All published articles of this journal are available on ScienceDirect.

Investigating the Waste Management Knowledge and Performance of Health Personnel in the COVID-19 Epidemic
Authors Info & Affiliations
Abstract
Objective:
The aim of this study was to investigate the waste management knowledge and performance of health personnel in the COVID-19 epidemic.
Methods:
This cross-sectional study was conducted on 470 of personnel in hospitals, health centers, and affiliated subordinate units of Jiroft University of Medical Sciences were selected utilizing the available sampling method from June to December 2020. The researcher-made questionnaire was developed utilizing available articles and books in the field of waste. The results were analyzed by SPSS software version 24 and independent t-test and Kruskal-Wallis tests.
Results:
According to the results of study, the status of information, production, and collection of waste in employees were desirable, but separation, transportation, and recycling were not appropriate. Moreover, there was a statistically significant difference in information (p = 0.000), production (p = 0.000), collection (p = 0.000) and general waste management (p = 0.001) among health centers. Also it was a significant relationship between residence (p = 0.006), education (p = 0.029), and location of work (p = 0.001) with waste management. Samples living in the village had a higher average score than city residents. The location of work also showed that the employees of the Health homes had a higher waste management score than other health centers.
Conclusion:
According to the low performance of employees working in cities and hospitals in the field of waste separation, transportation and recycling, it is recommended that continuous training of employees electronically and virtually (preparing a short video on how to sort and recycle waste, inviting a recycling management specialist for training, role-playing). Also it is importance to improve performance and motivation and the existence of practical rules, instructions and adequate monitoring.
1. INTRODUCTION
Increasing population and continuous expansion of cities and the expansion of hospitals and health centers raise the quality in public health, as well as the prevalence of COVID-19. Using N95 masks, scrubs, glasses, a special gown, gloves, and boots increases infectious waste and hazardous pollution, especially soil pollution and climate change [1]. Such wastes cause health and environmental problems, and, in most cases, their management, due to the facilities and budget, has led to many problems, which makes waste management (production, collection, separation, transportation, and recycling) critical to devote more attention [1].
According to the Organization for Economic Co-operation and Development (OECD), waste management is the processing and conversion of consumables into new products and materials in order to avoid wasting potentially useful materials, reduce material consumption, raw material, energy consumption, air pollution due to burning materials and water pollution resulting from landfilling and reducing greenhouse gas emissions [2].
Efficient waste separation increases the possibility of recycling, and if consumers and employees separate waste carefully and safely, they will enjoy economic and occupational health benefits [3]. If proper waste management is applied, part of the national capital can be returned. In fact, the collection, separation, and recycling of materials are one of the undeniable principles of higher productivity in economics. Clearly, recycling makes consumption levels remain constant and increase even without pressure on primary resources and the environment, which is one of the main manifestations of sustainable development [4]. Globally, the waste management sector faces numerous challenges. Currently, 3.4 to 4 billion tons of municipal and industrial solid waste and up to 300 million tons of hazardous waste (infectious and medical) are produced annually worldwide [4]. The issues caused by waste to humans and the environment include: health hazards, ecosystem degradation, soil and water pollution, as well as greenhouse gas emissions, which are more evident in developing countries [5]. According to the South Korean Ministry of Environment [6], about 295 tons of COVID-19 medical waste was generated from early February to early March 2020, of which 61% was allocated for hospitals, 21% for temporary isolation facilities and 18% for health centers [7].
According to Poudel’s study in 2010, infectious health waste was introduced as the second most hazardous waste in the world, and it should be properly managed by trained staff in an organization. The lack of training for hospital staff and the public on waste collection and recycling were the main mentioned problems [8], and government support of hospitals is vital to provide regular training to hospital staff on the proper collection of infectious and non-infectious waste [9]. In Wang et al.'s study, hospitals in China were identified as potential sources of environmental pollutants from diagnostic, laboratory, and research activities [10]. In the study of Joachim Vogt et al., the rate of separation and recycling of waste was very low, and it was reported at about 23% [3].
The importance of a waste management plan in Iran is also important in the sense that waste components and compounds can be recycled up to about 60 to 70% [1]. Inadequate management in such a crisis poses potential risks to health personnel and causes to increase in the transmission of the virus among them. Therefore, motivation and competition will be created by conducting research in the field of waste management for hospitals and health centers and affiliated units and familiarity with their status in order to protect the environment, which makes it possible to apply effective interventions. Therefore, the aim of this study was to investigate the waste management knowledge and performance of health personnel in the COVID-19 epidemic (Fig. 1 and Table 1).
| Waste Management Components | Virtual Lessons |
|---|---|
| Separation | • Prepare a video clip of the following activities: • Tele-education for the use of three trash cans written on each: dry waste and wet and perishable waste • Training staff to properly separate by preparing pamphlets, Philip charts and What Sapp • Teaching in schools to influence families through Adobe Connect software |
| Transportation | • Forming virtual groups and raising the sensitivity of employees • Play a role in the proper transfer of waste • Training employees who do not behave properly through televisions installed in health centers |
| Recycling | • Invite a recycling management specialist for education and send in virtual groups • Existence of strict rules and monitoring of instructions • Forming discussion groups of 6 to 8 people in the health center |
2. MATERIALS AND METHODS
2.1. The Study and Setting
This cross-sectional study was conducted on 470 personnel in hospitals, health centers, and affiliated subordinate units of Jiroft University of Medical Sciences were selected utilizing the available sampling method from June to December 2020.
Inclusion criteria consisted of at least 2 years of work experience for employees in health centers affiliated with Jiroft University of Medical Sciences, and informed consent to participate in the study; and the exclusion criterion was non-cooperation. 40% of health centers affiliated with Jroft University of Medical Sciences were randomly selected as the research sample. The samples were from Jiroft city (10 centers), Anbarabad city (3 centers), Kahnooj city (4 centers), Faryab city (1 center), Manojan city (4 centers), Ghale Ganj city (4 centers), Rudbar city (4 centers) and available sampling was conducted in each health center. Therefore, after stating the study purpose and data confidentiality, and the individuals' authorization, the questionnaire link was shared with them on social media. Considering the prevalence of waste management and recycling at 23% in a similar study in Germany (3), applying the formula to estimate the prevalence and 95% confidence level, considering an error of 0.04, the sample size was calculated at 428 health personnel. According to the 10% probability of sample loss, the desired sample size was 470 (Fig. 2).
2.2. Data Collection
The data collection consists of two tools. The first one consists of demographic information and the second consists of 6 sections. The components of the waste questionnaire included 11 items on information questions about waste status, 5 items on waste generation, 7 items on the collection, 10 items on separation, 6 items on transportation, and 7 items on recycling based on a five-point Likert scale (strongly agree 5, and strongly disagree 1). In designing items, the 4th item in the information section, item 7 in the collection section, items 3-7-10 in the separation section, items 1-2-2-4 in the transportation section, and items 1 and 7 in the recycling section had inverted scoring. The lowest score was considered 46 and the highest was 230.
The researcher-made questionnaire was developed utilizing available articles and books in the field of waste. The questionnaire validity was confirmed by 7 environmental health and related experts. Finally, the content validity index score was calculated more than 0.85 for the questions of all model constructs. The questionnaire reliability was confirmed by 15 health personnel with higher than 0.80 Cronbach's alpha coefficients of all components
2.3. Ethics Approval
This project acquired an ethical committee approval from the Jiroft University of medical science (IR.JMU.REC.1399. 034).
2.4. Data Analysis
Descriptive and inferential statistical methods were used to describe and analyze the data. Data were expressed as mean (standard deviation) for quantitative data and as frequency (percentage) for qualitative data. The results were analyzed by SPSS software version 24 and independent t-test and Kruskal-Wallis tests.
3. RESULTS
The range of participants' age was 20 to 56 years with a mean age of 32.16±7.03 years. The 341 (79.7%) participants were female and 87 (20.3%) were male (Fig. 3 and Table 2).
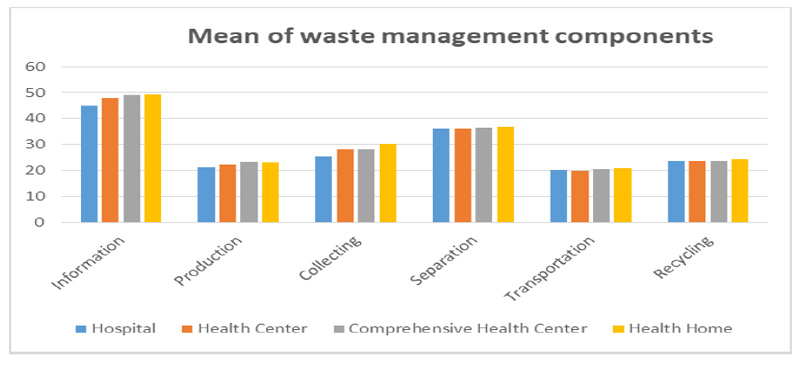
According to the results of the Kruskal-Wallis test, the status of information, production, and collection of waste in employees were desirable, but separation, transportation, and recycling were not appropriate. Moreover, there was a statistically significant difference in information (p = 0.000), production (p = 0.000), collection (p = 0.000) and general waste management (p = 0.001) among health centers (Table 3).
| Variable | N | % | |
|---|---|---|---|
| Age | 20-30 | 181 | 42.3 |
| 30-40 | 182 | 42.5 | |
| 40-50 | 65 | 15/2 | |
| Gender | Female | 341 | 79.7 |
| Male | 87 | 20.3 | |
| Education | Diploma and less | 118 | 27.6 |
| Associate Degree | 52 | 12.1 | |
| Bachelor | 190 | 44.4 | |
| MA | 42 | 9.8 | |
| PhD | 26 | 6.1 | |
| Marital Status | Married | 309 | 72.2 |
| Single | 113 | 26.4 | |
| Widow | 2 | 0.5 | |
| Divorced | 4 | 0.9 | |
| Residence | Private | 245 | 57.2 |
| Rental | 95 | 22.2 | |
| Organizational | 54 | 12.6 | |
| Other | 34 | 7.9 | |
| Habitat | City | 255 | 59.6 |
| Village | 173 | 40.4 | |
| Income | Under one Million | 10 | 2.3 |
| One to two Million | 38 | 8.9 | |
| 2 to 5 Million | 308 | 72 | |
| 5 Million and more | 72 | 16.8 | |
| Total | 428 | 100 | |
| Variable | Hospital | Health Center | Comprehensive Health Center | Health Home | P-Value | Minimum | Maximum |
|---|---|---|---|---|---|---|---|
| Standard Deviation ± Mean | |||||||
| Information | 44.87±5.48 | 47.88±6.1 | 49.13±5 | 49.31±4.5 | 0.000 | 11 | 55 |
| Production | 21.36±3.5 | 22.35±2.9 | 23.37±2.5 | 23±2.4 | 0.000 | 5 | 25 |
| Collecting | 25.40±6.7 | 28±5.6 | 28.26±4.85 | 30.12±4.39 | 0.000 | 7 | 35 |
| Separation | 36±5.6 | 36±4.27 | 36.26±3.92 | 36.60±3.82 | 0.80 | 10 | 50 |
| Transportation | 20.19±4.92 | 19.73±4.60 | 20.34±4.38 | 20.65±4.38 | 0.4 | 6 | 30 |
| Recycling | 23.54±2.95 | 23.81±3.54 | 23.74±3.63 | 24.21±3.54 | 0.35 | 7 | 35 |
| General waste management | 171.47±21.50 | 177.87±20.21 | 181.12±16 | 183.89±15.84 | 0.001 | 117 | 216 |
| Variable | Waste Management | P-Value | ||
|---|---|---|---|---|
| Mean | Standard Deviation | |||
| Age | 20-30 | 179.72 | 18.40 | 0.26 |
| 30-40 | 179.40 | 18.25 | ||
| 40-50 | 184.02 | 15.40 | ||
| 50-60 | 197.71 | 16.87 | ||
| Gender | Male | 181.79 | 18.94 | 0.2 |
| Female | 179.98 | 17.96 | ||
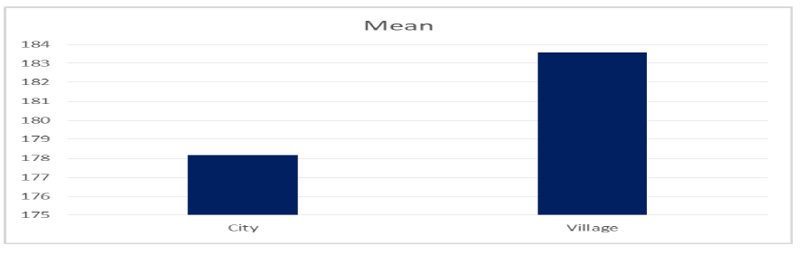
| Habitat | City | 178.17 | 19.50 | 0.006 |
| Village | 183.57 | 15.46 | ||
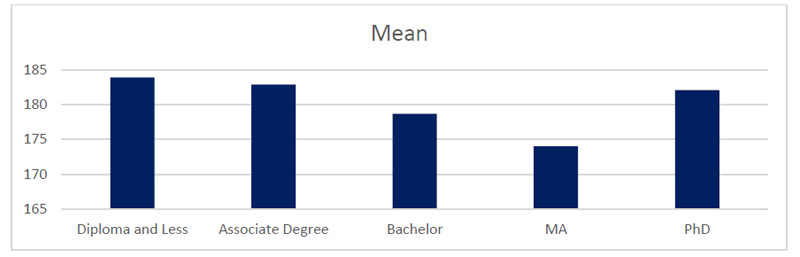
| Education | Diploma and Less | 183.88 | 16.56 | 0.029 |
| Associate Degree | 182.86 | 16.66 | ||
| Bachelor | 178.69 | 18.23 | ||
| MA | 174.02 | 21.27 | ||
| PhD | 182.07 | 19.28 | ||
| Working Place | Hospital | 171.47 | 21.50 | 0.001 |
| Health center | 177.87 | 20.21 | ||
| Comprehensive Health Center | 181.12 | 16.09 | ||
| Health home | 183.89 | 15.84 | ||
| Marital Status | Married | 180.29 | 17.57 | 0.43 |
| Single | 180.05 | 19.89 | ||
| Divorced | 189 | 13.43 | ||
| City | Jiroft | 178.51 | 18.92 | 0.08 |
| Anbar Abad | 193 | 6.6 | ||
| Kahnoj | 182.57 | 18.45 | ||
| Rodbar | 175.96 | 19.42 | ||
| Manojan | 178.19 | 17.01 | ||
| Faryab | 183.85 | 18.95 | ||
| Galeh Ganj | 179.90 | 16.66 | ||
| Residence | Private | 182.45 | 17.17 | 0.08 |
| Rental | 177.26 | 19.24 | ||
| Organizational | 178.16 | 19.44 | ||
| Other | 177.32 | 18.59 | ||
| Income | Under one Million | 176.80 | 24.73 | 0.9 |
| One to two Million | 181.89 | 17.77 | ||
| 2 to 5 Million | 180.30 | 17.63 | ||
| 5 Million and More | 180.25 | 19.83 | ||
The results of the Kruskal-Wallis test showed that there was a significant relationship between residence (p = 0.006), education (p = 0.029), and location of work (p = 0.001) with waste management. Samples living in the village had a higher average score than city residents. Regarding education, the score of waste management of individuals was decreased by increasing the level of education except in Ph.D groups. The location of work also showed that the employees of the Health homes had a higher waste management score than other health centers, (Table 4).
4. DISCUSSION
The research results showed that the knowledge of employees about waste management and their performance in the production and collection of waste caused by COVID-19 was desirable, but their knowledge and practice about the separation, transportation, and recycling of waste caused by COVID-19 were not desirable. The results also showed that for employees who were more knowledgeable about waste management, their performance scores were higher in the production and collection of waste. Furthermore, health personnel living in the village and working in the Health homes had a higher average score than the employees working in the city. Regarding education, the score of waste management decreased with the increasing level of education except in Ph.D groups.
The research results showed that employees working in all health centers acquired adequate knowledge about the production and collection of waste caused by COVID-19. Consistent with our study, in the study of Khorpisheh et al., individuals' knowledge and attitudes were appropriate about waste management [11]. But in the study of Mahmoodabad et al., public awareness was weak about waste management [12]. Sample selection discrepancy can be one of the reasons for differences. In Mahmoodabad’s study, all people living in the city were selected as the sample size, but in our study, they were health personnel. In addition, COVID-19 prevalence and culture and geographical environment diversity are subsequent causes.
The performance of health staff in the Health homes in terms of production and collection was better and more desirable than in other health centers, especially hospitals; however, in Pazokinejad’s study, individuals had low performance in waste management [13]. Additionally, in the study of Mahmoodabad et al., physicians and nurses had only a 27% role in transferring waste management information to other employees [12]. But in Tabeshian’s study, physicians working in health centers and hospitals had a 63% and health personnel a 24% role in the knowledge transmission on waste management and it seems that physicians and hospital staff are more aware of waste management than employees in the Health homes [14].
The results indicate that the performance of health personnel in different locations is not the same, and more extensive studies should be conducted. However, the status of waste collection and separation within hospitals was evaluated as fine in the study of Nourmohammadi et al. [15]. Organizing suitable structures such as waste storage containers like plastic bins and durable and suitable garbage bags is one of the proper and desirable waste management reasons. Furthermore, waste caused by COVID-19 is one of the reasons for the discrepancy in the results of the present study. Due to less workload and referrals in the Health homes than in hospitals; health personnel can pay more attention to the collection and separation of waste of COVID-19 virus disease. In addition, patients referred to hospitals are in a worse physical condition and require more medical care, which in turn can generate more waste.
There is a maximum of 2 or 3 health personnel in the Health homes, but in hospitals, due to the considerable number of health personnel, collective participation is needed. Therefore, the results show that health personnel working in Health homes and health personnel living in rural areas were more sensitive to proper waste management than those working in the city, and were more careful about the benefits of waste management. But in Tayebi 's study, people living in rural areas did not know the methods of waste disposal and waste management, thus proper waste management in rural areas requires proper interaction of people, which should be provided by education and public information to warn the locals about the consequences of improper waste disposal in addition to the damage to the environment [16]. In the present study, conflicting results were observed regarding education and waste management. With the exception of PhDs, in other groups, with increasing education, performance in waste management decreased. But in other studies [17, 18], people with higher education had better performance.
The status of production and collection of waste caused by COVID-19 was favorable in our study and was consistent with the study of Namdar et al., Mobaraki et al. and Motaghi et al. [19-21]. In our study, 75% of health personnel had poor waste collection performance. Same as the study of Moradi and Barakat, in which the waste collection was not fulfilled well [22]. Therefore, continuous training of staff is necessary, as training has a significant effect on increasing awareness and encouraging employees to observe health issues and take the disease seriously. Also, according to the study of Nourmohammadi et al., storage and separation of infectious and non-infectious wastes were not fine accomplished in the hospital [15], which was consonant with the study of Mohammadian et al. [23]. In Rhee's study in 2020 in South Korea, appropriate and timely guidelines for training, collection, and separation of COVID-19 waste were properly implemented, and cooperation between people and staff was desirable [7]. In Spain, in order to produce less waste and collect and sort the waste of COVID-19, they launched a program of online shopping and home delivery at a reasonable and affordable price. But they also emphasized training people and health personnel in waste management [24].
In our study, the overall status of waste management in hospitals was poor compared to Health homes, which is consistent with a study in Bazrafshan Province [25], but in Tehran and northern parts of Iran, the situation of waste management was relatively favorable in hospitals [26]. The geographical environment and suitable infrastructure in the center of Iran are the reasons for the difference.
The state of knowledge and practice of individuals regarding separation, transportation, and recycling was not desirable in our study. In many developing countries, which are relatively low-income, the waste recycling status is not fine [27]. In the United States, the COVID-19 recyclable waste collection program was discontinued due to the dangers of the COVID-19 outbreak [24], but the United Kingdom carried out the COVID-19 recycling program properly [28]. Kulkarni et al. emphasized a decentralized approach to the waste management system in their study, so that waste treatment and recycling are done besides the waste production. This reduces the burden of waste collection and transportation, and it can significantly reduce the risk of infection in the involved personnel [29]. Such wastes are a threat, so it seems that the lack of awareness and performance of staff regarding the separation and recycling of waste is acceptable in the present study, and it should be done by specialized people with special equipment for separation, transportation, and recycling. In the United States, appropriate methods have been utilized to increase performance and waste management among employees and the public.
The United States Federal Emergency Management Agency (FEMA) recommends developing temporary waste storage and reduction sites between waste generation sites and final disposal sites [30]. For instance, in the UK, to manage the additional waste generated during the COVID-19 pandemic, temporary waste storage capacity has been increased [28].
The status of waste transportation was not desirable in the present study, but Kulkarni et al. carried out a training program, supervision, safety management, and proper waste disposal during the COVID-19 pandemic in their study in order to improve the performance of employees and people; in which, the time and way of medical waste collection related to COVID-19 and their transportation were different from public waste and which it causes to reduce the risk of leakage and damage during the transferring process [31].
CONCLUSION
The situation of knowledge, production, and collection of waste caused by COVID-19 among the staff of the Health homes in the villages was more desirable than the hospital in the cities, and in terms of separation, transportation and recycling, the situation of all staff was not convenient. This shows that despite proper knowledge in the field of production and collection, the performance of individuals in terms of separation and recycling was not appropriate. Therefore, it is suggested that continuous training of employees electronically and virtually (preparing a short video on how to sort and recycle waste, inviting a recycling management specialist for training, role-playing), especially employees working in cities and hospitals, is of particular importance to improve performance and motivation. In addition to increasing knowledge, it is essential to pay attention to rules and guidelines, control and supervision, and use the experiences of other studies.
AUTHOR'S CONTRIBUTION
Conceptualization was done by E.M and F.S. Data curation was done by A.KH and M.T. Formal analysis was conducted by E.M. Investigation was done by Z.S. Methodology was selected by F. S and M.M. Project administration was done by E.M and A.KH. Writing the original draft was done by E.M and F.S, and review & editing were done by M.T and M.M. All authors have read and agreed to the published version of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This project acquired an ethical Committee approval from the Jiroft university of medical science (IR.JMU.REC.1399. 034).
HUMAN AND ANIMAL RIGHTS
No animals were used that are the basis of this study. All human procedures were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed written and verbal consents were taken from all participants prior to data collection.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available from the corresponding author [E.M] upon reasonable request.
FUNDING
The authors were funded for research by Jiroft University of Medical Sciences.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors extend their appreciation to the participants for their cooperation throughout the study. They also appreciate the assistance of the members of the Ethics and Research Boards of Jiroft University of Medical Sciences.

