All published articles of this journal are available on ScienceDirect.

Growth Monitoring and Promotion and Index Development for Improved Child Health: A Scoping Review Using Rodgers Concept Analysis Framework
Abstract
Purpose:
The purpose of this scoping literature review is to explore the breadth of the available literature, and identify knowledge gaps to inform future research through the use of Rodgers evolutionary concept analysis framework. The literature review also seeks to describe the key child indices developed and their characteristics so as to guide the development of a GMP index for improved child health in Zimbabwe.
Methods:
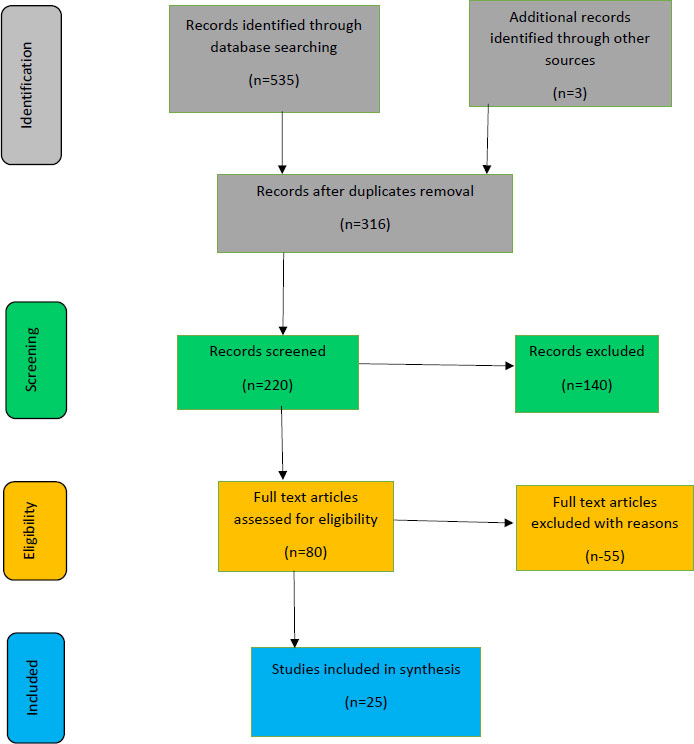
The keywords growth monitoring and promotion, community health workers, caregivers of children under five years, child health indices, and index development were used to search for relevant literature from Science Direct, Google Scholar, EBSCO, and PUBMED databases in English. The initial electronic database search yielded 535 research articles, and 316 were further assessed for their relevance to the study. An additional 140 articles were excluded from the search as they did not contain adequate evidence as per the Rodgers Evolutionary Framework. After the full-text review, 80 articles out of 220 articles met the inclusion criteria. Those found to be suitable were 25 articles and were thus included in the final analysis.
Results:
Key Antecedents: distance and socio-cultural constraints, CHW activeness, participation of fathers in GMP activities, poor understanding and interpretation of growth charts, poor communication between caregivers and CHWs, full vaccination status and complacency; Attributes: education status of parents, knowledge, attitude, and practices of caregivers and Consequences: timely health interventions, improved child health outcomes, a platform to promote optimal child health practices of GMP activities were identified.
Conclusion:
More research needs to be explored to form indices that incorporate behaviour change metrics. This will lead to an increased evidence base to guide the health system, funders, and policy makers conclusively.
1. INTRODUCTION
Globally, nearly 229 million children under three years were malnourished in 2019. Of these, more than one-quarter of all wasted children lived in Africa [1]. The last National Nutrition survey of 2018 showed that 26.2% of children under five years in Zimbabwe were stunted. Given these statistics, it is increasingly important to monitor the growth of children to improve child nutrition and detect early any serious underlying conditions [2]. According to the World Health Organisation [3], growth monitoring and promotion (GMP) is a composite of (1) the routine measurement of a child’s weight and height/length; (2) the plotting of the child’s measurements and comparison of the child’s status to a standardized growth chart to assess growth adequacy; (3) growth-informed counselling; and, if necessary, (4) the undertaking of remedial, health-promoting action.
Implemented properly, GMP programmes have brought linkages to key preventive and curative health services, led to increased knowledge by the family of appropriate infant and young child feeding practices while also providing a platform for the early diagnosis and treatment of undernutrition by community health workers (CHWs) [4]. Growth monitoring can provide an entry point to preventive and curative health and has also been considered an integral part of programmes associated with significant reductions in malnutrition and mortality among children under five years [5].
Where community GMP programmes currently exist, and there is potential for improvement, it is important to maximise their potential [6]. Some of the gaps that have been identified in the literature have been a lack of essential supplies and an unsupportive health system that demotivated CHWs thereby leading to unsatisfactory growth-monitoring practices [5]. A Zimbabwean study [6] revealed that half of the CHWs had one scale each, implying that those with no scales possibly did not weigh any children monthly, while only 62% of CHWs had Mid-Upper Arm Circumference measuring tapes (MUAC measuring tapes). This highlighted some of the many challenges faced by GMP programmes in communities.
There is, however, a dearth of research in Zimbabwe with regards to GMP activities against a background that the National Nutrition Survey of 2018 acknowledged that the provision of child health services such as growth monitoring was low and there was a need to strengthen community-based programme delivery for communities through improved GMP by CHWs. The CHWs are the link between the health facility and the community and are thus an important element of the health system. It was against this background that this scoping literature review was carried out.
2. PURPOSE
The purpose of this scoping literature review was to explore the breadth of the available literature, identify knowledge gaps to inform future research, and describe the key characteristics related to GMP Index development. In this study, the breadth of available literature on GMP activities was explored along with any GMP indexes that have been developed and their contribution towards child health.
3. METHODOLOGY
The following steps were used in this scoping literature review.
3.1. Step 1. Defining the Research Questions
In developing the research questions, it was important to take into account the purpose and scope of the review along with the overall study objective of GMP index development [7, 8]. Against this background, the research questions that were defined through discussions with the study supervisors were:
(1) What are the gaps for further research on GMP activities?
(2) What indexes have been developed towards improving child health through GMP?
3.2. Step 2. Setting up Inclusion and Exclusion Criteria
To ensure that a review is done in an organised way, the researcher set inclusion and exclusion criteria and provided transparency with regard to the strengths and any limitations of the study [9].
Inclusion Criteria: Based on the definition of GMP, this scoping review considered all published studies in English and reports about GMP activities at the community level as conducted by CHWs. The GMP activities were for children under 5 years of age. There was no restriction based on the location of the study. These studies were published in peer-reviewed journals the world over up to April 2022, along with unpublished (grey literature) found up to April 2022. The review also targeted both quantitative and qualitative research and reports.
Exclusion Criteria: This scoping literature review excluded GMP activities done at the primary health facility level along with any other GMP activities not conducted by CHWs or equivalent cadres within the health system. This is due to the overall study objectives, which looked at GMP activities conducted by CHWs at the community level.
3.3. Step 3. Search Strategy
The search strategy combined sets of keywords using and/or terms. The keywords growth monitoring and promotion, community health workers, caregivers of children under five years, child health indices, and index development were used to search for relevant literature from Science Direct, Google Scholar, EBSCO, and PUBMED databases. Reference lists of identified articles were searched for additional sources. The literature obtained was screened for relevance per the review methods in the following sections.
3.3.1. Methods of Review
Study titles and abstracts were reviewed independently by the primary researcher and then shared with the promoters to identify and compare studies and reports relevant to this scoping review. Once defined as relevant, the full articles were reviewed. Disagreements were solved through discussions, and all promoters reached a consensus. A detailed flow chart (Fig. 1) below was made to show the article selection process.
3.4. Step 4. Data Extraction and Quality Review
3.4.1. Rodgers Evolutionary Concept Analysis Framework
The Rodgers’ evolutionary concept analysis framework was used to guide this study phase. According to Rodgers, for one to understand concepts clearly, contextual forces influencing a specific idea at a particular point in time need to be understood [10]. Attributes are the characteristics describing a concept which for the study were GMP activities and index development. Antecedents and consequences give context and answer the questions about what has been affecting GMP, along with any indexes that have been developed towards improving child health. This would thus enable identifying gaps for further research on GMP activities [11].
A data collection form was developed, which was guided by Rodgers’ Evolutionary Conceptual Analysis Framework [11], to ensure uniformity and quality in the extraction of data from studies that met the inclusion criteria by reviewers. Through the use of this framework, antecedents, attributes, and consequences were assessed. The strength of this framework is that it can contribute to clarifying, describing, and explaining GMP activities and index development concepts by analysing how a chosen concept has been used within the discipline [10]. Articles and reports were assessed for clarity in presenting attributes, antecedents, and consequences of GMP activities and index development.
All the selected articles were subjected to the AMSTAR quality assessment tool and met the minimum standards required. These findings are presented in Table 1 below:
Table 1.
| AMSTAR Criteria | Response | Action Taken |
|---|---|---|
| 1. Was an ‘a priori’ design provided? | Yes | Before the scoping literature review, a review protocol was developed. |
| 2. Was there a duplicate study selection and data extraction? | Yes | Three reviewers reviewed articles |
| 3. Was a comprehensive literature search performed? | Yes | Original quantitative and qualitative research articles and reports were obtained from Google Scholar, Science Direct, PUBMED, and EBSCO databases. |
| 4. Was the status of publication (i.e., grey literature) used as an inclusion criterion? | Yes | This is as per the literature search inclusion criteria. |
| 5. Was a list of studies (included and excluded) provided? | No | This was not supplied but was available on request. |
| 6. Were the characteristics of the included studies provided? | Yes | These are summarised in Table 2 as per three characteristics of Rodgers’ Evolutionary framework, i.e., antecedents, attributes, and consequences. |
| 7. Was the scientific quality of the included studies assessed and documented? | Yes | These were assessed based on the 14-point quality assessment tool and Rodgers’ Evolutionary Conceptual Framework. |
| 8. Was the scientific quality of the included studies used appropriately in formulating conclusions? | Yes | Included studies were guided by Rodgers’ Evolutionary framework. |
| 9. Were the methods used to combine the findings of studies appropriate? | N/A | The Rodgers’ Evolutionary Framework guided the articles for this review. |
| 10. Was the likelihood of publication bias assessed? | N/A | The review was guided by Rodgers' Evolutionary Concept Analysis framework. The limitations of this Scoping review are highlighted. |
| 11. Was the conflict of interest stated? | Yes | All the authors declared that they had no conflicts of interest. |
3.5. Step 5. Data Analysis, Synthesis, and Dissemination of Results
The initial electronic database search yielded a total of 535 research articles, and 316 were further assessed for their relevance to the study. After screening the titles and abstracts, 140 articles were excluded from the search as they did not contain adequate evidence per the Rodgers Evolutionary Framework. After the full-text review, it was agreed that 80 articles out of 220 articles met the inclusion criteria. A total of 25 articles were included in the final analysis, as shown in Fig. (1). The studies included fell within the Rodgers Evolutionary Framework as either antecedents, attributes, or consequences. The results are shown in the PRISMA flow diagram shown below:
4. ANTECEDENTS, ATTRIBUTES, and CONSEQU-ENCES of GMP ACTIVITIES
4.1. Antecedents
The antecedents found in the literature were distance and socio-cultural constraints, participation of fathers in GMP activities, CHW activeness, poor understanding and interpretation of growth charts, poor communication between caregivers and CHWs, and full vaccination status and complacency. These are shown in Table 2.
4.1.1. Distance and Socio-Cultural Constraints
Some studies have noted that in many rural settings, distance is a determent to caregivers in seeking GMP services. Carrying the child long distances, some beyond 10 kilometres, particularly as the child ages, has been expressed as a burden by many mothers. This aspect is further compounded by seasonality and extreme weather conditions, such as heavy rains resulting in flooding. Also, on the other hand, mothers are burdened by long hours of agricultural and domestic chores. Due to gendered divisions of labour, mothers were primarily responsible for seeking health care for their children despite whatever workload was on their shoulders [5, 12-15].
4.1.2. Participation of Fathers in GMP Activities
Fathers are the household heads and, in most instances, the financial providers for their families. A few studies have identified that the participation of husbands in GMP activities is low, and many view child health-related education activities as insignificant [16, 17, 19]. Other studies have noted through discussions with the fathers how they did not perceive it as part of their responsibility to take children to health centres, and without the support of husbands, GMP is unlikely to succeed in some communities [18, 17, 13]. This means that if support from fathers is absent, this may ultimately affect the attendance of GMP by mothers.
4.1.3. CHW Activeness
Counselling offered to caregivers during routine GMP activities has been seen to be weak [6, 21, 22]. CHWs seem to mainly give emphasis weighing the children in the absence of giving counselling based on the child’s growth curve [20, 24, 25]. This then results in the caregivers not fully understanding their child’s growth pattern along with whether they are practising the age-appropriate IYCF practices or an improvement needs to be done.
4.1.4. Understanding and Interpretation of Growth Charts
This aspect is both on the part of the caregivers and the CHWs. There is inconsistency by CHWs in performing GMP activities, leading to faulty interpretation of children’s growth patterns. On the other hand, despite having good knowledge of the purpose of the growth chart, some caregivers are also unable to interpret the growth curves [6, 27-32, 50].
4.1.5. Communication Between Caregivers and Health Workers
The viewpoints of mothers and CHWs are of concern in GMP activities. A few studies have shown that poor communication between mothers and health workers was one of the reasons for a decrease in the use of health facilities and GMP activities. While mothers interpret health concepts from a social standpoint, health workers do so in relation to their technical knowledge, and this, at times, results in a never-ending standoff between them [33-36].
4.2. Attributes
The attributes of GMP are the independent components of growth monitoring and promotion which were identified to be the education status of parents and the knowledge, attitude, and practices of caregivers. These are shown in Table 2 below.
4.2.1. Education Status of Parents
The educational status of the mother has been found to be significantly associated with positive childcare practices, such as improved IYCF practices and routine GMP attendance. A positive influence of the higher educational status of fathers on GMP utilisation has been noted as well. This also confirmed that fathers/husbands are indeed very influential regarding decisions for the utilisation of health services [13-15, 38, 39, 49]. Literature has thus shown the importance of parental education to positive child health outcomes.
4.2.2. Knowledge, Attitude and Practices of Caregivers
Caregivers/mothers generally have high knowledge of the child’s GMP and its benefits. This does not always, however, translate to the utilisation of available GMP services though there are some studies that have shown that mothers who had adequate knowledge of GM were more likely to utilise GMP than those with inadequate knowledge. The same can be said for the attitude of caregivers as well. [13-15, 26, 32, 40, 41].
4.3. Consequences
The consequences identified from the reviewed literature were timely health interventions, improved child health outcomes, and a platform to promote optimal child health practices. These are shown along with their literature sources in Table 2.
4.3.1. Timely Health Interventions
The frequent contact with caregivers of children under five years, in most cases, leads to the strengthening of essential nutrition and child health services such as child immunisations. Furthermore, when caregivers attend GMP activities routinely, it enables timely interventions to be given to a child should they need it. GMP is an opportunity for growth faltering to be identified and the allowance for remedial action to be provided timely [21, 23, 42, 43].
4.3.2. Improved Child Health Outcomes
The first two years of a child’s life are extremely important. They are a ‘critical window of opportunity’ during which caregivers are able to ensure that they practice age-appropriate infant and young child feeding practices in order to prevent malnutrition. Malnutrition increases the risk of diseases and death, reduces cognitive development, and may lead to decreased productivity in later years, with consequences affecting the economic development (Gross Domestic Product) of a nation. Through routine GMP, child health outcomes have the potential to be improved and thus also saving nations a lot of money used in treating certain conditions that end up developing as a result of malnutrition [13, 21, 23, 42].
4.3.3. A Platform to Promote Optimal Child Health Practices
The time when a caregiver and health worker interact is very important in a child’s life. This interaction is expected to raise awareness and knowledge of appropriate childcare practices, which in some cases leads to improved child healthcare behaviour [21, 22, 44]. Regular GMP increases the frequency of contact between CHWs and mothers while also encouraging the use of preventive and curative health services by mothers. Increasing time for interaction with caregivers could also improve their knowledge [43]. This is important as it aids in the early detection of preventable diseases, such as measles and polio, which can be prevented through vaccinations.
| Antecedents | Literature Sources | Years of Studies were Published |
|---|---|---|
| Distance and socio-cultural constraints | [5, 12-14] | 2018 – 2021 |
| Participation of fathers in GMP activities | [16-19] | 2014 – 2017 |
| CHW activeness | [6, 20-25] | 2008 – 2022 |
| Understanding and interpretation of growth charts | [ 5, 5, 23, 26-32] | 2007 – 2022 |
| Communication between caregivers and CHWs | [33-36] | 1999 – 2007 |
| Attributes | Literature Sources | Years of Studies were Published |
| Education status of parents | [13-15, 38, 39, 49] | 2005 – 2022 |
| Knowledge, attitude, and practices of caregivers | [13-15, 26, 32, 40, 41] | 2017 – 2021 |
| Consequences | Literature Sources | Years of Studies were Published |
| Timely health interventions | [21, 23, 42, 43] | 2008 – 2022 |
| Improved child health outcomes | [13, 21, 42] | 2008 – 2019 |
| A platform to promote optimal child health practices | [21, 22, 42-44] | 2008 – 2021 |
4.5. What Indexes have been developed towards improved child health through GMP
There are several child health and development indexes, namely Weight-for-height (WFH), Height-for-age (HFA), Weight-for-age (WFA), etc., which all provide health practitioners with different inferences. While some of the indices from the literature are location specific, i.e., USA, European Union, and those developed by the World Health Organisation, such as the WHO Growth Standards, and are for global use, they all have something in common. Their value resides in providing a measure of the general well-being of populations, formulation of health-related policies, and enabling interventions to be planned and monitored [3]. The different indexes identified are shown in Table 3 below:
| Name of Index | Year Developed and by | Specific Country used | Objective |
|---|---|---|---|
| Weight-for-height/length (WFH) | 2006, WHO | Worldwide | To determine the prevalence of wasting |
| Height-for-Age (HFA) | 2006, WHO | Worldwide | To determine the prevalence of stunting |
| Weight-for-Age (WFA) | 2006, WHO | Worldwide | To determine the prevalence of underweight |
| Mid Upper Arm Circumference (MUAC) | 1950s, Jelliffe | Worldwide | To measure levels of malnutrition |
| Child Well-being Index | 2009, Bradshaw, Hoelscher, and Richardson | European Union | Multi-dimensional understanding of child well-being |
| Child Opportunity Index | 2014, Acevedo-Garcia et al. | USA | A tool to monitor health equity |
From the literature review, it is clear that no existing indices interlink CHW activities and caregiver behaviours toward GMP. The Child Well-being index [46] and the Child Opportunity Index [47] are not very commonly used, whilst the WHO growth Standards only focus on measuring the child's nutrition status. At the same time, no consideration is given to caregiver behaviours towards GMP.
It is thus imperative that more population-based indices are developed that not only focus on children under five years, but also take into consideration caregiver behaviours. These behaviours encompass any barriers and facilitators towards GMP activities.
5. DISCUSSION
It was noted that there are a plethora of opinions on GMP effectiveness based on the varying types of evidence or a lack thereof, and this has resulted in the quality of GMP itself being questioned [21, 25, 30]. GMP is complex with no ‘one size fits all’ approach towards an effective way to improve it.
Perhaps looking at the different activities encompassed under GMP, i.e., accurate weight measurements, plotting on the growth chart, interpreting the growth curve, discussing options with caregivers, and evaluating the child’s response [21], it may be necessary to strengthen the caregiver involvement as literature has shown that the GMP attributes, antecedents, and consequences have one common denominator, i.e., caregivers of the children.
With a new paradigm shift being brought about by the era of Social Behaviour Change (SBC) towards strengthened GMP activities, it is necessary to explore the strong evidence that SBC can improve GMP through locally tailored messaging which is delivered with sufficient coverage, frequency, and salience [42, 45, 48].
This use of strategies such as formative research to develop robust SBC plans, which include counselling and other communication promoting child growth and development interventions; strengthening community health worker facilitation and counselling capacity with appropriate performance support; and amplifying actions by linking with other sectors providing inputs that enable social and behavior change, [20, 37]. Using growth-outcome data to stimulate collective action and improve community accountability for creating an environment that fosters healthy growth merits attention as part of a strong SBCC plan. The underlying logic is that if growth faltering is detected early and is made visible to health workers and families, then families can respond by changing their child-care practices [21].
The use of different SBC techniques in index development could contribute significantly towards more meaningful GMP indices, which also combine caregiver behaviours as these are also key in GMP activities.
6. GAPS FOR FURTHER RESEARCH
Based on this scoping literature review on GMP activities, much work remains to be done regarding GMP activities and evidence to support in sub-Saharan Africa. This is despite a lot of efforts in putting GMP programmes in place. There is often little to no effort in setting aside funding for research and publishing what has worked. Information remains grey literature despite the numerous programmatic reports and program evaluations done.
(i) There is a need to measure at the output and not outcome level the extent to which caregivers affect routine GMP activities and how their poor participation affects child health outcomes.
(ii) There is a need to expand operational research to unpack delivery approaches along with targeting, cost-effectiveness, and scalability of a more comprehensive and fully inclusive GMP activity model. Among many other aspects, this can involve looking at how the participation of fathers impacts GMP activities.
(iii) There is a need for the development of novel indexes which tie together some of the modern approaches/strategies of SBC toward improved child health.
(iv) More GMP Indices need to be developed that use different methodologies to capture barriers and facilitators of caregivers towards GMP Index development.
7. STUDY LIMITATIONS
The findings from different literature sources reviewed were presented according to themes, i.e., attributes, antecedents, and consequences, and not independently. This then limits the extent to which opinions can be generalized, along with possible biases towards themes.
CONCLUSION
GMP is complex, and as such, indicators of measurement are rendered complex due to the multi-dimensional nature of factors affecting GMP. Programmes implementing GMP activities need to invest in further research so as to provide an increased evidence base to guide the health system, funders, and policymakers conclusively.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS FOR REPORTING
PRISMA guidelines and Rodgers concept analysis framework.
AVAILABILITY OF DATA AND MATERIALS
Data will be available upon request from the corresponding author. This was a literature review and all sources of literature were listed in the References Upon graduation, all data will be placed in the University of Venda Repository.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIALS
PRISMA checklist is available as supplementary material on the publisher’s website along with the published article.

