All published articles of this journal are available on ScienceDirect.

Evaluation of the Results of the Screening Program of Phenylketonuria in the South East of Iran during the Years 2014-2020
Authors Info & Affiliations
Abstract
Aim:
The aim of the study was to evaluate the results of the screening program for phenylketonuria in the South East of Iran during the years 2014-2020.
Background:
Screening and timely treatment of neonatal phenylketonuria can prevent the irreversible complications of the disease. Therefore, screening is essential during the early days post birth.
Methods:
This cross-sectional (descriptive analytical) study was conducted by census sampling method in the south of Iran during the years 2012-2019. Of 110,073 babies born in 7 cities affiliated with Jiroft University of Medical Sciences, 105,778 (96.09%) babies were screened. Data analyses and statistical analyseswas completed using SPSS software version 24. Descriptive statistics was used to calculate the frequency and prevalence of the disease using the formula of the number of new cases of the disease divided by the population at risk each year.
Results:
The highest percentage of timely screening (87.82%) was related to Jiroft city. 221 babies initially tested positive and resampling was completed. After measuring the level of phenylalanine by the HPLC method, 12 babies were referred to the phenylketonuria treatment center as a positive confirmation of the diagnosis. They were treated with the opinion of a pediatrician as a definite positive for phenylketonuria. The incidence of phenylketonuria was 1.09 per 10,000 live births. The highest incidence was related to South Roudbar (1.81 per 10 thousand live births) and Jiroft (1.58 per 10 thousand live births) cities, respectively.
Conclusion:
Since evaluating any health-related program requires a rigorous data collection system, more attention must be taken to record the data needed to evaluate the program.
1. INTRODUCTION
Phenylketonuria is an autosomal recessive genetic metabolic disease caused by a defect in the enzyme phenylalanine hydroxylase, which converts phenylalanine to tyrosine [1]. Accumulation of phenylalanine causes problems in the body's natural metabolism and delays in a person's cognitive, personal, social, and motor development [2]. The most obvious clinical manifestation of this disease is severe mental retardation. Other symptoms of this disease include hyperactivity, epilepsy, defects in skin and hair pigments, and a small head circumference with a prominent upper jaw [3]. The affected child is normal at birth, and if he is not treated, his IQ will decrease by four points per month, and he will lose 50 points in the first year [4].
In 1934, Asborn identified phenyl pyruvic acid in the urine of mentally disabldisabled children [5], a year later, Penrose named this condition phenylketonuria [6]. Based on studies conducted, the incidence of the disease varies in different countries, such that the lowest incidence of the disease is 1 in 327,740 births in Thailand [7], and the highest incidence is 1 in 2600 in Turkey [8]. According to studies, the incidence of PKU in various regions of Iran has been reported as ranging from 0.66 per 10,000 [9] to 1.91 per 10,000 live births [10] According to the latest report of the Ministry of Health, the incidence of the disease is calculated as one in 6000 live births for the whole country [11]. Researchers have stated the most important reason for the high incidence of the disease is the high frequency of consanguine marriages [12]. In studies conducted in various regions of Iran, most of PKU patients’ parents had a consanguineous marriage [10, 13-15].
In the early 1960s, Guthrie introduced Guthrie's test to measure the blood level of phenylalanine [16]. Diagnosis of this disease in its early stages is done through a screening test. In some developed countries, more than 50 years have passed since the commencement of screening programmes for this disease [17]. Prior to the commencement of screening programs, early diagnosis of the disease was delayed due to the non-specificity of the symptoms in the first days of life, and this issue was associated with the loss of IQ to varying degrees [18].
Today, in the first few days following birth, patients with phenylketonuria are diagnosed using a screening test. During the screening stage, just a few drops of blood are taken from the baby's heel, by performing the test hidden cases in babies can be identified [19]. Appropriate treatment of newborns, which mainly includes nutritional therapy during the first two weeks of life, changes the consequences of the disease and leads to normal growth and development in the newborn [20].
Phenylketonuria, by causing mental and physical complications, in addition to affecting the quality of life of patients, imposes a significant economic, social, and psychological burden on the patient's family and a large financial burden on the health system [21]. This disease has been mentioned as one of the problems of the health system, which has led health system administrators to implement appropriate solutions to reduce the burden of this disease [22].
Considering the social and economic burden caused by the birth of patients with fetal abnormalities and genetic diseases, laws and regulations were established in Iran to prevent the occurrence of these diseases, and it is possible to issue an abortion license before the 20th week of pregnancy [23]. Considering that the diagnosis of phenylketonuria is possible in the first months of pregnancy [24], the prognosis of these patients depends on the control of the disease in the first years of life, especially the first four years [25].
Patients with phenylketonuria, like other hereditary metabolic diseases, should be monitored in a special clinic for metabolic diseases under the supervision of a team consisting of nutritionists, pediatricians, psychologists, social workers, and nurses, and successful treatment requires the continuous cooperation of the child and the parents of the affected child with the treatment team [26].
By knowing the incidence of PKU, it is possible to plan and focus on solving this problem within the region, additionally by knowing the percentage of family marriages that have a direct relationship with PKU cases, it is possible to plan to reduce the cases of family marriages that play an important role [27] and increase the accuracy of the follow-ups and control programs of the University Health Vice-Chancellor to prevent the occurrence of diseases.
Newborn screening for this disease has been operational in the medical sciences of Jiroft since June 2013. However, no study has been conducted on the screening results and the incidence rate in the cities affiliated with Jiroft University of Medical Sciences. Therefore, this study aims to determine the incidence of phenylketonuria and evaluate laboratory indicators, including sensitivity, specificity, and positive and negative predictive values based on the results of newborn screening since the commencement of the screening program in the affiliated cities of Jiroft University of Medical Sciences.
2. MATERIALS AND METHODS
This study is a health system management study and a cross-sectional study (descriptive-analytical) that is conducted on all phenylketonuria patients identified by heeldiagnostic tests on babies 72 hours after birth. The optimum conditions for testing include from 72 hours to 5 days following birth and where the mother is breastfeeding. Just a few drops of blood are taken from the heel of the foot and collected on special papers (Guthrie card). confirmatory test of all suspicious and positive samples are then conducted in partner laboratories. This study will be carried out during the years 2014 to 2020 under the supervision of Jiroft University of Medical Sciences. The inclusion criteria is all screened Iranian and non-Iranian babies living in the cities affiliated with Jiroft University of Medical Sciences and the patients subsequently identified during the screening process including false negative casesExclusion criteria includes babies who live in other provinces but were screened in Jiroft, were found to be positive and were under the supervision of a focal point physician. Rarely, newborn screening results are falsely negative but the baby actually has that disease. Possible reasons for false negatives include laboratory errors such as mixing samples and performing the test too early. Because false negatives are possible, more tests should be done if the baby's family has a history of a particular disease or if the baby shows signs and symptoms regardless of the screening results. Within 2 to 3 weeks after the newborn screening test, the results are sent to the child's doctor or clinic. Positive results mean that at least one test was outside the normal range. Other terms for a positive result include failed, out of range, or abnormal. The treatment provider will notify the parents of a positive result. A positive result does not mean that the baby will definitely have the disease, but it indicates that more tests should be done as soon as possible (diagnostic tests that detect the disease). If the baby has the disease, further tests will quickly allow for treatment or management, such as a special diet that should be started immediately after birth.
Often, when the screening result is positive, subsequent diagnostic tests show that the child does not have the disease. In these cases, the results of the child's test are called false positives, that is, the test shows the risk of a disease while the child is not really suffering from it. False positives occur when screening tests are designed to identify as many sick infants with treatable diseases as possible. Because it is important not to miss the affected babies, some babies who are not affected also give positive results. Occasionally, the results of the newborn screening test are reported as borderline. These results are not completely normal, but they are not clearly abnormal either. In these cases, the provider of the baby's medical services repeats the test. Moreover, true and false positives and negatives are determined, and then the screening indices, including sensitivity, specificity, and positive and negative predictive values are calculated using the following formulas.
 |
 |
 |
 |
The measurement tool in this research will be the national form of epidemiological investigation of cases of genetic diseases. From this form, the sections related to the patient's profile (gender, date of birth, care status, treatment start date, status of other physical siblings) and parents' profile (year of marriage, kinship relationship) are extracted.
Using the information received from the patient's family, the information in the genetic file, family health file, and patient treatment file, this form was completed by the genetics program expert of the health center and approved by the genetics program expert of the deputy health department.
Screening information will also be used in the comprehensive social genetics program form, the summary form of PKU and hyperphenylalaninemia screening information, which is completed at all health centers. The sampling method is census. In this study, all newborns were screened and patients identified during the years 2012-2019 were included in the study. The method of data analyses and statistical analyses of data extracted using SPSS software version 24. Weused descriptive statistics to calculate the frequency and prevalence of the disease using the formula of the number of new cases of the disease divided by the population at risk in each year.
In order to comply with ethical considerations, patient information was kept confidential, only approved persons could access the information In order to collect data, the names of patients and their families were excluded, and data collection commenced after obtaining the code of ethics (IR.JMU.REC.1400.023) from Jiroft University of Medical Sciences.
3. RESULTS
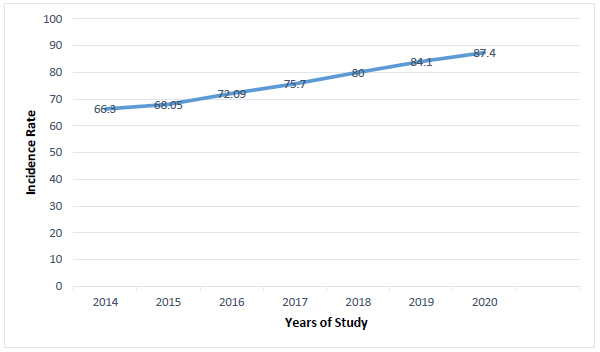
Over the duration of the study 110,073 babies were born in the 7 cities affiliated with Jiroft University of Medical Sciences, 105,778 (96.09%) babies were screened. 79,991 (75.62%) of the babies participated in the screening program during the 3rd to 5th day post birth. Timely screening increased from 66.3% in 2014 to 87.4% in 2020 (Fig. 1). The highest percentage of timely screening (87.82%) was related to Jiroft city. 221 babies initially tested positive, and re-sampling were then completed. After measuring the level of phenylalanine by the HPLC method, 12 babies were referred to the phenylketonuria treatment center as a positive confirmation of the diagnosis and were treated with the opinion of a pediatrician as a definite positive for phenylketonuria.
The incidence of phenylketonuria was 1.09 per 10,000 live births. The highest incidence was related to South Rudbar (1.81 per 10 thousand live births) and Jiroft (1.58 per 10 thousand live births) cities, respectively.
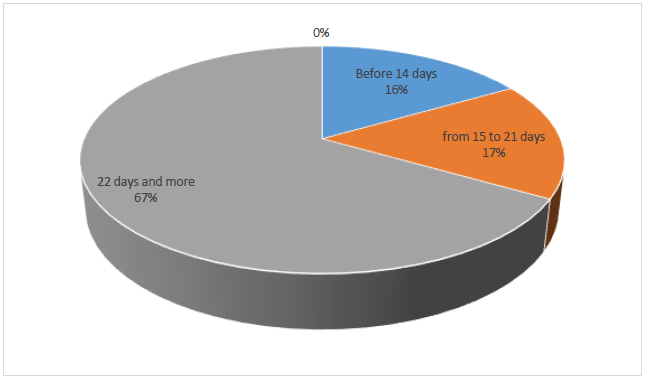
The results of newborn screening and the incidence rate are presented in Table 1. Frequency and annual occurrence rates are presented in Table 2. The time of the first visit of 33% of sick babies to the phenylketonuria treatment center was before 21 days of age (Fig. 2).
| Location | Number of Live Births |
Number of Newborn Screened (Percentage) |
Number of Newborns Screened during First 3 to 5 Days (Percentage) |
Phenylalanine Levels (At Screening) |
Phenylalanine Levels (At Diagnosis Confirmation) |
Number of Patients | Incidence (PKU) in 10000 Live Births | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
<4 mg/dl |
4-19.9 mg/dl | ≥ 20 mg/dl |
<3.4 mg/dl |
3.4-19.9 mg/dl | ≥ 20 mg/dl | ||||||
| Kahnouj | 19096 | 14095(73.8) | 8986(63.75) | 14071 | 24 | 0 | 23 | 1 | 0 | 1 | 0.52 |
| Ghaleghanj | 12683 | 12251(96.6) | 7954(64.92) | 12231 | 20 | 0 | 19 | 1 | 0 | 1 | 0.78 |
| Anbarabad | 12574 | 11311(89.9) | 7635(67.50) | 11283 | 28 | 0 | 28 | 0 | 0 | 0 | 0 |
| Faryab | 3336 | 4813(144.2) | 3616(75.12) | 4793 | 20 | 0 | 20 | 0 | 0 | 0 | 0 |
| Jiroft | 31464 | 32123(102) | 28213(87.82) | 32054 | 68 | 1 | 64 | 4 | 1 | 5 | 1.58 |
| Manoojan | 8921 | 10440(117) | 7849(75.18) | 10419 | 21 | 0 | 20 | 1 | 0 | 1 | 1.12 |
| Roudbar | 21999 | 20745(94.2) | 15738(75.86) | 20705 | 38 | 2 | 36 | 2 | 2 | 4 | 1.81 |
| Total | 110073 | 105778(96.1) | 79991(75.62) | 105556 | 219 | 3 | 210 | 9 | 3 | 12 | 1.09 |
| Date | Number of Live Births |
Number of Newborn Screened (Percentage) |
Number of Patients who Screened Positive for PKU | Incidence (PKU) in 10000 Live Births |
| 2014 | 18509 | 16284 (87.9) | 1 | 0.54 |
| 2015 | 17668 | 17225 (97.5) | 0 | 0 |
| 2016 | 17419 | 15679 (90.1) | 3 | 1.72 |
| 2017 | 15620 | 15221 (97.4) | 3 | 1.92 |
| 2018 | 14554 | 14647 (100.6) | 2 | 1.37 |
| 2019 | 13489 | 13315 (98.7) | 1 | 0.74 |
| 2020 | 12814 | 13407 (104.6) | 1 | 0.78 |
| Total | 110073 | 105778 (96.1) | 12 | 1.09 |
In this study showed that indicators are equal to False positive: 210, False negative: 0, True positive: 12, True negative: 105,556 and also Sensitivity: 100%, specificity: 99%, positive predictive value: 0.05%, negative predictive value: 100%
The first visit of patients identified in the screening program, to the PKU treatment center based on the neonate's age indicate in Fig. (2).
4. DISCUSSION
Many countries in the world, including Iran, have implemented comprehensive national NBS programs with relatively high coverage. The purpose of the phenylketonuria screening program in Iran is to reduce physical disability, mental retardation and medical and non-medical costs. Moreover, this study was conducted to investigate the screening and prevention program of PKU in the areas covered by Jiroft University of Medical Sciences.
The results of this study showed that the screening coverage in all cities of Jiroft is 96.09%, which is lower than the national average (100.65%). The results of previous studies in other provinces of Iran, including South Khorasan, have reported 100% PKU screening coverage between 2013 and 2014 [28]. However, in a study conducted in Tehran, 91.4% of infants were screened for PKU in 2011 [29]. Ganji et al. also reported 100% screening coverage in Chaharmahal and Bakhtiari Province [30], which is consistent with the results of the present study. In studies conducted in Brazil and China, the average screening coverage was reported to be 94.5% and 93.6%, respectively [31, 32]
According to the results of the present study, 79,991 (75.62%) newborns had received timely screening; the highest percentage was from Jiroft city (87.8%). Timely screening has increased from 66% in 2014 to 87 percent in 2020, which has caused a decrease in the incidence of the disease from 2014 to 2020. This may be due to increased awareness and referral of mothers to health care centers. In the study of Ganji et al. in Chahar Mahal and Bakhtiari provinces, the initial sampling in the studied years had an upward trend and reached 84.6% in 2014 [30], which is consistent with the results of this study.
Due to mental retardation in patients with PKU, early diagnosis of the disease and the need for timely medical interventions play a prominent role [33]. In this study, 221 babies initially tested positive screening and re-sampling was completed. After measuring the level of phenylalanine by the HPLC method, 12 babies were referred to the phenylketonuria treatment center as a positive confirmation of the diagnosis and were treated. The first visit of 33% of sick babies to the phenylketonuria treatment center was before 21 days of age (Fig. 2).
Before the start of the newborn screening program, patients were identified late and most had complications. In a study in Ahvaz, which was conducted on patients aged 1-18 years, the age at which this disease was diagnosed was over six months in 77.7% of cases [34]. In a study conducted in Mazandaran, the mean age of PKU patients at the time of diagnosis was 20 [35]. Factors such as failure to perform screening on time, delay in reporting positive cases, insufficient sampling conditions and disease of the baby, and lack of cooperation of parents affected this index.
In this study, like the study conducted by Ganji et al., no false negative cases were reported [30]. However, in other similar studies, there was no mention of false negatives [28, 36].
The prevalence of PKU varies among ethnic groups and geographic regions around the world. A global comparison of PKU incidence among countries with NBS shows that Japan, among Asian countries, reports the lowest rate at 1: 125,000, while the incidence in China is 1: 17,000 [37]. The incidence of PKU in Saudi Arabia is 1: 14,623 [38] and in the UAE is 1: 12,369 [37], which is similar to Japan. In a comprehensive systematic study conducted in Iran, the incidence of PKU was estimated to be 16.5/100,000 (95% confidence interval: 21.2-12.9). The incidence of PKU in male and female infants was was estimated as 13.3/100,000 (95% confidence interval: -7.5- 15.8) and 10.9/100000 (95% confidence interval: 7.5-15.8) respectively [8].
The results of studies in Iran showed a significant difference in the prevalence of PKU across different regions, this may be due to ethnic differences in different geographical regions [35, 39].
In the present study, the incidence of phenylketonuria in Jiroft City was 1.09 in 10 thousand live births. The highest incidence was related to South Roudbar (1.81 per 10 thousand live births) and Jiroft (1.58 per 10 thousand live births) cities. PKU incidence rate was reported to be 0.66 in 10,000 in Mazandaran [9], 0.99 in 10,000 in Southern Khorasan [40], 1.35 per 10,000 in Kerman [13]. 1.6 In 10,000 in Fars [41], and 1.91 in 10,000 in live births in Lorestan [10].
PKU disease has a hereditary pattern and is influenced by consanguineous marriages, which may double the chance of contracting the disease [42]. In a study in a village in Kermanshah province, the incidence rate of this disease was estimated to be 1 in 80 people, and the main reason for the high prevalence of the disease was the high desire for consanguineous marriages in the village [43]. In the studies conducted by Motamedi et al., 82% [44], and Eshraqhi et al., 60% [15] of parents of PKU patients were married within the family.
CONCLUSION AND RECOMMENDATIONS
Starting treatment before one month has the best prognosis in the treatment of patients. In addition to the necessity of implementing a screening program, a quality control system should also be used for newborn screening to guarantee the performance of the program in order to witness a decrease in the incidence of the disease phenotype within a population. Therefore, the attention and awareness of families and doctors in this matter is essential. With timely treatment, 90% of people benefit from the appropriate treatment regimen. Screening should be undertaken for all members of the patient's family. In order to promote the screening program in countries where this is being implemented, parents arents, and doctors should be informed about the benefits of newborn screening, and there should be a robust follow-up, and documentation system in place .
LIMITATIONS OF THE STUDY
Among the limitations of the present study, we can point out the type of study (cross-sectional), the small number of samples, and its implementation at the level of the affiliated cities of Jiroft University of Medical Sciences. Therefore, because this study was conducted at the level of several cities, it is necessary to be cautious about generalizing the findings. To solve the mentioned limitations, it is recommended to conduct similar research at national . In this study, only the incidence rate was calculated based on the newborn screening program, false negative cases and cases that did not participate in the screening program may be detected late, so the actual incidence rate may be higher than the current reported rate.
AUTHORS' CONTRIBUTIONS
E.R. wrote and conceptualized the study, completing the final draft of the article. S.H. and S.K. performed data capturing and analysis. S.D. and R.R. completed the methodology section.
LIST OF ABBREVIATIONS
| PKU | = Phenylketonuria |
| SPSS | = Statistical Package for Social Sciences |
| NBS | = National Bureau of Standard |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
.This study was approved by the Biomedical Research Ethics Committee of Jiroft University of Medical Sciences and issued the study’s code of ethics (IR.JMU.REC.1400.023).
HUMAN AND ANIMAL RIGHTS
No animals were used for the studies which are the basis of this research. All human procedures followed were per the guidelines of the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
In order to comply with ethical considerations, patient information was kept confidential and only accessible to au8thorized personnel. In order to collect data, the names of patients and their families were not used, and data collection was done after obtaining the code of ethics from Jiroft University of Medical Sciences.
FUNDING
This article has been completed with the financial support of Vice-Chancellor of Research and Technology of Jiroft University of Medical Sciences.
STANDARDS OF REPORTING
STROBE guidelines has been followed.
AVAILABILITY OF DATAS AND MATERIALS
The data that support the findings of this study are available from the corresponding author [S.D] upon reasonable request.
CONFLICT OF INTERESTS
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This article is the result of the research project approved by the Vice-Chancellor of Research and Technology of Jiroft University of Medical Sciences, for which we are deeply grateful. We thank and appreciate the cooperation of the health department of Kerman University of Medical Sciences and the staff of the genetic counseling center.

