All published articles of this journal are available on ScienceDirect.

Application of Geographic Information Systems in the Study of COVID-19 in Morocco
Abstract
Introduction:
The 2019 coronavirus disease (COVID-19) was first identified as a respiratory disease that originated in Wuhan, Hubei Province, China. The WHO declared the COVID-19 outbreak a public health emergency of international concern on 30 January 2020. Morocco reported its first coronavirus case on 2 March 2020. During the week of 9-15 March 2020, Morocco took steps to limit the spread of the epidemic. This article describes the use of spatial data applications in epidemiological research in Morocco, specifically its response to the COVID-19 epidemic.
Methods:
To conduct this study, we relied on the use and analysis of data provided by the Moroccan Ministry of Health for the study period from May to July 2021, as well as the geographical and administrative map of the Kingdom of Morocco. Spatial analysis of COVID-19 was performed using ArcGIS 10.8 and QGIS, a geographic information processing software. Health data for the 12 regions of the Moroccan territory were presented in the number of COVID-19 cases as a discrete quantitative variable and over time as a continuous time variable.
Results:
According to a map created using GIS, the concentration of COVID-19 cases appeared to be highest in the Casablanca Settat region. Depending on the number of documented COVID-19 cases, regions were ranked as follows: Casablanca-Settat> Rabat-Sale-Kenitra> Marrakech-Safi > Fes-Meknes > Tangier-Tetouan-Alhouceima>Oriental>Souss-Massa > Béni Mellal-Khenifra> Draa-Tafilalet> Laayoune-Sakia El Hamra >Guelmim-Oued Noun > Dakhla-Oued Eddahab. The increase in cases in major cities was due to several factors, including demographic, social and environmental factors. This demonstrated the need to consider demographic contributions to environmental health. Demographic factors helped us understand the health of our environment empirically. Geography improved health decision-making and accountability. Incorporating the geographic context of the spread of COVID-19 helped decision-makers understand the impact of location on strategies and goals to combat this pandemic.
Conclusion:
This study identified areas with high and low COVID-19 clusters and hotspots. The produced maps can serve as an excellent management tool to control and effectively eliminate the COVID-19 pandemic, contributing to investments in epidemiological surveillance programs.
1. INTRODUCTION
In November 2019, an epidemic of an infectious disease called coronavirus or COVID-19, caused by the infectious agent SARS-COV-2, broke out in Wuhan, China [1]. This epidemic spread rapidly around the world, becoming one of the most devastating epidemics to infect the planet in the 21st century and spreading much faster compared to other epidemics of the past. The outbreak was declared a “public health emergency of international concern,” affecting many countries and regions [2]. On 11 March 2020, the disease was classified as a pandemic by the World Health Organization (WHO). The COVID-19 pandemic continued to grow, with Europe becoming the epicenter of the outbreak, experiencing more cases and deaths than the rest of the world combined, except China, according to the WHO. During this time, the WHO also published a clinical trial for severe acute respiratory infection (SARI) in suspected COVID-19 cases to improve the management of patients with suspected or confirmed COVID-19. Management guidelines were issued, and several countries introduced precautionary measures in an attempt to contain the spread of this pandemic.
In its response to the COVID-19 pandemic, Morocco's strategy was based on an action plan designed around three axes: health, economy and social order. In each of these areas, the contributions of public authorities, the private sector, and civil society limited the damage and brought the pandemic under some control. Regarding health, the intervention aimed to control the progression of the disease in order to better manage the flow through the resource-limited and unevenly distributed health system across the country.
Increasing the supply of healthcare infrastructure was a priority. Civil society also provided assistance, notably with hotels that offered rooms for health workers and convalescents mobilized in the face of the pandemic. The process was based on the Ministry of Health's Trusted Communication Policy, which ensured the daily distribution of information about the disease's progression and hygiene recommendations.
Coronavirus emerged as a major and prioritized public health problem in Morocco. Moroccan authorities mobilized all means and resources to combat this phenomenon. The fight against infectious diseases was facilitated by new data processing tools, such as satellite remote sensing, global positioning (GPS), computer hardware, image processing and database management software [3].
In epidemiology, spatial analysis integrates classical epidemiology and provides elements to support research and model construction [4]. It also allows us to deepen our analytical approaches in health geography, and its methodological corpus integrates the full range of qualitative approaches. The descriptive spatial analysis includes map analysis, geometric and spatiotemporal feature retrieval, analysis of spatial variation in values, aggregation retrieval, analysis and synthesis scale retrieval, environmental correlation retrieval, etc. Statistical model searches include spatial relationships between individuals [5].
Geographic information systems help create a spatial database of epidemics and determine the extent and pattern of their spread by mapping their geographical distribution to model the optimal management of health emergencies in affected geographic areas.
To implement preventive measures, we needed to better monitor the evolution of this pandemic using appropriate geographic information systems (GIS). This pandemic was in full swing and supported by population movements. This study is retrospective in nature and aims to map risk areas and their hierarchy according to the degree of potential risk of COVID-19 in Morocco during the three months of May, June and July 2021. It seeks to identify and utilize GIS to improve epidemiological surveillance systems. From an empirical perspective, we use spatial analysis techniques to identify areas that are particularly affected.
2. METHODS AND MATERIALS
In order to carry out this study, we used and analyzed data provided by the Moroccan Ministry of Health for the study period from May to July 2021, as well as the geographical and administrative map of the Kingdom of Morocco. Spatial analysis of COVID-19 was performed using ArcGIS 10.8 and QGIS, a geographic information processing software. Health data for the 12 regions of the Moroccan territory were presented in the number of COVID-19 cases as a discrete quantitative variable and over time as a continuous time variable.
3. RESULTS
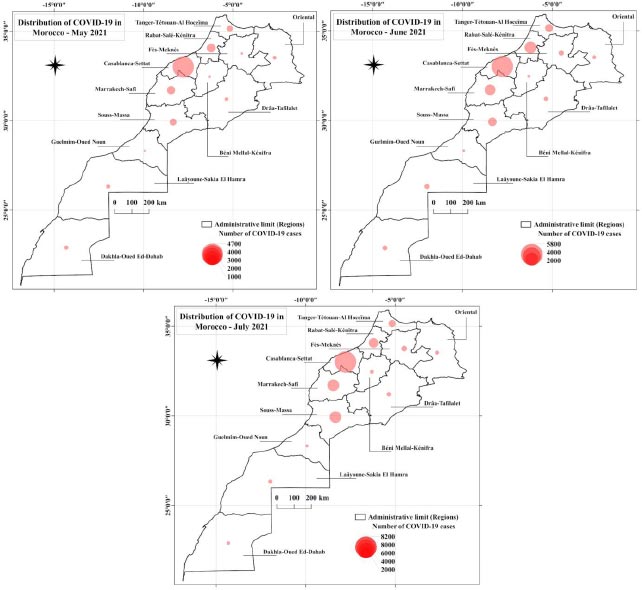
In the summer of 2021, the epidemiological situation in Morocco witnessed a significant increase in the number of COVID-19 cases. As of 31 July 2021, 623528 cases had been registered since the pandemic began to spread, resulting in a cumulative incidence rate (per 100,000 population) of 1711.3, according to the Office of Epidemiology and Disease Control. The mortality rate was 1.6%, while the recorded cure rate was 90.1%. Morocco observed an acceleration of the pandemic over the three months (May, June, and July 2021). Indicators showed an increase in epidemic activity with rising incidence and detection of clusters in different regions of Morocco.
Regional data shows that Morocco's most developed and populated regions top the rankings. Notably, the Casablanca-Setat area has 4,700 cases, followed by the Rabat-Sale-Kenitra area with 4,000 cases, and 3,000, 2,000, and 2,000 cases in Marrakech-Safi, Tangier-Tetouan-Al Hoceima, and Souss-Massa, respectively, whereas the rest of the areas have 1,000 cases. Thus, it can be concluded that just five regions account for more than three-quarters of registered cases in the country. As COVID-19 emerged strongly (but in 2021), we recognize that the different ratios obtained are important, but over time, cases increased sharply in all regions of Morocco (May 2021).
Due to this situation, our country adopted many strict measures in response, such as closing land, air and sea borders, suspending classes at all primary, secondary and higher education levels, and implementing social distancing measures at the level of mosques, including the suspension of prayers. Gradual containment of the population took place later. These measures, whose effects may be observed, could possibly allow the spread of the epidemic to be relatively slow.
The dynamics of the epidemic showed the cumulative number of COVID-19 cases in the Casablanca-Setat area (5,800 cases), Rabat-Sale-Kenitra (4,000 cases), and the rest of the regions (fewer than 2,000 cases). On the other hand, this dynamic was comparable to that observed in all regions in southern Morocco (June 2021).
Indeed, Morocco has adopted very strict containment measures compared to those of other developing countries in response to the COVID-19 outbreak. Initially, containment was effective in limiting the spread of the virus, but it could not be maintained for very long due to high social and economic costs. The pandemic hit again.
The map below depicts the distribution of confirmed cases of COVID-19 infection in the 12 administrative regions of Morocco. The regions of Casablanca-Settat and Rabat-Sale-Kenitra had the highest number of cases, with between 8,000 and 8,200 cases, respectively, followed closely by the regions of Fez-Meknes, Tangier-Tetouan-Al-Hoceima, and Draa-Tafilalt with between 4,000 and 6,000 cases [7]. In addition, the southern and eastern regions remained the least affected by the epidemic. For example, Laayoune-Sakia-El Hamra, Dakhla-Oued Eddahab, Guelmim Oued Noun, and Draa-Tafilelet, as well as The Oriental, recorded less than 2,000 confirmed cases of COVID-19 each, respectively (July 2021) (Fig. 1).
The map shows significant differences in COVID-19 cases, with densely populated areas being more susceptible to the virus. This susceptibility was influenced by factors such as humidity, vulnerability of surveillance systems, and the presence of asymptomatic cases, all contributing to the increase of this plague. Consequently, there might have been a rise in the number of infected people. Moreover, government initiatives, such as strengthening viral screening and surveillance, were being implemented to create and improve the detection of COVID-19 cases.
To slow down COVID-19, Morocco has proposed strict measures, extensive efforts towards economic compensation, and continued demonstrations of solidarity and hope from communities and individuals to mitigate the impact of the crisis. However, several sectors have been severely affected, including tourism, transport, culture, and event activities. Additionally, the informal sector, which is much more difficult to measure, has also been significantly impacted, and its workers have been among the most affected by the adverse effects of the crisis.
Each identified region is represented by a polygon marked on the map with a risk index ranging from 1 to 3, indicated by a color gradient from green for low-risk areas (index 1) to red for the highest-risk areas (index 3). Additionally, each polygon is characterized by a number of attributes specified in the database (Fig. 2). As of 2021, shortly after the easing of containment measures began, the areas of Casablanca Setat and Rabat-Sale-Kenitra were classified as high-risk, while Marrakech-Safi and Tangier-Tetouan-Al Hoceima, Souss-Massa and Oriental exhibited a medium risk. The rest of the areas were considered low-risk.
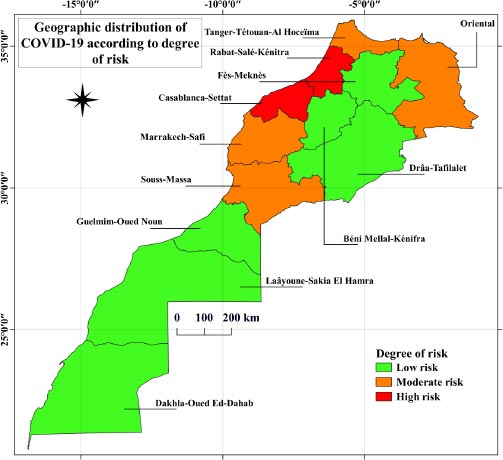
The risk indices were calculated using the following formula:
Number of new cases/ Total population exposed
This is the average risk of contracting the epidemic during the period of May, June, and July of the year 2021.
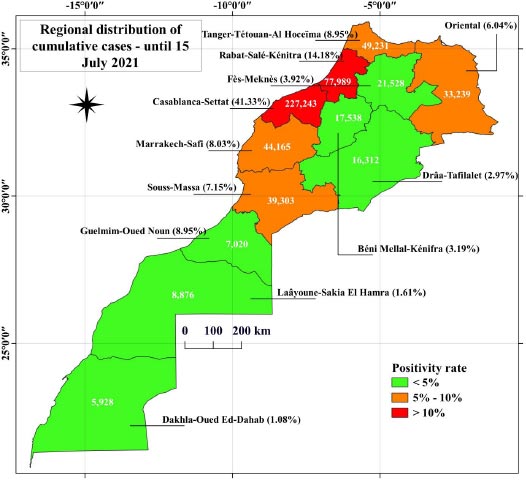
The positivity rate measures the percentage of positive cases compared to the number of tests.
In this sense, we calculated the different positivity rates for all regions of the Kingdom of Morocco. On 15 July, the Casablanca region recorded a 41.33% positivity rate, followed by the Rabat-Sale Kenitra region with a 14.18% rate. At the same time, the southern and oriental regions recorded low rates. This is illustrated in Fig. (3). The white values correspond to the cumulative number of COVID-19 in each region.
As in all other parts of the world, the first coronavirus cases in Morocco came from international contacts (travel, trade, tourism, business trips). Furthermore, Morocco had the highest international ties and was hit hardest in the early stages of the crisis. Morocco's public health system regularly faces the challenge of localizing the spread of infectious diseases.
4. DISCUSSION
Maps have become a primary mode of visualizing the COVID-19 pandemic and identifying local disease outbreaks [8]. The public health system's ability to screen for COVID-19, especially in densely populated areas, is critical for identifying, isolating, and treating infected individuals and ultimately mitigating the social impact [9]. Moreover, these skilled professionals are essential for maintaining the capacity of health services, making it a particular priority to protect health workers in countries with weaker health systems than others. Additionally, strong public health institutions are essential for sharing information, disseminating good practices among health professionals, and facilitating better adaptation and communication with the public [10].
In addition, in the fight against the spread of the virus, vulnerable health services were reluctant to conduct critical screenings and monitor disease progression, thereby promoting transmission and suppressing the number of reported cases. In general, the concentration of COVID-19 cases appeared to be highest in the Casablanca-Settat region, according to maps created using GIS. Depending on the documented COVID-19 cases, the regions were ranked as follows: Casablanca-Settat> Rabat-Sale-Kenitra> Marrakech-Safi > Fes-Meknes > Tangier-Tetouan-Alhouceima>Oriental>Souss-Massa > Beni Mellal-Khenifra> Draa-Tafilalet> Laayoune-Sakia El Hamra >Guelmim-Oued Noun > Dakhla-Oued Eddahab. The increase in cases in major cities was due to several factors, including demographic, social and environmental factors. This demonstrates the need to consider demographic contributions to environmental health. Demographic factors help us understand the health of our environment empirically.
Geography improves health decision-making and accountability. Incorporating the geographic context of the spread of COVID-19 helps decision-makers understand the impact of location on strategies and goals to combat this pandemic [11]. Health geography identifies risk factors associated with the spatial distribution of health problems (using mapping and spatial analysis). GIS has become an essential tool for health services as it connects geographic concepts to the many dimensions of disease programming [12]. Spatial analysis techniques aim to determine the characteristics of the spatial distribution of individuals in a geographic area. When analyzing data on the regional distribution of the number of COVID-19 cases (geographical persons), GIS was implemented to depict and create risk maps showing the spread of COVID-19 and different risk areas: high-risk areas, medium-risk areas, and low-risk areas.
GIS can be used to understand the geographic distribution of diseases and perform disease prevalence analysis and spatial classification. GIS supports digital map visualization and spatial analysis, enabling epidemic localization and facilitating spatio-temporal epidemiological planning, analysis, and assessment [13]. Through map analysis and the use of spatial models, the effectiveness of spatial analysis in analyzing COVID-19 spread factors at the level of 12 regions in Morocco was demonstrated. We chose the 12 regions of Morocco as our analytical framework due to the lack of empirical studies focusing on the contribution of spatial dimensions in studying health-related phenomena. GIS helps identify potential risk factors for developing COVID-19. The majority of COVID-19 cases were associated with population density and certain environmental covariates [13]. The strength of this paper is that it provides a spatial analysis to measure the extent of the spread of the coronavirus in Morocco and makes suggestions to help improve the epidemiological situation in Morocco. It helps us improve the quality of our service, which can greatly enhance the quality and efficiency of health research [14].
Despite Morocco's policies against COVID-19 at all levels and the lack of statistical data that would help researchers get a clear picture of the issues relevant to society, COVID-19 has resulted from many previous mistakes and concealments, uncovering imbalances [15]. A large proportion of the Moroccan population has health insurance. The situation is exacerbated by the failure of healthcare systems in most areas, which suffer mainly from staff shortages. This requires the intervention of state and private actors to develop health system services and democratize social protection. In this sense, research has shown that employing large numbers of skilled health workers was more likely to cope with the challenges of COVID-19 [9]. Recommendations in this article include enhancing geographic information systems and spatial analysis tools to identify prevalence points of risk affecting human health. COVID-19 influences urban planning in terms of adequacy and quality of services, the extent of urban sprawl, and population migration in order for Moroccan cities to achieve safety standards that contribute to urban disaster management. It shows that the standards need to be reconsidered. In addition, the daily publication of the latest map of the pandemic in the media had encouraged residents, who began to understand their negative role in the spread of the disease, to take more responsibility and help by complying with applicable laws, actively participating in limiting the spread. It is important to introduce infection simulation techniques that can generate effective distributions of the spread of infection and evaluate algorithms for detecting it [16].
In this sense, several perspectives have been proposed to prevent the spread of COVID-19 and avoid its complications:
- Explain the importance of compliance with preventive health measures;
- Organize continuous training for the staff in terms of cognitive needs regarding the novelties of the national plan for the fight against COVID-19;
- Accelerate the national operation of vaccination against COVID-19;
- Encourage epidemiological and biotechnological research to develop and manufacture vaccines at the local level;
- Institute geospatial applications in the study of the distribution of COVID-19 in Morocco.
CONCLUSION
The study has identified regions with clusters and hotspots of both high and low levels of COVID-19. The produced maps can serve as excellent management tools to control and effectively eliminate the COVID-19 pandemic and contribute to investments in epidemiological surveillance programs. However, current research remains inadequate due to a lack of literature on this subject. The use of GIS in epidemiology, particularly in the spatial analysis of COVID-19, has made it possible to successfully visualize the geography of this pandemic. This visualization will help us better manage the epidemiological situation in Morocco. Nevertheless, to analyze epidemic spatial heterogeneity, other methods, such as spatial autocorrelation, should be integrated.
LIST OF ABBREVIATIONS
| GIS | = Geographic Information System |
| COVID-19 | = Coronavirus Disease 2019 |
| WHO | = World Health Organization |
| SARS-COV-2 | = Severe Acute Respiratory Syndrome Coronavirus 2 |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No humans or animals were used for the studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analysed during this study are available from the corresponding author [D.H] on request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
I would like to thank my thesis supervisor, Professor Bouaiti el Arbi, for the trust and supervision of this work.

