All published articles of this journal are available on ScienceDirect.

SARS-CoV-2 (COVID-19) Clinical Manifestations and Risk Factors among Healthcare Workers In Palestine
Authors Info & Affiliations
Abstract
Background:
Healthcare workers are the White army compacted the COVID-19 epidemic, and reports worldwide have shown an increase in SARS-CoV-2 among healthcare workers due to their direct interactions with infected patients. This study aimed to examine the clinical manifestations and risk factors for SARS-CoV-2 infection among healthcare workers in Palestine and offer recommendations to ensure health workers' safety and adopt workplace safety policies.
Methods:
This questionnaire-based cross-sectional observational study was conducted using an online questionnaire to collect information about SARS-CoV-2 transmission, signs, symptoms, and treatment reported by healthcare workers. Furthermore, we explored policies, protocols, and practices that make health workers vulnerable to SARS-CoV-2 infection.
Results:
A total of 389 healthcare workers were included, 216 (55.5%) were exposed to the SARS-CoV-2 virus, 173 (44.5%) were infected with the virus, and the prevalence of hospitalization was 16%. The most commonly reported symptoms are fatigue, weakness, and muscle pain. Female healthcare workers experienced a significantly extended duration of symptoms than male workers. Direct contact (working less than 1.5 m) with suspected or confirmed COVID-19 patients and lack of COVID-19 and PPE training were risk factors for COVID-19 infection among HCWs.
Conclusion:
The healthcare system must ensure a safe work environment and adopt policies and procedures to ensure HCW safety, proper training, and resource availability to cope with crises.
1. INTRODUCTION
Coronaviruses (CoVs) are a large family of viruses that cause a plethora of illnesses, ranging from the common cold to more severe diseases, such as Middle East respiratory syndrome (MERS-CoV) and severe acute respiratory syndrome (SARS-CoV) [1]. The outbreak of coronavirus pneumonia started in Wuhan, China. The disease rapidly spread across many states within China as well as globally until it reached Palestine and became known as COVID-19 in 2019-2020 [2].
Healthcare workers are the white army compacting this epidemic, and reports worldwide have shown an increase in COVID-19 among healthcare workers due to their direct interactions with infected patients. Reports in Italy indicate that 20% of healthcare workers managing COVID-19 patients are infected with the virus [3]. In Spain, by March 2020, approximately 15% of healthcare workers had been infected with SARS-CoV-2 [4]. Studies in the UK and USA have shown an increased risk of COVID-19 infection among frontline HCWs and recommended strategies to protect against and minimize infection risk. Some of these strategies include providing personal protective equipment (PPE), including gloves, medical masks, goggles, or face shields, and providing the proper PPE training to achieve full effectiveness and the ultimate goal of protection and life-saving. There has been a more than 3-fold increase in the chances of a positive SARS-CoV-2 test among HCWs compared to other populations [5].
As of 12 February 2022, there were 552,432 COVID-19 cases in Palestine, with 4,983 deaths and 496,452 recovered cases [6]. The WHO-occupied Palestinian territory reports show that COVID-19-infected healthcare workers (HCWs) constitute 2% of COVID-19 cases. Moreover, this number tripled from 1129 cases in October 2020 to 3748 cases in March 2021 [7].
The well-being, health, and safety of HCWs are critical, as they are key forces in maintaining community health, controlling the virus outbreak, and saving lives. Under normal circumstances, HCWs in Palestine face many challenges in providing health care services. Lack of resources, equipment, isolation facilities, and increased workload are all risk factors for COVID-19 transmission [8]. During this pandemic, they faced additional challenges, such as failures in the healthcare system's response, including inadequate PPE, lack of guidelines, training, and long work hours [9].
This study explored the characteristics and risk factors associated with healthcare workers' infection or exposure to SARS-CoV-2 in Palestine. In addition, it offers recommendations to ensure the safety of health workers in the workplace.
2. MATERIALS AND METHODS
A cross-sectional questionnaire-based observational study was conducted among HCWs at different institutions in occupied Palestinian territory to explore healthcare workers' risk factors and characteristics for COVID-19. This study was conducted between December 2020 and April 2021. The targeted respondents were all HCWs with different specialists, working at different hospitals or clinics in the west bank, and having Internet services. Critical ill healthcare workers, healthcare workers who died from COVID-19, and who could not complete the questionnaire were excluded.
The questionnaire was developed after reviewing the literature, reviewed by faculty members of the Pharmacy Department at Birzeit University for accuracy and relevance, and changes made according to the recommendations [2]. A pilot study was then conducted to assess the clarity and appropriateness of the questionnaire.
The final questionnaire was composed of 25 questions divided into five sections. Section one revealed the study objectives, obtained the participants’ consent, and assured the confidentiality of the information provided. Section two consisted of five sociodemographic questions, including age, gender, occupation region, type, and facility. Section three consisted of seven questions evaluating the health system's readiness, HCW's COVID-19 training, PPE training, PPE availability, method of contact with patients, and the following actions after exposure. Section four consisted of 11 questions completed only by COVID- 19 infected respondents regarding signs, symptoms, treatments, comorbidities, smoking status, and length of hospital stay. The questions were multiple-choice, and the respondents could choose more than one answer. Finally, Section five contains three open questions regarding the participants' comments and concerns about the COVID-19 epidemic (Table S1).
The sample size was determined using the online Raosoft calculator with a 95% confidence interval and a 5% source of error; according to the Palestinian ministry of health report, the number of HCWs in 2020 was 14000 [10], the minimum sample size is recommended to be 374. An online survey was launched using social media, e-mails, Facebook, and WhatsApp to target the infected and exposed HCWs.
Data were collected online using Google Forms, converted to a Microsoft Excel spreadsheet, cleared, separated, and coded. Patients with incomplete questionnaires were excluded from the study. Statistical analysis was performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics 22). First, counts within cases and recordings were performed to categorize the data. Descriptive statistics were used to present the data. Pearson's chi-squared test with a 95% confidence interval was used to identify sociodemographic variables associated with the possibility of infection. A second Pearson's chi-square test with a 95% confidence interval was used to assess the association between the characteristics of the infected participants, their treatment regimen, and the intensity of the symptoms.
The Ethical Committee of Birzeit University approved the study at the Faculty of Pharmacy, Nursing, and Health Professions, Birzeit University (reference number BZUPNH2004).
3. RESULTS
Table 1 shows the characteristics of the 389 HCWs. There were 212 (54.5%) males and 177 (45.5%) females variate in their job positions as 98 (25.2%) doctors, 79 (20.3%) nurses, 114 (29.3%) pharmacists, 32 (8.2%) receptionists, 31 (8%) lab technicians, and 35 (9%) maintenance personnel. The participants worked in different healthcare settings, mainly hospitals, with 190 (48.8%).
3.1. Risk Factors and Protective Actions
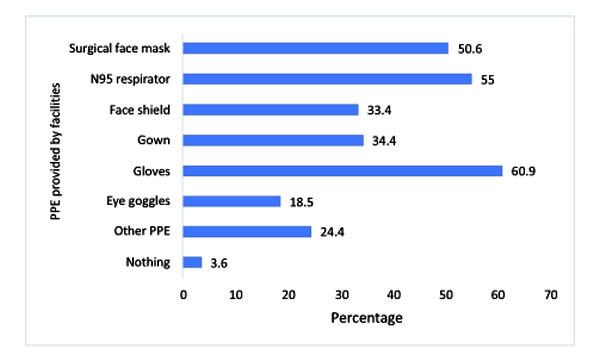
Of 389 respondents, 191 (49.1%) revealed that their institutions provided SARS-CoV-2 safety training, and 346 (88.9%) were provided with PPE. However, when asked if they had been trained in how to use PPE, only 182 (46.8%) said they had been trained. In addition, 63 (16.2%) reported being trained before the pandemic reached Palestine, 133 (34.2%) were trained after the pandemic, and 14 (3.6%) did not remember when they had been trained.
Fig. (1) summarizes the PPE used; gloves and face masks were available to approximately half of the participants.
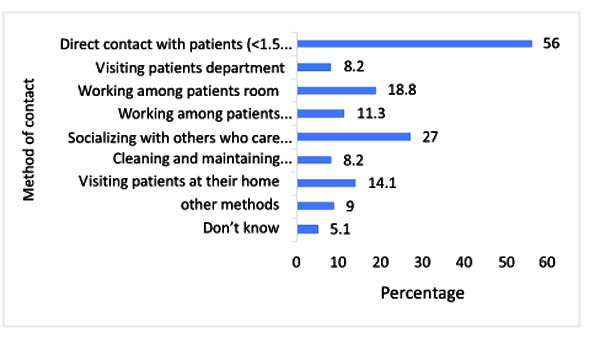
When participants were asked about maintaining a safe distance while dealing with patients, 218 (56%) HCWs answered that they were directly in contact with COVID-19 patients at a distance of less than 1.5 meters as part of their work. The remaining HCWs were visiting or working within the COVID-19 quarantine floor, patients' rooms, or dealing with other workers who directly contacted infected patients or were contacted with patients outside of their work or did not know how they socialize infected patients (Fig. 2).
Associations between demographics, PPE training, direct patient contact, and COVID-19 training were assessed for the risk of COVID-19 infection. Pearson's chi-square test results revealed a significant association between COVID-19 training, PPE availability, PPE training, and COVID-19 infection (p ≤0.001). COVID- 19 trained (32.5%) and PPE-trained personnel (31.3%) were significantly less likely to be infected than were untrained personnel (56.1% and 56%, respectively). Furthermore, institutes that provided PPE (41.6%) than workers unprovided PPE (67.4%) were significantly less likely to be infected (Table 2). In addition, workers in direct contact with COVID-19 patients were significantly more likely to be infected (p = 0.013, 50%) than those who worked farther from patients (37.4%).
As shown in Table 2, participants wearing N95 respirators were significantly less likely to be infected (P= 0.037, 39.7%) than those using other types (50.3%). On the other hand, surgical face mask users were significantly more likely to be infected (P= 0.011, 50.8%) than users of other types (38%). Furthermore, workers aged 18–24 years were significantly more likely to be infected (55%, p = 0.019) than older workers.
| Characteristic | Categories | n (%) |
|---|---|---|
| Gender | Males | 212 (54.5) |
| Females | 177 (45.5) | |
| Age (in years) | 18-24 | 80 (20.6) |
| 25-34 | 121 (31.1) | |
| 35-44 | 91 (23.4) | |
| More than 45 | 97 (24.9) | |
| Occupation | Doctor | 98 (25.2) |
| Nurse | 79 (20.3) | |
| Pharmacist | 114 (29.3) | |
| Receptionist | 32 (8.2) | |
| Lab Technician | 31 (8) | |
| Maintenance | 35 (9.0) | |
| Type of Healthcare Facility | Private Hospital | 97 (24.9) |
| Governmental Hospital | 93 (23.9) | |
| Outpatient Clinic | 77 (19.8) | |
| Pharmacy | 95 (24.4) | |
| More than one facility | 27 (6.9) | |
| Work Place Location (n = 408) | Jerusalem | 70 (18.0) |
| North | 95 (24.4) | |
| Middle | 186 (43.2) | |
| South | 38 (9.8) | |
| Others | 18 (4.6) |
| Variable | Infected with COVID-19 | Not Infected with COVID-19 | p-value | ||
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age | 18-24 | 44 (55) | 36 (45) | 0.019 | |
| 25-34 | 59 (48.8) | 62 (51.2) | |||
| 35-44 | 38 (41.8) | 53 (58.2) | |||
| >44 | 32 (33) | 65 (67) | |||
| Gender | Female | 83 (46.9) | 94 (53.1) | 0.38 | |
| Male | 90 (42.5) | 122 (57.5) | |||
| COVID-19 Training | Yes | 62 (32.5) | 129 (67.5) | < 0.001 | |
| No | 111 (56.1) | 87 (43.9) | |||
| PPE use Training | Yes | 57 (31.3) | 125 (68.7) | < 0.001 | |
| No | 116 (56) | 91 (44) | |||
| Availability of PPE Equipment | Yes | 144 (41.6) | 202 (58.4) | 0.001 | |
| No | 29 (67.4) | 14 (32.6) | |||
| Direct contact (<1.5 m) | Yes | 109 (50) | 109 (50) | 0.013 | |
| No | 64 (37.4) | 107 (62.6) | |||
| Occupation | Doctors | 42 (42.9) | 56 (57.1) | 0.962 | |
| Nurses | 39 (49.4) | 40 (50.6) | |||
| Pharmacist | 50 (43.9) | 64 (56.1) | |||
| Receptionist | 14 (43.8) | 18 (56.3) | |||
| Lab Technician | 13 (41.9) | 18 (58.1) | |||
| Maintenance | 15 (42.9) | 20 (57.1) | |||
| Region | Jerusalem | 38 (54.3) | 32 (45.7) | 0.023 | |
| Middle | 72 (42.9) | 96 (57.1) | |||
| North | 37 (38.9) | 58 (61.1) | |||
| South | 13 (34.2) | 25 (65.8) | |||
| Others | 12 (72.2) | 5 (27.8) | |||
| Place of Employment | Private Hospital | 44 (45.4) | 53 (54.6) | 0.255 | |
| Governmental Hospital | 50 (53.8) | 43 (46.2) | |||
| Outpatient Clinic | 29 (37.7) | 48 (62.3) | |||
| Pharmacy | 39 (41.1) | 56 (58.9) | |||
| Working at 2 facilities | 11 (40.7) | 16 (59.3) | |||
| PPE. | Surgical Face Mask | Yes | 100 (50.8) | 97 (49.2) | 0.011 |
| No | 73 (38) | 119 (62) | |||
| N95 Respirator | Yes | 85 (39.7) | 129 (60.3) | 0.037 | |
| No | 88 (50.3) | 87 (49.7) | |||
| Face Shield | Yes | 64 (49.2) | 66 (50.8) | 0.181 | |
| No | 109 (42.1) | 150 (57.9) | |||
3.2. COVID-19 Status and Clinical Manifestation
Among the 389 participants, 173 (44.5%) were infected with SARS-CoV-2 and 28 (16.2%) were admitted to the hospital. The prevalence of COVID-19 infection was higher among nurses than among other HCWs however no significant difference was detected (Table 2).
Participants variate in their reflection actions after being exposed to the COVID-19 virus; 65 (16.7%) of respondents revealed that they were tested immediately after exposure to the virus, 166 (42.7) started home isolation, while 111 (28.5%) did not take any action. Among those with confirmed positive test results, 80 (46.2%) started home isolation, while 9 (5.2%) were quarantined at a health facility. In addition, 51 (29.5%) patients were followed up by the health department or healthcare provider during their isolation.
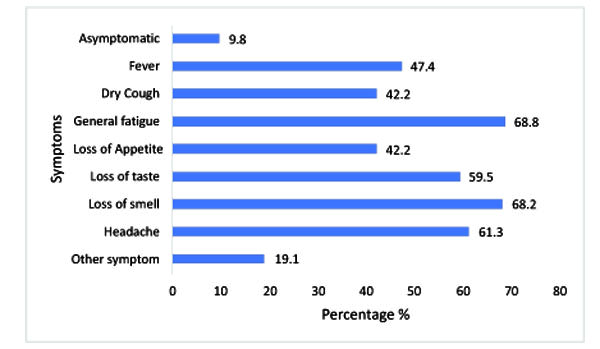
With regard to the symptoms (Fig. 3), 9.8% of the infected workers were asymptomatic. The most common symptoms were loss of smell and general fatigue in approximately 70% of infected patients, followed by headache and loss of taste. Furthermore, half of the patients (47.4%) reported a fever.
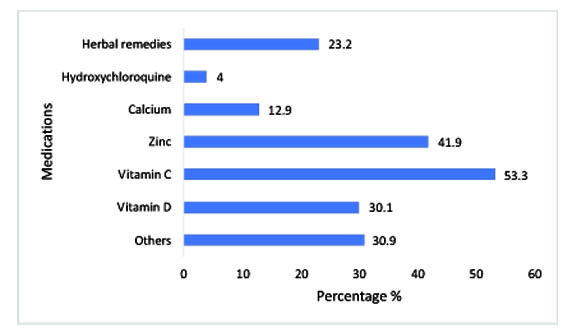
Vitamin C and zinc were the most widely used complementary supplements (53.3% and 41.9%, respectively), and 23.2% tried herbal medicines (Fig. 4).
| Characteristic | Category | n (%) | Symptomatic for >7 days | Symptomatic for ≤7 days | Asymptomatic | P-value | |
|---|---|---|---|---|---|---|---|
| Gender | Male | 90 (52) | 33 (36.7) | 46 (51.1) | 11 (12.2) | 0.011 | |
| Female | 83 (48) | 45 (54.2) | 36 (43.4) | 2 (2.4) | |||
| Age | 18-24 | 44 (25.4) | 19 (43.2) | 22 (50) | 3 (6.8) | 0.891 | |
| 25-34 | 59 (34.1) | 24 (40.7) | 31 (52.5) | 4 (6.8) | |||
| 35-44 | 38 (22) | 18 (47.4) | 16 (42.1) | 4 (10.5) | |||
| >44 | 32 (18.5) | 17 (53.1) | 13 (40.6) | 2 (6.3) | |||
| Comorbidities | Non | 149 (86.1) | 12 (50) | 9 (37.5) | 3 (12.5) | 0.41 | |
| Cardiovascular | 10 (5.8) | 66 (44.3) | 73 (49) | 10 (6.7) | |||
| Chronic lung disease | 4 (2.3) | ||||||
| Diabetes | 8 (4.6) | ||||||
| Immunocompromised | 3 (1.7) | ||||||
| Others* | 16 (9.2) | ||||||
| Smoking status |
Smoker | 54 (31.2) | 21 (38.9) | 26 (48.1) | 7 (13) | 0.165 | |
| Non- smoker | 119 (68.8) | 57 (47.9) | 56 (47.1) | 6 (5) | |||
| Medication | Multivitamins | Yes | 148 (85.5) | 71 (48) | 70 (47.3) | 7 (4.7) | 0.005 |
| No | 25 (14.5) | 7 (28) | 12 (48) | 6 (24) | |||
| Herbal medicine | Yes | 62 (35.8) | 34 (54.8) | 24 (38.7) | 4 (6.5) | 0.166 | |
| No | 111 (64.2) | 44 (39.6) | 58 (52.3) | 9 (8.1) | |||
Others: Acetaminophen, dexamdexamethasone, azithromycin, Levofloxacine, and Aspirin.
Among the infected HCWs, 90 (52%) were male, 119 (68.8%) were non-smokers, and 133 (76.9%) were not diagnosed with any chronic disease (Table 3). Although a significant association was found between being female and the appearance of symptoms (P- value= 0.011), females (54.2%) were significantly more likely to complain from symptoms for an extended period (more than 7 days) compared to males (36.7%). A significant association was observed between vitamin intake (Ca, Zn, and Vit. C, Vit. D) and experiencing COVID- 19 symptoms for an extended period (P= 0.005). Patients who took vitamins (48%) at least once were significantly more likely to be symptomatic for a more extended period than those who were not on vitamins (28%). There were no significant associations between the administration of herbs, being a smoker, or suffering from any comorbid disease on the appearance of the symptoms or their persistence for an extended period (over 7 days). Furthermore, when respondents were asked to evaluate the effectiveness of the recommended treatment plan, 99 (57.2%) affirmed its effectiveness, 50 (28.9%) were unsure about its treatment effect, and others denied the statement of effectiveness.
4. DISCUSSION
The study included 389 participants exposed to SARS-CoV-2, and 44.5% reported confirmed COVID-19 cases while working during the pandemic. The study participants worked in different healthcare settings, including the public and private sectors, pharmacies, medical offices, and other healthcare facilities. This study explored the risk factors associated with HCW exposure to SARS-CoV-2 infection and aimed to understand their characteristics, actions, symptom severities, associated comorbidities, and treatment used during infection.
4.1. COVID- 19 Risk Factors and Protective Actions
Appropriate COVID-19 training, proper use of PPE, availability, and type of PPE are essential to decrease the risk of (SARS-CoV-2) infection and control virus spread among HCWs. The data analysis revealed a significant association between COVID-19 training, PPE training, and COVID-19 infection (p = 0.001) (Table 2). A WHO study supports this finding: risk reduction of respiratory disease infection among HCWs who have adequate training and correct use of PPE [3]. In a study in China, 420 healthcare providers were trained on the proper use of PPE and reallocated to work directly with critically ill covid-19 patients. None of the practitioners reported covid-19 symptoms, and all tested negative for SARS-Cov-2 antibodies [11].
Furthermore, the availability of PPE and training on appropriate use are the responsibility of healthcare institutions and governments during such pandemics; unfortunately, Palestine lacks resources to compact this pandemic and primarily relies on donations from other countries. Data analysis showed differences in protection rates among the different masks, with N95 providing the highest level of protection. This finding supports the National Center for Immunization and Respiratory Diseases (NCIRD, 2021), the Division of Viral Diseases, recommending that HCWs prioritize N95 respirators certified by the CDC's National Institute for Occupational Safety and Health (NIOSH).
Infection rates were lower among healthcare workers in outpatient clinics than those in other healthcare settings. This variance could be attributed to the risk factors associated with COVID-19 infection, such as a higher workload, encounters with more COVID-19 patients, less training, and PPE availability. In a study in Oman, hospital-acquired covid-19 infections among health workers were higher than in other settings due to contact with infected colleagues and non-adherence to social distancing and PPE [12]. Furthermore, the infection rate was higher among nurses than other healthcare workers, with an infection rate of 47, because of many factors such as the workload, more time spent with the patient, and direct contact. This finding is supported by a meta-analysis where the most affected healthcare workers were nurses, with a rate of 48% [13] (Table 2).
An alarming finding regarding healthcare workers' actions post-COVID-19 exposure is that most did not take appropriate social isolation. One-third of HCWs began isolation only after a confirmed COVID-19 positive test, and one-third did not begin isolation following exposure. This type of behavior is dangerous and unacceptable, and it can disseminate the virus among other HCWs and patients. COVID-19 training and compliance with COVID-19 protocols should be reassessed, evaluated, and enforced with continual education, workshops, and protocol updates to reflect the current status of the pandemic [14]. The CDC advises that critical infrastructure employees who have been exposed to COVID-19 may be allowed to return to work if they are asymptomatic and further steps are taken to protect them and the community, such as pre-screen, regular monitoring, contact information, mask, social distance, disinfected and clean workspaces, and no sharing. HCWs should always be aware of and follow the local health department's quarantine and contact tracing regulations and obtain adequate training, which may supersede these recommendations [15].
Another important finding was the apparent relationship and significant association between infection and contact distance with suspected or infected COVID-19 patients. Infection rates were significantly lower in cases with non-direct contact (work more than 1.5 meters away) than in those with direct contact (work less than 1.5 m) (p = 0.013). When a person is in close contact (within 1 m) with someone who has respiratory symptoms (e.g. coughing or sneezing), his or her mucosae (mouth and nose) or conjures are at risk of infection. Transmission may also occur via fomites in the immediate area of an infected person. As a result, COVID-19 can be transmitted through direct contact with infected individuals. Adherence to recommended social distancing can effectively limit disease transmission [16, 17].
According to the UK's Scientific Advisory Group for Emergencies (SAGE), the SARS-CoV-2 transmission risk at 1 m might be 2-10 times higher than that at 2 m. In addition, physical distancing steps concerning coronavirus transmission were the subject of a systematic analysis conducted by the WHO. Physical distancing of 1 m resulted in a 12.8 percent transmission risk compared to 2.6 percent at distances less than 1 m, indicating that physical distancing rules of 1 m or more are recommended [18, 19].
Based on the study training of HCWs on appropriate PPE, establishing COVID-19 safety protocols and policies is essential to maintain healthcare workers' well-being and prevent the virus's spread. Policies must be adopted to provide training and to increase the level of protection for HCWs. Emphasis on compliance with procedures upon exposure or confirmed infection from immediate examination to quarantine for the recommended period is essential to limit the spread of the disease. Furthermore, not deducting wages for quarantine days increases adherence to policies and procedures. WHO recommended suitable training for different healthcare workers (including the supervisors) and adequate resources (human, material, and financial), owing to the urgency during the COVID-19 pandemic [20].
4.2. COVID-19 Status and Clinical Manifestation
Besides looking at risk factors associated with the development of COVID-19 infection, we analyzed the characteristic of COVID-19-infected HCWs based on symptoms, comorbidities, and treatment. 173 out of 389 exposed HCWs reported a confirmed COVID-19 infection. Among the HCWs, 90.2% reported symptoms of COVID-19, including weakness, muscle pain, headache, loss of taste, loss of smell, dry cough, and fever. In a case-control study of COVID-19 symptom severity and duration in six countries, Kim et al. [21] reported similar findings. Another observational study in a large Belgian tertiary care centre showed that participants had cough, headache, myalgia, loss of smell or taste, and fever as the main symptoms [22]. This study reported fatigue, weakness, and muscle pain in 70% of the infected HCWs. Many studies have reported fatigue and weakness among HCWs while combating the pandemic [23].
Approximately 48% of infected HCWs were females and experienced a significantly longer duration of symptoms than males, with a (P value of 0.013). Females are more likely to suffer from healthcare problems and complications post covid-19 [24]. Approximately 14% of the infected participants have comorbidities, including cardiovascular disease, chronic lung disease, diabetes, and compromised immune systems. No significant association was found between comorbidities and the duration of COVID-19 symptoms. However, this finding could not be extrapolated because of the small number of participants with comorbidities in this subgroup. No association was found between smoking or other comorbidities and the incidence or duration of the symptoms. Even though some studies have noted that persons with comorbidities (lung disease, immune impression, and cardiovascular disease) are more likely to contract the virus and become severely ill and deteriorate, the available data are limited [25, 26].
Multiple vitamins and herbal remedies have been tried during the pandemic for either covid-19 treatment or prophylaxis because of the lack of definite treatment and their known effects on enhancing immunity. This study revealed a significant association between vitamin intake (Ca, Zn, and Vit. C, Vit. D) being symptomatic and experiencing longer symptom duration than patients who took these supplements (P= 0.005). Some studies have reported no significant association between vitamin C or zinc use and symptom severity and duration. According to a multicentre study published in the JAMA open network, an open-label trial included 214 patients diagnosed with SARS-CoV-2 infection who received high doses of zinc and vitamin C compared with the traditional standard of care. The study revealed that the combination product did not affect symptom severity or duration [27]. In contrast, other studies have shown that vitamins C and D are sufficient to boost immunity against COVID-19 infection and positively impact symptom duration reduction [28]. However, these contradictory results may be attributed to a deficiency of vitamins, and there are insufficient data to prove an association between covid-19 and the benefits of nutritional supplements [29].
COVID-19 ranges from mild respiratory disease to severe illness, requiring intubation and mechanical ventilation. Therefore, patients with comorbidities should take all the necessary precautions to avoid being infected with COVID-19, as they usually have the worst prognosis. This warrants appropriate precautions and safeguards measures, such as regular hand washing with soap and water, using alcohol-based hand sanitizer, limiting person-to-person contact and practicing social distancing, wearing a face mask in public places, and overall limiting going to public areas unless it is necessary [30].
4.3. Strengths and Limitations
The strengths of this study include healthcare staff from various backgrounds and work conditions, which allows for risk comparisons using a structured sample. In addition, our sample characteristics are comparable to the overall population patterns of all HCWs, which display a similar distribution by sex and age and are well represented by a wide variety of HCW roles. Therefore, this study is likely to be applicable to Palestine. However, the study was not devoid of some drawbacks. First, the analysis had a limited sample size because of the lack of cooperation among medical staff to complete the questionnaire. We were also unable to collect information from HCWs who died of COVID-19 or were too sick to respond to. Second, in healthcare settings, using a composite outcome to diagnose suspected or confirmed COVID-19 infection was ineffective in the early stages of the pandemic; monitoring for healthcare staff was often minimal; however, this practice changed significantly as the pandemic progressed. Hence, clinical diagnosis is often relied on. Third, other limitations, distances were calculated according to the participant's beliefs (subjective, 1.5 m was considered near in one participant but distant in another, for example), but they were all combined in the final review. Finally, all the data presented here are subjective and reflect hypothesis-generating associations among the participants. Therefore, further research is warranted.
CONCLUSION
As information about COVID-19 continues to evolve, and with the availability of the COVID-19 vaccine, adherence to WHO standards and regulations on safety policies and practices within healthcare institutions will help keep the virus curve down and decrease infection risk. In this study, half of the participants were not trained on appropriate PPE training; furthermore, most participants exposed to the SARS-Cov-2 virus did not take appropriate actions of either testing or isolation. Social isolation and availability of personal protective equipment (PPE) are essential factors that negatively correlate with virus transmission and spread.
The healthcare system must ensure a safe work environment and practice for healthcare workers by providing appropriate resources and proper training to combat the epidemic. Therefore, policymakers must ensure that all HCWs have a controlled environment to enhance the healthcare workforce safety and decrease the risk of COVID-19 infection.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Ethical Committee of Birzeit University approved the study at the Faculty of Pharmacy, Nursing, and Health Professions, Birzeit University (reference number BZUPNH2004).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans were used in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants in this study.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial, or otherwise.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIALS
Supplementary material is available on the Publisher’s website.

