All published articles of this journal are available on ScienceDirect.

A New Consistent Concept Between the I-change Model and the Transtheoretical Outcome to Imply the Leading Guideline of Depression Behavior Health Change Using Social Media
Abstract
Introduction
The number of patients suffering from depression is growing. It has become a serious global public health issue affecting individuals of all ages, contributing to the primary causes of disabilities and suicides. Therefore, proper care and treatment for patients with depression have become unprecedentedly important.
Objective
The main objective of this study was to present a new, consistent conceptual model for changing the health behavior of patients with depression using social media by combining factors from the I-change model theory with the transtheoretical outcome of behavioral health change and to present guidelines that have implications for practice.
Methods
The research design is quantitative, in which data are collected from a questionnaire according to the proposed conceptual model. One hundred and eighty patients with mild and moderate depression who were aged 18 years and over were recruited using simple random sampling, and the data were analyzed using structural equation modelling.
Results
The results of the study from the perspective of patients with depression found that all elements of the I-change model information, awareness, motivation, intention, and action can explain the consistent relationship between the I-change model factors and the transtheoretical outcome, which represents a related relationship in terms of theory.
Conclusion
Based on the transtheoretical model, the results can be translated into practice for changing health behavior in patients with depression, which may lead to guidelines for designing and implementing treatments targeting behavior modifications in such patients, their caregivers, and other parties involved. Guidelines based on the findings of this study can help reduce the risks of the use of social media in such patients and provide psychiatric knowledge to those involved in the treatment processes. Such guidelines may improve the effectiveness of treatment programs targeting behavior change in patient care.
1. INTRODUCTION
Many individuals have suffered from negative physical and/or mental well-being [1, 2], especially mental health issues (e.g., stress, anxiety, dread, and loneliness [1, 3]), due to the recent societal conditions and economies as well as the prevalence of diverse epidemics. Either of them can result in severe psychological or emotional symptoms [4-6] that, over time, become mental health disorders, such as a major depressive disorder (i.e., depression) [3, 7]. A report from the World Health Organization has found that depression is a global public health issue affecting people of all ages and a main cause of disabilities and suicides [8]. Specifically, it ranks as the second most common cause of mortality among people aged 15-29 years [9]. More than 280 million people around the world suffer from depression, yet the rate is still rapidly increasing [10]. In addition, the Department of Mental Health, in Thailand has indicated that 1.5 million Thais aged 15 and older suffer from depression, with only 28% of them having access to treatment, which causes more than 70% of Thais to die prematurely [11]. Depression is defined as a psychiatric disorder [12] in the Diagnostic and Statistical Manual of Mental Disorders and the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Two main symptoms have been indicated: depressed mood and loss of interest in hobbies due to intellectual disturbances. Depression is considered to be caused by biological, psychological, and social factors [13-15]. Numerous studies on predictors of depression have found that social media addiction is a robust indicator of mental health issues because this addiction affects daily behaviors (e.g., studying, working, interacting with people) and leads people to more risky behaviors till depression [8, 16-18].
Social media have become an important element in people's lives [8, 19] through various platforms, such as Facebook, Line, TikTok, Instagram, and Twitter [20, 21]. They serve as a dissemination tool for fostering trust in information about a variety of topics (e.g., health, sanitary safety, environment, entertainment, tourism) [22]. However, engaging in activities on social media for a long time may result in addiction [23-25]. Specifically, spending excessive time on social media may negatively affect the human body and mind, which, in turn, leads to depression [18, 26, 27]. A study on people with depression who are vulnerable to psychological stimuli showed that social media use could lead them to suicide [28]. It is an issue that has received a lot of study attention. Furthermore, by researching the link between social media and influencing the behavior of depressed patients, it was found that interfering with social media activities in various forms can affect the health behavior of patients with depression [29]. The research is a study of patients' intentions to change health behaviors through lifestyle intervention on social media. There will also be a presentation on the effects of content on social media, risks, relationships between factors, and behavior changes that may lead to suicide [30]. This reflects the relationship that social media has in affecting behavior change in patients with depression. Therefore, it is an issue that should be given importance and consideration in the care of patients with depression and various treatment methods appropriate to the patient according to the level of symptoms and severity of the disease.
Four types of treatments for patients with depression are pronounced: (a) medication, (b) transcranial magnetic stimulation [31], (c) electroconvulsive therapy [31, 32], and (d) psychotherapy [33, 34], which is a treatment method based on psychological theory. It is an important part of treatment for patients in addition to drug treatment. Treatment approaches that may be employed include cognitive behavior therapy, behavioral activation therapy, interpersonal psychotherapy, problem-solving therapy, non-directive counseling, and others, depending on the suitability of the patient's features [35, 36]. Through psychotherapeutic therapies that focus on behavioral modification, it helps to reduce the symptoms of depression. It enhances drug collaboration as well as reduces depression degeneration and recurrence. Based on research that has been studied on behavioral change, it will focus on bringing the theory of healthy behavior into the framework of the study of subjects. 1) Predicting health behavior using the theory of planned behavior (TPB) [37] and The Health Belief Model (HBM) [38], proposed by Rosenstock in 1974, is utilized to forecast women's intentions toward breast cancer screening. The predictors of smoking behavior are examined in adolescents using the Attitude-Social Influence-Self efficacy theory. (ASE) 2) A study of factors affecting behavior using a combination of prevention motivation theory (PMT) and a survey of Filipinos' opinions on the efficacy of various COVID-19 prevention methods [39] and the extended theory of planned behavior (TPB). 3) Behavioral modification patterns by evaluating preventive health behavior from COVID-19 based on a health belief model [40]. However, limitations were discovered because of the inability to explain relevant elements of the health behavior change process. From this limitation, the I-change model theory [41, 42] is introduced, a model that can describe factors that influence health behavior modification, which is largely the result of a comprehensive intention to predict future health behavior change [42]. There is research that studies the perspectives of the health behavior change process using the I-change Model theory of patients with depression and examining the impact of social media acceptance of lifestyle interventions on individuals' intentions to modify their health behavior [29]. The study's findings shed light on the elements that impact behavior change in depressed patients and their caregivers. The findings explain the link between the variables that influence intentions. In addition, there are studies that focus on information and risk factors in using social media that examine, utilizing the I-change model as a conceptual framework, the impact caused by content type, channel, source, and perceived privacy risk on alterations in health behavior change in depressed patients [30]. It was found that the I-change model theory is suitable for studying behavior modification in patients with depression, which is a complex behavior. However, from the study of related research it was found that most health behavior theories are abstract concepts, by testing the relationship of each factor within the theoretical framework. However, it has not yet led to concrete behavioral changes in the form of actual practice through various processes or steps to permanently change problematic behaviors and to result in the sustainability of behavior change.
The Transtheoretical model (TTM) is a theoretical idea that integrates various existing psychotherapy and behavior modification theories to be used to alter behavior based on the phases of behavior [43, 44]. In addition, by modeling the processes and stages in the form of practice, the six stages are Pre-contemplation, Contemplation, Preparation, Action, and Maintenance, until that leads to the termination step. This is the stage at which people are fully confident that they will not return to their old behaviors [43, 45]. Once successful in one step, it evolves into a change in the next step, into a continuously occurring behavior that becomes a new targeted behavior. From recent research work on theoretical models of behavioral modification, this has often been used as a line of thought in the design of programs to modify health behavior [46], such as Quitting Smoking [47], Food Control [48], Exercise [49]Sleep Behavior Adjustment [50] etc. These results are presented in the form of behavioral interference activity but have not yet been applied to complex behaviors and have not been analyzed for factors or causes that influence behavior change processes or for testing the relationship of variables that affect behavioral modification processes.
The study was specifically developed to address the existing gaps by developing a new conceptual model that shows the relationship between the components of factors within the framework of the I-change model theory, which includes information, awareness, motivation, intention, and action that influence the outcome of health behavior modification under the transtheoretical model of patients with depression caused by using social media, as well as to examine the relationship between factors using a structural equation model (PLSSEM) to produce such outcomes. The results reveal the relationship of factors between theories and demonstrate the importance of social media usage in influencing behavior change in patients with depression. This brings benefits to patients, caregivers, and those involved in applying the knowledge gained in designing guidelines for managing and designing treatment processes related to behavior modification for further patient care. It can also be further developed through an in-depth study of the TTM model to lead to a sustainable framework for changing the behavior of patients with depression by explaining the research objectives with the following research questions.
Research Question: What factors of the I-Change model affect and are consistent with the transtheoretical outcome for patients with depression from the use of social media?
2. THEORY AND LITERATURE REVIEW
2.1. Social Media with Depression
Social media is a digital tool used for a variety of activities, such as communicating, sharing news, exchanging opinions [51, 52], and doing business. Through research on popular platforms (e.g., Facebook, Line, TikTok, Instagram, Twitter) [52, 53] it has been found that social media have their benefits and disadvantages. In a study on health effects, it was found that activities on social media were an important predictor of individuals’ mental state and living in society [54] that led to depression [55-57], which may, in turn, result in suicide [26, 58]. As a result, additional research was conducted to validate these results. Similarly, the current study was divided into two components: (a) the correlation between social media use and addictive behavior, which, in turn, affects the course of depression, and (b) the association between social media use and the health behavior of individuals diagnosed with depression (Table 1).
| Author/Year | Context | Study Design | Statistical Analysis | Outcome Variable |
|---|---|---|---|---|
| [26] | Social media addictive behavior related to depression and suicide | Cross-sectional | Descriptive statistics, reliability, normality test, correlations (in SPSS), and structural equation modeling (in Amos) |
Depression and suicide |
| [17] | Social media use associated with adolescents' depressive symptoms | Cross-sectional | T-test, logistic regression, structural equation model (in Stata) | Depression symptoms |
| [27] | Social media use and depression | Cross-sectional | Multivariable logistic regression | Depression symptoms |
| [58] | The relation between addiction to social networking sites, moderation by self-esteem, and mediation by rumination | Cross-sectional | Descriptive statistics, Correlation (in SPSS), and regression (in SPSS PROCESS macro) | Depression |
| [29] | Social media lifestyle intervention and health behaviors change | Cross-sectional | Structural equation modeling (SEM) | Behavior Change |
| [56] | Facebook addiction, depressive symptoms, and behavioral health | Cross-sectional | Descriptive statistics (frequencies, percentages, means, and chi-square tests in SPSS) and logistic regression | Depression and Behavior Change |
| [57] | The relation between social media use and depression | Cross-sectional | Regression analyses | Depression symptoms |
| [24] | The relationship between depressive symptoms and social media and mobile device use | Cross-sectional | Structural equation modeling (SEM) | Depression |
| [59] | Depression, emotion regulation difficulty, social media use, and psychological distress | Cross-sectional | Descriptive statistics (correlations, t-tests, and one-way ANOVA) | Depression |
| [25, 60] | Whether Facebook could help with a community-based group intervention in lifestyles for those with serious mental illnesses | Cross-sectional | One-way ANOVA | Behavior changes (Weight loss and improved fitness) |
| [30] | Variables that affect health behavior changes in individuals with depression, including the effects of content, channel, source, and perceived privacy risks when utilizing social media | Cross-sectional | Structural equation modeling (SEM) | Behavior Change |
These studies show that information on the impact of social media use or lifestyle interference on psychiatric patients is increasingly presented today. This leads to social media relationships with patients with depression, which influence and lead to depression [16, 17, 20, 61] and influences the behavioral modification of depression patients [58, 62]. Research has confirmed that social media has entered a role and a major role in the daily life of patients with depression [63, 64], influencing intentions to act or modify health behavior on various issues [29, 65, 66]. Social media have been used as a medium to engage in groups and share health information [67, 68], and social media has transformed popular methods to promote health effectively, interacting through various channels [69, 70]. In addition, there has been an in-depth study of data, including content type, channel, and source, that can confirm that content received on social media affects the changing health behaviors of patients with depression [30]. Therefore, this research focuses on how information received from social media interventions will affect the process of changing health behaviors.
2.2. Health Behavior Theories
Health behavior encompasses health, actions, or expressions of human actions or inactions for health [71, 72] in the physical, psychological, and social aspects [73, 74] expressed to oneself, family, and community [75]. Health behavior can be divided into five categories: disease treatment, disease prevention, health promotion, health care participation, and consumer health protection [76, 77]. However, if any action is detrimental to one's health, one must find a way to change health behavior further [78, 79]. Presently, various concepts and theories are employed to elucidate behavior in order to understand healthy behaviors and health behavioral modifications [77, 80], and influential social psychological factors have been identified in individual health behavior [80, 81]. It can be divided into three levels: individual health behavior theory and model, interpersonal health behavior theory and model, and community and group health theories and models [77, 82]. The research focuses on the theory of personality that emphasizes the understanding of individuals that influence behavioral change, such as the health belief model (HBM) [38], which is a theory focused on various aspects of perception. It is a factor of belief that arises from the perception of something that influences healthy behavior. The results focus on disease prevention and treatment. The theory of reasoned action (TRA) [83] is a theory that studies healthcare intentions based on a person's behavior as the result of thinking and reasoning. The theory of planned behavior (TPB) [84] is a theory that studies behavioral change by intent and behavior control. A person's healthy behavior is the result of an intention to act that is influenced by beliefs about attitudes to behaviors, the influence of reference groups, and the perception of the ability to control behaviors. The Protection Motivation Theory (PMT) [39] uses a study of risk-prevention behavior. The ASE model [85] is utilized to explain health behavior by considering the factors of attitude, social influences, and self-efficacy. In addition, this theory considers perceived self-efficacy through behavioral intentions and actual behavior. The above theory focuses mainly on explaining factors [81], thus, the argument is that a factor focuses on the cognitive perspective and affects the health behavior of the person. However, there are limitations in each of these theories because they are unable to explain factors from the perspective of the health behavior change process. Furthermore, because of this, theories that are elected to be used should be in line with the goals of the studies and have sufficient complexities to explicate health behavior problems in a study on behavior modification processes. The concepts for explaining health behavior are summarized in Table 2.
| Theory | Description | Outcome Variable |
|---|---|---|
| Health Belief Model (HBM) | Study the relationship between the health behavior of an individual, focusing on the level of perception and understanding of health information generated by the individual. 1. Perceived susceptibility 2. Perceived severity 3. Perceived benefits 4. Perceived barriers 5. Cues to action 6. Perceived self-efficacy |
Preventive health behavior |
| Theory of Reasoned Action (TRA) | To study personal behavioral changes based on reasons for actions caused by 1. Attitude toward behavioral changes 2. Subjective norm |
Behavioral intention and behavior |
| Theory of Planned Behavior (TPB) | To study a person's behavioral changes caused by intentions leading to behavior caused 1. Attitude toward the behavior 2. Subjective norm 3. Perceived behavioral control |
Behavioral intention and behavior |
| Social-cognitive Theory (SCT) | To study behavioral changes resulting from learning by observation or modeling. Related factors include: 1) Personal 2) Environment 3) Behavior |
Behavior |
| Information Motivation Behavioral Skills Theory | To study a person's changing behavior, considering motivational information and behavioral skills that result in the individual's behavioral changes is important. 1) Information 2) Motivation 3) Behavioral skills |
- |
| Attitude-Social influences and Self-Efficacy | Use health-behavioral descriptions, considering the factors involved: 1) Attitude 2) Social influence 3) Self-efficacy |
Behavioral intention |
The I-change model [42].
Available online under the terms of creative commons Attribution 4.0 License.
2.3. I-change Model
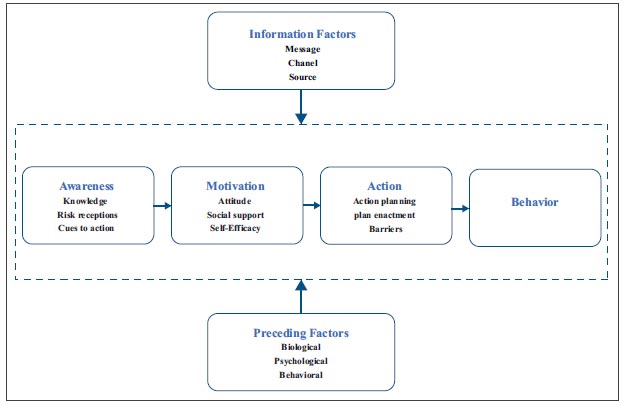
The I-change model (ICM) is a health behavioral theory that places emphasis on the consequences of intentions that lead to behavior changes [41, 86] with the relevant factors presented in each component. Part one is: 1) information factors (health-related information) evaluated from personal, message, channel, and source. Part two is: 2) about predisposing factors. Next, part three is represented in the form of processes but not as a practical process. It consists of three main factors: 1) awareness factors, assessed from knowledge, cues to action, and risk perceptions; 2) motivation factors, evaluated by attitude, social influence, self-efficiency, and action intention; and 3) action, planning, skill, and barrier until the result is in the behavior [29, 41, 42], as shown in Fig. (1). Within the theoretical framework, it illustrates the interconnections among each factor. The ICM theory is an extensively recognized concept utilized to influence health behaviors such as exercise, drinking alcohol [87], predictive smoking behavior [88], sleeping behavior [89], weight loss [90], eating behavior [91], and cyberbullying [92]. In each of the various health behaviors mentioned above, factors from the I-change model, including predisposing, information, awareness, motivation, intention, action, and behavior, were used for analysis. Different factors may be used in the analysis depending on the issues and goals of the work. The analysis is conducted in the form of logistic regression, multiple linear regression analyses, and structural equation modeling (SEM). Furthermore, ICM has been used for patients suffering from depression, which is a group with complex behavior. Moreover, by studying the intention to change health behavior, we can see how it is affected by accepting social media interference [29]. The results of the study revealed the factors that led to the intention to modify health behavior, which resulted in an explanation of only the relations between factors of the I-change model. Additionally, there was also a study using the I-change model that focused on information issues (e.g., content type, channel, source, perceived privacy risk) that influence changes in health behavior affected by social media risk factors among patients with depression [30]. The study found associations between content type, channel, and source and perceived privacy risk only under the theoretical framework of the I-Change model. In many studies, associations between factors within this theoretical framework were analyzed, which is a non-practical nature in explaining concepts. There has not been any research that has analyzed the elements of the I-change model, or each factor separately. Determine the relationship between each factor that influences the outcome of the health behavior change process.
2.4. The Transtheoretical Model
The transtheoretical model that describes the process of change in individual behavior [43, 94] passed through a six-stage implementation [44]. The first stage is re-contemplation, which means they are not planning to change their behavior in the next six months. Contemplation is confusion or thinking about change; preparation is moving towards change; action is attempting to change; and maintenance is a behavior change that can be maintained for more than 6 months and works to prevent relapse, leading to the termination phase. This is the stage where people are fully confident that they will not return to their old behavior [94-96]. Achieving success at each stage depends on individual variations. It involves emotions, cognition, behavior, social support, information received, etc [97]. Each step can change up and down over time based on a variety of factors. Many people change their desired behavior and soon return to their original behavior again. By changing successful behaviors, new behaviors should be sustainable [44]. TTM has become one of the most referenced and widely used models for health behavioral change interventions, it is clinically the most widely utilized in the field of mental health [95] and is effective in solving many problems, such as smoking [98-100] drinking alcohol [101] use of drugs, physical activity [49, 102] accepting and maintaining PA [103] weight control [104] medication adherence [105, 106] and contraceptive [107]. Several earlier studies have shown that the Transtheoretical Model (TTM) can be used to change behavior. Each work will focus on a different analysis model based on the main concepts of the TTM model, which include state of change, process of change, decision balance, and self-efficacy [44]. In the analysis, statistical principles will be used, such as correlation analysis, one-way ANOVA, and path analysis. Descriptive statistics and logistic regression analyses, etc, are also used to analyse health behavior. This model focuses on creating behavioral interventions at each stage [108]. In addition, TTM has been introduced for patients with behavioral complications, such as patients with combined depression and other disorders [108-110]. However, there are currently few studies for people suffering from depression. Moreover, by showing behavioral interventions through activities or methods in each step to treat and adjust patient behavior on issues such as eating, exercising, medication adherence, etc., and discovering research into how to use TTM as a framework to examine the structural relationships of the theory has been considered.
The I-Change and transtheoretical models incorporate health behavioral alterations employed in various subjects to target results in behavior change (see Items 2.3 and 2.4). The difference, however, is that the I-Change model is a conceptual theory which does not reflect the process or stage of behavioral modification (Table 3). Research related to the use of the I-change model has only described the factors and the relations between the studied variables. It explains the potential cause and effect between external and internal variables to assess the model's consistency with other relevant theories. It is a proof-of-concept examination of the relationships between each factor within the I-Change model. It has not led to actual implementation in the form of processes. No studies have analyzed each factor separately. In contrast, the transtheoretical model represents the process of behavior change and is characterized by the practice of the processes in five stages. When a person goes through a behavior change phase without a relapse, the person enters the final phase, i.e., termination, at which a person can change behaviors permanently. Research has focused on behavioral interventions using various methods in each step and has examined the structural relations of the theory by looking at behavioral interventions in each phase, wherein processes at each level are the results of the behavioral intervention within the framework of the model.
These comparisons show clear pictures of the I-change model, a theory integrating the relations between factors, and of the transtheoretical model, a theory that focuses on changing behavior practiced through various steps to lead to permanent and sustainable new behaviors. Therefore, this leads to a new idea that studies the relationship between the two theories. Additionally, by using the I-Change Model, each factor is separated into components to lay out their relation to the overall results of the health behavior change process under the theoretical framework of the transtheoretical model. A case study has been carried out of a group of patientswith depression from using social media. This confirms the relationship between the theory that is the conceptual model and the theory that models the process, leading to an in-depth study of the TTM model separately at each stage in the future.
3. PROPOSED RESEARCH MODEL AND HYPOTHESES
3.1. Proposed Conceptual Model
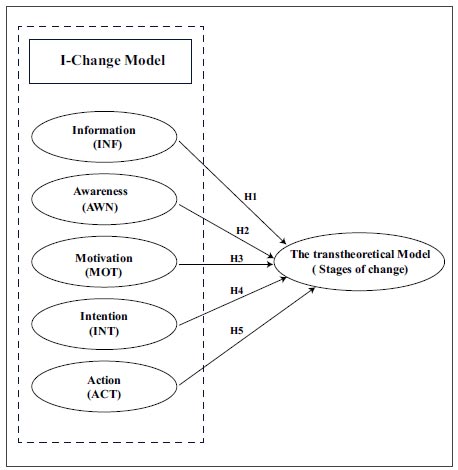
The examination of the elements that affect the health behavior change in people with depression is based on the effects of information, awareness, motivation, intention, and action, which are factors that can explain modifying health behaviors through integrating the TTM, which was used as a framework for the study as shown in Fig. (2).
3.2. Hypotheses
Predisposing factors were the basic data of the patients, which were divided into behavioral factors, psychological factors, social factors, and Environment factors [42], and these factors influenced the behavior of patients.(Huang, 2022; Keles et al., 2020, Shensa et al., 2018). For this study, the following baseline data were included: gender, age, education level, social media usage experience (hour), platform of social media use, and total time per day (hour).
| Theories | Definitions | Type | ||
|---|---|---|---|---|
|
Factors and Theory |
Process and Framework |
Practical Treatment | ||
| I-change model [42] |
It is a form of health behavior theory that explains changes in health behavior that result from motivation or intention. |  |
- | - |
| The transtheoretical model [44] |
It is a model that outlines the process of altering individual behavior at each stage, which results from a person's goal and preparedness to modify their own conduct. | - | |
|
| This Paper | A new consistent concept between the I-change model and the transtheoretical outcome to imply the leading guideline of depression behavior health change using social media | |
|
|
A proposed conceptual model.
An information factor is a description of information obtained from various sources. This focuses on information about health and behavioral modification. It consists of 1) personal factors. 2) message factors related to the content, type of content, frequency, quantity of content received, and quality of information. 3) channel factors: channel for obtaining health information; and 4) source factors: source for receiving health information. Recent research has demonstrated the relationship between the information or content received from social media, describing the relation between the quality of the information and the perception of the reliability of the source, which is important to the content shared on social media that influences individual perceptions [111, 112]. In addition to obtaining online health information, communicating health information on social media can lead to future behavioral changes [113, 114]. Moreover, research has confirmed the importance of information that influences behavior changes in TTM processes, such as eating behaviors and weight gain in young children [115]. Therefore, this study describes the information and advice received from social media about health behavior caused by group membership or obtaining information from various sources. The following is the assumption:
H1: Information factors have a positive effect on the patient's health behavior change process because of the social media use intervention.
Awareness factors are the factors that refer to awareness, which is the perception that self-behavior affects behavior [116, 117] and influences a person's behavioral motivation [42, 118]. These include 1) knowledge about such behaviors that cause harm to health [117], 2) risk perceptions are the perception of the symptoms, severity, and severity of the disease that affects health [119, 120], and 3) cues to action, events or alarms caused by close friends or people that cause a change in behavior or environment [90, 117-119]. Therefore, this study will focus on the advantages, disadvantages, and advice on the awareness of social media use that influences behavioral change caused by the following assumptions:
H2: Awareness factors have a positive effect on the patient's health behavior change process because of the social media use intervention.
Motivation factors are behavior-modification motivations [121] in which motivation factors are influenced by: 1) attitudes as perceptions of the advantages and disadvantages of behaviour [42, 90, 121], 2) social influences as norms or comments on such behaviours from intimate persons, which are important and motivating in behavioural modification [42, 119]); and 3) self-awareness as the perception of a person's level of ability in a situation or at the time of conduct, or confidence in his or her ability to conduct behavioral actions [122, 123]. Motivation influences a person's intention toward changing behavior [29] and is the determinant that causes action in a behavioral modification process. As a result, this study describes the motivation for health behavior change because of social media interference caused by the following assumptions:
H3: Motivation factors have a positive effect on the patient's health behavior change process because of the social media use intervention.
Intention factors are the intention to do something if referred to in terms of behaviour, it is the intent to modify a person's behavior [41], which is a post-motivation phase [29] that leads to those behaviors and involves the planning and implementation of a plan for targeted behavior [117, 124]. Furthermore, it mostly defines intention as the outcome of the work. This study examines the impact of social media interference on the patient's intention to change their health behavior.
H4: Intention factors have a positive effect on the patient's health behavior change process because of the social media use intervention.
Action factorss mention barriers, which are problems and constraints in behavioral modification, and are factors that may interfere with behavior adaptation, occurring between intentions and behaviors [125], which affects the achievement of health behavior goals [126, 127]. Therefore, this study will evaluate the involvement, problems, and barriers that affect behavioral modification caused by social media usage.
H5: Action factors have a positive effect on the patient's health behavior change process because of the social media use intervention.
4. RESEARCH METHODOLOGY
4.1. Study Participants and Setting
Moreover, to determine the sample group used for testing the hypothesis of the research, a total of 180 individuals were chosen for the sample group using the method of simple random sampling. This is how everyone in the population has the same probability of being randomly selected into a sample by using calculations from statistical formulas. In this research, the formula for calculating the size of the population according to the formula for finding the number of samples using the table of Krejcie & Morgan will select the sample group that meets the study's objectives, which were to primarily include patients who were diagnosed with mild to moderate depression. The sample utilized for this study was 180 patients with mild and moderate depression who were evaluated for depression symptoms using the 9-question (9Q) Depression Scale to determine the severity of symptoms at all 3 levels: mild, moderate, and severe in the 2 weeks preceding study participation. The results were evaluated by a psychiatrist, clinical psychologist, or psychiatric nurse. During the months of November 2022 and February 2023, data were collected from a facility in Thailand. All participants provided written informed consent before answering the question, and the study approach was authorized by Mahidol University's Centre for Ethical Reinforcement for Human Study (CIRB) with the reference number COA. No.MU-CIRB 2022/119.0711.
4.2. Data Collection
The questionnaire was developed in accordance with the Transtheoretical model and the I-change model. The questionnaire consists of three sections, from which thirty questions were selected to comprise the questionnaire. Section 1 outlines the information in general and social media use; Section 2 outlines the information, awareness, motivation, intention, and action factors; and Section 3 outlines the recommendations. The questionnaire replies were graded on a five-point Likert scale, with 1 being strongly disagreeing and 5 being strongly agreeing. The third section contains open-ended inquiries, including suggestions and recommendations.
Prior to commencing data collection, a clinical psychologist or psychiatric nurse conducted a Mental Status Examination (MSE) to evaluate the patient's level of awareness and ascertain their preparedness to respond to questions. After that, a clinical psychologist or psychiatric nurse read the questionnaire questions to the patient in a personal conversation with the patient in a manner like the therapy process to prevent possible questioning from provoking the patient's symptoms. In addition, it was also about observing and evaluating the situation. The clinical psychologist or mental nurse wrote down the patients' answers after talking with them to evaluate them and made sure they do not have to answer questions that could make their condition worse. This is also performed to evaluate the situation before the questionnaire phase. Each conversation lasts no more than 15 minutes (Table 4).
4.3. Data Analysis
In research, statistics are employed. It is a study of causal links using SmartPLS 4.0.9 [129] is utilized to analyze the partial least squares structural equation model (Partial Least Square Structural Equation Modeling). There are two types of analysis shown: measurement model analysis and equation model analysis structure [130].
5. RESULTS
5.1. Descriptive Statistics
A random sample of 200 persons who have been diagnosed with depression was recruited, and complete data were obtained from 180 participants. Table 5 displays the characteristics of the participants' demographics.
| Construct | Items | Questions | Source |
|---|---|---|---|
| Predisposing factors | - | Gender, age, education, social media usage experience, social media use platform, and total time per day (hour). | [20] |
| Information factors (INF) | INF1 | The information and health advice I get from my use of social media influences behavioral change. | [29, 30, 128] |
| INF2 | I get beneficial information and advice and support behavior change activities by joining groups and studying health facts through social media lifestyle interventions. | ||
| INF3 | The amount of content and health information I get from different sources through social media affects my health behavior. | ||
| INF4 | A warning about the health dangers associated with depression from social media affecting behavior change. | ||
| Awareness factors (AWN) | AWN1 | I understand the pros and cons of using social media that will affect my preparation for behavior change. | [29, 30, 129] |
| AWN2 | Social media use is beneficial for me and has resulted in behavior change. | ||
| AWN3 | I am aware about the pros and cons of using social media to join groups and look for health information about depression health information that promotes healthy behaviors. | ||
| AWN4 | I am aware of the serious effects thatabusive social media use may have on health-related behavior. | ||
| AWN5 | I am aware that social media's lifestyle interventions have an influence on healthy behavior. | ||
| Motivation factors (MOT) | MOT1 | Utilizing social media is one means by which I can acquire useful health information. | [29, 30, 128] |
| MOT2 | I think joining groups and searching for depression health information through social media is beneficial to health and behavioral change. | ||
| MOT3 | Experts, friends, and family members have all driven me to start a hidden group and investigate depression health information via social media treatments. | ||
| MOT4 | I think the support of professionals, friends, and relatives is an important and motivating part of behavior change. | ||
| MOT5 | I think joining groups and looking up depression health information is helpful to my health habits. | ||
| Action factors (ACT) | ACT1 | Social media lifestyle interventions, joining various groups from each fan page, and searching for health information about depression hinder initiatives to change health behaviors. | [29, 30, 128] |
| ACT2 | Cooperate in following expert advice on using groups and researching depression health information through social media interventions. | ||
| ACT3 | I cooperate in providing professionals with information relevant to my behavior. | ||
| ACT4 | I cooperate in following expert advice on healthy behavior change. | ||
| ACT5 | Lifestyle interventions on social media both by joining different groups and looking up health data about depression. It is a barrier to altering health-related behavior. | ||
| Intention factors (INT) | INT1 | Social media lifestyle interventions result in the intention to health behavior change according to the behavior change process. | [29, 30, 128] |
| INT2 | Being motivated plays an important role in bringing about intentions to change behavior. | ||
| INT3 | Social media lifestyle interventions, as a result, can help make initiatives and keep awareness of behavioral change can be made according to the behavior change process. | ||
| The transtheoretical model | TTM 1 | Do you think procedurally changing old, problematic behaviors is good for your health? | [128] |
| TTM 2 | Do you think that the process of modifying the original problematic behavior results in a continuous behavior change? | ||
| TTM 3 | Do you think that modifying the old problematic behavior according to the process results in new behaviors that are good for your life? |
| Characteristics | Patients (n=180) | |
|---|---|---|
| Number | Percentage | |
| Gender | ||
| Male | 74 | 41.11 |
| Female | 106 | 58.89 |
| Age | ||
| 18-25 | 57 | 31.67 |
| 26-35 | 74 | 41.11 |
| 36-45 | 34 | 18.89 |
| 46-55 | 12 | 6.67 |
| 56 years and above | 3 | 1.66 |
| Education level | ||
| Secondary school level or less | 47 | 26.11 |
| College degree | 35 | 19.44 |
| Bachelor's degree | 85 | 47.22 |
| Postgraduate degree | 13 | 7.22 |
| Social media usage experience | ||
| Less than 1 year | 0 | 0.00 |
| 1-3 years | 0 | 0.00 |
| 3 years and above | 180 | 100.00 |
| Platform of social media use | ||
| 67 | 37.22 | |
| 12 | 6.67 | |
| 7 | 3.89 | |
| Line | 30 | 16.67 |
| YouTube | 10 | 5.56 |
| TikTok | 54 | 30.00 |
| Total time per day (hour) | ||
| Less than 1 hour | 27 | 15.00 |
| 1-3 hour | 63 | 35.00 |
| 3-5 hour | 54 | 30.00 |
| 5 hour and above | 36 | 20.00 |
Table 5 shows the demographic characteristics, revealing that 58.59% of participants were female, 41.11% were between the ages of 26 – 35 years, and most of them had a bachelor's degree. Most of the samples, which made up 47.22 percent, had used social media for more than 3 years. Facebook was the most used social media, with 37.22 percent, and 47.22 percent of the time was spent on social media for 1–3 hours, which accounts for 35%.
5.2. Measurement Model
The examination of variable quality was conducted based on the criteria outlined in a study [130] and the questionnaire's measurement list of questions. According to the findings, all composite reliability (CR) values fall within the range of 0.884–0.942, and this fits the criteria of not being less than 0.7. Similarly, Cronbach's α values range between 0.882 and 0.938, also meeting the criterion of not being less than 0.7. Additionally, the average variance extracted (AVE) values ranged from 0.711 to 0.809, which is greater than the 0.5 minimum criteria, as shown in Table 6.
The following is a compilation of inquiries utilized in quality assessment surveys, satisfying all requirements pertaining to weight values. The dependability of the question list used in educational measurement is demonstrated by considering a value that is equal to or greater than 0.7 based on specific criteria. The set of questionnaires exhibited a weight outer loading ranging from 0.800 to 0.926. Additionally, the Fornell-Larcker criteria were employed [35], for evaluating the relationship between variables in the form of a diagonal matrix, it was found that the square roots of AVEs in each variable (bold letters) are greater than the corresponding horizontal and vertical values. This shows that the interpreter had discriminant validity and can be used for structural equation model analysis, as shown in Table 7.
| Constructs | Items |
Outer Loading (>0.70) |
Cronbach's α (> 0.70) |
Composite Reliability (> 0.70) |
AVE (> 0.50) |
|---|---|---|---|---|---|
| Information | INF1 | 0.800 | 0.898 | 0.905 | 0.711 |
| INF2 | 0.858 | ||||
| INF3 | 0.866 | ||||
| INF4 | 0.869 | ||||
| INF5 | 0.821 | ||||
| Awareness | AWN 1 | 0.822 | 0.915 | 0.918 | 0.746 |
| AWN 2 | 0.855 | ||||
| AWN 3 | 0.883 | ||||
| AWN 4 | 0.883 | ||||
| AWN 5 | 0.875 | ||||
| Motivation | MOT1 | 0.850 | 0.938 | 0.942 | 0.801 |
| MOT2 | 0.920 | ||||
| MOT3 | 0.889 | ||||
| MOT4 | 0.896 | ||||
| MOT5 | 0.919 | ||||
| Intention | INT1 | 0.861 | 0.923 | 0.925 | 0.765 |
| INT2 | 0.857 | ||||
| INT3 | 0.885 | ||||
| INT4 | 0.894 | ||||
| INT5 | 0.875 | ||||
| Action | ACT1 | 0.874 | 0.934 | 0.936 | 0.746 |
| ACT2 | 0.894 | ||||
| ACT3 | 0.904 | ||||
| ACT4 | 0.891 | ||||
| ACT5 | 0.884 | ||||
| TTM | TTM1 | 0.899 | 0.882 | 0.884 | 0.809 |
| TTM2 | 0.926 | ||||
| TTM3 | 0.874 |
| Construct | AWN | ACT | INF | INT | MOT | TTM |
|---|---|---|---|---|---|---|
| AWN | 0.864 | - | - | - | - | - |
| ACT | 0.413 | 0.890 | - | - | - | - |
| INF | 0.681 | 0.585 | 0.843 | - | - | - |
| INT | 0.558 | 0.836 | 0.677 | 0.875 | - | - |
| MOT | 0.599 | 0.513 | 0.688 | 0.626 | 0.895 | - |
| TTM | 0.521 | 0.791 | 0.647 | 0.763 | 0.598 | 0.900 |
| Hypothesis | Relationship | Patients (n= 180) | Supported | ||||
|---|---|---|---|---|---|---|---|
|
Coefficient (β) (>0.1) |
p-value (<0.05) |
t- value (>1.96) |
VIF (<5.00) |
Q2 | |||
| H1 | INF -> TTM | 0.156 | 0.017* | 2.379 | 1.917 | 0.751 | Supported |
| H2 | AWN -> TTM | 0.112 | 0.037* | 2.091 | 2.312 | Supported | |
| H3 | MOT -> TTM | 0.236 | 0.016* | 2.401 | 1.467 | Supported | |
| H4 | INT -> TTM | 0.175 | 0.000** | 1.983 | 2.589 | Supported | |
| H5 | ACT -> TTM | 0.368 | 0.000** | 3.532 | 2.459 | Supported | |
Model testing results.
5.3. Structural Model
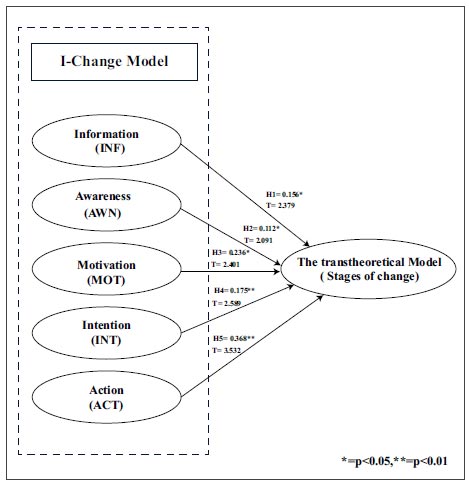
Subsequently, the structural model should be validated by employing the bootstrap approach on resampled patient data with 5,000 lists, to enhance the reliability of examining the associations among components. Multicollinearity tests were conducted using VIF values, revealing that the causative variables exhibit no correlation over the threshold of 5 [131]. When evaluating the importance of path coefficients, p-values and t-values are examined based on predetermined thresholds. These thresholds are set at t-values greater than 1.96 (at a significance level of 5%), 2.58 (at a significance level of 1%), and 3.29 (at a significance level of 0.1%) [131]. Furthermore, it was found that accepting hypotheses H1: Information Factors (INF) had a positive effect on the transtheoretical model (TTM) outcome at the significant level 0.05 (β = 0.156, t=2.3). Accepting H2: Awareness (AWN) had a positive effect on that the transtheoretical model (TTM) outcome at the significant level 0.05 (β = 0.112, t=2.091). Accepting H3: Motivation (MOT) had a positive effect on that the transtheoretical model (TTM) outcome at the significant level 0.05 (β = 0.236, t=2.421). Accepting H4: Intention (INT) had a positive effect on the transtheoretical model (TTM) outcome at the significant level 0.05 (β = 0.047, t=1.983). Accepting H5: Action (ACT) had a positive effect on the transtheoretical model (TTM) outcome at a significant level 0.01 (β = 0.368, t=3.532). The results are shown in Table 8 and Fig. (3).
| Construct | R-Squared | Adjusted R-Squared | SRMR | GoF |
|---|---|---|---|---|
| The transtheoretical model (TTM) | 0.776 | 0.769 | 0.050 | 0.769 |
5.4. Model Fit
Moreover, to determine model fit, all model structures proposed were evaluated. The outcomes of the model's goodness of fit analysis can be categorized into three components [132]. The first component is the determination coefficient (R2), with the criterion that the model is unacceptable if the determination coefficient (R2) is less than 0.19. If the value falls between 0.19 and 0.33, the low-level performance of the model is acceptable. If the value is within the interval of 0.33 to 0.67, the model's acceptability can be deemed moderate. On the contrary, when the value surpasses 0.67, the model's acceptability can be deemed to be at a good level. The present study revealed that the endogenous variables, namely the transtheoretical model (TTM), exhibited an R-squared value of 0.776. It is noteworthy that the R-squared values surpassed the required threshold, therefore showing that the model adequately reflected the gathered data. This observation suggests a good fit for the model, as depicted in Table 9. The second component is concerned with the Standardized Root Mean Square Residual (SRMR) measure, which should not exceed 0.08 [133, 134], with an SRMR value of 0.050 being acceptable. The third component is the Goodness of Fit (GoF) value, which is derived by taking the square root of the product of the average determination coefficient (R2) and the average variance extracted (AVE). The acceptable bounds for the GoF value are as follows: less than 0.1, signifying no fit; between 0.25 and 0.25, signifying a moderate fit; and greater than 0.36, signifying a high fit [135]. Exploiting the same measurement technique is based on defined methods and results [136-138]. The outcome of this experiment yields a substantial Goodness-of-Fit (GoF) rating of 0.769. The result of the goodness-of-fit (GoF) may be computed using the equation shown as Eq. (1).
 |
(1) |
6. DISCUSSION AND COMPARISONS BETWEEN A PROPOSED RESEARCH MODEL AND PREVIOUS WORKS
This study is the first study to present a new model to explain the relation between the I-change model and the TTM in behavior modification for patients with depression from social media use. Furthermore, the relationship was analyzed by PLS-SEM with factors within the framework of these theories. It comprises information, awareness, motivation, intention, and action, which are factors that influence behavior change. Moreover, by analyzing the relations of these factors to the process of behavioral modification under the TTM and testing behavioral change in the new conceptual framework, the relations between factors of these theories will benefit future studies on the processes of behavioral change. Likewise, it is worth noting that more than half of the patients were female (58.9%). Through surveying social media use, it can be concluded that most patients have more than 3 years of social media experience. The most popular social media users are on Facebook (37.2%), and the time spent on social media, on average, is 1-3 hours (35%). Based on the model results shown in Fig. (3), the perspective of patients with depression on their behavior in using online social media is consistent with the hypotheses of this study, and it can be explained that the factors of the I-change model in each construct are considered significant to the TTM, respectively, with all factors showing statistically significant paths to the TTM outcome and thus linking the two theories.
While the results of the analysis of each construct of ICM found that the information factor was positively related to the behavior change process (TTM), as shown in Fig. (3), this is consistent with past studies that have described information and recommendations regarding the health received, affecting behavior change [113, 114, 139]. Moreover, if a patient gets information from social media that results from the exchange of health information between them by joining a health group or getting information from published pages that are quality, useful, and reliable information with clear channels and sources, it will have a positive effect on the patient's health behavior [30, 140]. and patient behavior modification as well [141, 29, 90, 114]. There is research that confirms the importance of information that influences behavioral changes in TTM processes, such as eating behavior, and weight gain in young children [115]. Therefore, information is an important part of the early stages of a patient's behavioral change process, and it will play a key role in supporting ideas to adjust their own behavior as a problem.
Then, as shown in Fig. (3), awareness factors have a statistically significant positive affect on the transtheoretical outcome of behavioral health change, which is evaluated from knowledge, risk perceptions, and cues to action. Research shows that if a patient has increased awareness of the knowledge acquired, the pros and cons of problematic behavior, as well as the perception of the risks and violence that will arise from the use of social media, it will lead to an incentive to modify behavior [91, 121, 142]. This is consistent with numerous studies demonstrating the significance of awareness in influencing health behaviors [29, 41, 92, 118], such as eating [91]and sleeping [143]. Therefore, if patients have knowledge and awareness of the risks that affect their health from using social media, it will have a positive effect on the behavior change process at the stage of taking the initiative to change behavior.
The motivation factor, as shown in Fig. (3), has a positive and statistically significant effect on the transtheoretical outcome of behavioral health change in patients with depression. In particular, patients perceive the benefits of using social media as a channel that helps them receive useful health information [144]. Furthermore, having a positive attitude toward the health-risk behaviors of patients will help create more motivation to change their health behaviors [28, 91, 117]. Similarly, the influence of intimate people, friends, and relatives who play an important role in targeted behavioral modification [119], affecting the patient's intention to modify behavior and leading to plans for further behavioral modification is demonstrated in a study. This can be summarized by the importance of motivation that influences health behavior modification through behavioral modification processes [48, 145]. Therefore, patients should be encouraged to see the importance of healthy behavior by developing a positive attitude towards accepting social media interference that affects action in the transtheoretical model.
Furthermore, in Fig. (3), on the intention factor, there is a statistically significant positive effect on the transtheoretical outcome of behavioral health change in patients with depression. The results of the research show that the intention to modify behavior is due to the fact that the patient is planned and executed accordingly to the goal of targeted behavior [117, 124]. Consistent with past studies that studied the intentions of depressed patients from social media lifestyle interventions that influence behavior [29] and an in-depth study of information (content type, channel, source) and perceived privacy risk from the using social media that affect health behavior change [30]. The above-mentioned information shows the importance of the intention factor that will lead to changing the behavior of patients and affect the process of changing behavior in the preparation stage for entering the next stage of practice.
The last section, action factor, shown in Fig. (3), shows the importance of barriers in affecting behavior change (Paterson et al., 2019) by interfering with social media usage. It is a major obstacle to changing the health behaviors of patients [147], affecting the process of behavior change [147, 148]. by affecting initiative consideration, planning, and behavior change in the initial period and the long term. If the patient is addicted to social media, spends time immersed in social media, or receives information that is not useful [149], it causes obstacles to behavior change and will affect the behavior change process in the action stage.
From the results mentioned above, the relationship between the elements of the I-change model and each of the elements that affect the transtheoretical model in modifying the behavior of depression patients from social media usage is shown in Fig. (3). The results can be applied to the benefit of patients, caregivers, and those involved in the treatment of patients who understand the relationship and influence of social media use that affects the disease and patient behavior, leading to guidelines to prevent risks from social media usage by patients. Moreover, the results can be used as a guideline for those involved in building knowledge in psychiatry. This will result in the behavior modification process, which is one of the most effective method of treating patients. Therefore, obtaining information and knowledge about the use of social media that demonstrates its advantages and disadvantages is important. It will help patients become more aware of the social media used in ways that are beneficial to their own health behaviors and lead to a change in behavior for the better. As a result, patients are motivated and have intentions to change problematic behaviors according to the steps in the health behavior change process. The results can be further studied in detail in the behavior change process at each step, and to lead to a conceptual framework for sustainable health behavior change.
7. THEORETICAL, PRACTICAL IMPLICATIONS AND FUTURE RESEARCH
From the results shown in Fig. (3), it is possible to confirm the new relationship between the components of the I-change model that is consistent with the overall results of TTM in changing health behaviors using social media among patients with depression. The results can be explained and extended from the form of structural equation modeling to practical guidelines that are consistent with the objectives and questions of the research. From Table 10, the factors of the I-change model are shown in each component, which is described using examples of social media usage behavior. The information factor is the first component of the I-change model, encompassing content, channel, and source. In this case, we receive information from social media by reading information from various pages related to depression. Joining various groups related to depression will allow the user to receive information and exchange information, either from a group of patients or experts. There are various forms of social media, including Facebook, Line, Instagram, TikTok, etc. Moreover, the awareness factor described in this study is receiving knowledge and advice about depression or ways to change behavior from using social media through various channels, which will help increase awareness and recognize the benefits of using social media that affect health, and recognize the risks from inappropriate use of social media to prevent harm from using social media as well. The motivation factor describes a positive attitude towards using social media and receiving social influence from peopleon social media, experts, or various influencers through joining groups and following pages through various channels can inspire health behavior change. Next is the intention factor, which is related to and influenced by motivation and is a result of using social media. This is a stimulating part that leads to the intention of depressed patients to change their behavior.
The last component is the action factor, which focuses on managing obstacles that may occur in changing behavior, by practicing and planning setting goals to maintain the continuity of newly adopted behavioral changes. From the above, the components of the I-Change model are explained in each factor of the social media use behavior of patients with depression. It will be related to the results of the TTM model on behavior change. This will lead to an in-depth study of the behavior change process in each next step that consists of pre-contemplation, contemplation, preparation, action, and maintenance to lead to guidelines for managing and designing treatment processes related to behavior modification and the development of a framework for sustainable behavior change in patients with depression caused by intervention in social media use, which are described in detail in Table 10. For further research,to maximize the benefits of behavioral modification, further in-depth studies should be conducted at each stage of the behavior change process to identify what factors are causing or triggering permanent behavioral change, and they should be superimposed on conceptually modeled outcomes to develop in the form of a framework, to show that all the relevant components of behavior modification can be applied as guidelines in patient care or treatment undertakings, which have an impact on flexibility in behavior change.
Table 10.
| Type of Social Media | I-change Model Theory | ||||
|---|---|---|---|---|---|
| Information | Awareness | Motivation | Intention | Action | |
| - Feed news Various groups - related to depression - Facebook fan page of a person or organization created to provide information about depression. |
- Knowledge of depression. - Being aware of the advantages and disadvantages of using social media. - Being aware of the risks of using social media to follow people, pages, or join groups. - Being aware of the benefits of tracking the pages of individuals or groups that provide information and knowledge or sharing information among groups of people with depression. - Being aware of the risk of using social media for a long time. |
- Have a good attitude towards using social media. - Receive support from people around you, experts, or various influencers. - Get inspiration from people on social media, experts, or various influencers when using social media. |
Tracking individuals or influencers from pages and groups with the same behavior stimulates the intention to change behaviors. | - Plan a daily schedule and set times for using social media. - Join groups on social media to get information and exchange information with others. - Find alternative activities to avoid spending too much time on social media. |
|
| Line | - Line group - Line open chat - Line Official Account (OA) |
||||
| - Tracking pages or individuals to track information about topics of interest or relevance |
|||||
| TikTok | - Following a page or person to obtain information - Feeding information |
||||
 |
|
|
|
|
|
|
Theoretical, Practical, and Managerial Implication of the TTM Model According to the results of the above study on the use of social media by patients with depression, we can translate the results into practical implications of the process of changing health behavior in patients with depression according to the steps of the transtheoretical model to lead to guidelines for managing and designing treatment processes related to behavior modification. |
|||||
CONCLUSION
This study shows a new consistent concept between the I-Change and the TTM outcome in changing the health behavior of patients with depression because of using social media. The results of the research presented through a conceptual model in the form of structural equations found that all factors of ICM, namely information, awareness, motivation, intention, and action, were significant with the transtheoretical model (TTM). This shows the relationship between ICM theory in a non-practical form that explains the relationship of each factor within the framework of theory, which is related to TTM theory, which is a practical theory . From such results, the relationship between the theory and the importance of using social media has also influenced the modification of the behavior of a depressed patient. Such findings can lead to further study of the process of behavioral modification in each step to analyze the factors that influence each stage of behavioral modification, and to intervene in a manner that is appropriate to each individual depression patient, as well as to establish a sustainable working framework for the adjustment of depression patients' behaviors.
The limitation of this study is that the grouping of samples are not yet grouped to separate the analysis by the severity of different depressive symptoms, which may lead to a study result that can describe patient behavior more clearly and a lack of behavioral analysis of specific health problems in each case, such as not to take medication behaviors, eating behaviors, and sleeping behaviors. Furthermore, it makes the data analysis more clear, and this has been beneficial for applying data to more targeted problem-solving interventions. In addition, we focused on patients with depression. If these participants could have been categorized by symptom levels, we may be able to see the differences by group, which will lead to more helpful results. Finally, the variation of age may have affected the thoughts or actions of people in each age group.
AUTHORS' CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to itssubmission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| TTM | = The Transtheoretical Model |
| ICM | = I-change Model |
| SEM | = Structural Equation Modeling |
ETHICS APPROVAL AND CONSENT PARTICIPATE
This study was approved by the Institutional Review Board of Mahidol University, which authorized the questionnaire and assigned it the approval number COA.MU-CIRB 2022/119.0711.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All participants provided written, informed consent before answering the question in this study and voluntarily participated after the researcher assured them of anonymity and that their responses were solely for academic purposes
AVAILABILITY OF DATA AND MATERIALS
The data analyzed in this study cannot be shared publicly because of the Personal Data Protection Act and is managed by the Institutional Review Board of Mahidol University, which authorized the questionnaire and assigned it the approval number COA.MU-CIRB 2022/119.0711 only.

