All published articles of this journal are available on ScienceDirect.

Analyzing the Adoption of Clean and Healthy Living Behaviors against COVID-19 Students in Indonesia
Abstract
The ease of obtaining information influences students adopting the behavior.
Purpose:
To analyze the indicators of clean and healthy living behavior (PHBS) on students and find the effect of information in dealing with COVID-19.
Methods:
This is a quantitative study using a cross-sectional design and was conducted from March – to June 2020. The sample of students at one of the State Universities in Medan City was 352 respondents. Furthermore, the data were collected through a questionnaire, and path analysis determined the relationship between variables x and y. The influence of the respondents’ characteristic variables (X1) on the consumption of nutritious food (Y1), exercise habits (Y2), handwashing habits (Y3), environmental hygiene (Y4), smoking habits (Y5), wearing masks (Y6), water consumption (Y7), consumption of cooked food (Y8), use of health facilities (Y9), the habit of praying (Y10) was analyzed. Meanwhile, the effect of access to information (X2) on the consumption of nutritious food (Y1), exercise habits (Y2), handwashing habits (Y3), environmental hygiene (Y4), smoking habits (Y5), wearing masks (Y6), water consumption (Y7), consumption of cooked food (Y8), use of health facilities (Y9), and praying habit (Y10) was studied.
Results:
This study found that information affected the consumption of nutritious food, exercise habits, handwashing habits, and health facilities with a T-statistic value of 2.603, 1.970, 2.941, and 4.631, respectively, while individual characteristics influenced the use of masks with a value of 2,167.
Conclusion:
Information affects PHBS, and information media is an effective way and impetus for students to adopt the behavior. Furthermore, behavior change will be impacted when information is presented well.
1. INTRODUCTION
The emergence of the COVID-19 pandemic in Wuhan has spread around the world, including Indonesia. From March 2020 to January 13, 2021, there were 91,968,829 million confirmed positive cases, with 231,846 patients declared cured, and 10,819 died [1]. Furthermore, the rapid and deadly spread has become a global health problem. All countries have been affected by COVID-19, thereby reducing income and asset investment [2]. In addition, international trade is significantly affected by restrictions on access between countries [3], resulting in unemployment, job losses, and company closures [4]. The World Health Organization (WHO) stated that the rapid increase is due to person-to-person transmission [5]. Therefore, it is necessary to limit social contact and implement clean and healthy living behavior (PHBS) to break the chain of transmission. When these efforts are not made, the number of these diseases will continue to increase with the threat of death.
The Ministry of Health has developed a strategy to improve the quality of public health through a movement for PHBS that began in 2016 [6]). This program includes 1) consumption of nutritious food, 2) exercise habits, 3) hand washing habits, 4) environmental hygiene, 5) smoking habits, 6) using masks, 7) water consumption, 8) consumption of cooked food, 9) utilizing health facilities, and 10) praying habit (Decree of the Minister of Health No. HK.01.07-Menkes-328-2020 concerning health protocols in places and public facilities to prevent the pandemic). However, the implementation has not been conducted by the entire community. Families who had a clean and healthy lifestyle in Jakarta city in 2017 were 51% of the 466,828 household heads surveyed [7]. Following the spread of the COVID-19 pandemic in Indonesia, modifications were made to the application of a clean and healthy lifestyle in the family to prevent the spread. Previous studies carried out the implementation of PHBS in health and non-health students and found no significant difference between the two groups [8]. The Indonesian government has socialized the clean and healthy living movement and protocols in public places to suppress COVID-19 cases through health promotion activities. However, this behavior has not been applied specifically to students. Kumar (2013) stated that promotion is an effective and relevant medium to improve health globally [9].
The WHO provided strategic steps to reduce the spread of this disease by staying at home, maintaining physical distance, wearing masks, eating nutritious foods, and getting used to washing hands. This is relevant to Wang (2021) that social isolation and self-quarantine are optimal strategies to prevent increased cases [10]. Jalal explained that long-term restrictions to minimize the spread would not be accepted by the community, and people’s lives will slowly return to normal [11]. This condition has occurred in Indonesia, showing the end of social restrictions and the start of a new normal society that does not heed health procedures in public places. The approach to the concept of behavior, according to L. Green, is influenced by supporting and driving factors. However, in this study, the theory has not been able to explain the phenomenon of someone who applies a clean and healthy lifestyle. Another factor to be considered is the role of information media, which was thought to influence a person’s willingness to adopt healthy behavior. A previous study stated that student behavior is influenced by their environment [12]. The environment has a very large influence on a person’s adopting behavior.
The Indonesian government has socialized the implementation of PHBS and the application of health protocols to all levels of society, workers, and students. One of the implementations of PHBS is in the school environment to strengthen the culture of the community. PHBS is 93.7% in the poor category [12], meaning it has not been implemented. The application of PHBS to non-health students is 49.2% lower than the health group. The subjects are distinguished based on the fields of social science, humanities, and health. The PHBS program is studied in health student courses. A previous study found the results of interviews with informants at State Junior High School X, where many students did not conduct PHBS, such as washing hands with soap and running water [13]. It is necessary to promote socialization of the application of PHBS at all levels of society, including students, to suppress the spread of COVID-19. Furthermore, access to information affects PHBS.
Based on this, it is necessary to study the implementation of PHBS in students and their tendency to adopt the behavior. Therefore, a description of students’ awareness of implementing PHBS in dealing with COVID-19 and PHBS indicators is obtained. This study becomes input in assessing the indicators of PHBS applied by students and the factors influencing the behavior. It aimed to determine the indicators of PHBS carried out by students and to prove that access to information affects these variables in dealing with the pandemic. This study contributes to the Indonesian government by using easily accessible information media as an approach to the community to implement PHBS to prevent the spread. Other studies only analyzed PHBS, and there is no variable of access to information.
2. MATERIALS AND METHODS
2.1. Study Design and Participants
This quantitative study was conducted using a cross-sectional design, and the data were collected once during the period before analysis [14]. According to Hardadini (2020), there are 2 forms of surveys, namely cross-sectional and longitudinal [15]. This study was conducted on students of Universitas Islam Negeri Sumatera Utara in Medan City. This is based on the consideration that it was carried out during a pandemic, and restrictions on activities outside the home, campus, and public places were imposed. Data were collected using a survey from March – to June 2020.
2.2. Inclusion Criteria
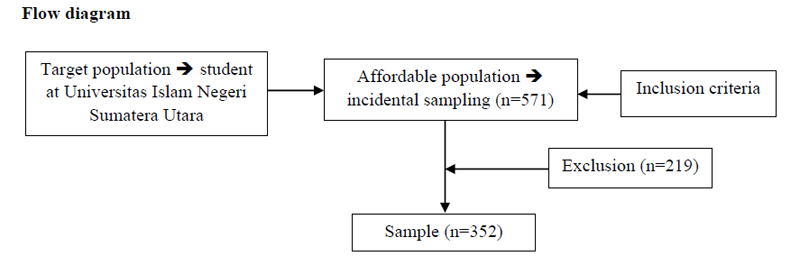
To avoid selection bias, this study established sample eligibility criteria. The sample was determined by purposive sampling, with the specified criteria: 1) willing to become respondents; 2) fill out the questionnaire completely; and 3) the status of active students in the universities studied. Furthermore, 571 respondents who filled out the questionnaire were obtained, and 352 were used as samples that met the inclusion criteria. Exceptions to the sample were because students did not complete the questionnaire and alumni because they were inactive. An example of the recruitment process is through student organizations at the Universitas Islam Negeri Sumatera Utara. Fig. (1) shows a Flowchart of the study criteria:
2.3. Data Collection
Data was collected using an online questionnaire with the addition of 2 variables, namely characteristics and access to information. Questionnaires were sent through a Google form, then distributed by student organization members to the target population. Indicators of PHBS include: 1) consumption of nutritious food, 2) exercise and rest habits, 3) habit of washing hands with soap, 4) maintaining environmental cleanliness, 5) smoking behavior, 6) use of masks, 7) consumption of water minerals, 8) eating perfectly cooked food, 9) utilization of health facilities, and 10) praying habit. The number of questions is 30 items, consisting of 4 scales such as 4 = yes, always, 3 = yes, often, 2 = sometimes, and 1 = no. In addition, the minimum and maximum scores are 30 and 120, respectively.
The information access questionnaire was developed based on [16]. It consists of 4 indicators, namely 1) source of information, 2) frequency of accessing information, 3) ease of access, and 4) time of accessing information. The number of questions is 4 items, and this study refers to previous results using a mixed method design, which combines quantitative and qualitative methods to enrich understanding in the scientific field. This method is developing in health sciences, social psychology, and education [17]. The sample size of the quantitative approach uses the Slovin formula, and the probability sampling technique determines the sample. Quantitative data analysis uses SEM-PLS, and the qualitative approach was carried out using a Focus Group Discussion. The data were analyzed using TAM (Technology Acceptance Model) to measure technology acceptance. A previous study analyzed the relationship between acceptance of information technology and other variables [16].
Internal consistency was measured using Cronbach alpha and consistent when > 0.6. The instrument scale consists of 4 scales, namely 4 = yes, always, 3 = yes, often, 2 = sometimes, and 1 = no. The minimum score is 12, and the maximum is 48. Access to information is classified into high (score 25 – 48) and low (score 12 – 24) categories.
This study has received ethical approval from the Health Research Ethics Committee No: RK.07/KEPK/STIK/IV/2020. The questionnaire used was previously tested for validity and reliability by 30 respondents. This test was conducted at the Faculty of Science and Technology, State Islamic University of North Sumatra, Medan, and the results of the questionnaire test are declared valid and reliable.
2.4. Statistical Analysis
Characteristic data were analyzed using frequency distribution. Analysis of the application of PHBS was conducted by path analysis using PLS Version 3.0 software. The hypothesis was accepted based on the significance level of p-value < 0.05 or T-statistic > 1.96. The questionnaire is equipped with a respondents’ consent form. Outer model analysis was conducted to assess the relationship between latent variables and indicators. The indicator declared the value of the outer model (> 0.5) is valid. The hypothesis was proven using path analysis with PLS application software, and a significant T value was obtained after the bootstrapping stage. After the process, the result of the T-statistic is significant when the value is > 1.96.
Research hypotheses: 1) there is an effect of respondent's characteristics on the consumption of nutritious food. 2) there is an effect of the respondent's characteristics on exercise habits. 3) there is an influence of the respondent's characteristics on the habit of washing hands. 4) there is an effect of the respondent's characteristics on environmental cleanliness. 5) there is an effect of respondent's characteristics on smoking habits. 6) there is an effect of the respondent's characteristics on the habit of using a mask. 7) there is an effect of respondent's characteristics on drinking water consumption. 8) there is an effect of respondent's characteristics on the consumption of cooked food. 9) there is an effect of respondent's characteristics on the utilization of health facilities. 10) there is an effect of respondents' characteristics on prayer habits. 11) there is an effect of access to information on the consumption of nutritious food. 12) there is an effect of access to information on exercise habits. 13) there is an effect of access to information on handwashing habits. 14) there is an effect of access to information on environmental cleanliness. 15) there is an effect of access to information on smoking habits. 16) there is an effect of access to information on the habit of using masks. 17) there is an effect of access to information on drinking water consumption. 18) there is an effect of access to information on the consumption of cooked food. 19) there is an effect of access to information on the utilization of health facilities. 20) there is an effect of access to information on prayer habits.
3. RESULTS
The results of descriptive data analysis based on the respondents’ characteristics are shown in Table 1. The hypothesis testing is shown in Fig. (2), and Table 2 shows the significant results.
| Characteristic | Frequency | Percentage |
|---|---|---|
| Age | ||
| < 20 | 166 | 47.2 |
| > 20 | 186 | 52.8 |
| Gender | ||
| Man | 49 | 13.9 |
| Women | 303 | 88.1 |
| Faculty | ||
| Sains dan Health | 86 | 24.2 |
| Non sains | 266 | 75.6 |
| Area of residence | ||
| Village | 252 | 71.6 |
| City | 100 | 28.4 |
| Variable | Frequency | Percentage |
|---|---|---|
| Information | ||
| High | 183 | 52 |
| Low | 169 | 48 |
| Nutritional food | ||
| Good | 307 | 87.2 |
| Not good | 45 | 12.8 |
| Sport | ||
| Routine | 217 | 61.6 |
| Not a routine | 135 | 38.4 |
| Wash hand with soap | ||
| Routine | 325 | 92.3 |
| Not a routine | 75 | 21.3 |
| Environmental hygiene | ||
| Good | 277 | 78.7 |
| Not good | 75 | 21.3 |
| Smoke | ||
| Yes | 207 | 58.8 |
| Not | 145 | 41.2 |
| Using a mask | ||
| Routine | 338 | 96 |
| Not a routine | 14 | 4 |
| Water consumption | ||
| Good | 259 | 73.3 |
| Not good | 94 | 26.7 |
| Eat perfectly cooked food | ||
| Yes | 316 | 89.8 |
| Not | 36 | 10.2 |
| Utilization of health facilities | ||
| Yes | 22 | 6.3 |
| Not | 330 | 93.8 |
| Pray | ||
| Routine | 323 | 91.8 |
| Not a routine | 29 | 8.2 |
The results of a cross-sectional survey on 352 samples show the characteristics of the majority of the sample are > 20 years old, 186 (52.8%), minimum age of 17 years, and a maximum of 23 years. Sex was dominated by women, 303 (88.1%), non-science faculty 266 people (75.6%), and the majority of respondents live in villages with 252 people (71.6%) compared to 100 respondents living in urban areas.
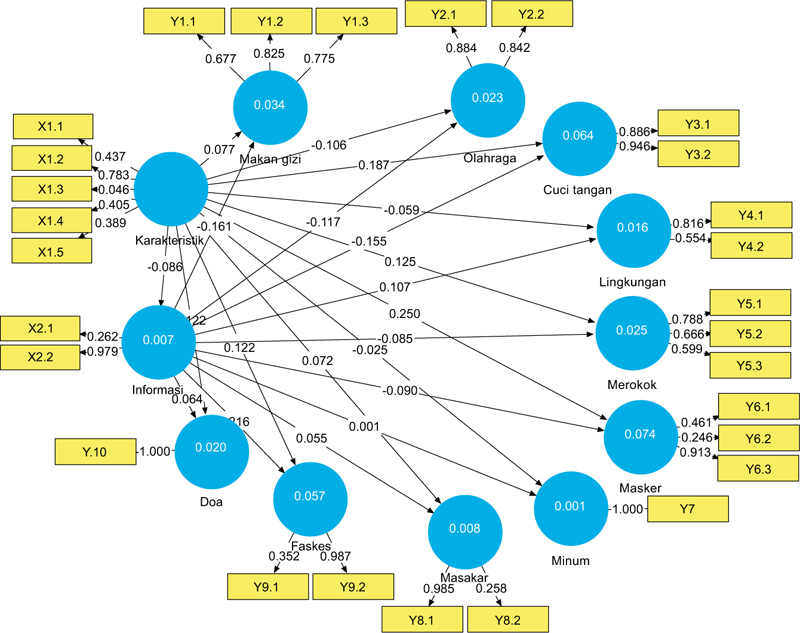
Access to information in the high category was dominated by 183 students (52%), consumption of nutritious food in the good category, 307 people (87.2%), exercise habits in the routine category, 217 people (61.6%), the habit of washing hands with soap in the routine category, 325 people (92.3%), environmental hygiene in the good category, 277 people (78.7%), having smoking habits or smoking family members, 207 people (58.8%), the habit of using masks in routine category, 338 people (96%), the habit of consuming water in the good category, 259 people (73.3%), having the habit of eating food that is not cooked perfectly, 316 people (89.8%), the majority do not use health facilities, 330 people (93.8%), having the habit of praying, 323 people (91.8%). Good criteria based on a questionnaire score of 8-12 respondents answered 3 questions with a positive answer of “yes, always” weighting (4) or “yes, often” weighting (3). The criteria are not good based on a questionnaire score of 4-7 respondents answered 3 questions with negative answers “sometimes” with a weight of (2) or “no” weight of (1). Furthermore, Fig. (1) shows the relationship between latent variables and indicators in the outer model. Referring to the concept of SEM-PLS indicator declared valid determined based on the Cronbach loading factor value of more than 0.7, composite reliability value above 0.6, and AVE value greater than 0.5 [18].
Valid indicators measuring the characteristics of respondents are gender (0.783), the frequency indicator of accessing information is declared valid (0.979), only 1 indicator of the habit of using masks is valid (0.973), and 1 indicator of health facility utilization is valid (0.987). The indicators that were declared entirely valid were the consumption of nutritious food, exercise, hand washing, environmental hygiene, smoking, drinking water consumption, cooking food, and praying habits (> 0.5).
The relationship between latent variables and indicators is known from the analysis of the outer model. An indicator is declared valid if the value of the outer model is (> 0.5). Proof of the hypothesis through the relationship path using the PLS application with the bootstrapping stage the t-statistical value is significant if (t-statistics > 1.96.) After the bootstrapping process, the results of the t-statistics are shown in Table 3.
| Hypothesis | Original Sampel | Sample Mean | Standard Deviation | T statistic | P-value |
|---|---|---|---|---|---|
| Information -> consumption of nutritious food | 0.161 | 0.166 | 0.062 | 2.603 | 0.009* |
| Information -> exercise habits | 0.117 | 0.121 | 0.059 | 1.970 | 0.049* |
| Information -> hand washing habits | 0.155 | 0.155 | 0.053 | 2.941 | 0.003* |
| Information -> utilization of health facilities | 0.216 | 0.218 | 0.047 | 4.631 | 0.000* |
| Individual characteristics -> use of masks | 0.250 | 0.241 | 0.115 | 2.167 | 0.031* |
Table 3 proves the hypothesis through the variable relationship path (X1, X2), respondent characteristics, and access to information on 10 indicators of clean and healthy living behavior in preventing COVID-19, using the PLS application with a bootstrapping stage. After the process, the results of the t-statistic are significant if (t-statistic > 1.96), so there are a few accepted hypotheses, namely: information affects the consumption of nutritious food, the T-statistic value is 2.603, the mean is 0.166, and the standard deviation is 0.062. Information affecting exercise habits T-statistic value 1.97, mean 0.121, and standard deviation 0.053. Information affecting hand washing habits is T-statistic value was 2,941, mean was 0.053, and standard deviation was 0.155. Information affecting the use of health facilities is T-statistic value of 4.631, mean of 0.218, and standard deviation of 0.047. Individual characteristics affect the use of masks, the T-statistic value is 2.167, the mean is 0.241, and the standard deviation is 0.115. Because access to information supports the clean and healthy behavior of students, the government needs to increase the socialization of the application of clean and healthy living behavior through television, radio, and social media as well as easy access to information for all regions in Indonesia.
The research paradigm refers to the L. Green concept that behavior is influenced by supporting, motivating, and enabling factors. However, the researcher assumes that there are other factors, namely information media, that influence clean and healthy living behavior. Therefore, the hypothesis is set to refer to the L. Green concept and add information access variables.
4. DISCUSSION
Gender is a valid indicator to measure the characteristics of respondents. The majority of respondents are female; this is supported by data from the Central Statistics Agency in 2018, where the ratio of male to female sex is 1:10. This data is sourced from 25 regencies and 8 cities in North Sumatra Province [19]. All research respondents were students from North Sumatra Province, Indonesia. The greater distribution of female sex ratios influences behavior and competition among women themselves. Therefore women have more courage to compete in everything. Other indicators of age, faculty, ethnicity, and area of residence are not valid. The age range of the respondents is 17 – 23 years, the age category of young adults has the same development, so there is almost no difference in the age range, which is declared invalid by the age indicator.
The degree of health of a community group is influenced by genetics, which is inherited from parents, the availability of health facilities, the environment in which they live, and individual behavior. Individuals will change their behavior when they are in a threatening situation. This explanation is based on the health belief model, situations that threaten health and individuals who have the belief that they are in a dangerous situation require individuals to adopt behaviors that support health [20].
Support for individual behavior to implement clean and healthy living behavior during a pandemic can reduce the spread of COVID-19, but a collaborative approach by building community immunity through vaccination must be carried out. Moreover, Shi's research (2021) states that Covid-19 has a permanent impact in Indonesia [21]. Giving vaccines is important to prevent the spread of the pandemic [22]. The pattern of the COVID-19 pandemic is unpredictable, therefore a strict step that needs to be taken is to increase vaccination [23]. Other researchers mentioned that the COVID-19 outbreak created job opportunities in pharmaceutical, vaccine, and laboratory tests [24].
The results of the study prove that information affects clean and healthy living behavior; it is necessary to share information through social media such as Facebook, Twitter, or Instagram. Relevant to previous research, it is stated that social media is the right tool to build behavior in society because it is widely used, and is efficient, and convenient [25]. Respondents apply clean and healthy living behavior by consuming nutritious food, doing sports activities, washing hands, and utilizing health facilities because of the information submitted by the Ministry of Health from time to time the number of new patients who were declared positive, died and recovered through television, electronic paper, web, and other social media. This number continues to grow so that the information provides a positive stimulus for the community to implement clean and healthy living behaviors. The results of this study have similarities with Kim's previous research (2018), which states that health education is a way of providing information and knowledge to a community to increase understanding of health and adopt healthy behavior [12, 20]. Behavior change is supported by effective communication with the community [26]. A good understanding will encourage individuals to adopt behaviors that are beneficial for themselves.
On the other hand, individual behavior to adopt healthy behavior is determined by independent responsibility. Martini (2019) argues that behavior is driven by a desire to do and a caring attitude towards something. This behavior change is driven by the role of health promotion activities that prioritize individual responsibility for the environment [27]. Health promotion in the UK emphasizes individual responsibility so that they want to change healthy living behavior [28, 27]. The age of respondents is in the adult category, having the ability to decide independently to adopt behaviors that they think are beneficial, so the trend of positive data. This is to the results of the study that individual characteristics affect the use of masks. In fact, in public places such as markets, and places of worship, people wear masks, but groups of children aged < 12 years, both in schools and places of worship, do not wear masks. Previous research explained that the differences in age and gender showed significant behavioral differences [29].
Concerns about the risk of transmission of COVID-19 in children are supported by previous research that coronavirus infection also occurs in the group of children, and almost half of the cases are asymptomatic. Radiological examination results were declared normal. It is suspected that this transmission occurred due to contact with adults or being in a pandemic area. On the other hand, children do not yet have responsibility for themselves, especially for health problems. Even a survey of the group of children aged 10 years and over found out the results of the Basic Health Research on correct hand washing habits of 49.8% [30]. This means that the potential for transmission in this group is possible. The spread of COVID-19 infection can be stopped through the habit of washing hands with soap or hand sanitizer. Health promotion activities such as health education through the provision of information, and social and environmental approaches will increase understanding and beneficial behaviors, to adopt healthy behaviors [12].
The advantage of this research is that the findings on the role of information expand the theory of behavior change based on L. Green's theory, and the theory of health belief models has the privilege of the concept of self-efficacy, a person's belief to act. Beliefs will be stronger encouraging individuals to act supported by the information they receive. The community plays a role in suppressing the spread of COVID-19. Naeini argues that success in preventing the spread of COVID-19 is determined by community involvement and plays an important role in the spread of this disease [31]. Public awareness of the spread of COVID-19 is determined by trust in health information. Information about COVID-19 affects people's social behavior. The public does not take safe actions to protect themselves from the COVID-19 outbreak due to the information crisis [32]. Current health problems can be overcome by adopting a holistic approach [9] to community empowerment and building cross-sectoral policies to foster public trust [9]. Similarly, research conducted by Fuller et al. (2021) found that uncertain health information resulted in public doubts about vaccines, therefore a policy of removing systematic barriers must be carried out [33].
The results of the study apply to the study population, which has the same characteristics as the adult age sample and is in the same campus environment situation. The population of Indonesia currently reaches 300 million people and lives in areas separated by islands, so the dissemination of information widely needs to be increased by emphasizing personal responsibility to invite people to adopt clean and healthy lifestyles. Education on clean and healthy living behaviors starting from household members can help increase the scope of clean living in the community [34]. The role of such information is large and effective. The use of information media must take into account the ease of access, cost, speed, and content of the information for all age groups. It is essential to package health information properly so that it is right to target.
CONCLUSION
Consumption of nutritious food, exercise, hand washing, use of masks, environmental hygiene, smoking habits, drinking water consumption, cooking food, utilization of health facilities, and prayer habits are 10 indicators of proper clean and healthy living behavior to prevent the spread of the COVID-19 infectious disease. Information is the right way to change behavior. The delivery of information to change behavior through the media must be innovative. Information is presented well and attractively makes it easier for the public to accept and implement the message conveyed. Individual characteristics affect the use of masks. Research respondents are students, so they have the independence to make choices to act based on considerations that they think are useful.
Practical benefits are the results of this study that can be used as corrections for practitioners, especially health promotion officers, so that health policy programs can be implemented properly through well-packaged messages or information, utilizing media that are widely used by the community, and implementing good message management strategies in providing services and easy access to information.
The Indonesian government should instruct the ministry of education and culture and the ministry of higher education to implement clean and healthy living behaviors from elementary school to university. Establish policies so that educational institutions support health promotion programs, and are directly involved by placing posters, banners, billboards, or running texts at educational institutions at entrances, parking lots, or locations that are easily accessible to students. It is expected that behavior modification is based on conditioning through stimuli that are around the individual.
The Directorate General of Health Promotion and Community Empowerment of the Ministry of Health of the Republic of Indonesia promotes health promotion through social media such as Facebook, Instagram, YouTube, and Twitter, motivating the public to be directly involved in health promotion, such as holding various competitions for the use of masks, implementing clean and healthy living behaviors, implementing health protocols through TikTok at national health day events, commemorating national nutrition day, and so on.
This study complements the behavioral concept of previous researchers. The originality of the research lies in the difference in behavior, according to L. Green, which is influenced by predisposing, reinforcing, and enabling factors. The results of the study found the role of information in encouraging changes in a person's behavior. The frequency of accessing information affects individual beliefs. The more often you receive information, the stronger it forms individual beliefs so that it encourages them to change behavior.
The results of this study provide input to academics, especially in the field of public health, to develop knowledge through behavior change research using new variables in the adult group, such as information needs and the availability of free information so that effective strategies for delivering health information become more effective. Further researchers can conduct research using the theory of the social-ecological model using social, community, organizational, and interpersonal variables that can influence changes in individual behavior.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Health Research Ethics Committee of the College of Health Science “Maluku Husada (No: RK.07/KEPK/STIK/IV/2020).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All human procedures followed were by the guidelines of the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants of this study.
STANDARDS OF REPORTING
STROBE guidelines have been followed.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the manuscript.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

