All published articles of this journal are available on ScienceDirect.

Assessing Knowledge and First-Aid Practice Scores of Caregivers of Epilepsy Patients Before and After an Educational Programme in the Kingdom of Saudi Arabia
Authors Info & Affiliations
Abstract
Background
Although epilepsy is one of the most prevalent and severe neurologic disorders, our knowledge of its intricate pathophysiology and skills to manage are still limited. Recognising its early signs and symptoms are crucial skills for caregivers of epileptic patients to acquire. This study was aimed at assessing the effectiveness of an education programme on improvement in the caregivers’ knowledge of epilepsy and first-aid practices. The findings will assist caregivers of children with seizures who frequently experience fear and anxiety relative to their perceived confidence to manage seizures. Education to caregivers could improve their perceived level of self-efficacy.
Methods
A community-based, pre- and post-intervention survey was conducted at neurologic care clinics across Saudi Arabia. Data were collected using a pretested, semi-structured, interviewer-administered questionnaire. The educational intervention was aimed at disseminating information via a short talk and video demonstration of epilepsy-related first-aid good practices. Data were analysed using SPSS version 21.
Results
Pre-intervention survey of 586 caregivers revealed that nearly 60% had inadequate knowledge of epilepsy; this was reduced to 23.2% after education. Similarly, 84% of caregivers had inadequate knowledge of first-aid practices before the educational intervention, but this was reduced to 32.4% after that. Having resided in the Western regions was a negative predictor of good first-aid practice knowledge scores, both before and after education. A university degree or higher education was positive predictor of higher knowledge scores both before (T=-4.564; p<0.001) and after education (T=-2.775; p=0.025). The oldest caregivers (>50 years) exhibited a significantly lower mean first-aid practice knowledge score (F=7.771; p=0.001).
Conclusion
Caregivers’ general and first-aid practice knowledge were generally poor prior to but were both markedly improved after educational interventions. Targeted educational health promotion could bring awareness to those with lower levels of education and older caregivers living in particularly the Western regions of Saudi Arabia.
1. INTRODUCTION
Epilepsy is a neurological condition characterized by recurrent seizures. A seizure is a transient disturbance of cerebral function secondary to abnormal paroxysms in the brain, resulting in sudden and excessive disorderly discharge of the cerebral neurons. People with epilepsy have an increased risk of developing a variety of psychological problems, including depression, anxiety, and psychosis [1]. Most cases of epilepsy are idiopathic; however, some cases may result from brain injury, stroke, brain tumour, or drugs/alcohol abuse. In addition, some cases of epilepsy have been shown to arise from specific genetic mutations [2].
In contrast to seizures and epilepsy in adults, generalised tonic-clonic seizures in children may have various origins and a different natural history. Children may also be more sensitive to the effects of drugs. The doctor must consider the likelihood of future seizures as well as any potential repercussions when deciding whether or not to treat a child who has only had one or a few seizures. Signs and symptoms can range from mild to severe and vary depending on seizure type. Seizure signs and symptoms may include (a) temporary confusion; (b) staring spells; (c) uncontrollable jerking movements of the arms and legs; (d) loss of consciousness or awareness; and (e) cognitive or emotional symptoms such as fear, anxiety, or déjà vu [3].
The worldwide prevalence of epilepsy in children has been reported to be 6.38 per 1,000 persons [4], while in the Kingdom of Saudi Arabia, the prevalence has been reported to be 6.54 per 1,000 persons [5]. A recent study in the Qassim region of Saudi Arabia indicated that public knowledge about epilepsy is insufficient [6, 7]. In Riyadh, it has been reported that both the general public and schoolteachers require improvement in epilepsy-related knowledge [8, 9]. Another study conducted among schoolteachers showed that their knowledge regarding both epilepsy and first aid is insufficient [10].
Although epilepsy is one of the most prevalent and severe neurologic disorders, our knowledge of its intricate pathophysiology and, consequently, the rationale for much of its therapy and management is still limited. Caregivers of children with epilepsy must have an adequate awareness of the disease in order to provide sufficient care. To the best of our knowledge, this study is the first to investigate caregivers' general knowledge and first-aid practice of epilepsy management and the effectiveness of education on those parameters in the Kingdom of Saudi Arabia.
2. METHODS
2.1. Study Design and Sampling
This community-based study used a pre- and post-interventional design to assess caregivers’ basic knowledge about epilepsy and their proficiency with first aid both before and after receiving educational intervention. Six neurology clinics across the Kingdom of Saudi Arabia were sampled.
2.2. Epilepsy Diagnosis
A diagnosis of epilepsy was made if the patients of the caregivers had recurrent seizures. Patients were usually diagnosed if (a) they had experienced at least two seizures, and (b) there was a period of at least 24 hours between the seizures, and (c) there was nothing to suggest that the seizures were singular events.
2.3. Sample Size Determination
The sample size used in this study was determined according to the formula n=NZ2P(1-P)/(D2+Z2P(1-P)), with significance adopted at P>0.05. According to the above equation, a sample of 586 respondents was selected.
2.4. Data Collection Tools
Data were collected using a pre-tested, semi-structured, interviewer-administered questionnaire. The first part of the questionnaire collected sociodemographic information about the participants, the second part assessed the participants’ knowledge, and the third part assessed first aid practices. After completing the pre-education questionnaire, a short talk was held for the caregivers to receive general knowledge and improve their awareness of epilepsy, as well as a video demonstration of epilepsy-related first aid good practices.
At the end of the day or the very next day after the educational sessions, the same questionnaire was readministered. The participants were blinded to the existence of the post-education questionnaire until just before it was administered.
2.5. Inclusion and Exclusion Criteria
Caregivers aged 21 and older and those who had been providing care for at least three months were included. Caregivers were excluded if they met any of the following criteria: (1) had mental disabilities or diseases, (2) had psychiatric illnesses, (3) refused to participate, (4) their patients were only recently diagnosed with epilepsy, (5) their patients had a reversible cause of epilepsy, (6) their data was missing or they decided to withdraw, (7) they were not involved in patient care.
2.6. Scoring
Knowledge related to epileptic seizures was measured using 7 questions, while first aid practices were measured using 9 questions. For each questionnaire item, participants were given a score of 1 if they knew the related information and a score of 0 if they did not know or were unsure. The score for each of these sections was calculated by adding the sum scores for all questions in the particular section. The knowledge score thus ranged from 0 to 7 points, while the first aid score ranged from 0 to 9 points. Higher scores indicate better knowledge and first-aid practices. We set 60% as the cut-off score to divide participants by level for both knowledge and first-aid practices. Thus, participants were considered to have a poor knowledge level if they received a knowledge score of 0 to 4 points and a good knowledge level if they received a score of 5 to 7 points. Similarly, for the first-aid questions, participants were considered to have poor first-aid practices if their scores ranged from 0 to 5 points and good first-aid practices if their scores ranged from 6 to 9 points. These cut-off values were used for both the pre-and post-education questionnaires.
2.7. Statistical Analysis
Descriptive statistics are presented using count, proportion (%), mean, and standard deviation as appropriate. Normality was assessed using the Shapiro-Wilk test. To compare pre- and post-education test results, the Mann-Whitney U test or the Kruskal Wallis test (non-parametric tests) were applied. A two-sided p-value of <0.05 was used to indicate statistical significance. Pearson’s correlation coefficients were calculated to determine the relationships between both knowledge and first-aid scores before and after education. When the population means of only two groups were compared, the t-test was used, but when means of more than two groups were compared, ANOVA was performed. All data analyses were performed using the Statistical Package for Social Sciences, version 21 (IBM Corp, Armonk, NY, USA).
2.8. Ethical Approval
Upon obtaining approval from the Regional Research Ethics Committee (RREC), access to the data of interest was available to the primary investigator. The participants’ names were erased from the required data list to assure the anonymity of the participants. The collected data were each assigned serial numbers to ease the identification of data. Secured devices protected with passwords were used for the storage of data and were only accessible to the dominant investigator only. This is for the purpose of establishing the data's confidentiality so that once it has been obtained, it will not be made publicly available to any unauthorized third parties.
The study was approved by the General Director of Health Affairs for the Al-Qassem Region under the number 29288-1441 on September 3, 2019. All respondents were informed about the aims of the study, the confidentiality of collected data and that they could withdraw from the study at any time and signed the informed consent. This research followed the principles outlined in the Declaration of Helsinki 1975.
3. RESULTS
We enrolled 586 caregivers from different regions of Saudi Arabia and administered questionnaires to assess their knowledge and first-aid practices. Table 1 presents the sociodemographic characteristics of the sample. The age range was 17 to 74 years (mean age, 38.7 years). Middle adults (31–40 years) were the most common age group (38.1%). More than half (52.4%) of the sample comprised males, and the most common region of residence was the southern region (39.1%). A majority of respondents reported achieving either a university degree (45.4%) or a high school (32.4%) level of education. As for employment status, 49.8% were employed, 44.9% were unemployed, and 5.3% were students.
| - | N (%) |
|---|---|
| Age Group | - |
| 17–30 years | 143 (24.4%) |
| 31–40 years | 223 (38.1%) |
| 41–50 years | 141 (24%) |
| >50 years | 79 (13.5%) |
| Gender | - |
| Male | 307 (52.4%) |
| Female | 279 (47.6%) |
| Region of residence | - |
| Central | 107 (18.3%) |
| Eastern | 143 (24.4%) |
| Western | 53 (9.0%) |
| Southern | 229 (39.1%) |
| Northern | 54 (9.2%) |
| Education level | - |
| None | 20 (3.4%) |
| Primary (Grade 1-3) | 51 (8.7%) |
| Intermediate (Grade 4-6) | 45 (7.7%) |
| High school | 190 (32.4%) |
| Higher education -degree | 266 (45.4%) |
| Higher education - postgraduate | 14 (2.4%) |
| Employment status | - |
| Employed | 292 (49.8%) |
| Unemployed | 263 (44.9%) |
| Student | 31 (5.3%) |
| - | N (%) |
|---|---|
| Relationship to Patient | - |
| Mother | 194 (33.1%) |
| Father | 116 (19.8%) |
| Other relatives | 276 (47.1%) |
| Pre-intervention knowledge about seizures | - |
| Yes | 250 (42.7%) |
| No | 336 (57.3%) |
| Prior knowledge about first aid | - |
| Yes | 233 (39.8%) |
| No | 353 (60.2%) |
Table 2 presents the relationship between caregivers and the patients and the caregivers’ pre-intervention knowledge about seizures and first aid practices. The proportion of caregivers who reported having knowledge about epilepsy and first aid was 42.7% and 39.8%, respectively. About one-third (33.1%) of the caregivers were mothers, and 24.4% reported that other persons who were close to the patient were taking care of the patient.
Fig. (1) depicts the information sources regarding seizures. It was found that the commonest source of information was the patient’s doctor (18.4%), followed by the internet (14.3%). Family and friends were the least common source of information (2.6%). Fig. (2) depicts the most frequently reported sources of information regarding first aid. The most commonly reported source of information was the patient’s doctor (21.8%), followed by the internet (9.6%) and courses attended (3.9%). As with the information about seizures, family and friends were the least commonly used source (1.9%).
Fig. (1) presents percentage of patients who reported using doctors, the internet, courses, family and friends, or others as their primary source of information about seizures.
Fig. (2) presents percentage of patients who reported using doctors, the internet, courses, family and friends, or other as their primary source of information about seizure-related first aid practices.
Table 3 shows the results of the knowledge assessment regarding epilepsy before and after education. The top 3 items where caregivers exemplified good understanding were; “Ictus: Sweating, blackouts, jerking movements, twitching, chewing or lip-smacking, unable to move, repeated blinking of eyes”, for which 85.5% of caregivers demonstrated pre-education knowledge and 96.4% of caregivers demonstrated post-education knowledge; “Treatment for epilepsy are anticonvulsants while surgery is indicated in some cases”, for which 73.9% of caregivers demonstrated pre-education knowledge and 85.8% of caregivers demonstrated post-education knowledge, and “CNS disorder”, for which 63.5% of caregivers demonstrated pre-education knowledge and 85.5% of caregivers demonstrated post-education knowledge. Overall, the t-value between pre and post-intervention was -2.94, with a statistically significant p-value of 0.006, indicating an improvement in knowledge following the educational intervention.
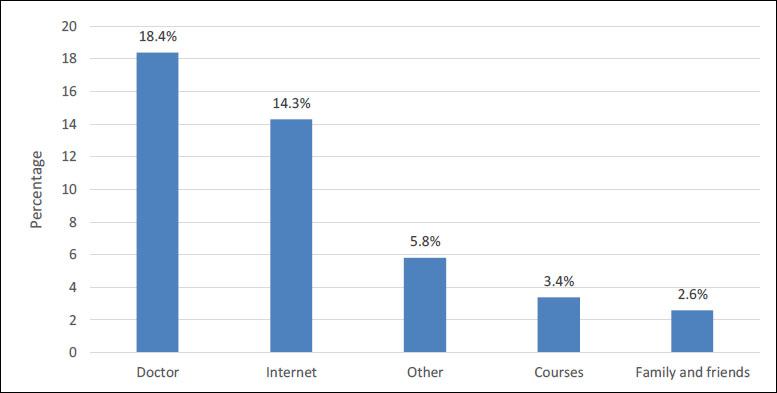
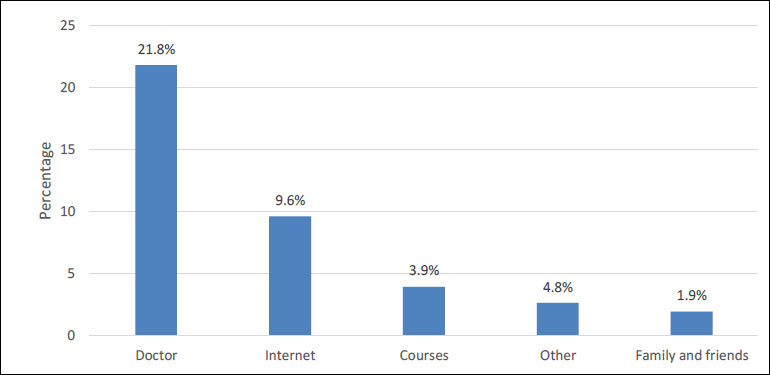
Table 4 shows the results of the questionnaire on first-aid practices both before and after caregiver education. Prior to education, caregivers showed the best first-aid practices for the items: “call 911 if needed” (57.8%), “stay with the patients until awake” (49.1%), and “stay with the patient and start timing the seizure” (42.2%). After education, caregivers showed improved first-aid practices for the items: “Turn the patient on his/her side” (90.4%), “Call 911 if needed” (87.5%), and “Keep the patient safe and remove or guide away from harmful objects” (83.3%). Overall, the t-value between pre and post-intervention is -4.4265, with a statistically significant p-value of 0.0002, indicating an improvement in first-aid practices following the educational intervention.
Table 5 shows the mean questionnaire scores and a summary of the levels of caregiver knowledge about seizures and seizure-related first-aid practices before and after education. For our sample, the mean knowledge score was 3.96 (SD 1.69) before education and 5.58 (SD 1.63) after education. Approximately 60% of caregivers demonstrated poor seizure-related knowledge prior to education, but this number was reduced to 23.2% after education. For the first-aid practices questionnaire, the mean score was 3.08 (SD 2.19) before education and 6.32 (SD 2.08) after education. Before education, a strong majority (84%) of caregivers exhibited poor knowledge of proper first-aid practices, but after education, this number was reduced to 32.4%.
| Statement | Information | |
|---|---|---|
|
Pre-education Yes (%) |
Post-education Yes (%) |
|
| 1. CNS disorders | 372 (63.5%) | 501 (85.5%) |
| 2. Chronicity | 224 (38.2%) | 394 (67.2%) |
| 3. Does the caregiver know the cause of the patient’s disease? | 266 (45.4%) | 419 (71.5%) |
| 4. Pre-ictal stage: Vision loss or blurring, hallucinations (strong feelings of joy, sadness, fear, or anger), dizziness, headaches, the patient may say he/she will have a seizure | 235 (40.1%) | 436 (74.4%) |
| 5. Ictus: Sweating, blackouts, jerking movements, twitching, chewing or lip-smacking, unable to move, repeated blinking of eyes | 501 (85.5%) | 565 (96.4%) |
| 6. Post-ictal stage: Sleepiness, memory loss, frightened, embarrassment, loss of control of bladder or bowels | 292 (49.8%) | 450 (76.8%) |
| 7. Treatment is anti-epileptic drugs (anticonvulsants); surgery is indicated in some cases | 433 (73.9%) | 503 (85.8%) |
| Statement | First-aid Practice | |
|---|---|---|
|
Pre-education Yes (%) |
Post-education Yes (%) |
|
| 1. Stay with the patient and start timing the seizure | 247 (42.2%) | 419 (71.5%) |
| 2. Keep the patient safe and remove or guide the patient away from harmful objects | 195 (33.3%) | 488 (83.3%) |
| 3. Turn the patient on his/her side | 243 (41.5%) | 530 (90.4%) |
| 4. Put something small and soft under his/her head | 162 (27.6%) | 453 (77.3%) |
| 5. Loosen tight clothing around the neck | 61 (10.4%) | 176 (30.0%) |
| 6. Do not put something in the patient’s mouth | 146 (24.9%) | 362 (61.8%) |
| 7. Do not restrain | 124 (21.2%) | 306 (52.2%) |
| 8. Stay with the patient until he/she awakens | 288 (49.1%) | 458 (78.2%) |
| 9. Call 911 if needed | 339 (57.8%) | 513 (87.5%) |
| - | Education | |
|---|---|---|
| Before | After | |
| Knowledge score (mean ± SD) | 3.96 ± 1.69 | 5.58 ± 1.63 |
| Knowledge level | - | - |
| Poor | 351 (59.9%) | 136 (23.2%) |
| Good | 235 (40.1%) | 450 (76.8%) |
| Practice score (mean ± SD) | 3.08 ± 2.19 | 6.32 ± 2.08 |
| First-aid practices | - | - |
| Poor | 492 (84.0%) | 190 (32.4%) |
| Good | 94 (16.0%) | 396 (67.6%) |
3.1. Analyses
When measuring the statistical differences between pre-and post-education epilepsy knowledge scores in relation to caregiver sociodemographic characteristics, female caregivers showed significantly higher knowledge scores before education (Table 6, T=-3.245; p=0.001), but this difference was not statistically significant after education (T=0.553; p=0.602). We also observed that caregivers with a university degree or higher education showed significantly higher knowledge scores both before (T=-4.564; p<0.001) and after education (T=-2.775; p=0.025).
Furthermore, before education, caregiver employment status was not significantly associated with knowledge scores (F=1.541; p=0.215); however, students exhibited significantly better knowledge scores after education (F=3.848; p=0.014). Similarly, previous knowledge about seizures (T=5.446; p<0.001) and previous knowledge about first aid (T=5.635; p<0.001) were associated with significantly higher pre-education knowledge scores, but these variables were no longer statistically associated with scores after education (both p>0.05). In contrast, the oldest age group (>50 years) exhibited a significantly lower mean knowledge score both before (F=2.762; p=0.042) and after (F=8.480; p<0.001) education. In addition, caregivers living in the western region of Saudi Arabia showed significantly lower knowledge scores both before (F=9.996; p<0.001) and after (F=29.505; p<0.001) education.
Table 7 shows the first-aid practice scores before and after education in relation to caregiver sociodemographic characteristics. We found that gender was not significantly associated with knowledge scores before education (T=-0.514; p=0.956) although females showed significantly higher scores after education (T=-1.670; p=0.037). Similar to the epilepsy knowledge questionnaire, caregivers living in the western region showed significantly lower first-aid practice scores both before (F=24.982; p<0.001) and after education (F=29.323; p<0.001).
| - | Pre-education Knowledge Score | Post-education Knowledge Score | ||
|---|---|---|---|---|
|
Score (7) Mean ± SD |
T/F test; P-value |
Score (7) Mean ± SD |
T/F test; P-value |
|
| Age groupa | - | - | - | - |
| 17–30 years | 4.04 ± 1.71 | F=2.762; 0.042* |
5.99 ± 1.33 | F=8.480; <0.001* |
| 31–40 years | 4.04 ± 1.71 | 5.65 ± 1.69 | ||
| 41–50 years | 4.05 ± 1.62 | 5.43 ± 1.59 | ||
| >50 years | 3.46 ± 1.69 | 4.89 ± 1.80 | ||
| Gender b | - | - | - | - |
| Male | 3.75 ± 1.59 | T=-3.245; 0.001* |
5.61 ± 1.60 | T=0.553; 0.602 |
| Female | 4.20 ± 1.77 | 5.54 ± 1.67 | ||
| Region of residencea | - | - | - | - |
| Central | 4.25 ± 1.83 | F=9.996; <0.001* |
5.51 ± 2.06 | F=29.505; <0.001* |
| Eastern | 3.71 ± 1.64 | 4.87 ± 1.52 | ||
| Western | 3.00 ± 1.52 | 4.34 ± 1.47 | ||
| Southern | 4.00 ± 1.64 | 6.26 ± 1.23 | ||
| Northern | 4.83 ± 1.38 | 5.89 ± 1.08 | ||
| Education levelb | - | - | - | - |
| High school or less | 3.66 ± 1.57 | T=-4.564; <0.001* |
5.39 ± 1.76 | T=-2.775; 0.025* |
| Higher education -degree or postgraduate level | 4.29 ± 1.76 | 5.77 ± 1.46 | ||
| Employment statusa | - | - | - | - |
| Employed | 3.93 ± 1.67 | F=1.541; 0.215 |
5.63 ± 1.59 | F=3.848; 0.014* |
| Unemployed | 3.94 ± 1.69 | 5.44 ± 1.70 | ||
| Student | 4.48 ± 1.89 | 6.26 ± 1.21 | ||
| Relationship to patienta | - | - | - | - |
| Mother | 4.05 ± 1.79 | F=0.394; 0.502 |
5.52 ± 1.61 | F=0.408; 0.272 |
| Father | 3.94 ± 1.55 | 5.53 ± 1.53 | ||
| Other relatives | 3.91 ± 1.69 | 5.64 ± 1.69 | ||
| Previous knowledge about seizuresb | - | - | - | - |
| Yes | 4.39 ± 1.72 | T=5.446; <0.001* |
5.55 ± 1.66 | T=-0.368; 0.769 |
| No | 3.64 ± 1.61 | 5.59 ± 1.62 | ||
| Previous knowledge about first aidb | - | - | - | - |
| Yes | 4.44 ± 1.73 | T=5.635; <0.001* |
5.54 ± 1.69 | T=-0.485; 0.861 |
| No | 3.65 ± 1.60 | 5.60 ± 1.59 | ||
| Other person taking care of the patienta | - | - | - | - |
| Close to patient and disease oriented | 3.87 ± 1.61 | F=0.294; 0.685 |
5.59 ± 1.56 | F=2.169; 0.062 |
| Not close to patient with less knowledge | 4.02 ± 1.69 | 5.79 ± 1.59 | ||
| None | 3.98 ± 1.73 | 5.45 ± 1.69 | ||
bP-value was calculated using t-test.
*Significant at p<0.05 level.
Additionally, caregivers who had obtained at least a university degree showed significantly higher scores on the first-aid practices questionnaire both before (T=-2.564; p=0.022) and after (T=-2.700; p=0.018) education. Caregivers who had previous knowledge about seizures also showed higher scores before education (T=5.470; p<0.001), as did those who had previous knowledge about first aid (T=8.371; p<0.001). However, both of these variables were no longer significantly associated with scores following education (both p>0.05). Additionally, respondents who had other persons taking care of the patients in a disease-oriented manner showed a significantly higher mean first-aid practice score than the other groups (F=2.877; p=0.026). As with the knowledge questionnaire, the oldest caregivers (>50 years) exhibited a significantly lower mean first-aid practice score (F=7.771; p=0.001).
| - | Pre-education | Post-education | ||
|---|---|---|---|---|
|
Score (of 9) Mean ± SD |
T/F test; P-value |
Score (of 9) Mean ± SD |
T/F test; P-value |
|
| Age groupa | - | - | - | - |
| 17–30 years | 3.26 ± 2.07 | F=0.807; 0.360 |
6.64 ± 1.79 | F=7.771; 0.001* |
| 31–40 years | 2.98 ± 2.17 | 6.59 ± 1.98 | ||
| 41–50 years | 3.18 ± 2.26 | 6.04 ± 2.19 | ||
| >50 years | 2.87 ± 2.33 | 5.48 ± 2.39 | ||
| Genderb | - | - | - | - |
| Male | 3.04 ± 2.02 | T=-0.514; 0.956 |
6.19 ± 2.10 | T=-1.670; 0.037* |
| Female | 3.13 ± 2.36 | 6.47 ± 2.15 | ||
| Region of residencea | - | - | - | - |
| Central | 2.66 ± 2.27 | F=24.982; <0.001* |
6.58 ± 2.59 | F=29.323; <0.001* |
| Eastern | 3.13 ± 2.27 | 5.67 ± 1.98 | ||
| Western | 1.68 ± 1.46 | 4.57 ± 1.98 | ||
| Southern | 3.03 ± 1.89 | 6.59 ± 1.61 | ||
| Northern | 5.39 ± 1.89 | 8.15 ± 0.96 | ||
| Education levelb | - | - | - | - |
| High school or less | 2.86 ± 2.02 | T=-2.564; 0.022* |
6.10 ± 2.21 | T=-2.700; 0.018* |
| Higher education -degree or postgraduate level | 3.32 ± 2.34 | 6.56 ± 1.91 | ||
| Employment statusa | - | - | - | - |
| Employed | 3.03 ± 2.14 | F=0.602; 0.289 |
6.24 ± 2.03 | F=0.695; 0.202 |
| Unemployed | 3.09 ± 2.30 | 6.43 ± 2.19 | ||
| Student | 3.48 ± 1.63 | 6.16 ± 1.63 | ||
| Relationship to patienta | - | - | - | - |
| Mother | 2.86 ± 2.35 | F=1.563; 0.070 |
6.46 ± 2.17 | F=1.249; 0.169 |
| Father | 3.15 ± 2.36 | 6.08 ± 2.05 | ||
| Other relatives | 3.21 ± 1.99 | 6.33 ± 2.04 | ||
| Previous knowledge about seizuresb | - | - | - | - |
| Yes | 3.64 ± 2.32 | T=5.470; <0.001* |
6.28 ± 2.10 | T=-0.386; 0.717 |
| No | 2.66 ± 1.99 | 6.35 ± 2.08 | ||
| Previous knowledge about first aidb | - | - | - | - |
| Yes | 3.96 ± 2.25 | T=8.371; <0.001* |
6.49 ± 2.12 | T=1.575; 0.052 |
| No | 2.49 ± 1.94 | 6.21 ± 2.06 | ||
| Other person taking care of the patienta | - | - | - | - |
| Close to patient and disease oriented | 3.44 ± 2.42 | F=2.852; 0.175 |
6.65 ± 2.03 | F=2.877; 0.026* |
| Not close to patient with less knowledge | 2.86 ± 1.91 | 6.08 ± 1.91 | ||
| None | 3.02 ± 2.19 | 6.29 ± 2.19 | ||
bP-value was calculated using t-test.
*Significant at p<0.05 level.
| - | Pre-education Knowledge Score | Post-education Knowledge Score | Pre-education First-aid Score | Post-education First-aid Score |
|---|---|---|---|---|
| Pre-education knowledge | 1 | - | - | - |
| Post-education knowledge | 0.544** | 1 | - | - |
| Pre-education first aid | 0.441** | 0.202** | 1 | - |
| Post-education first aid | 0.483** | 0.660** | 0.436** | 1 |
Table 8 describes the findings of Pearson coefficients to measure the relationships between both knowledge and first-aid practice scores before and after education (Table 8). Our results have shown that the relationships between pre- and post-education knowledge scores (r=0.544; p<0.01), between pre-education knowledge score and pre-education practices score (r=0.441; p<0.01), and between pre-education knowledge score and post-education first-aid score (r=0.483; p<0.01) were each highly statistically significant. We also found that there was a significant and positive correlation between post-education knowledge score and both pre-education first-aid score (r=0.202; p<0.01) and post-education first-aid score (r=0.660; p<0.01). Finally, the correlation between pre- and post-education first-aid scores was also positive and highly statistically significant (r=0.436; p<0.01).
4. DISCUSSION
This study assessed the effectiveness of education in improving knowledge of epilepsy and first-aid practices of caregivers in Saudi Arabia. The findings of the current study may be useful to improve knowledge of patients' caregivers and the outcomes for patients with seizures. A disease-oriented caregiver is most likely to provide safe first-aid treatment to a child having a seizure episode. After educational intervention, a good knowledge level was attained among a majority of the participants.
Al Harbi et al. [9] reported that primary school female teachers showed slightly better overall knowledge, with approximately 80% of their sample demonstrating above-average knowledge about epilepsy, than what the current study reports. Consistent with our findings, several studies have reported significant improvements in knowledge of seizures among caregivers of children [3, 11-15] after interventions. However, Abbasi Kangevari et al. [16] reported a low level of knowledge in a sample taken from the general population of Iran.
In this study, several factors influenced epilepsy knowledge level. In particular, higher levels of education were associated with good knowledge levels, while older age and living in the western regions of Saudi Arabia were associated with poor knowledge levels. These findings were consistent with studies by Teferi and Shewangizaw [1] and Eze et al. [3]. Furthermore, respondents with previous knowledge about seizures showed significantly better knowledge prior to education. Still, following the educational sessions, the difference between those who did or did not have previous knowledge was not statistically significant, even though both groups exhibited an improvement in knowledge. Similar to the current study, Teferi and Shewangizaw [1] observed a difference in knowledge between respondents based on prior knowledge about epilepsy. They also reported various other factors as being associated with knowledge, including having heard about epilepsy, distance to health facility from the place of residence, having witnessed an epileptic seizure, having an age range from 46 to 55 years, occupational history of being self-employed or a laborer, and having a history of epilepsy or a history of epilepsy in family members. A study in Nigeria reported that a multivariate regression model identified marital status and department of study as possible predictors of knowledge in a sample of trainee teachers [3].
In order to provide urgent and safe care in response to seizures, it is necessary for caregivers of patients with epilepsy to have adequate practical knowledge of effective first-aid techniques. In the current study, a majority of caregivers (84%) performed poorly in first-aid practices, with only 16% of respondents achieving good scores. However, after education, the percentage of caregivers with poor levels of practice decreased to 32.4%, while 67.6% showed good practices. These results are similar to improvements following education reported in Nigeria [1], Iran [14], and India [15]. Other papers have reported overall good practices toward first aid management. For example, Teferi and Shewangizaw [1] reported that 33.5% of respondents adopted safe practices related to epilepsy, while Abbasi Kangevari et al. [16] reported that 45.4% of their respondents showed good and 42.5% showed very good levels of practical techniques. In contrast, Al-Harbi et al. [9] indicated that the overall practices were poor in the Kingdom of Saudi Arabia, with only 31.8% of female teachers reporting an ability to provide first-aid care to epileptic students.
Additionally, we observed that showing a good understanding of first-aid practices was significantly dependent on knowledge level, while having a poor understanding was significantly associated with caregivers' residence originating from the western regions of the Kingdom of Saudi Arabia. We also observed that the age group was not significantly associated with first-aid practices before the educational intervention; however, after the sessions, the oldest age group (>50 years) showed significantly lower practice scores. Another important finding was that gender was not significantly associated with first-aid practices before education, but after education, females showed significantly higher practice scores than males. In contrast, previous knowledge about seizures and first aid did not significantly improve the scores after education.
Finally, caregivers who were close to patients and had a diseased-oriented relationship did not show a significant difference from relative caregivers in pre-education first-aid practice scores, but after education caregiver type was significantly associated with first-aid practices. Few studies have evaluated the factors associated with first-aid practices before and after education. However, a study in Ethiopia reported that several factors were observed to be related to practical knowledge, including living alone, living in rural areas, years of formal education, age, and prior knowledge about epilepsy [1]. The results of that study conflicted with those of a study conducted in Nigeria [3], which reported observing no relationships between first-aid management and general characteristics in a sample of trainee teachers.
In the present study, the correlations between and among pre-education knowledge, post-educational knowledge, pre-education first-aid practices, and post-education first-aid practices were positive and significant. That is, pre-education knowledge was positively and strongly correlated with post-education knowledge, pre-education first-aid practices, and post-education first-aid practices. Similarly, post-education knowledge was positively correlated with both pre- and post-education first-aid practices, and the correlation between pre-education first-aid practices and post-education first-aid practices was also significant. This indicates that as pre-education knowledge increases, all domains are likely to increase for both pre-and post-education.
Knowledge of information sources is necessary to address gaps in both knowledge and use of first-aid practices. In this study, our results revealed that the source of information for knowledge about seizures and for practical knowledge about first aid were strikingly similar in nature. Caregivers reported that doctors, the internet, and courses were the most commonly used sources to obtain information about seizures and first aid. This result is consistent with the results of Neyaz et al. [2], who reported that teachers listed doctors and the internet as their main sources of information regarding first aid. Other studies have reported conflicting results. For instance, several studies have reported that participants are more likely to rely on information from media [3-15], while others have reported that participants rely on relatives, family, and friends for information [16].
5. LIMITATION
The limitations of the research must be acknowledged. The study was constrained by the lack of a control group given the nature of the pre- and post-test intervention design; as a result, it was underpowered to determine the magnitude of the associations between variables and improvement in both knowledge and practice. It is important to consider the time of the post-test intervention assessment as it could have caused recollection bias among the caregivers.
CONCLUSION
Prior to education, caregivers' knowledge about seizures and seizure-related first aid practices was suboptimal, but these were markedly improved following education. Our results suggested that having a university degree was positively associated with seizure-related knowledge and first-aid practices. A collective effort is therefore needed in order to increase both caregiver general knowledge and practical knowledge related to first-aid. Government institutions play a vital role in addressing the education gaps among caregivers. An awareness campaign might aid in effectively delivering education through community-based programs or print ads. These targeted educational health promotions could bring awareness to those with lower levels of education and older caregivers living in particularly the Western regions of Saudi Arabia.
ABBREVIATION
| RREC | = Regional Research Ethics Committee |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study has been approved by the Regional Research Ethics Committee (RREC) with the approval number 29288-1441.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All respondents signed informed consent and were informed about the aims of the study, the confidentiality of collected data, and that they could withdraw from the study at any time.
ACKNOWLEDGEMENTS
We would like to thank the following amazing doctors who participated in collecting the data for this project: Drs. Mona Ali AlQarni, Noura Mesned Almutairi, Amjad Salem Alshlaqy, Bandar Aqeel Alharbi, Zainab Hussain Alrashed, Rawan Habib Alhameed, Sarah Musaad Alrashidi, Esra Ali Alghamdi, Sarah Abdullah Alshehri, Sharaf Abdullah S Ghawa, Daliah Abdulrahman Alharbi.

