All published articles of this journal are available on ScienceDirect.

A Comprehensive Review of Toxoplasmosis: Serious Threat to Human Health
Authors Info & Affiliations
Abstract
Toxoplasmosis is a parasitic disease caused by Toxoplasma gondii. Despite infecting a major fraction of the global population, T. gondii rarely results in clinically significant disease. Cats are the only known definitive host for this parasite, which sheds millions of oocysts in its feces every day, which then sporulate and become infective in the environment. This comprehensive review article aims to explain the etiology, pathogenesis, epidemiology, transmission, clinical symptoms, diagnosis, risk factors, public health importance, economic effect, treatment, and prevention of toxoplasmosis. A search for various publications in English with the criteria of reviewing articles explaining toxoplasmosis was carried out. T. gondii reproduces through two life cycles, namely the sexual cycle and the asexual cycle. In general, consuming parasite cysts in tainted food or water is how humans and other warm-blooded animals become infected with T. gondii. Nearly every region of the world has reported incidences of toxoplasmosis in humans, and around one-third of people are susceptible to latent infection. According to the reports, the main ways through which diseases spread are by water, tainted food, eating tissue cysts or oocysts, and congenital transmission. Infected individuals may experience asymptomatic cervical lymphadenopathy during an acute systemic infection. Diagnostic evaluation is very important for early detection, prevention of transmission, and as a reference for treatment options for infected pregnant women. Consuming undercooked meat is traditionally seen as a significant risk factor for developing toxoplasmosis. The impact of toxoplasmosis is very significant in humans because it causes abortion and disease in newborns, resulting in serious economic losses. To treat toxoplasmosis, dihydropteroate synthetase and dihydrofolate reductase inhibitors are advised. Toxoplasma transmission to humans can be avoided by thoroughly washing your hands with soap after handling meat, poultry, or shellfish.
1. INTRODUCTION
A zoonotic condition called toxoplasmosis is caused by the protozoan parasite Toxoplasma gondii [1]. This species belongs to the phylum of Apicomplexa intracellular coccidian parasite [2]. This parasite is typically spread by animals, including domestic pets like dogs, cats, and birds, as well as livestock like pigs, cows, goats, and sheep [3]. This parasite is found throughout the world [4]. It is a parasite with characteristics resembling the malaria-causing disease [5]. Despite infecting a major fraction of the global population, T. gondii rarely results in clinically significant disease [6]. Although toxoplasmosis is typically asymptomatic, it can become serious and even fatal during pregnancy when it affects the fetus, the infant, and people with compromised immune systems [7]. The majority of toxoplasmosis cases in immunocompetent people are benign or subclinical [8]. Individuals with immunodeficiency and congenital forms of the condition experience the most severe symptoms [9].
T. gondii is a parasite that is extensively researched due to its value in medicine and veterinary science, as well as its appropriateness as a model for cell biology and molecular investigations with unicellular organisms [10]. The name Toxoplasma gondii comes from the Greek words toxon (arc) and plasma (shape), while gondii comes from the rodent Ctenodactylus gundi, which was first isolated in 1908 [11]. There are various kinds, such as oocysts, tachyzoites, and cysts [12]. This parasite lacks host specificity and has a universal nature [13]. While it only infects cats during the sexual stage, it can parasitize any mammals during the asexual stage, including humans and cats [14]. The wide variety of warm-blooded mammalian hosts, including the risk of infection in a third of the global human population, makes T. gondii the most feared parasitic organism worldwide [15].
The prevalence of the disease varies significantly worldwide [16]. For instance, toxoplasmosis prevalence can reach approximately 90% in specific demographic groups in highly endemic areas, such as portions of Africa, whereas it might reach 60% in some communities in Europe [17]. Cats are the only known definitive hosts for this parasite, shedding millions of oocysts in their feces every day, which then sporulate and become infective in the environment [18]. Although oocyst shedding in domestic cats only happens 1-3 weeks after the first infection, it may occasionally occur throughout a cat's lifetime in feral cats [19]. The two primary horizontal routes of transmission are ingestion of these sporulated oocysts, which infect plants, soil, and water supplies, or intake of bradyzoites from raw or undercooked meat [20].
Meat, which is raw or undercooked, with Toxoplasma cysts or oocysts can transmit the disease [21]. These cysts are resistant to stomach acid when swallowed, and the parasite is prepared to infect if swallowed [22]. It is possible that a pregnant woman who has toxoplasma will pass it on to the fetus through the placenta without exhibiting any clinical symptoms; nevertheless, the symptoms will emerge after the baby is born [23]. Infection in ruminant animals is thought to be spread through cat feces-contaminated food and insect vectors, such as flies and cockroaches [3]. The disease can also spread through the mucous membranes of infected hosts through inhalation, saliva, mucus, feces, and milk from patients [17]. When this disease breaks out, immune-compromised adults experience acute and sporadic symptoms. People with impaired immune systems, such as those with HIV/AIDS, experience severe outbreaks (after the reactivation of bradyzoites into disseminated tachyzoites) [24].
The clinical manifestations of this illness are persistent and subclinical for the duration of the infection [25]. Due to the fact that toxoplasmosis does not always result in pathological conditions in the host, especially in patients with strong body immunity, many infected people are unaware that they are infected [26]. The most obvious symptom is if this infection develops during pregnancy, which increases the risk of miscarriage, stillbirth, live delivery with birth defects, such as hydrocephalus or microcephalus, motor difficulties, retinal and brain damage, as well as indicators of mental disorders [27]. In addition, prenatal infection caused by toxoplasmosis might result in chorioretinitis in people [28]. The onset of clinical signs includes fever, malaise, soreness in the muscles, pneumonia, inflammation of the meninges of the brain, and psychomotor abnormalities [8].
Toxoplasmosis infections are recognized as a concern and a serious public health issue due to the great prevalence of transmission in humans, the chronic nature of the disease, its potentially lethal effects, and the fact that many people are unaware they have the infection [29]. This comprehensive review article aims to explain the etiology, pathogenesis, epidemiology, transmission, clinical symptoms, diagnosis, risk factors, public health importance, economic impact, treatment and prevention of toxoplasmosis. The scientific literature that the public can utilize to prepare for toxoplasmosis is provided by the data gathered through this review.
2. ETIOLOGY
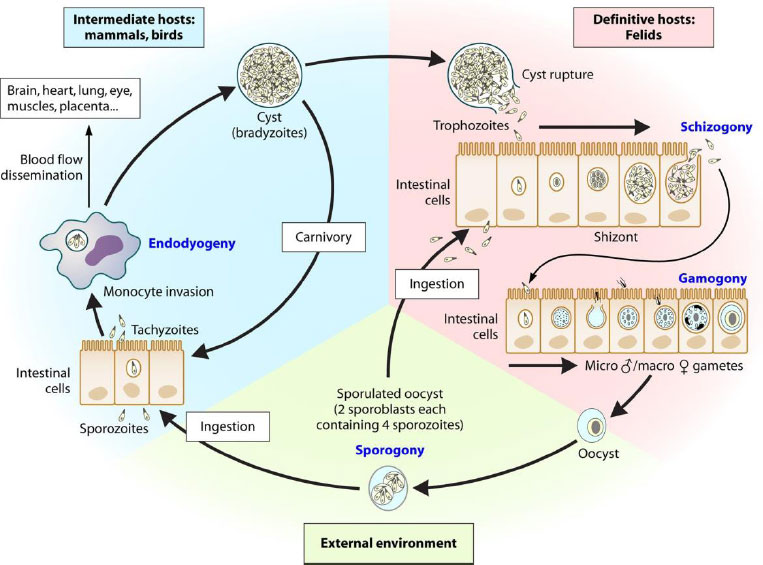
In 1908, Nicole and Manceaux made the initial discovery of T. gondii in rats (Ctenodactylus gundi) in Africa [30]. T. gondii belongs to the Genus Toxoplasma, Subfamily Toxoplasmatinae, Family Sarcocystidae, Subclass Coccidia, Class Sporozoa, and Phylum Apicomplexa [31]. The first form is a trophozoite, which contains a crescent-shaped nucleus with a karyosome in the middle and is 4-6 microns in length and 2-3 microns in breadth [2]. When stained with Romanowsky's stain, the nucleus will be red, while the cytoplasm will be pale blue. The second form, bradyzoites, a stage of chronic toxoplasmosis, divide slowly in tissue cysts while doing endogenous division in cysts [32]. Tissue cysts are found in chronic or asymptomatic infections in the brain, skeletal muscle, and heart [29]. These cysts, which can hold up to 60,000 bradyzoites, can persist in the tissue for several days after the host has passed away [33]. The third form, oocysts, which are typically discharged in the cat's feces and are located in the cat's intestines, particularly those that have sporulated (contain sporozoites), can endure temperatures of 24°C for 10 months or 37°C for 28 days [34]. The life cycle of T. gondii is shown in Fig. (1).
T. gondii reproduces through two life cycles, namely the sexual cycle and the asexual cycle [1]. The asexual cycle occurs in hosts between humans and warm-blooded animals, such as birds, but the sexual (enteroepithelial) cycle occurs in true hosts, such as cats [35]. The asexual stage begins with the ingestion of infective cysts or oocysts by the true host (cats eat mice containing the first or third forms of T. gondii) [36]. The time needed for T. gondii to develop from the bradyzoite prepatent stage (second form) is 3-10 days, but the time needed for tachyzoites (first form) is 5-10 days, and the third form takes 24 days or longer to develop into oocysts [18].
The five forms of bradyzoite and tachyzoite cysts that form are types A, B, C, D, and E, each of which differ in the number of organisms present and in the way those organisms divide [37]. Type A, which first manifests 12 to 18 hours after infection and is the smallest division, seems to have two or three organisms in the small intestine [38]. Type B, which appears 12-54 hours after infection, contains a primary nucleus in the center [39]. Type C, which is separated into schizogony and occurs 24 to 54 hours after infection, is made up of endodiogeny and endopolygeny [40]. This type has a subterminal nucleus. Type D occurs from 3-15 days after infection, and according to Hatter et al. [41], a total of 90% of toxoplasma is found in the small intestine at that time. Type D is smaller than type C and is divided into endodiogeny and schizogony [18]. Type E is divided into schizogony, which occurs 3-15 days after infection and is similar to type D [39].
The sexual stage begins with the development of merozoites into macrogametes and macrogametes in the intestinal epithelial cells. The two gametes undergo a fertilization process, and a zygote is formed, which then grows into an oocyst [42]. Oocysts pass out with the feces after entering the intestinal lumen [43]. The oocysts either sporulate or become infectious after 2-3 days at 24°C [44].
This cycle occurs concurrently with the cycle in the epithelium of the intestinal cells of the actual host and is the subsequent life cycle that takes place outside the intestinal tissue of the true host, particularly in the intermediate host [45]. The tachyzoites that are produced after oral infection develop into vacuoles of various types of cells that are targeted [46]. Then, eight or more tachyzoites are built up in cells; this is known as pseudocyst [47]. When a pseudo-cyst ruptures, tachyzoites attack the surrounding cells and spread throughout the body through the blood and lymph flow [48]. Tachyzoites will be eliminated by the body's immunity, with the exception of those that have evolved into bradyzoites in tissue cysts, such that parasitemia may repeat multiple times until antibodies are generated in the plasma [32]. Tissue cysts are found as early as the eighth day following the host's first infection, and they can endure for the duration of the host's life [49]. A repeat of the acute Toxoplasma infection could occur if bradyzoites are released and grow into tachyzoites as the body's immunity declines [50].
3. PATHOGENESIS
In general, consuming parasite cysts in tainted food or water is how humans and other warm-blooded animals become infected with T. gondii [51]. T. gondii lacks the specialized organelles needed for mobility during its voyage, such as cilia or flagella [52]. This parasite will move with the actin-myosin motor complex [53]. T. gondii can move in three different ways: helical motion, circular motion, and spiral motion [54]. The parasite can advance by helical movement [55]. This parasite's cytoskeleton is made up of adhesins that are secreted from micronemes, which are apical organelles [56]. T. gondii can migrate more easily because of this micronema protein's attachment to host cells [57].
Following ingestion, the stomach of the host breaks down the T. gondii cyst wall and produces bradyzoites, which are immune to the gastric peptide enzyme [58]. This parasite can, therefore, enter the small intestine. T. gondii will develop into tachyzoites in the small intestine, reproduce inside the cells to create parasitoporous vacuoles, and then start to infect the neighboring cells [59]. Soedarto (2012) demonstrated that parasitoporous vacuoles can quickly enter host cells [60]. The host's surface cells and the parasite's walls are only loosely connected [61]. This weak affinity is mediated by surface proteins from parasites called SAGs (surface antigens), SRSs (SAG-related sequences), and SUSAs (SAG-unrelated surface antigens) [62]. More than one host molecule is thought to have a role in mediating this attachment to host cells [61]. Although specific receptors have not been found on host cells, it is suspected that laminin, lectin, and SAG1 play a role in the attachment and entry of tachyzoites [63].
After piercing the intestinal epithelial layer in the small intestine, tachyzoites will go to the lamina propria [49]. Tachyzoites in the lamina propria cause a potent immunological response that includes polymorphonuclear neutrophils, monocytes, and dendritic cells [64]. This immune reaction will kill certain parasites, while others will continue to multiply in cells [65]. Parasites that grow in cells travel through the intestinal lymphatics to the lymph nodes [66]. Additionally, tachyzoites will be spread via the transendothelial migration (TEM) mechanism in conjunction with blood flow through lymph flow [67]. The organs and tissues of the host's body with nuclear cells can eventually become infected with T. gondii [68].
Seven days after infection, cysts start to grow in tissue and last for the duration of the host's life [18]. These tachyzoite cysts will proliferate and form necrosis [69]. The tachyzoites will be removed from the host's tissue if the immune reaction is effective [32]. However, if the host's immune system is weak or compromised, an acute infection will develop, progress, and perhaps result in clinical symptoms [70]. These clinical symptoms differ in each tissue and might cause significant damage by triggering an inflammatory response [71].
4. EPIDEMIOLOGY
Toxoplasmosis infection has been reported in warm-blooded animals and humans, and its spread has been reported throughout the world [1]. Almost every species, including mammals and various bird species, is affected by this disease [72]. Nearly every region of the world has reported incidences of toxoplasmosis in humans, and around one-third of people are susceptible to latent infection [17]. The incidence of toxoplasmosis in developing and underdeveloped countries is reported to be very high, but it has been found that the transmission rate is low in developed countries [6]. Africa, the Middle East, Southeast Asia, Central Europe, Latin America, and Eastern Europe are among the regions with the highest recorded rates of toxoplasmosis [38]. Toxoplasmosis rates in the US range from 15 to 22%, and the current percentage is lower than in prior years [73]. In Europe, a similar pattern is also present [74]. Its prevalence can be affected by a number of elements, including culture, environment, ethical standards, and the presence of cats [75].
According to Shapiro et al. [20], oocysts have a high percentage of environmental survival. Due to the chilly climate, toxoplasmosis is extremely rare in European countries and more common in warm climates [1]. The frequency of toxoplasmosis in cats is estimated to be around 40% based on climatic factors; however, it drops to 16.1% in the southwest and reaches a high of 59.2% in Hawaii [76]. Food preparation habits, such as undercooked or undercooked food, are important factors that influence transmission [77]. Consuming raw shellfish and oysters has been identified as a significant risk factor for the spread of toxoplasmosis in a number of nations [78]. T. gondii infection affects between 25 and 30% of the world's population [79]. Many climatic factors influence oocyst survival rates, and ruminants play an important role in disease transmission [3].
Additionally, it appears that seroprevalence is higher in older adults, depending on the socioeconomic circumstances of the individuals [80]. Water containing oocysts, drinking unfiltered water, or drinking water in recreational facilities all help spread this illness [81]. The incidence of toxoplasmosis infection is influenced by socioeconomic status [82]. In Brazil, the upper socioeconomic group has a seroprevalence of 23%, the middle socioeconomic group 62%, and the bottom socioeconomic group 84% [83]. Unfiltered water consumption raises the possibility of contracting Toxoplasma [84]. These analyses are especially important in underdeveloped and underprivileged countries [85]. However, toxoplasmosis infection is predominantly linked to poverty in the United States [86]. Additionally, different communities in the US have different rates of toxoplasmosis infections [17].
Over the past 20 years, toxoplasmosis rates have decreased in many nations due to improvements in socioeconomic situations, drinking water quality, hygiene standards, consumption of frozen meat, modifications to livestock systems, and feeding autoclaved food to cats [87]. Infections with T. gondii were found in 14.1% of US citizens between the ages of 12 and 49 from 1988 to 1994. However, they dropped by 9% between 1999 and 2004 [1]. In France, toxoplasmosis infected around 80% of expectant mothers in the 1960s, but that number fell by 44% by 2003 [23]. There are reports of this declining trend in practically all of the European nations [88]. In the Netherlands, women of reproductive age experienced a 50% decline in the disease's seroprevalence between 1995 and 2007 [89].
5. TRANSMISSION
According to reports, the main ways that diseases are spread include water, tainted food, eating tissue cysts or oocysts, and congenital transmission [87]. However, this disease's spread throughout groups varies significantly, largely depending on dietary and behavioral patterns [90]. Unpasteurized milk can cause infection, and tachyzoites can contaminate blood [91]. The majority of intermediate hosts are tissue cysts found in the muscles and brain [32]. As hosts for the continuation of sexual reproduction, enteroepithelial cycling, and oocyst formation, cats have been documented to contract toxoplasmosis from infected prey, such as birds or rodents [39]. Carnivorous animals from wild habitats, such as skunks, foxes, raccoons, and bears, also contract toxoplasmosis by consuming cysts from tissue [92]. Consuming tainted uncooked meat, such as lamb or pork, causes toxoplasmosis in humans [93]. Numerous proteolytic enzyme activities in the stomach of the host break down ingested tissue cysts, releasing parasites in the form of bradyzoites [58]. This parasite is shown to be extremely protease-resistant and persists in the small intestine of the host organism [94]. According to one study, within two weeks of consumption, more than 10 million cysts are expelled in cat feces [95]. Oocysts that have been released into the environment will sporulate within five days [20]. These sporulating organisms persist in soil samples for almost a year [96].
A primary risk factor for spreading toxoplasmosis is generally eating vegetables, fruits, or anything that has been infected with oocysts [97]. Prior reviews of these risk variables and transmission methods were carried out by Ebrahimi et al. [98]. Infections from oocysts in people are more severe and complex than infections from cysts [99]. However, it has been observed that waterborne infections are sporadic [20]. In the US, toxoplasmosis outbreaks have been associated with marine animal contact, while in Canada, outbreaks of the disease have been linked to oocyst contamination of municipal water reservoirs [100]. Cats shed their oocysts over a short period of time, and despite their non-infectious oocyst shedding, direct contact with cats does not increase the chance of contracting a cat infection [101]. Oocysts remained persistent for six months in seawater, demonstrating that coastal habitats are a significant source of infection [102]. Additionally, oocysts switch between hosts [103]. Fish like sardines and anchovies, which are filter feeders, contain oocysts that can tolerate a variety of conditions and continue to survive [104].
There have also been reports of congenital transmission, which happens when toxoplasmosis is in the acute phase [105]. Tachyzoites, which are parasites from the mother that cross the placenta and infect the fetus, are contagious [106]. Based on the stage of pregnancy, maternal toxoplasmosis has different effects [23]. Maternal toxoplasmosis levels are very low during the first trimester of pregnancy, but as the pregnancy progresses, the transmission rate rises to about 80% [107]. Early maternal toxoplasmosis is associated with a number of issues, including mental impairment, hydrocephalus, and spontaneous abortion [108]. However, the transmission rate is particularly high during the final trimester, and children have been documented to experience a variety of subclinical interventions, including recurrent chorioretinitis and subclinical interventions that may result in blindness or vision issues [109]. According to earlier research by Galvan-Ramírez et al. [110], congenital toxoplasmosis affects about 1 in 1000 to 1 in 10,000 newborns in most population groups. In a study, Faral-Tello et al. [111] employed PCR to identify vertical transmission through umbilical cord tissue, and the transmission rate was close to 19.8%. The transmission rate is roughly 75% in mouse models; however, it has been noted to drop to 65% in sheep [112]. These results suggest that the degree of vertical transmission in humans is not yet fully understood because the majority of investigations only employ serological techniques. Oocysts are abundant in a wide range of habitats, so it is crucial to examine oocysts in the environment to determine health concerns [113]. Recent research demonstrates that oocysts contaminate marine, aquatic, and terrestrial habitats [114]. Environmental and geological factors like soil texture, temperature, and chemistry have a major impact on T. gondii oocyst survival [75]. There is a dearth of information on oocyst survival rates, persistence in soil samples, and pathogen traits, including tissue cyst infectivity.
6. CLINICAL SYMPTOMS
The majority of immunocompetent people would not experience symptoms for the rest of their lives, although both competent and immunocompetent people can contract the illness, particularly retinochoroiditis [115]. Infected individuals may experience asymptomatic cervical lymphadenopathy during acute systemic infection, as well as signs and symptoms that resemble infectious mononucleosis, such as myalgia, sore throat, myocarditis, maculopapular rash, fever, meningitis, polymyositis, muscle pain, malaise, pneumonia, and psychomotor disorders [8].
6.1. Ocular Toxoplasmosis
Ocular toxoplasmosis (OT) frequently results in distinctive, localized, white-appearing retinal lesions that are typically smaller than 1,000 microns [116]. A significant vitreous inflammatory response gives the unmistakable “headlights in the fog” image [117]. These lesions are caused by immune reactions against the parasite and direct parasitic tissue invasion [118]. Active lesions are frequently accompanied by nearby old scars [119]. The clinical indicators and illness presentation of patients with AIDS varied significantly, and other infectious diseases, such as cytomegalovirus, chorioretinitis, and syphilitic retinitis, should be considered in the differential diagnosis [29].
During primary or recurrent eye infections, retinochoroidal inflammation typically lasts for 2 to 4 months [119]. Nearly one in four patients with active OT lesions experienced blindness in at least one eye and one in five patients experienced a recurrence, especially in eyes that had previously experienced retinal scarring, according to an observational case series of 154 patients with active OT lesions who were monitored for at least five years [120]. People over the age of 40 and those who were exposed to the parasite within the first five years of their recovery have a higher risk of developing OT again [121].
6.2. Toxoplasmic Encephalitis
Toxoplasmic encephalitis (TE), which is typically caused by the reactivation of latent infections, continues to be a significant source of morbidity and mortality in AIDS patients, even in the era of highly active antiretroviral therapy [122]. Particularly in areas where the disease is more prevalent, like South America, TE should be suspected since it can present with a wide range of nonspecific symptoms, including dementia, ataxia, lethargy, and seizures [123].
The most distinguishing sign of T. gondii infection in AIDS patients, although it is not pathognomonic, is the appearance of numerous brain abscesses [124]. Although the basal ganglia and corticomedullary junction are the most often infected areas of the brain with T. gondii, postmortem brain examination shows that both hemispheres are involved globally [125].
6.3. Congenital Toxoplasmosis
Congenital toxoplasmosis in newborns can be asymptomatic or cause retinochoroiditis and CNS involvement [126]. Congenital toxoplasmosis is thought to affect 1-10 out of every 10,000 live births in the United States, 770 live births in Brazil, and 3,000 live births in France [67]. The burden of this disease in the Netherlands, however difficult to calculate, is roughly 620 disability-adjusted people each year, primarily because of retinal disease and fetal death [127]. This burden is equivalent to the widespread and frequent foodborne pathogen Salmonella spp [128].
The infection is typically more severe if transmitted early in pregnancy, but the danger of vertical transmission is higher in the latter stages of pregnancy [27]. The infection's most obvious symptom is when it affects a pregnant woman, which increases the risk of abortion, stillbirth, live births with malformations, such as hydrocephalus or microcephalus, motor difficulties, retinal and brain damage, and indicators of mental disorders [106]. Ultrasonography may be used to find and diagnose intracranial calcifications [129]. Epilepsy and delayed mental development are among the clinical signs and symptoms, which are comparable to those of other complex congenital illnesses like rubella, CMV, and the herpes simplex virus [130].
Congenital OT is generally more sight-threatening than acquired infections because the retinal lesions found in congenitally infected newborns are often located in the macula, the region responsible for central vision, and children who experience blindness or nearsightedness due to toxoplasmosis will remain disabled for years [117].
In contrast to other countries, where rates are significantly higher, congenital toxoplasmosis affects about 9% of children with serious visual impairment in the United States [131]. In Europe, 29% of children experience visual impairment, compared to 87% of children in Brazil, within three to four years of birth [132].
7. DIAGNOSIS
Diagnostic evaluation is very important for early detection, prevention of transmission, and as a reference for treatment options for infected pregnant women [133]. Although not routinely performed, diagnostic testing includes maternal serum sampling, the use of early fetal ultrasound, and amniocentesis [23]. Maternal examinations are performed periodically in high-risk settings, particularly in European nations [27]. Given that food intake has been established as a significant contributor to maternal infection, cultural behaviors involving food preparation and consumption are a significant element influencing the present transmission process [134]. In some nations, standardized newborn and mother screening procedures are infrequently used [135]. However, in order to prevent congenital infection, pregnant women who are in the high-risk category for getting toxoplasmosis must be examined [109].
The initial diagnostic procedure for identifying both present and historical infections is serological testing [136]. Serum markers identify the presence of immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies in maternal blood samples [137]. These antibody markers are indicative of T. gondii infection [138]. They can be detected using a variety of testing techniques, including dye tests, indirect fluorescent antibody tests, and enzyme immunoassay tests [139]. It is important to thoroughly evaluate IgM and IgG titers to differentiate between acute and chronic infections [140]. Five days to weeks after the initial exposure, IgM titers rise dramatically in response to acute illness [141]. Approximately one to two months later, the peak rise in IgM antibodies occurs [27]. One to two weeks after the first infection, IgG antibodies are typically found [142]. IgG titers increase for years after initial exposure [143].
The date of maternal infection is predicted by the presence of both serum antibodies [134]. There is no sign of infection in the mother if IgG and IgM markers are not found [144]. Persistent infection has been identified if the test reveals a positive IgG antibody marker with a negative IgM signal [138]. A new infection is believed to have occurred if both antibody markers are increased [145]. A repeat serum test is advised in situations of acute infection two to three weeks after the original findings [146]. Acute infection is indicated by a substantial rise in serum IgG antibody titer that is typically at least four times the baseline level [147]. The necessity of verifying a positive test through laboratory results arises from the prevalence of false positive results [133]. In nations that use serum testing, blood samples will still be taken for screening during the pregnancy even if the mother tests negative [148]. This screening technique enables early diagnosis in the mother and serves as a start toward therapy and prevention before the fetus undergoes seroconversion [136].
Amniocentesis can be carried out on pregnant patients whose toxoplasmosis test results are positive [149]. The ideal time to do an amniocentesis is no earlier than 18 weeks of pregnancy and four weeks following a suspected infection [109]. The high rate of false positive results and the significant risk of premature labor necessitate that amniocentesis is not to be carried out before 18 weeks [23]. T. gondii parasite detection in the amniotic fluid is necessary for the amniocentesis-based prenatal diagnosis of congenital toxoplasmosis [73]. Polymerase chain reaction (PCR) fluid testing is a popular diagnostic technique [150]. The positive predictive value of PCR testing is almost 100% [151]. Traditionally, fetal blood sampling via cordocentesis was once considered the gold standard of diagnostic testing [133]. Due to the increased fetal dangers of cordocentesis compared to amniocentesis, it is no longer practiced [149].
Fetal ultrasonography was used in the last diagnostic studies [27]. Ultrasound is recommended for women suspected of or diagnosed with an acute infection [144]. Fetal ultrasound checks for anomalies in the developing nervous system, kidneys, and liver [152]. Using ultrasound, it is possible to identify intracranial anomalies, such as hydrocephalus, ventriculomegaly, and intracerebral calcifications [109]. Along with the toxoplasmosis diagnosis, ultrasonography also reveals splenomegaly, congenital nephrosis, and ascites [153]. The prevalence of numerous fetal screening procedures is rising as a result of an increase in congenital toxoplasmosis presentations in neonates [107]. Fetal screening through neonatal screening is a process that is another detection approach in addition to newborn screening [154]. These screening techniques are crucial for detecting infants who are impacted; therefore, treating symptoms as they arise rather than taking preventative steps is necessary.
8. RISK FACTOR
Human infection is typically contracted by eating undercooked or raw meat that contains cyst tissue or by drinking water that has been contaminated with oocysts discharged by cats [97]. Consuming undercooked meat is traditionally seen as a significant risk factor for developing toxoplasmosis, particularly when it comes to lamb and hog [155]. Variations in T. gondii seroprevalence seem to be correlated with the food and hygiene practices of a population [156]. The prevalence of toxoplasmosis has decreased as a result of better farming techniques and improved public knowledge of the dangers of eating undercooked meat [157]. Transmission of T. gondii through organ transplantation from seropositive donors to seronegative recipients is an important potential cause of disease in heart, liver, kidney, and pancreas-liver transplant patients [158]. The epidemiology of this parasite has been expanded by the discovery of waterborne toxoplasmosis in humans [159]. There have not been any reports of transmission during nursing or direct human-to-human transmission other than from mother to fetus.
9. PUBLIC HEALTH IMPORTANCE
A zoonotic protozoan parasite called T. gondii affects almost all warm-blooded creatures, including humans, domestic animals, and wild animals [1]. T. gondii-related human disease was first identified in the late 1930s [160]. According to reports, the rate of human infection varies worldwide [17]. Human toxoplasma infection can have catastrophic consequences, particularly for those with weakened immune systems, pregnant women, HIV/AIDS patients, youngsters, and those with co-occurring disorders [161]. The leading cause of death among AIDS patients is toxoplasmosis [29]. Infection during pregnancy can cause retinochoroiditis, hydrocephalus, intracranial calcification, and congenital infections of the fetus, in addition to abortion and other birth defects [162].
10. ECONOMIC EFFECT
The impact of toxoplasmosis is very significant in humans because it causes abortion and disease in newborns, resulting in serious economic losses [65]. There are several factors to take into account when analyzing the economic impact of disease. In addition to losses, the direct costs of disease also include the costs of treating affected animals and the costs of disease prevention [3]. Other factors are loss of expected output value and wastage of resources due to disease [163]. T. gondii is thought to be the primary cause of reproductive failure in commercial small ruminants like sheep and goats, and infections in these animals may be a significant factor in the parasite's transmission to humans [1].
Primary T. gondii infection is most likely to result in abortion in small ruminants that produce wool, milk, and meat [3]. Sheep that are congenitally infected are incapable of feeding themselves, have poor physical conditions, and lack muscle coordination [164]. Toxoplasmosis has a significant socioeconomic impact on human suffering and health care costs, particularly for children who are mentally retarded or blind [165]. Clinical illness often has a low incidence rate and occurs intermittently [166].
11. TREATMENT
To treat toxoplasmosis, dihydropteroate synthetase and dihydrofolate reductase inhibitors are advised [167]. One of the dihydrofolate reductase inhibitors used to effectively treat this disease is pyrimethamine [168]. Additionally, medications like sulfamethoxazole and trimethoprim are used to treat this infection [165]. Almost all medications that are prescribed work best against the tachyzoite stage rather than cysts that contain bradyzoites [169]. Cysts remain latent in the retina or uvea, and bradyzoite reactivation is frequently seen in immunocompetent patients [32]. Oocyst eradication using a reliable treatment has not been documented.
Treatment for toxoplasmosis, which can sometimes harm the eyes, includes the use of pyrimethamine together with clindamycin or sulfadiazine [170]. The combination of pyrimethamine and sulfadiazine is thought to be helpful in cases of immune system deterioration. Sulfadiazine coupled with pyrimethamine is an alternative to it [171]. Additionally advised for the treatment of this condition are medications like pyrimethamine and trimethoprim-sulfamethoxazole [172]. In order to prevent parasite infections of host cells in immunocompromised hosts, vaccination is also advised [173]. Recombinant anti-Toxoplasma antibodies stop tachyzoite proliferation or early parasite invasion [174]. Although effective therapy has been reported, drug safety, duration of therapy, and drug potency are major concerns in the treatment of Toxoplasma infections [175]. Spiramycin is helpful for expecting mothers up until the 16th week of pregnancy, and different combinations of sulfadiazine, pyrimethamine, and folinic acid are advised [176]. Spiramycin has been frequently utilized to lower mother-to-child transmission [177]. Neonatal infections are treated with pyrimethamine and sulfadiazine [178]. However, the effectiveness of the drug is still unclear. Pyrimethamine, sulfadiazine, and corticosteroids have been reported to be particularly efficient for treating ocular toxoplasmosis [179].
12. PREVENTION
Toxoplasma transmission to humans can be avoided by thoroughly washing your hands with soap after handling meat, poultry, or shellfish [20]. It is also advisable to wash with soap and water any cutting boards, sinks, knives, or other items that come into contact with raw meat [180]. Washing is efficient because T. gondii stages in meat can be eliminated by exposure to soap and water [181]. Extreme heat or cold can cause T. gondii organisms in meat to perish [22]. Meat tissue cysts can be eliminated by either heating it to 67°C or cooling it to -13°C [182]. Toxoplasma in tissue cysts is also killed by exposure to 0.5 kilorad gamma irradiation [162]. The meat of any animal should be cooked to 67°C before consumption, and tasting the meat while cooking or when seasoning should be avoided [10].
Pregnant women must refrain from handling cats, coming into contact with soil, and consuming raw meat [183]. To prevent the spread of this parasite, pet cats should only be fed dry, tinned, or cooked food [106]. Daily cat litter box emptying is recommended, and pregnant women should avoid this [27]. Due to the danger of coming into contact with cat excrement, gardening gloves should be worn [97]. Vegetables should be washed thoroughly before eating because there is a possibility of being contaminated with cat feces when harvested [184]. The hazards of toxoplasmosis must be understood by expectant mothers [162]. As of right now, people cannot be protected against toxoplasmosis using a vaccination [185].
Health professionals should advise women of childbearing age about the spread of T. gondii [186]. Pregnant women should learn about food safety and, if at all possible, avoid contact with cat excrement at their first prenatal appointment, according to health professionals [162]. The creation of toxoplasmosis vaccines has advanced significantly in recent years, and a veterinary vaccine based on the live attenuated S48 strain was created [187]. However, this vaccination is expensive, has side effects, and has a short shelf life [185]. Furthermore, this vaccination might produce pathogenic strains, rendering it unfit for use in humans [46]. Numerous experimental experiments have demonstrated that it is feasible to create a vaccine to prevent human toxoplasmosis.
CONCLUSION
Toxoplasmosis is a dangerous threat to human health, especially for pregnant women. Diagnostic evaluation is very important for early detection, prevention of transmission, and, as a reference, treatment options for infected pregnant women. Currently, there is no vaccine to prevent toxoplasmosis in humans. Inhibitors of dihydrofolate reductase and dihydropteroate synthetase are recommended to treat toxoplasmosis. Washing your hands properly after handling meat, poultry or seafood with soap and water before performing other tasks will prevent the transmission of Toxoplasma to humans.
LIST OF ABBREVIATIONS
| OT | = Ocular Toxoplasmosis |
| TE | = Toxoplasmic encephalitis |
| PCR | = Polymerase Chain Reaction |
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
This study was supported in part by the Skema Penelitian Unggulan Airlangga (PUA) Universitas Airlangga Year 2023, Number: 1710/UN3.LPPM/PT.01.03 /2023.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

