All published articles of this journal are available on ScienceDirect.

Anxiety over the Spread of COVID-19 and its related Factors among Older Adults in Bangkok
Abstract
Background:
Older adults are the population most at risk of death from the outbreak of COVID-19. Promotion of health literacy and COVID-19 prevention behavior among older adults is needed to lessen their anxiety.
Objective:
To analyze the relationships among age, health literacy, health behavior, and anxiety over the spread of COVID-19 among older adults in Bangkok.
Methods:
The participants were 480 male and female Thai older adults aged 60 and over who lived in Bangkok as listed in the household registration. A multi-stage sampling was used to select the participants. The research tools were interview forms covering data about personal information, health literacy, and health behavior. The research period was from September to November 2022. The data were analyzed using descriptive statistics, Pearson’s correlation coefficient, and multiple regression analysis through an SPSS (version 24)
Results:
Older adults in Bangkok had a high level of anxiety over the spread of COVID-19 ( = 16.02, SD = 5.22). Health literacy (r =−0.220) and health behavior (r =−0.390) were associated with the anxiety of older adults at a statistical significance level of 0.05 and could significantly predict 16.5% of older adults’ anxiety.
= 16.02, SD = 5.22). Health literacy (r =−0.220) and health behavior (r =−0.390) were associated with the anxiety of older adults at a statistical significance level of 0.05 and could significantly predict 16.5% of older adults’ anxiety.
Conclusion:
A holistic system or approach should be established to promote older adults’ access to health services and enhance their health literacy in preventing COVID-19. This will make them have appropriate health behavior, be able to prevent the disease continuously, and have less anxiety during the COVID-19 outbreak.
1. INTRODUCTION
1.1. BACKGROUND AND SIGNIFICANCE OF THE PROBLEM
The COVID-19 pandemic has caused a large number of deaths and has affected people around the world. The spread of COVID-19 began at the end of 2019 and has lasted til now. All countries suffer from this pandemic, which has killed millions of people worldwide [1]. In Thailand, the outbreak of COVID-19 began in December 2020. Two years later, the spread and severity of the disease tended to decrease. On October 1, 2022, the Ministry of Public Health announced the downgrading of COVID-19 from a dangerous infectious disease to a communicable disease under surveillance according to Communicable Diseases Act B.E. 2558 (2015) [2]. However, COVID-19 appears to be seasonal. Although the number of infected patients in Thailand has steadily declined, more deaths have been reported among older adults [3]. This is consistent with the World Health Organization’s report on the infection rate and severity of COVID-19, which indicates that older adults are at risk of severe infection and death. The risk increases with age and comorbidities, such as coronary heart disease, diabetes, hypertension, and chronic respiratory disease. The mortality rate was 7.6-13.2%. in February 2020. [3]
Old age is a period of physical, mental, and social changes. Due to increasing age, various organs in the body deteriorate, leading to low immunity and poor physical performance. As a result, older adults are more prone to getting sick than people in other age groups. This is probably one of the factors that puts older adults at high risk of catching COVID-19, severe infection, and death. According to a survey on the impact of the COVID-19 pandemic, In July 2020, 20% of older adults in Thailand had worse health. In China and Italy, it was found that deaths from COVID-19 were correlated with increasing age, and elderly patients aged 70-79 years had a mortality rate of 8.0%. In Thailand, elderly patients aged 70 and over had a mortality rate of 12.7% in February 2020, while elderly patients aged 60-69 years had a mortality rate of 5.0% [3]. This evidence emphasizes that older adults are in danger of serious infection and death from COVID-19. In Turkey, 95% of older adults have died from COVID-19, and most of them were found to have at least one underlying disease, such as diabetes, heart disease, vascular disease, or hypertension. [3] In addition to physical impacts, the spread of COVID-19 also affects the mental conditions of both infected and uninfected older adults. In other words, older adults are physically vulnerable with comorbidities and low immunity, and their mental health is easily affected by stress and anxiety [3].
Moreover, it was found that European older adults had the highest anxiety over COVID-19 (54.6%), followed by American older adults (31.5%) and Asian older adults (28.3%) [4]. Female older adults were found to have higher anxiety than male older adults at a statistical significance level of 0.05 [4]. This is in line with the survey results about the impact of the COVID-19 pandemic from United Nations Population Fund [UNFPA] Thailand and the College of Population Studies at Chulalongkorn University, which show that 1 in 4 older people had at least one mental health problem during the COVID-19 pandemic. Most of them were found to experience anxiety (57.2%), loss of appetite (47.3%), loneliness (25%), and unhappy feelings (23.3%). In terms of anxiety, older adults were most anxious about the finances of their families and themselves, followed by COVID-19 infection and deteriorating health [3].
Anxiety is a mental health problem commonly found in older adults. Emotional and physical reactions in response to anxiety may lead to a loss of ability to function, sleep disturbances, defenselessness, and hopelessness, affecting older adults’ daily life activities. Older adults with a disease are more likely to be anxious, making them have problems with thinking, memory, and problem-solving skills. Normally, when people face a crisis, four emotions arise: fear, anxiety, sadness, and anger [5]. The physical impacts of the COVID-19 pandemic on older adults include fatigue, muscle tension, insomnia, and irritation, while the mental impacts are social isolation, loneliness, stress, anxiety, and concern about their family members’ economic problems that may finally affect their well-being. The mental state of older adults is affected in terms of loneliness, stress, and anxiety, which may result in depression and a poor quality of life [6].
According to a literature review, anxiety in older adults is concerned with several factors [7, 8-11]. Age is associated with severe infection and mortality [7, 8]. Increasing age is correlated with increasing anxiety. If anxiety remains chronic, it can lead to depression. As COVID-19 is an emerging disease, there is both reliable and unreliable information “floating around” about this disease and its prevention, which may cause older adults to receive false information. Health literacy is essential for reducing the spread of COVID-19 and preventing infection. According to the World Health Organization (1998), “Health literacy refers to the cognitive and social skills that define a person’s motivation and ability to acquire, comprehend, and make use of information in ways that support and preserve good health” [9, 10]. If people can understand and effectively use information, it will contribute to good health behavior and reduce infection severity. Yang BX et al. (2020) [11] found that health literacy was negatively associated with psychological health during the COVID-19 pandemic. Health literacy helped older adults afraid of COVID-19 develop health behavior that could promote physical and psychological health and lessen infection risks. Good health behaviors are critical for minimizing stress and anxiety in older adults. Hara et al. (2021) also indicated that health behaviors were statistically significantly correlated with anxiety (p<0.01) [8].
Based on the literature review, most previous descriptive studies have focused on the association between older adults’ health literacy and COVID-19 prevention practices. In comparison, there has been no research investigating the anxiety of older adults during the COVID-19 pandemic. Thus, this research examines the relationships among age, health literacy, health behavior, and anxiety over the spread of COVID-19 among older adults in Bangkok. Older adults are considered a vulnerable group with the highest mortality rate and are at risk of severe infection and death, causing them to feel more anxious about the COVID-19 pandemic than people in other age groups. The findings of this study will be useful for developing a holistic healthcare system to support older adults’ quality of life and well-being in the long run.
1.2. Research Objectives
1. To investigate the anxiety over the spread of COVID-19, health literacy, and health behavior of older adults in Bangkok
2. To analyze the relationships among age, health literacy, health behavior, and anxiety over the spread of COVID-19 among older adults in Bangkok
1.3. Conceptual Framework
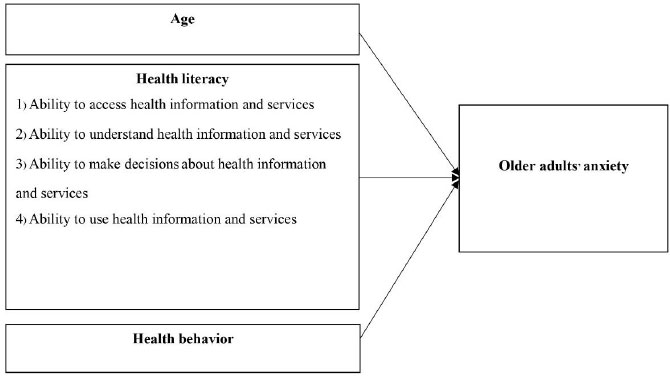
This study applied the anxiety concept of Spielberger (1972) [5], which states that anxiety arises from individuals’ assumptions and appraisals of a stimulus that may cause harm or dissatisfaction. The assumptions and appraisals of each individual vary depending on their perceptions and thinking processes. If they feel threatened or dissatisfied, they will react or behave in response to that stimulus. Anxiety is an emotional state of uneasiness caused by the appraisal of situations over a specific period of time. When individuals’ thinking processes are aroused and feel threatened by that arousal, they will develop anxiety. Ladder and Mark [12] developed a model to describe the anxiety that occurs in everyday life based on Spielberger’s anxiety theory, aiming to demonstrate the causes of anxiety and the mechanisms of brain perceptions, reactions, and anxiety-reducing behaviors when individuals perceive or appraise a stimulus that arouses them. Individuals who perceive a stimulus as threatening will show three reactions: 1) they will exhibit physiological changes, such as rapid heartbeats and excessive sweating, stimulated by the central nervous system; 2) they will feel anxious facing that situation; and 3) they will use coping mechanisms to reduce their anxiety and eliminate the cause of anxiety [13]. These three reactions are correlated. When physiological changes are perceived, individuals will assess their anxiety and find ways to minimize it as follows: 1) change the environment that causes the anxiety; 2) learn to react appropriately; 3) re-evaluate the stimulus; and 4) learn how to directly decrease anxiety in order to reduce central nervous system stimulation and physiological changes.
The factors associated with older adults’ anxiety included in the present study are age, health literacy, and health behavior, as seen in the conceptual framework in Fig. (1).
2. MATERIALS AND METHODS
This research applied a descriptive cross-sectional study design to examine the relationships among age, health literacy, health behavior, and COVID-19 anxiety among older adults in Bangkok.
2.1. Population and Sampling
The target population was male and female older adults aged 60 and over who have Thai nationality and live in Bangkok as listed in their household registration. The participants were selected according to the following inclusion criteria: 1) having a normal orientation regarding date, time, and location; 2) being able to communicate in Thai; and 3) giving written consent to participate in this research. The exclusion criteria included: 1) being unable to help themselves, handicapped, or disabled; 2) having complications from chronic illness or being unable to take care of themselves; 3) being diagnosed with depression or psychiatric disorders; and 4) being absent on the data collection date.
From a total of 1,020,917 older adults in Bangkok [14], the Taro Yamane formula [15] was used to calculate the sample size and the allowable sampling error was set at 0.05. Finally, the sample size of 400 was determined. In order to prevent data loss and errors, an additional 20% of the sample size was added to the study. As a result, the study had a total of 480 participants. The multi-stage random sampling technique was used to select the participants through sampling with replacement. The name of each participant was randomly picked according to the list of each community until the required sample size was reached.
3. RESEARCH TOOLS
The research tools were interview forms consisting of the following four parts:
Part 1 covered 1-9 questions about the personal information of the participants, including age, gender, marital status, education, residence, occupations, underlying diseases, family members infected with COVID-19, and income sufficiency.
Part 2 was the health literacy assessment form of the Health Education Division (2021) [13], which comprised 16 questions regarding four main abilities: 1) ability to access health information and services; 2) ability to understand health information and services; 3) ability to make decisions about health information and services; and 4) ability to use health information and services. All of the questions were positive. This part was measured using a 5-point rating scale, ranging from poor to very good. A total score can be lower than the range of 48-80. The results were interpreted according to the interpretation criteria of the Health Education Division (2021) [13]. Total scores are divided into four levels: 1) poor (48 and lower); 2) fair (48-55); 3) good (56-63); and 4) very good (64-80).
Part 3 was the health behavior assessment form of the Health Education Division (2021) [13], which consisted of 22 questions. The health behavior assessment form can be divided into two parts: 1) non-infectious disease prevention behavior such as food consumption, exercise, stress management, smoking, and alcohol use, and 2) COVID-19 prevention behavior. A 5-point rating scale, ranging from poor to very good, was applied to measure this part. Total scores can fall below the range of 66-110. The interpretation criteria of the Health Education Division (2021) [13] were used to interpret the results. Total scores are categorized into four levels: 1) poor (66 and lower); 2) fair (66-76); 3) good (77-78); and 4) very good (88-110).
Part 4 was the Thai geriatric anxiety scale (Thai GAS-10). Segal et al. (2010) developed the original geriatric anxiety scale with 25 questions. Later, Mueller et al. (2015) [16] created a shorter scale with only 10 questions called the GAS-10 [16]. ) Then Sutthida Phongphanngam et al. (2021) [17] translated the GAS-10 into Thai. The Thai GAS-10 is a 4-point rating scale. All questions on this scale are positive. The results are divided into four levels: 1) minimal anxiety (1-6); 2) mild anxiety (7-9); 3) moderate anxiety (10-11); and 4) severe anxiety (12-30).
3.1. Validity and Reliability of the Research Tools
This study used research tools that were published in previous research and that were proven to meet acceptable standards without additional modifications. Therefore, the researchers did not examine the validity of the content. However, the reliability of the research tools was tested by trying out the health literacy assessment form, the health behavior assessment form, and the Thai GAS-10 with 30 older adults in Lat Phrao, Bangkok, who had similar characteristics to the sample group of this study. The reliability was confirmed with Cronbach’s alpha coefficients of .85, .90, and .91, respectively.
3.2. Human Subject Protection
This research received ethical approval from the Human Research Ethics Committee of Chulabhorn Research Institute (Certificate No. 182/2564). The research objectives, the benefits of the study, the risks that might occur, and the data collection procedures were clarified to all participants. The participants were also informed about their rights to decide whether to participate in this project, data confidentiality, and the destruction of data records after research completion. The research data were presented in an overall manner for educational purposes only. The participants willing to participate in this study were asked to sign a consent form.
3.3. Data Collection
The researchers collected data by interviewing older adults in the selected communities according to the following procedures:
1. The researchers visited the leaders of the selected communities to introduce themselves, clarify the research details, and ask for cooperation regarding the data collection. One or two public health volunteers were asked to bring the researchers to meet the older adults who were randomly selected.
2. The researchers met the participants, introduced themselves, explained the details of the research project, and asked for the participants’ cooperation. During an interview, the researchers read every question on the interview form to the participants and then recorded their answers in the form. The duration of the interview was about 40-60 minutes per case. The researchers continually collected data from the participants one by one until they reached the required number of 480.
3.4. Data Analysis
The data were analyzed using descriptive statistics, Pearson’s product-moment correlation coefficient, and multiple regression analysis with stepwise regression. The level of statistical significance was set at .05. The assumptions of multiple regression analysis were tested. The results indicated that the noise variance was constant (homoscedasticity), and the independent variables did not correlate (multicollinearity). The Kolmogorov-Smirnov test results showed normal data distribution. The Durbin-Watson value was 1.9, indicating no autocorrelation.
4. RESULTS
The results of this research are described below.
4.1. The Personal Information of the Participants
Most of the participants were early older people aged 60-69 (58.3%), followed by middle-aged people aged 70-79 (31.9%), and late older people aged 80 and over (9.8%). Most were female (69.2%), and their education was at the elementary school level (52.5%). Most were married (44.6%), and most had an underlying disease (78.8%). They mostly had at least two comorbidities, such as diabetes, hypertension, and hyperlipidemia (31.7%), followed by at least one comorbidity, including hypertension (23.1%), diabetes (7.9%), hyperlipidemia (4.8%), and chronic kidney disease (1.7%). Most participants lived with their children (31%), followed by their spouses (28.1). Most of their family members were not infected with COVID-19 (58.8%). Most were jobless (70.4%) and had insufficient income (65%).
4.2. The Participants’ Health Literacy, Health Behavior, and Anxiety
The results showed that the overall health literacy of the participants was at a good level ( = 58.12, SD = 10.98), and their overall health behavior was at a very good level (
= 58.12, SD = 10.98), and their overall health behavior was at a very good level ( = 88.64, SD = 9.10). In terms of non-infectious disease prevention behavior, the participants had a fair level of exercise (
= 88.64, SD = 9.10). In terms of non-infectious disease prevention behavior, the participants had a fair level of exercise ( = 6.38, SD = 2.34), a good level of food consumption (
= 6.38, SD = 2.34), a good level of food consumption ( = 22.32, SD = 4.27) and stress management (
= 22.32, SD = 4.27) and stress management ( = 7.58, SD = 2.15), and a very good level of smoking (
= 7.58, SD = 2.15), and a very good level of smoking ( = 9.12, SD = 1.76) and alcohol use (
= 9.12, SD = 1.76) and alcohol use ( = 4.77, SD = .73). Their COVID-19 prevention behavior was at a poor level (
= 4.77, SD = .73). Their COVID-19 prevention behavior was at a poor level ( = 21.96, SD = 3.17). Most of them were found to have severe anxiety (
= 21.96, SD = 3.17). Most of them were found to have severe anxiety ( = 16.02, SD= 5.22). Additional details are shown in Table 1.
= 16.02, SD= 5.22). Additional details are shown in Table 1.
When considering each aspect of health literacy, it was found that the participants had a high level of ability to access health information and services ( = 14.21, SD = 3.39),ability to understand health information and services (
= 14.21, SD = 3.39),ability to understand health information and services ( = 14.79, SD = 2.99), ability to make decisions about health information and services (
= 14.79, SD = 2.99), ability to make decisions about health information and services ( = 14.11, SD = 3.49), and ability to use health information and services (
= 14.11, SD = 3.49), and ability to use health information and services ( = 15.01, SD = 2.94), as detailed in Table 2.
= 15.01, SD = 2.94), as detailed in Table 2.
4.3. The Relationships between Anxiety and its related Factors
According to Pearson’s product-moment correlation coefficients, health literacy and health behavior had a low negative relationship with anxiety (r = −.220 and −.390, respectively) at a statistical significance level of .05. It was found that the participants’ age had no relationship with their anxiety at a statistical significance level of .05. The details are presented in Table 3.
4.4. Factors Predicting Older Adults’ Anxiety
The results of multiple regression analysis with stepwise regression showed that health literacy and health behavior could significantly predict 16.5 percent of anxiety (R2 = .165, p <.001). Health behavior had the highest predictive power (Beta =-.356, p <.001), followed by health literacy (Beta =-.120, p <.01). Additional details are provided in Table 4.
| Factor |  |
SD | Level |
|---|---|---|---|
| Health literacy | 58.12 | 10.98 | Good |
| Health behavior | 88.64 | 9.10 | Very good |
| Anxiety | 16.02 | 5.22 | Severe |
| Health Literacy |
Very Good (%) |
Good (%) |
Fair (%) |
Poor (%) |
|
SD |
|---|---|---|---|---|---|---|
| 1) Ability to access health information and services | 53.3 | 11.0 | 18.8 | 16.9 | 14.21 | 3.39 |
| 2) Ability to understand health information and services | 57.7 | 17.9 | 12.5 | 11.9 | 14.79 | 2.99 |
| 3) Ability to make decisions about health information and services | 55.4 | 11.7 | 15.6 | 17.3 | 14.11 | 3.48 |
| 4) Ability to use health information and services | 66.9 | 10.4 | 11.0 | 11.7 | 15.01 | 2.94 |
| Factors | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Age | 1 | - | - | - |
| 2. Health literacy | -.104* (.023) | 1 | - | - |
| 3. Health behavior | -.075 (.100) | .282** (.000) | 1 | - |
| 4. Anxiety | .068 (.135) | -.220** (.000) | -.390** (.000) | 1 |
| Factors | R2 | b | SE | Beta | t | p-value |
|---|---|---|---|---|---|---|
| Health literacy | 152 | -.223 | 0.24 | -.356 | -8.168 | .000 |
| Health behavior | .165 | -.057 | .021 | -.120 | -2.741 | .006 |
| Constant (a) | - | 37.424 | 2.214 | - | 16.655 | .000 |
4. DISCUSSION
The results concerning the anxiety of older adults in Bangkok are discussed as follows. According to the research results, the participants had a high level of anxiety over the spread of COVID-19 ( = 16.02, SD = 5.22). The study participants were older adults living in an urban area of Bangkok, and most of them had an underlying disease (78.8%). They mostly lived with their children (31%), followed by their spouses (28.1%), and their family members were not infected with COVID-19 (58.8%). They were mostly jobless (70.4%) and had insufficient income (65%). They were also a vulnerable group with comorbidities and low immunity [18], so they were at risk of COVID-19 infection. Based on the interview results, the participants were anxious and afraid of contracting COVID-19 even after taking the vaccine. They had poor physical health due to increasing age and underlying diseases; they feared that if they caught COVID-19, they would die extremely ill [19, 20]. This is congruent with the anxiety concept of Spielberger (1972) [5], which states that emotional and physical anxiety-related reactions can result in a lack of capacity to perform, sleep difficulties, defenselessness, and hopelessness. Each person has a different level of anxiety depending on how they perceive things and think. Anxiety is an unpleasant emotional state resulting from evaluating different situations over time. Anxiety can arise when a person’s thinking process is stimulated and he or she assesses that the stimulus is threatening. Although the surge of COVID-19 continues to decrease, older adults are still fearful and worried that their family members or themselves may be infected and suffer from deteriorating health. This is consistent with the Foundation of Thai Gerontology Research and Development Institute’s report [2], which specifies that older adults with low income have less access to digital technology and information (12.9%). Older adults must adapt to changes by adopting a new way of living, such as using modern technology or paying for goods using mobile banking applications instead of cash, in order to reduce exposure to the environment that may promote the spread of COVID-19. It was found that 83.6 percent of older adults do not use mobile banking applications to pay for goods-their utilization of modern technology is the lowest compared to other age groups. Older adults mostly receive information from television (78.6%), followed by close intimates (44.6%) and community leaders or volunteers (38.5%). They are also worried about how the financial difficulties of their relatives may ultimately affect their well-being. These factors influence the mental health conditions of older adults, such as loneliness, stress, and anxiety, leading to depression. The findings of the present study indicated that the participants’ overall health literacy was at a good level (
= 16.02, SD = 5.22). The study participants were older adults living in an urban area of Bangkok, and most of them had an underlying disease (78.8%). They mostly lived with their children (31%), followed by their spouses (28.1%), and their family members were not infected with COVID-19 (58.8%). They were mostly jobless (70.4%) and had insufficient income (65%). They were also a vulnerable group with comorbidities and low immunity [18], so they were at risk of COVID-19 infection. Based on the interview results, the participants were anxious and afraid of contracting COVID-19 even after taking the vaccine. They had poor physical health due to increasing age and underlying diseases; they feared that if they caught COVID-19, they would die extremely ill [19, 20]. This is congruent with the anxiety concept of Spielberger (1972) [5], which states that emotional and physical anxiety-related reactions can result in a lack of capacity to perform, sleep difficulties, defenselessness, and hopelessness. Each person has a different level of anxiety depending on how they perceive things and think. Anxiety is an unpleasant emotional state resulting from evaluating different situations over time. Anxiety can arise when a person’s thinking process is stimulated and he or she assesses that the stimulus is threatening. Although the surge of COVID-19 continues to decrease, older adults are still fearful and worried that their family members or themselves may be infected and suffer from deteriorating health. This is consistent with the Foundation of Thai Gerontology Research and Development Institute’s report [2], which specifies that older adults with low income have less access to digital technology and information (12.9%). Older adults must adapt to changes by adopting a new way of living, such as using modern technology or paying for goods using mobile banking applications instead of cash, in order to reduce exposure to the environment that may promote the spread of COVID-19. It was found that 83.6 percent of older adults do not use mobile banking applications to pay for goods-their utilization of modern technology is the lowest compared to other age groups. Older adults mostly receive information from television (78.6%), followed by close intimates (44.6%) and community leaders or volunteers (38.5%). They are also worried about how the financial difficulties of their relatives may ultimately affect their well-being. These factors influence the mental health conditions of older adults, such as loneliness, stress, and anxiety, leading to depression. The findings of the present study indicated that the participants’ overall health literacy was at a good level ( = 58.12, SD = 10.98). Since COVID-19 is an emerging disease, older adults may receive incorrect information about this disease and its prevention due to a lot of true and false information being communicated in society. Hence, health literacy is vital to preventing infection and decreasing the spread of COVID-19. The participants’ overall health behavior was at a very good level (
= 58.12, SD = 10.98). Since COVID-19 is an emerging disease, older adults may receive incorrect information about this disease and its prevention due to a lot of true and false information being communicated in society. Hence, health literacy is vital to preventing infection and decreasing the spread of COVID-19. The participants’ overall health behavior was at a very good level ( = 88.64, SD = 9.10). Considering their non-infectious disease prevention behavior, they had a fair level of exercise (
= 88.64, SD = 9.10). Considering their non-infectious disease prevention behavior, they had a fair level of exercise ( = 6.38, SD = 2.34), a good level of food consumption (
= 6.38, SD = 2.34), a good level of food consumption ( = 22.32, SD = 4.27) and stress management (
= 22.32, SD = 4.27) and stress management ( = 7.58, SD = 2.15), and a very good level of smoking (
= 7.58, SD = 2.15), and a very good level of smoking ( = 9.12, SD = 1.76) and alcohol use (
= 9.12, SD = 1.76) and alcohol use ( = 4.77, SD = .73). However, they were found to have a poor level of COVID-19 prevention behavior (
= 4.77, SD = .73). However, they were found to have a poor level of COVID-19 prevention behavior ( = 21.96, SD = 3.17). Although the participants had good overall health behavior, their COVID-19 prevention behavior was poor, and a poor level of COVID-19 prevention behavior can lead to serious infection and death. Thus, promoting good health behavior among older adults is critical to prevent COVID-19 infection. Older adults should be supported to develop appropriate health behavior, contributing to good mental and physical health and COVID-19 risk reduction. Appropriate health behavior helps to reduce older adults’ stress and anxiety. Stress is a common occurrence caused by the fear of unpredictable incidents. Performing normal daily activities while adhering to COVID-19 prevention measures learned from reliable sources [3] and regularly communicating with family and friends will reduce anxiety.
= 21.96, SD = 3.17). Although the participants had good overall health behavior, their COVID-19 prevention behavior was poor, and a poor level of COVID-19 prevention behavior can lead to serious infection and death. Thus, promoting good health behavior among older adults is critical to prevent COVID-19 infection. Older adults should be supported to develop appropriate health behavior, contributing to good mental and physical health and COVID-19 risk reduction. Appropriate health behavior helps to reduce older adults’ stress and anxiety. Stress is a common occurrence caused by the fear of unpredictable incidents. Performing normal daily activities while adhering to COVID-19 prevention measures learned from reliable sources [3] and regularly communicating with family and friends will reduce anxiety.
Health literacy and health behavior could significantly predict 16.5% of the anxiety of older adults in Bangkok. (p <.05). This finding can be discussed as follows.-Health literacy could statistically significantly predict anxiety (p <.05); it was a predictive factor that had a negative relationship with anxiety. This implies that health literacy is crucial for limiting COVID-19 transmission and preventing infection. The World Health Organization states that health literacy is the set of cognitive and social skills defining a person’s motivation and ability to acquire, comprehend, and use information to support and preserve good health [9, 10]. People who can comprehend and use information effectively will have good health behavior and are less likely to face serious infections and illnesses. This is in line with Yang BX et al. (2020) [21], who revealed that during the COVID-19 pandemic, health literacy was inversely related to psychological health; an increase in health literacy will help to reduce anxiety, induce sleep, and promote good mental health [22].
Similarly, Yang BX et al. (2021) [21] stated that health literacy was negatively associated with the psychological status of Chinese residents. It was found that Chinese residents experienced depression (11.4%), insomnia (6.8%), and stress disorder (20.1%). Health literacy may improve sleep quality, mental health, and psychological well-being. Mohammadkhah et al. (2021) [23] also found that health literacy was associated with anxiety over COVID-19.
Health behavior could predict anxiety (p <.05) at a statistical significance; it was a predictive factor with a negative relationship with anxiety. This shows that health behavior is important for reducing COVID-19 infection, minimizing COVID-19 risk, and improving mental and physical health among older adults. Good health behavior can reduce older adults’ stress and anxiety. Older adults should only receive information from credible sources and consume news sparingly. As stress is a typical reaction to the uncertainty of life’s circumstances, when feeling stressed or anxious, people should constantly communicate with their close family members and friends to lessen their stress and anxiety. Maintaining a daily routine while following COVID-19 preventative strategies learned from reliable sources [3] will help reduce anxiety. According to Hara et al. (2021) [8], health behaviors were significantly associated with anxiety (p <.001).Further, Chayanit Luevanich et al. (2020) [24] found that the participants with a good level of health literacy had a very good level of new normal behavior; communication skills for COVID-19 prevention and media and information literacy could explain 52.2% of the participants’ new normal behavior.
Age could not predict the anxiety of older adults in Bangkok, contradicting the determined hypothesis. This was probably because the older adults were mostly jobless, did not go out to socialize with others, and had no family members infected with COVID-19. Moreover, most of the older adults were vaccinated while the outbreak of COVID-19 has continually decreased, lowering the severity of COVID-19 infection and death.
CONCLUSION
A holistic system or approach should be established to promote older adults’ access to health services and enhance their health literacy in preventing COVID-19. This will make them have appropriate health behavior, be able to prevent the disease continuously, and have less anxiety during the COVID-19 outbreak.
LIMITATIONS OF THE STUDY
This research is a cross-sectional study that was conducted during the COVID-19 pandemic. During that period, most older adults were vaccinated against COVID-19, resulting in fewer cases of infection and death. This could probably affect the anxiety level of the older adults in this study.
IMPLICATIONS OF THE STUDY
1. The research findings can be used as basic information to develop new strategies for preventing mental health problems in older adults. The findings can also be used to create a holistic healthcare system or approach to support older adults during the outbreak of emerging diseases.
2. The research findings are beneficial for determining preventive guidelines for older adults to cope with anxiety and other mental health problems.
RECOMMENDATIONS FOR FUTURE RESEARCH
1. A mobile application should be developed to promote older adults’ health literacy and health behavior because, at present, most older adults can easily and conveniently access technology via mobile phones.
2. More qualitative studies should be conducted in order to gain useful insights for developing a holistic healthcare system that can enhance the quality of life and well-being of older adults in a sustainable way.
LIST OF ABBREVIATIONS
| COVID-19 | = COronaVIrus Disease of 2019 |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The researchers have applied for a research ethics review from Chulabhorn Research Institute, IRB Study code 182/2564.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants of this study.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available on request from the corresponding author [A.S].
FUNDING
This research project was funded by the Chulabhorn Royal Academy No. 182/2564
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise
ACKNOWLEDGEMENTS
The researchers would like to thank Associate Prof. Dr. Vilaivan Thongcharoen, Associate Dean of the Agrarajakumari College of Nursing, for her helpful advice and support throughout this study.

