding contacting the agency (Table 2). On comparing the knowledge scores across various demographic factors, including gender, age, nationality, marital status, education, occupation and healthcare experience, it was observed that statistically significant differences existed between groups for gender, age, occupation, and healthcare experience (p<0.05). It was observed that males had more knowledge (94.4%, (OR=2.2, CI OR = 1.3, 3.7) as compared to the female respondents (88.3%), which is statistically significant (p = 0.001). The results showed that the distribution of knowledge varied across the different age groups (Table 3). A similar pattern of knowledge variance occurred among respondents of different occupations (p =.013), in particular those who worked in the healthcare sector (p=0.000)
| Questions | Yes (%) | No (%) | Not Sure (%) |
|---|---|---|---|
| Coronavirus Infection Spread | |||
| K1. Shaking hands | 927 (93.4) | 46(4.6) | 19 (1.9) |
| K2. Droplets of sneeze or cough | 976 (98.4) | 3 (0.3) | 13 (1.31) |
| K3. Goods imported from china | 131 (13.2) | 664 (66.9) | 197 (19.9) |
| K4: Contaminated surface or object | 915 (92.2) | 24 (2.4) | 53 (5.3) |
| K5: Fever cough cold, shortens of breath are symptoms | 978 (98.6) | 7 (0.7) | 7 (0.7) |
| High Risk Group | |||
| K6: Children less than 5 years old | 372 (37.5) | 444 (44.8) | 176 (17.7) |
| K7: People with chronic diseases | 945 (95.3) | 14 (1.4) | 33 (3.3) |
| K8: Elderly people | 959 (96.7) | 20 (2.0) | 13 (1.3) |
| K9: People with poor immunity | 970 (97.8) | 7 (0.7) | 15 (1.5) |
| K10: Symptoms appeared 2-14 days after infection | 956 (96.4) | 18 (1.8) | 18 (1.8) |
| Prevent Corona Infection | |||
| K11: Washing hands with soap | 986 (99.4) | 4 (0.4) | 2 (0.2) |
| K12: Using hand sanitizer | 956 (96.4) | 20 (2.0) | 16 (1.6) |
| K13: Wearing a facemask | 727(73.3) | 217 (21.9) | 48 (4.8) |
| K14: Sneezing into your elbow or tissue | 946(95.4) | 34 (3.4) | 12 (1.2) |
| K15: Staying at home | 989(99.7) | 2 (2.2) | 1 (0.1) |
| When One Should Contact 937 or Seek Medical Emergency | |||
| K16: Difficulty in breathing | 962(97.0) | 18 (1.8) | 12 (1.2) |
| K17: Fever | 907(91.4) | 54 (5.4) | 31 (3.1) |
| K18: Dry cough | 876(88.3) | 64 (6.5) | 52 (5.2) |
3.2. Attitude Regarding COVID-19
In the study population, most of the respondents (98.79%) strongly believed in adhering to the precautions implemented by the Ministry of Health, KSA. 92.64% believed that socializing with family and friends was not a safe practice during the lockdown period. 97.68% believed that anyone with flu-like symptoms should always cover their mouth when coughing or sneezing by the crook of the elbow (Table 4). Among the respondents in the analysis, a total of 80.7% showed a positive attitude, with a mean score of 29.52 ± 2.591.
The attitude score details are also given in (Table 3), which also summarizes the associations between demographic characteristics and attitudes, same as done earlier for the knowledge scores. Both genders showed almost the same level of positive attitude (81.7%) in males and (80.2%) in females; however, it was not statistically significant (P>0.05). Among the study respondents, the 36-45 years age group showed a more positive attitude 83.3%, followed by the 26-35 years age group (81.2%), 18-25 years (79.5%), 46-55 years (73.9%), respectively, however, the observed difference was not statistically significant at a 5% significance level (p>0.05).
| Demographic Variables | Good Knowledge Score | Positive Attitude Score | |||
|---|---|---|---|---|---|
| Characteristics | Respondents n (%) Total | n (%) | P value | n (%) | P value |
| Overall | 992 | 896(90.2) | 801(80.7) | ||
| Gender | |||||
| Male | 339(34.2) | 320(94.4) | 0.001* | 277(81.7) | 0.579 |
| Female | 653(65.8) | 576(88.3) | 524(80.2) | ||
| Age Group | |||||
| 18-25 | 264(26.6) | 222(84.1) | 210(79.5) | ||
| 26-35 | 436(44.0) | 402(92.2) | 0.001* | 354(81.2) | 0.125 |
| 36-45 | 239(24.1) | 224(93.7) | 199(83.3) | ||
| 46-55 | 46(4.6) | 42(91.3) | 34(73.9) | ||
| 56-65 | 4(0.4) | 4(100) | 3(75) | ||
| 65+ | 3(0.3) | 2(66.7) | 1(33.3) | ||
| Nationality | |||||
| Saudi | 814(82) | 733(90) | 661(81.2) | ||
| Non-Saudi | 178(18) | 163(91.6) | 0.533 | 140(78.7) | 0.434 |
| Marital Status | |||||
| Married | 512(51.6) | 472(92.2) | 415(81.1) | ||
| Divorced | 52(5.2) | 44(84.6) | 43(82.7) | ||
| Widowed | 7(0.7) | 5(71.4) | 0.055 | 5(71.4) | 0.895 |
| Single | 421(42.4) | 375(81.1) | 338(80.3) | ||
| Education | |||||
| High school or less | 143(14.4) | 128(89.5) | 113(79) | ||
| Diploma | 153(15.4) | 139(90.8) | 120(78.4) | 0.707 | |
| Undergraduate | 497(50.1) | 445(89.5) | 0.671 | 408(82.1) | |
| Postgraduate | 199(20.1) | 184(92.5) | 160(80.4) | ||
| Occupation | |||||
| Private | 151(15.2) | 137(90.7) | 118(78.1) | ||
| Government | 428(43.1) | 398(93) | 0.013* | 350(81.8) | 0.855 |
| Self-employed | 19(1.9) | 17(89.5) | 16(84.2) | ||
| Not working | 368(37.1) | 318(86.4) | 297(80.7) | ||
| Others | 26(2.6) | 26(100) | 20(76.9) | ||
| Working in Heath Care Sector | |||||
| Yes | 279(28.1) | 267(95.7) | 0.000* | 221(79.2) | |
| No | 713(71.8) | 629(88.2) | 580(81.3) | 0.443 | |
| Known to Diagnosed Patients family or friends | |||||
| Yes | 66(6.6) | 62(93.9) | 0.148 | 46(69.7) | |
| No | 870(87.6) | 780(89.7) | 709(81.5) | 0.062 | |
| Do not know | 56(5.6) | 54(96.4) | 46(82.1) | ||
| Questions | Positive Attitude (%) |
|---|---|
| A1: as I have not travelled, I am not worried about getting infected | 729(73.48) |
| A2: I believe that anyone with flu like symptoms should always cover their mouth when coughing or sneezing into their elbow | 969(97.68) |
| A3: Washing hands after touching any objects or surfaces outside the house can help prevent transmission of coronavirus infection. | 977(98.48) |
| A4: I think socializing with family and friends is a safe practice during the current curfew | 919(92.64) |
| A5: I believe I do not have to make any adjustments in my life | 790 (79.63) |
| A6: I believe that the adherence to the precautions imported by the ministry of health | 980(98.79) |
| A7: I believe consuming herbal or traditional remedies can help in preventing coronavirus | 144(14.51) |
Therefore, active engagement or when the participants totally agreed to abide by the statements or MoH standards such as “the participants should always cover their mouth who had flu like symptoms”, “washing hands after touching any surface outside the house can help in preventing transmission of corona” was considered a positive attitude that contributed to decreasing the prevalence of COVID-19. like, “the participants should always cover their mouth who had flu like symptoms”, “washing hands after touching any surface outside the house can help in preventing transmission of corona”. The attitude considered positive were those that completely adhered to the precautionary measures imposed by the ministry of health, which greatly helped in reducing the number of coronavirus cases, in corroboration with the report of Albarrak et al. [8].
3.3. Practice Regarding COVID-19
The overall mean practice score for COVID-19 was 19. 53, SD = 4.14. The average practice score for females was 19.58±4.20, and for males, 19.43± 4.04. Out of 992 respondents, only 589 (59.4%) showed good practice and that percentage was lower in comparison to the knowledge (90.2%) and attitude (80.7%) domains. These data provide clear evidence of observed differences in the knowledge and practice levels, which are significant (P=0.002) at a 5% significance level (Tables 5, 6).
Table 5.
| - | Always | Sometimes | Never |
|---|---|---|---|
| P1: I wash my hands | 749(75.5) | 231 (23.3) | 12 (1.2) |
| P2: If I do not find soap, I use sanitizer or disposable wipes or alcohol to clean my hands. | 731(73.7) | 242 (24.4) | 19 (1.9) |
| P3: When wearing a mask, I make sure it fits properly. | 861(86.8) | 112 (11.3) | 19 (1.9) |
| P4: I dispose of any used paper tissues in the trash. | 962(97.0) | 25 (2.5) | 5 (0.5) |
| P5: I avoid shaking hands | 884(89.1) | 90 (9.1) | 18 (1.8) |
| P6: I avoid being close to those who cough or sneeze | 835(84.2) | 68 (6.9) | 89 (9) |
| P7: I avoid touching my face | 504(50.8) | 393 (39.6) | 95 (9.6) |
| P8: I avoid going to supermarkets or grocery stores and prefer to purchase online | 774(78.0) | 68 (6.9) | 150 (15.1) |
| P9: I avoid touching door handles, stair rails, etc. | 615(62.0) | 279 (28.1) | 98 (9.9) |
| P10: I avoid using elevators if somebody else is using it at same time | 558(56.2) | 239 (24.1) | 195 (19.7) |
| P11: I avoid using currency note or coins | 467(47.1) | 365 (36.8) | 160 (16.1) |
| P12: I avoid using ATMs | 510(51.4) | 361 (36.4) | 121 (12.2) |
| Demographic characteristics | Good Practice | |
|---|---|---|
| - | Yes | No |
| Overall | 589(59.4) | 403(40.6) |
| Gender | ||
| Male | 195(57.5) | 144(42.5) |
| Female | 394(60.3) | 259(39.7) |
| Marital Status | ||
| Married | 318(62.1) | 194(37.9) |
| Divorced | 29(55.8) | 23(44.2) |
| Widowed | 3(42.9) | 4(57.1) |
| Single | 239(56.8) | 182(43.2) |
| Occupation | ||
| Private | 86(57.0) | 65(43) |
| Government | 259(60.5) | 169(39.5) |
| Self-employed | 14(73.7) | 5(26.3) |
| Not working | 214(58.2) | 154(41.8) |
| Others | 16(61.5) | 10(38.5) |
| Age Groups | ||
| 18-25 | 145(54.9) | 119(45.1) |
| 26-35 | 259(59.4) | 177(40.6) |
| 36-45 | 153(64.0) | 86(36.0) |
| 46-55 | 30(65.2) | 16(34.8) |
| 56-65 | 1(25.0) | 3(75) |
| 65+ | 1(33.3) | 2(66.7) |
| Nationality | ||
| Saudi | 475(58.4) | 339(41.6) |
| Non-Saudi | 114(64) | 64(36.0) |
| Education | ||
| High school | 84(58.7) | 59(41.3) |
| Diploma | 90(58.8) | 63(41.2) |
| Undergraduate | 286(57.5) | 211(42.5) |
| Postgraduate | 129(64.8) | 70(35.2) |
(Table 6) illustrates the gender comparisons for practice level with 60.3% of females having good practice, which was slightly higher as compared to males (57.5%), even though the difference was not statistically significant (P>0.05).The calculated correlation coefficient of knowledge versus attitude was (r= 0.239 with p=0.000), attitude versus practice (r=0.109 with p= 0.001), and knowledge against practice (r= 0.202 with p=0.00), which was statistically significant at a 5% significance level. From the total study population, more than half of the respondents had adequate knowledge and followed good practices (approximately 59.4%). Interestingly, the results showed that nearly 39% of the total study population did not follow good practices even though they had adequate knowledge (Table 7).
Table 7.
| Good Practice | P value | ||
|---|---|---|---|
| Good Knowledge | Yes | No | |
| Yes | 546(60.93) | 350 (39.06) | 0.002** |
| No | 43(44.79) | 53(55.2) | |
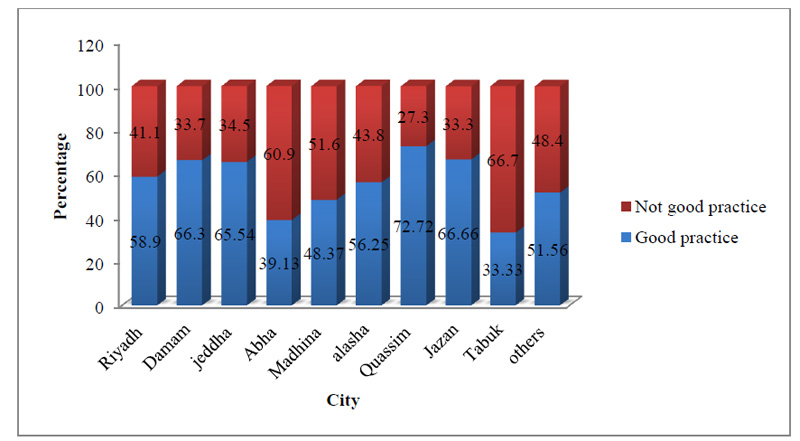
Fig. (1) depicts the geographic distribution of practice across the various regions of the Kingdom of Saudi Arabia. The respondents from the capital city of Riyadh had a noticeably less practice percentage (58.9%) compared to Dammam (66.3%), Jeddah (65.54%), Jazan (66.66%), and Qassim (72.7%). However, these variations across different regions were not statistically significant (P>0.05). While evaluating the association between adequate knowledge and good practice with sufficient information provided by the government, a statistically significant difference was found between the two groups, (p=0.014**) and (p=0.037**), inferring that majority of respondents with good knowledge (78.6%) observed good practice (80.5%) and believed that sufficient information and mechanisms were put in place by the government for the public (Table 8). Similarly, evaluating the association between adequate knowledge and good practice with reference to trust in the Saudi health system to manage the situation, it was found that a statistically significant difference was observed between the group, which had adequate knowledge as well as believed firmly in government’s ability to manage the situation well (86.8%, p=0.001**). However, with reference to the association between good practice and trust in the government system, no significant difference was observed (p=0.317) (Table 9).
| Domain | Sufficient Information provided by Saudi Government | |||
|---|---|---|---|---|
| Adequate Knowledge | Yes | No | Not sure | P value |
| No | 68(70.8) | 16(16.7) | 12(12.5) | 0.014** |
| Yes | 704(78.6) | 70(7.8) | 122(13.6) | |
| Good Practice | ||||
| No | 298(73.9) | 44(10.9) | 61(15.1) | 0.037** |
| Yes | 474(80.5) | 42(7.1) | 73(12.4) | |
| Participants Trust in the healthcare system | ||||
|---|---|---|---|---|
| Adequate Knowledge | Yes | No | Not sure | P value |
| No | 77(80.2) | 7(7.3) | 12(12.5) | 0.001* |
| Yes | 778(86.8) | 14(1.6) | 104(11.6) | |
| Good Practice | Yes | No | Not sure | P value |
| No | 340(84.4) | 11(2.7) | 52(12.9) | 0.317 |
| Yes | 515(87.4) | 10(1.7) | 64(10.9) | |
4. DISCUSSION
This study aimed to estimate the general level of awareness, practice, and attitude towards the second wave of COVID-19 pandemic spike in Saudi communities located across various major regions of the Kingdom. Various demographic characteristics of the population were explored to assess the impact of such factors on the population at large and to predict their effects on the course of the disease. Even though a majority (90.2%) had good knowledge, but did not culminate it into good practice. Only 60.93% of respondents who had good knowledge were found to have followed good practices in comparison to 39.06% of people who, despite having good knowledge, ignored good practice following (p=0.002**). This suggests that despite good knowledge and attitude, other factors would affect observing good practices in the society. This becomes even more imperative, especially in pandemic like corona when societal behavior at large can affect the disease courses quite strongly.
It is well known that knowledge, awareness, and practices are fundamentally important to changing the health behavior of people, which is especially relevant in managing the unpredictable challenges of the sudden appearance of a pandemic. In our study, it is clearly evident that knowledge of the respondents about the disease and other important aspects was quite high (90.2%), which got reflected in the form of an important factor of positive attitude in about 80.5% of the respondents, though statistically found insignificant (p>0.05) (Tables 3 and 8).
On comparing the knowledge level based on different demographic parameters, it was found that males had more knowledge (94.4%, (OR=2.2, CI OR = 1.3, 3.7) as compared to female respondents (88.3%), being statistically significant (p = 0.001). Recent studies have also suggested that men are affected more than women by the COVID-19 virus [9]. In another recent work by Kopel et al. [10], where racial and gender-based differences in Covid 19 were evaluated, it was found that COVID-19-associated hospitalization rates were higher among males than females (5.1 vs. 4.1 per 100,000 population). These data are also buttressed by the work of Liu et al. and Li et al. [11, 12].
It may be pointed out that such studies are quite limited and do not suggest anything conclusively. Male fatalities are 1.7 times higher than female fatalities, and this pattern may be seen in how men observe knowledge-based practice, which is amply supported by these findings [9]. These factors might be responsible for males having greater knowledge than females, though no corroborative evidence could be suggested presently, and more research needs to be done in this area. Correlating the association between good knowledge and good practice, a statistically significant difference was observed between the groups, with 60.93% of respondents who had ample knowledge of good practice in comparison to 39.06% of respondents who, despite having good knowledge, did not follow good practices (p=0.002**) (Table 7).
This difference could be attributed to the fact that some of the questions asked in the study in relation to good practices were quite straight forward and difficult to implement, for instance, when asked, “whether you avoid going to supermarkets or grocery stores (P8) or do you avoid touching door handles, stairs, and rails (P9) or do you avoid using elevators when somebody else is using it (P9) or do you avoid using currency notes or coins (P11) (Table 5)”? Self-improvement in one’s behavior culminating into a good habit is dependent upon noticing, wanting, doing, and liking, as suggested by Berridge and Kent [13]. Consequently, it may be quite possible that while many people, irrespective of having the best of the knowledge and knowing the practices that are good for health, may not likely do it at all or having done it once or twice may not culminate into positive behavior. This could be because of various reasons, including making extra effort difficult, being lazy or forgetfulness [14].
In response to these questions, the results suggested that the affirmative responses were recorded in percentages in descending order of 78%,62%, 56.2%, and 47.1%, respectively, as evident from (Table 5). These may be some of the valid reasons for scoring low in good practices despite having good knowledge. Although some studies imply that knowledge is strongly connected with attitude and practice in relation to infectious diseases, such phenomena may not necessarily result in affective practices in terms of COVID-19 [15, 16].
Since the initial outbreak of COVID-19 disease in China, it has been observed that the pandemic spread out quite fast during the 1st wave, which peaked from May 2020 to September 2020, followed by the 2nd wave, which saw cases surging from April 2021 to July 2021 in different parts of the world [17].
Critically evaluating the two important factors, the question to be answered is whether the KAP worked wonders or the Saudi government’s strict policies and their implementation brought about the desired results? Our study suggested that despite having high knowledge, good attitude and practices do not culminate overnight. Saudi Arabia Ministry of Health reports suggest that, apart from constant dissemination of knowledge, implementation of strict curfews and lockdown during the festive time, very heavy fines and penalties on breaking the rules, quarantine banknotes and coins for infinite period, sterilizing both paper and metal currencies, suspension of all domestic and international travel, etc., during the first wave, worked in conjunction with the KAP [18].
The phenomenon can be further explained in the light of the two questions that were put to the respondents to assess the association between adequate knowledge and good practice with reference to sufficient information provided by the government. It was observed that the respondents with good knowledge (78.6%) and good practice (80.5%) firmly believed that sufficient information and mechanisms were put in place via the orders of government for the symbiotic compliance of the public in their interest (p=0.014**, p=0.037**) (Table 8). Likewise, evaluating the association between adequate knowledge and good practice with trust in the Saudi health system, it was observed that a majority, 86.8%, with adequate knowledge, believed firmly in government’s ability to manage the situation very well (p=0.001**). However, no such inference could be drawn with respect to good practice and trust in government systems (p=0.317). The flattening of the curve in Saudi Arabia post September 2020 with the cases quite under control thereon is evident that the overall government’s strict initiatives and timely MOH actions led to controlling the situation with adequate public cooperation.
Some of the research studies, such as those by Qutob and Awartani, Asdaq et al. and Algaissi et al., have suggested that experience gained from the Middle East respiratory syndrome coronavirus (MERS-CoV) epidemic since 2012 helped the Kingdom apparently to be better in preparedness for the current COVID-19 pandemic [2, 6, 18]. The lessons drawn from the earlier model also get appropriate support from other likable cases. For instance, one research study, while evaluating the fight against corona between the two biggest superpowers viz China versus the USA, suggested that China was able to successively mobilize the masses to beat the virus and curb it down effectively, whereas US led to a disaster, which can be substantiated from the fact that the US was hardest hit with the highest rate of casualties. Strict implementation of rules and mandatory compliance to various preventive measures suggested were the key to success. However, despite having a highly educated population, the US failed miserably in most of its states to contain the disease [19, 20]. This again supports our argument that irrespective of adequate knowledge, positive attitude, and good practice, the upsurge can be contained due to the implementation of strict government measures with accurate precision.
Several publications on assessment of knowledge, attitudes, and practice (KAP) also have suggested that Testing, Tracing, Isolation, and Quarantine (TTIQ) is the only universally tested and effective method to contain pandemic situations, as neither vaccine nor any 100% effective anti-viral entity is at hand [2, 3, 16, 21-26]. It was also observed that the strategy was put in place for more aggressive testing, which again was observed to have provided the impetus to have more trust in government’s effort in containing the disease [27].
To our knowledge, to date, very few studies of this type have been conducted that assess deeply the factors responsible for evaluating KAP features in containing the pandemic disease as far as the Kingdom of Saudi Arabia is concerned [6, 18, 27, 28]. There are some fundamental differences between the studies conducted over KAP in literature in relation to our study. Some of the salient differences also exist with reference to various demographic parameters, including patient’s number, gender, income, and education levels. In our study, it was revealed that males had 90.2% more adequate knowledge, while other studies by Zhang et al., Zhong et al., Souli and Dilucca, Rugarabamu et al., Aakash et al., and Maheshwari et al. suggested that females fared better than males [3, 16, 22, 29-31]. For instance, a study published in Malaysia over KAP had 57.9% female respondents and 42.1% males [23]. This is also reflected in studies conducted in China, Tanzania, Bangladesh, and Vietnam, where the majority of respondents were females [3, 29, 30, 32]. Our study apart from the other two studies, has reported that a larger proportion of male respondents or almost equal in number to females exist [26, 27]. Similarly, comparing the education levels of the respondents to the KAP assessment, it was also observed that 70.2% of respondents were at the graduate level and above, whereas the 29.8% were diploma holders or high school pass or less with a mean knowledge score of16.14± 1.508, which was quite high by all standards, as reported in other studies [3, 25, 33].
Similarly, with respect to occupation, respondents working in the healthcare sector had more knowledge and information on COVID-19 as compared to the non-healthcare sector, which was found to be statistically significant in the present study (Table 3).
Other positive findings in our study suggest that 92.7% of the respondents already knew about the preventive measures being implemented, as 73.3% responded correctly that wearing face masks could help prevent virus transmission, which is almost similar to the findings from Paraguay, where 74.3% of the population believed that using masks can prevent transmission [21]. Other studies from Bangladesh and Nepal also reported that around 70 - 75.5% wore masks while going out [24, 30, 33]. Studies also suggest that masks were quite effective in containing infections, which can be attributed to key considerations, namely, the role of droplets as a transmission route, and whether masks can help reduce droplets' dispersal. Even though only a few studies have been conducted, all of them point to the possibility that, in contrast to the standard use of masks for wearer protection, their use in situations where physical distancing is unpredictable or impossible could reduce onward transmissions by asymptomatic and presymptomatic wearers [34, 35].
Assessing the linkage of one's occupation with knowledge, in the present study, it became clear that respondents working in either government, the private sector or being self-employed had better knowledge as compared to those who were not working, which is statistically significant (p*=0.013). This suggests that working people were more exposed to health awareness programs by the media in comparison to those who were at home during the lockdowns.
The knowledge, attitudes and practices (KAP) towards COVID-19 play an integral role in determining society’s readiness to accept behavioral change measures from health authorities. KAP studies provide baseline information to determine the type of intervention that would be helpful to provide better insight to address poor knowledge about the disease and the development of preventive strategies and health promotion programs. Among the lessons learned from the COVID- 19 was that knowledge and attitudes are also associated with levels of panic and emotions, which could further complicate measures to contain the spread of the disease [27, 35]. The results of the study are important to inform future efforts focusing on societal readiness to comply with pandemic control measures, and this can better prepare the government to address future health crises involving infectious diseases. Interestingly, while evaluating the differences in the geographic/regional distributions in relation to observed practices, it was observed that the capital city, Riyadh, had a lower percentage of practice (58.9%) as compared to Dammam (66.3%), Jeddah (65.54%), Jizan (66.66%), and Qassim (72.7%), showing that the practice percentage varied in descending order. However, these variations across regions were not statistically significant (p>0.05), suggesting that irrespective of KAP measures, it is the strict and timely intervention that brings effective results, which is well supported by the study conducted in the Kingdom by Khan et al. [28].
LIMITATIONS
One of the major limitations of our study was that we could gather data only through online mediums. It is worth noting here that all the reported COVID-19 KAP studies were conducted using internet-based surveys and thus could have an element of inherent bias. Such media can only be accessed by those who are literate, computer savvy, have active social media accounts, and are aware of the developments regarding COVID-19. Thus, to some extent, it might not be a true measure of the KAP among all citizens, as the study method inherently excluded those who were illiterate or who did not have access to the internet, such as the daily wagers. This may have led to a limited number of responses from this important expatriate population. Despite this limitation, the present data shows that the KAP measurements are reasonably apparent.
CONCLUSION
The findings of the study showed that the majority of the population had adequate knowledge and positive attitude irrespective of the demographic differences. However, this may not always transform into good practice, as evident in our study. This suggests that positive attitudes toward best practices, including intentions towards recommended behaviors, may hold stronger promise for future studies. Adequate knowledge and appropriate translation into the right attitude and good practices are of utmost importance for controlling pandemic like situations with strong and strict government public health initiatives.
LIST OF ABBREVIATIONS
| KAP | = Knowledge, Attitude / Awareness, and Practices |
| SPSS | = Statistical Package for Social Services |
AUTHORS CONTRIBUTIONS
All authors made substantial contributions to conception, design, acquisition of data, analysis, and interpretation of data, drafting the article or revising it critically for intellectual content and reasoning, provided final approval of the version to be published, and agreed to be accountable for all aspects of the work.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study approval was obtained from the Institutional Research Committee of Saudi Electronic University, under the Deanship of Scientific Research (REC Number SEUREC-CHS20100).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All human procedures followed were in accordance with the guidelines recommended by the Center for Disease Control and Prevention for COVID-19.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants of this study.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and/or analysed during the current study are not publicly available due to privacy and confidentiality agreements as well as other restrictions but are available from the corresponding author [M.A.M] upon reasonable request.
FUNDING
This project was funded by the Deanship of Scientific Research (DSR), Saudi Electronic University, Riyadh, Grant No. SEUREC-CHS20110.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors acknowledge the Deanship of Scientific Research (DSR), Saudi Electronic University, Riyadh, Saudi Arabia, for technical and financial support for this work.

