All published articles of this journal are available on ScienceDirect.

Prevalence and Management of Low Back Pain Among Health Workers in a Privately Owned Teaching Hospital in Nigeria
Authors Info & Affiliations
Abstract
Aim:
This study assessed the prevalence and management of LBP among health workers in a private teaching hospital in South West Nigeria.
Background:
Healthcare workers (HCWs) often experience low back pain (LBP) more than any other category of workers. While a lot has been documented about the prevalence of LBP among different categories of workers, little is known about how health workers manage LBP.
Objectives:
This study aimed to assess the prevalence and management of LBP among health workers in a private teaching hospital in South West Nigeria. Associations between variables: (a) sociodemographic variables (i.e., age, gender) and the prevalence of low back pain, and (b) interference with activities of daily living across different categories of health workers, were evaluated.
Methods:
A cross-sectional design was employed in this study. One hundred and eighty-nine HCWs were randomly selected from the wards and units of the hospital. The LBP questionnaire and the Nordic Musculoskeletal questionnaire were used for data collection. Data were analysed using descriptive (mean and percentages) and inferential (chi-square and ANOVA) statistics.
Results:
The prevalence of LBP among health workers was found to be 87.3%. Moreover, most of the health workers massage their back (78.3%), engage in exercise (72.0%), and use analgesics (69.3%) as a means of managing LBP. Furthermore, there was no significant relationship between gender (X2 = 0.31, P>0.05), age (X2 = 1.52, P>0.05), marital status (X2 = 2.93, P>0.05) of HCWs and prevalence of LBP. However, a significant difference was reported in the mean interference of LBP with activities of daily living across the different categories of healthcare workers that participated in the study (F= (7,181) 3.58, P = 0.01).
Conclusion:
The prevalence of LBP is high among HCWs that participated in the study. Therefore, it is recommended that HCWs might use massage, engage in exercise, and take analgesics as a means to combat LBP.
1. BACKGROUND
Globally, low back pain (LBP) is one of the leading musculoskeletal disorders [1]. It affects both young and old [2, 3]. A prevalence rate of 48% has also been reported among the adult population in the southern part of Nigeria [3]. In developed countries, scholars documented a prevalence rate between 1.4 to 20.0% [4]. Odebiyi and colleagues [5] reported a high prevalence of LBP (61.6%) among the obese population in Lagos, Nigeria [5]. However, different rates of LBP prevalence were reported among various categories of workers. Twenty-five percent (25%) prevalence of LBP was reported among manual materials handling workers [6], 48.3% among sawmill workers [7, 8], 53.5% among university lecturers [9], and 58.1% among hotel housekeepers [10].
Healthcare workers (HCWs) often experience LBP more than any other category of workers [11]. The prevalence rate ranges from 53% among the general healthcare workforce to 87% among health workers in the operating room [12-15]. Among different categories of healthcare workers, Walid and Hoque reported a 60.3% prevalence rate of LBP among doctors in the tertiary level of hospitals in Sylhet [16]. Among Iranian nurses, Mohammadi and colleagues [17] documented a prevalence rate of 68.4% [17], while a prevalence rate of 73.5% was documented among nurses in secondary and tertiary levels of hospitals in Bahrain [18]. Prevalence rates ranging between 38.1% and 63.8% of LBP were reported among nurses in Ethiopia [19, 20]. In South Africa, a prevalence rate of 59% was reported among nurses in a regional hospital in KwaZulu-Natal [21].
A previous study on nurses in Africa has shown that the prevalence of low back pain is at its highest in Nigeria [22]. In a study on nurses at a teaching hospital in Nigeria, Idowu et al. [23] reported a 71.4% prevalence rate of LBP [23]. Furthermore, female gender [2, 4, 3, 24], advanced age [5, 9], high body mass index [2, 12], lack of regular exercise, being married, long-standing while working, long years of service, and low job satisfaction had been found to increase risk of LBP among HCWs [14].
Low back pain has been found to result in negative health and socio-professional consequences among HCWs [15]. It has been documented to result in an increased rate of work absenteeism, movement restriction, and therapist consultation among HCWs [18]. A high workload has been found to increase the risk of LBP among workers [25, 26]. Moreover, a previous study documented that the risk of LBP is due to a higher workload resulting from client care among health workers in private hospitals compared to those in public hospitals [27]. It is worth noting that private teaching hospital is a new phenomenon in Nigeria that accompanies medical education approval for some private universities. While a lot has been documented about the prevalence of LBP among different categories of workers, little is known about HCWs in privately owned teaching hospitals and how these HCWs manage LBP. Previous studies in Nigeria concentrated majorly on nurses in the public sector with little attention to those working in the private sector. This has caused a paradigm shift regarding policy made on LBP to be concentrated on public health institutions HCWs leaving behind those in the private sector. Due to the aforementioned, the study, therefore, aimed to assess the prevalence and management of LBP among health workers in a private teaching hospital in South West Nigeria.
1.1. Objectives
The specific objectives of the study are to:
- Assess the prevalence of low back pain among health workers in a privately owned teaching hospital in Nigeria
- Investigate the prevalence of low back pain interference with the activity of daily living among health workers in a privately owned teaching hospital in Nigeria, and
- Identify the strategies adopted in the management of low back pain among health workers in a privately owned teaching hospital in Nigeria.
2. METHODS
2.1. Participants and Setting
A cross-sectional research design was employed in this study. The study was conducted among healthcare workers in a privately owned teaching hospital in the Southwestern Region of Nigeria. The teaching hospital is one of the foremost private teaching hospitals in Nigeria. The medical centre that transformed into the teaching hospital has a history of existence for over a hundred years. A total of one hundred and ninety-seven (197) healthcare workers were recruited from the wards and units of the hospital using a simple random sampling technique. However, only one hundred and eighty-nine (189) healthcare workers eventually participated in the study. Nurses, doctors, pharmacists, laboratory scientists, technicians, physiotherapists, ward aids, and cleaners working in the hospital participated in the study.
2.2. Inclusion/Exclusion Criteria
All the categories of HCWs, namely nurses, doctors, pharmacists, laboratory scientists, technicians, physiothe-rapists, ward aids, and cleaners in the hospital, were included in the study. While those on any form of leave (maternity, study, and annual leave) were exempted from the study.
2.3. Data Sources/Measurements
The LBP questionnaire [15] and the Nordic Muscu-loskeletal Questionnaire [28] were used in this study. The former has 16 items and two sections in total. The first section consists of six (6) items, asking questions about the socio-demographic characteristics of the participants. The socio-demographic data collected were gender, age, marital status, level of education, and professional years of service. The second section consists of 10 items, eliciting information about the prevalence of LBP.
The Nordic Musculoskeletal Questionnaire is a 29-item scale divided into two (2) sections. The first section has a 24-item all-answerable to “Yes or No” type of scale, assessing the interference of LBP with participants’ activities of daily living and work. The last section consists of 5 items scale, assessing strategies adopted in the management of LBP among participants. The LBP questionnaire [15] and the Nordic Musculoskeletal Questionnaire have been widely used in the assessment of prevalence, interference, and strategies adopted in the management of LBP among participants with good reliability and validity [28]. The internal consistency coefficient of this scale was tested, and the Cronbach alpha was reported to be 0.76.
2.4. Bias
In addressing the potential bias of the instrument, before the commencement of actual data collection, the questionnaire was pre-tested in 19 (10%) study subjects in another private teaching hospital, and necessary modifications were made to the instrument. Six bachelor of nursing science graduates with a research assistant were assigned for data collection. Furthermore, the self-administration technique was used for data collection. One of the authors and a research assistant (a registered nurse) were involved in data collection. A questionnaire was administered to prospective participants and retrieved the next day. Institutional permission and ethical approval (BUTH/REC/0002) were obtained from the appropriate research and ethical board for the study. Written informed consent was obtained from all healthcare workers that eventually participated in the study. Participation was made optional, and participants were duly informed that they could withdraw from the study at any time.
2.5. Sample Size Determination
The sample size was determined using Cochran’s formula (n=z2 p (1-p)/e2) (Singh & Masuku, 2014). The prevalence rates of low back pain were between 53% to 87% among healthcare workers (Alnaami, et al., 2019; Mukhtad & Mohamed, 2018; Şimşek, et al., 2017; and Wong, et al., 2010). Using p = 70%, z=1.96, and e=0.05, the sample size was calculated as n= 323. The n was corrected using Taro Yamane's formula, n= N/ [1+N (e)2], where, n = sample size; N = population size - 323; e = sampling error – 0.05. Therefore, n = 179, with no response rate of 10%, n = 197 healthcare workers.
2.6. Data Collection
Self-administration technique was used for data collection. This was done face-to-face. One of the authors and a research assistant (a registered nurse) were involved in data collection. A questionnaire was administered to prospective participants in their offices and retrieved the next day. Informed consent was obtained from all healthcare workers that eventually participated in the study. Confidentiality of information was addressed by asking them not to put identifiers. Participation was optional, and participants were duly informed of their right to withdraw from the study. Recruitment of participants for the study started in October, 2019, and the process of data collection ended in February, 2020.
2.7. Data Analysis
Data were checked for completeness. The cleaned and missing data were re-entered by cross-checking from the hard-copy questionnaires. The part of the scale assessing interference with the activity of daily living was recorded as “1” for “Yes” and ‘0” for “No”. The total mark obtainable was found to be 24 and the least “0”. The score was converted to a “0” to “10” scale to correspond with the visual analog pain scale. A score of “0” was regarded as no interference with activities of daily living, a score of “1” to “3” mild interference with activities of daily living, “4” to “6” moderate interference with the activity of daily living, and “7” to “10” severe interference with the activity of daily living. Descriptive (mean and percentages) and inferential (chi-square and ANOVA) statistics were used for data analysis. The level of significance was set at P <0.05. SPSS version 23 was used for all the analyses.
3. RESULTS
3.1. Characteristics of Participants
A total of 197 questionnaires were administered, and 189 were returned (95.9%). Most healthcare workers that participated in the study were female (72.9%), with one out of every four participants between the ages of 20 and 30 years (Table 1). Only 8 (4.3%) of the participants were above 50 years of age. Most of the participants were married (63.3%), and the majority completed a tertiary level of education (81.4%). Nurses (36.7%) and doctors (22.3%) accounted for more than half of the participants in this study. Also, results, as presented in the Table, revealed that 61.2% of the healthcare workers in this study were within their first 10 years of practice.
Table 1.
| - | - | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Female Male |
137 52 |
72.9 27.1 |
| Age | 20-30 31-40 41-50 51-60 |
77 65 39 8 |
41.0 33.6 20.6 4.3 |
| Marital Status | Single Married Divorced |
66 119 4 |
35.1 63.3 1.6 |
| Level of Education | No formal education Primary school completed Secondary school completed Tertiary school completed |
3 14 19 153 |
1.1 7.4 10.1 81.4 |
| Profession | Doctor Nurses Pharmacist Orderly Laboratory scientist Works Cleaners Physiotherapy |
43 69 6 20 15 15 20 1 |
22.3 36.7 3.2 10.6 8.0 8.0 10.6 0.6 |
| Years of Service | 1-10 11-20 21-30 31-40 41-50 |
115 58 10 3 3 |
61.2 30.9 5.3 1.6 1.1 |
3.2. Prevalence of Low Back Pain among Participants
The findings of this study (Table 2) revealed the lifetime, 12-month, and 7-day prevalence rates of LBP among the healthcare workers in the study to be 87.3%, 84.7%, and 54.5%, respectively. However, only 9.0% and 11.1% had been hospitalized or changed jobs/duties because of LBP, respectively. Furthermore, 54.5% said LBP had reduced their work activities in the last 12 months, while 29.6% said LBP had resulted in their reduced leisure time. More than half (51.3%) of the healthcare workers said LBP had caused between one to seven days of work absenteeism and 21.2% said they had been absent from work for eight to thirty days in the last year.
3.3. Prevalence of Low Back Pain Interference with Activities of Daily Living among Participants
Interference of LBP with activities of daily living among participants showed that 68.1% constantly changed positions to promote comfort because of LBP (Table 3). Forty-three (43%) opined that LBP makes them walk slowly; 15.4% said they could only walk a short distance because of LBP, while 35.6% mentioned they lie down very often because of LBP. Results further showed that 17.0% found it difficult to get out of the chair because of LBP, while 30.3% usually held something to get stand up. Fifty-four (28.7%) of participants in this study believed that LBP usually prevents them from doing their normal house chores, while 25.0% mentioned that they had to depend on people to do things for them because of their back pains.
Findings from this study further showed that LBP had prevented more than half (53.1%) of the health workers from performing their activities of daily living in the last month. About one-tenth (8.5%) had been hospitalised before because of LBP.
| Variables | Characteristics | Frequency | Percentage (%) |
|---|---|---|---|
| Have you ever had LBP? | Yes No |
165 24 |
87.3 12.7 |
| Have you had LBP in the last 12 months? | Yes No |
160 29 |
84.7 15.3 |
| Have you been hospitalized because of LBP in the last 12 months? | Yes No |
17 172 |
9.0 91.0 |
| Have you changed your job or duty before because of LBP in the last 12 months? | Yes No |
21 168 |
11.1 88.9 |
| LBP caused me to reduce my work activity in the last 12 months | Yes No |
103 86 |
54.5 45.5 |
| LBP has caused me to reduce my leisure time in the last 12 months | Yes No |
56 133 |
29.6 70.4 |
| The total length of time that LBP prevented me from doing my normal work in the last 12 months | 0 day 1 – 7 days 8 – 30 days More than 30 days |
50 97 40 2 |
26.5 51.3 21.2 1.1 |
| Have you seen by health professional because of LBP in the last 12 months? | Yes No |
66 123 |
34.9 65.1 |
| Have you used any drugs because of LBP before? | Yes No |
115 74 |
60.8 39.2 |
| Have you had LBP in the last 7 days? | Yes No |
103 86 |
54.5 45.5 |
| Variables | Yes (%) | No (%) |
|---|---|---|
| I stay at home most of the time because of my back. | 36 (19.1%) | 153 (80.9%) |
| I change position frequently to try to get my back comfortable. | 128 (68.1%) | 61 (31.9%) |
| I walk more slowly than usual because of my back. | 82 (43.6%) | 107 (56.4%) |
| Because of my back, I am not doing any jobs that I usually do around the house. | 54 (28.7%) | 135 (71.3%) |
| Because of my back, I use a handrail to get upstairs. | 39 (20.7%) | 150 (79.3%) |
| Because of my back, I lie down to rest more often. | 67 (35.6%) | 122 (64.4%) |
| Because of my back, I have to hold on to something to get out of an easy chair. | 57 (30.3%) | 132 (69.7%) |
| Because of my back, I try to get other people to do things for me. | 37 (25.0%) | 152 (75.0%) |
| I get dressed more slowly than usual because of my back. | 32 (11.7%) | 157 (88.3%) |
| I only stand up for short periods of time because of my back. | 34 (25.5%) | 155 (74.5%) |
| Because of my back, I try not to bend or kneel down. | 57 (30.3%) | 132 (69.7%) |
| I find it difficult to get out of a chair because of my back. | 32 (17.0%) | 157 (83.0%) |
| My back is painful almost all of the time. | 39 (20.7%) | 150 (79.3%) |
| I find it difficult to turn over in bed because of my back. | 44 (22.9%) | 145 (77.1%) |
| My appetite is not very good because of my back. | 33 (17.6%) | 156 (82.4%) |
| I have trouble putting on my socks (or stockings) because of the pain in my back. | 30 (15.4%) | 159 (84.6%) |
| I can only walk short distances because of my back pain. | 29 (15.4%) | 160 (84.6%) |
| I sleep less well because of my back. | 31 (16.5%) | 158 (83.5%) |
| Because of my back pain, I get dressed with the help of someone else. | 37 (19.7%) | 152 (80.3%) |
| I sit down for most of the day because of my back. | 35 (18.6%) | 154 (81.4%) |
| I avoid heavy jobs around the house because of my back. | 58 (30.9%) | 131 (69.1%) |
| Because of back pain, I am more irritable and bad-tempered with people than usual. | 25 (15%) | 163 (85%) |
| Because of my back, I go upstairs more slowly than usual. | 35 (17.0%) | 154 (83.0%) |
| I stay in bed most of the time because of my back. | 30 (11.0%) | 159 (99.0%) |
3.4. Severity of Interference of Low Back Pain with Activities of Daily Living
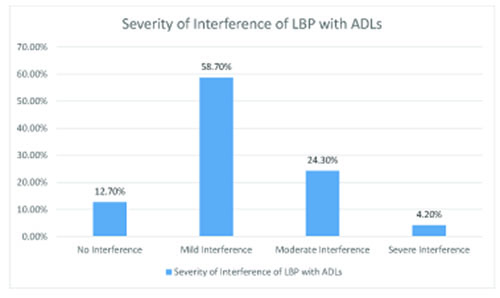
A summary of the interference of LBP with the activities of daily living of the participants showed that more than half (58.7%) of the participants had mild inferences of LBP with their activities of daily living. It was found that low back pain severely interfered with the activities of daily living of a few (4.2%) of the healthcare workers, while LBP did not interfere with the activities of daily living of 12.7% of the workers (Fig. 1).
3.5. Strategies Adopted in the Management of Low Back Pain
Healthcare workers in this study adopted several strategies to manage LBP. Findings showed that the healthcare workers in this study adopted both pharmacological and non-pharmacological strategies to manage LBP. Results, as presented in Table 4, showed that 69.3% of healthcare workers use analgesics to relieve LBP. Interestingly the most used strategy was found to be the non-pharmacological. The majority (78.3%) of participants mentioned that they usually massage the back to relieve pain, while those that engage in exercise to manage LBP experiences were found to be 72%.
Table 4.
| Management of Low Back Pain |
Yes (%) |
No (%) |
|---|---|---|
| Do you use any form of analgesic to relieve pain? | 131 (69.3%) | 58 (30.7%) |
| Do you engage in any form of exercise? | 136 (72.0%) | 53 (28.0%) |
| Do you massage the affected part? | 148 (78.3%) | 41 (21.7%) |
| Do you still work effectively even with the pain? | 131 (69.3%) | 58 (30.7%) |
| Do you usually rest while on duty due to the pain? | 66 (34.9%) | 123 (65.1%) |
3.6. Univariate Analysis of Sociodemographic Charac-teristics and Prevalence of Low Back Pain
No significant relationship was found between gender (X2 = 0.31, P>0.05), age (X2 = 1.52, P>0.05), marital status (X2 = 2.93, P>0.05) of HCWs, and prevalence of LBP among the healthcare workers in this study (Table 5).
Table 5.
| - | Prevalence of LBP | |
|---|---|---|
| X2 | P | |
| Gender | 0.31 | 0.58 |
| Age | 1.52 | 0.64 |
| Marital status | 2.93 | 0.23 |
3.7. Univariate Analysis of Interference of LBP with ADLW across the Different Categories of Healthcare Workers
A significant difference was found in the mean interference of LBP with activities of daily living across the different categories of healthcare workers that participated in the study [F= (7,181) 3.58, P = 0.01] (Table 6).
Table 6.
| ANOVA | |||||
|---|---|---|---|---|---|
| Pain Interference | |||||
| Sum of Squares | Df | Mean Square | F | Sig. | |
| Between Groups | 11.543 | 7 | 1.649 | 3.58 | .001 |
| Within Groups | 82.817 | 181 | .458 | ||
| Total | 94.360 | 188 | |||
4. DISCUSSION
The present study focused on the prevalence and management of low back pain among health workers. The study reported that most of the healthcare workers that participated in the study were female (72.9%), one out of every four participants was within the age range of 20 and 30 years, and 61.2% of the healthcare workers in the study were within their first ten years of practice. This is similar to the study carried out in Sokoto, Nigeria, among healthcare workers in tertiary health institutions, where the females were predominant (60.6%) [29]. This was also the case in a study carried out among healthcare workers in south-south Nigeria, where the male-to-female ratio was 2:3 [30]. The findings of a study by Abebe et al. [31] were at variance with ours, where the majority (52.1%) of the respondents were males. The current study offers some evidence that it seems females are now dominating most professions, especially in southwestern Nigeria, and nurses seem to be considered the backbone of the healthcare system.
4.1. Prevalence of Low Back Pain Among Participants
The findings of this study revealed the 12-month and 7-day prevalence rates of LBP among healthcare workers to be 87.3%, 84.7%, and 54.5%, respectively. Our finding was similar to the study carried out among healthcare workers in southwestern Saudi Arabia, where the overall prevalence of low back pain in 12 months was 73.9% [12]. It should be noted that prevalence data can differ from country to country. Shieh et al. [26] conducted a study among nurses in Taiwan, and a prevalence of 72% was found. In Turkey, LBP was found to be 53% among healthcare workers [14]. It was also established in a study in North-west Nigeria that low back pain among healthcare workers was 29% [32]. In Sokoto, Nigeria, the prevalence of low back pain among healthcare workers was 56.2%, 39.1%, and 17.2%, respectively [29]. These empirical data give insight into the global and local magnitude of low back pain among healthcare workers, which is of great concern. Furthermore, it has been reported in this study that HWCs had been hospitalised or changed jobs/duties because of LBP. In addition, respondents with LBP reduced their work activities in the last 12 months, and LBP has reduced the leisure time of the HCWs. More than half of the participants affirmed that LBP has caused between one to seven days of work absenteeism. Moreover, some took leave from work for eight to thirty days in the last year. Our findings were in agreement with that of Kotowski [33], where it was reported that HCWs take the least time off from work or lost time due to LBP. However, Abolfotouh et al. [34] conducted a study on nurses in Doha, Qatar, and reported individuals seeking medical care for LBP, possibly progressing to taking time off work for LBP, which culminated over time. Likewise, 13% of HWCs in Riyadh, Saudi Arabia, who had back pain took days off from work [35]. The increase in the prevalence of low back pain among the study participants could be that the nature of the work of each HWC contributed greatly to LBP. For instance, the doctors and physiotherapists sitting hours for consultation are long, while nurses work long hours without an adequate break during each shift.
4.2. Prevalence of Low Back Pain Interference with Activities of Daily Living Among Participants
The current study reported that for participants suffering from LBP, their activities of daily living are interfered with, and they constantly change positions to promote comfort. Healthcare workers also reported that LBP makes them walk slowly and short distances; some participants mentioned they lie down very often because of LBP. Results further showed that participants find it difficult to get out of the chair, while they usually hold something to stand up. Participants also reported that LBP usually prevents them from doing their normal house chores, and they have to depend on people to do things for them because of their back pains. Our study aligns with that of Mekonnen [19], stating that the majority of HCWs in Western Ethiopia had limited activity due to low back disorder. Low back pain interfering with activities of daily living and constant change in the positions to promote comfort among HCWs could be a result of the severity of the pain they experience daily.
4.3. Summary of the Interference of Low Back Pain with Activity of Daily Living
A summary of the interference of LBP with the activity of daily living showed that more than half of the participants had mild inference of LBP with their activities of daily living. This aligns with a study conducted by Yiengprugsawan [36], where difficulties in getting dressed, walking, climbing stairs, and bending/kneeling were reported to interfere with activities of daily living [36]. Moreover, 72.2% of HCWs in Western Ethiopia had limited activity due to low back disorder [19]. One can be concluded from the findings of this study that LBP is the most prevalent musculoskeletal condition, and this causes pain or discomfort. This leads to activity limitation that results in a significant loss in productivity at work.
4.4. Strategies Adopted in the Management of Low Back Pain
Findings showed that the healthcare workers in this study adopted both pharmacological and non-pharmacological strategies to manage LBP. Interestingly, the most used strategy was found to be non-pharmacological, which includes massaging the back for relief and engagement in exercises. Studies have also shown that HCWs' coping strategies for LBP included praying, hopping, and increased behavioural activity [37, 38]. At variance with our study is that of Ayanniyi et al. [39], where it was reported that the most common intervention in the management of back pain among adolescents in Nigeria is the use of pharmacologic agents through self-medication [39]. The decision by HWCs in the present study to use non-pharmacological agents probably was that they weighed the long-term effect of the damage that pharmacology agents could cause systemically. Consequentially, there was no significant relationship between the gender, age, and marital status of HCWs and the prevalence of LBP among the healthcare workers in this study. This is similar to the study carried out in Nigeria, where it was reported that gender had no association with back pain [39]. At variance with our study, older age and female sex were found to be significantly associated with LBP among HCWs in Sokoto, Nigeria [2, 12]. Furthermore, a significant difference was reported in the mean interference of LBP with activities of daily living across the different categories of healthcare workers that participated in the study. Similar to the findings in this study, previous studies have shown that the LBP was significantly more prevalent among HCWs and interfered with activities of daily living of cleaners/ward attendants, medical doctors, nurses, and other categories of HCWs in Sokoto, Nigeria, and Iran [29, 11]. It could be inferred from our study that perhaps the nature of the job of these categories of HCWs, such as long hours at work, carrying patients, bending to work, and performing repetitive tasks, might have accounted for this finding.
4.5. Study Limitations
Study limitations are mostly related to the fact that this study is a cross-sectional descriptive study. Moreover, there is an inability to generalise findings to men and HWCs over the age of 50 years. The management of low back pain instrument lists only five (5) strategies to manage low back pain in this study. However, many other strategies were not included that an open-ended question would have captured. Also, evaluating the correlation between the management of low back pain and other study variables is recommended for future studies. However, this study still provides empirical findings from a privately owned teaching hospital in a developing country, like Nigeria.
4.6. Study Implications (Research, Education, and Policy)
By leveraging on non-pharmacological management of LBP data, the health industry can transform how to conduct clinical research and provide maximum benefit to healthcare workers with LBP in the future. Incorporating non-pharmacological management in the health care system among HCWs in practice will stimulate critical thinking for educators, underscoring the importance of teaching students about non-pharmacological skills they need to support and prevent LBP while in practice. Adoption of non-pharmacological management of LBP among HCWs should be a critical decision; therefore, policymakers need to ensure its implementation in the healthcare sector. This is because it prevents the side effect of prolonged use of pharmacological agents.
CONCLUSION
Low back pain is prevalent among healthcare workers in Nigeria. This study assessed the prevalence of low back pain among healthcare workers, the interference of LBP with activities of daily living, and how healthcare workers manage their experience of LBP. The study concluded that the prevalence of LBP among healthcare workers in this study was high and interfered with their activities of daily living. Non-pharmacological pain management strategies were reported to be the most used to manage pain among the participants. Efforts should, therefore, be directed at reducing LBP among healthcare workers and promoting the use of non-pharmacological means of managing pain.
LIST OF ABBREVIATIONS
| HCWs | = Healthcare Workers |
| LBP | = Low Back Pain |
AUTHORS' CONTRIBUTION
All authors have equally contributed to collecting the data, analysing the data, reviewing the literature, writing the first draft, and revising and approving the final draft.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Institutional permission and ethical approval were obtained from the ethical board of BOWEN Teaching Hospital; approval number (BUTH/REC/0002).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were by the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
All data are available upon request from the corresponding author [I.O.O].
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the participants and management of the institution where the study was conducted.

