All published articles of this journal are available on ScienceDirect.

Exploring Anti-vaccination Beliefs among the Youth Population: A Comprehensive Validation of the Arabic VAX Scale for In-depth Attitude Analysis
Authors Info & Affiliations
Abstract
Background
The rise of anti-vaccination sentiments among the youth has become a significant public health concern, highlighting the need for effective tools to understand and address these beliefs.
Aims
This research introduces the Arabic VAX Scale, designed to assess and analyze the complex attitudes towards vaccinations within Arabic-speaking populations.
Methods
A cross-sectional study was conducted among undergraduate students from different disciplines in governmental universities in Riyadh, Saudi Arabia, between November 2020 and August 2021.
Results
The translated questionnaire was piloted among 39 Arabic-speaking participants. Subsequently, it was electronically sent to 2000 undergraduate university students attaining 319 complete responses. Majority were females (69.3%; n=221), averaging 21.6±2.7 years. The factor analysis of VAX-AR questionnaire loaded fittingly on the four subdomains previously defined in the original VAX questionnaire. The reliability analysis revealed a Cronbach's α score of 0.70 – 0.88 for all subdomains. Higher VAX-AR scores reliably correlated with negative behaviors and attitudes towards Flu, COVID-19, and mandatory vaccinations (p<.001). Anti-vaccination ideas stemming from religious beliefs were associated with ideas pertaining to the commercial profiting.
Conclusion
VAX-AR scale has good validity and reliability scores and can be used to assess the prevalence of anti-vaccination beliefs and ideas in Arabic-speaking populations.
1. INTRODUCTION
Infectious communicable diseases have burdened health by increasing mortality and morbidity [1]. With the emergence of vaccines and the implementation of vaccination programs, diseases have been eradicated [2]. Vaccines are considered cost-effective for disease prevention and health promotion [3]. However, in recent years, it has been noted that the number of unvaccinated children is on the rise [4]. According to the World Health Organization (WHO), vaccination coverage dropped from 86% in 2019 to 83% in 2020 [5]. This global drop in immunization coverage has led to the re-emergence of vaccine-preventable diseases [6]. Ironically, the very success of vaccination programs seems to undermine their perceived value by the public, as their benefits become less visible.
Vaccination programs can be affected through the spread of public misbeliefs regarding vaccines' safety, efficacy, or distrust in the production process. These misbeliefs usually rely on spreading misinformation regarding vaccines, which leads to vaccine hesitancy [7, 8]. Vaccine hesitancy is a delay in accepting or refusing a vaccine despite its availability [9]. In Saudi Arabia, a study found that 20% of parents are hesitant to vaccinate their children claiming that vaccines are not essential or effective [10]. These anti-vaccination beliefs will lead individuals to abstain from getting the required vaccines for themselves and their children despite the risk of morbidity and mortality associated with preventable infectious diseases [11-13]. Understanding anti-vaccination beliefs and attitudes compromise the first step towards implementing further measures to boost vaccination adherence and promote public health.
Multiple questionnaires have been designed to assess vaccine hesitancy and anti-vaccination beliefs. Some questionnaires are directed toward special groups or vaccines, such as Parent Attitudes about Childhood Vaccines (PACV), Vaccine Hesitancy Scale, and Attitudes and Behaviors Regarding Vaccination Decisions [14, 15]. Recently, a scale was constructed focusing on individuals' anti-vaccination beliefs; the Vaccination Attitude Examination (VAX) Scale [12, 16]. Through the VAX scale, concerns about vaccine efficacy and safety are probed, and also concerns about commercial profiting and preference for natural immunity. To our knowledge, the VAX Scale had not been translated into the Arabic language.
In this study, we aim to translate the VAX questionnaire into Arabic and measure the prevalence of anti-vaccination ideas among undergraduate students in Riyadh, Saudi Arabia. Acknowledging the dominant conservative religious background of the Saudi population, and because an association has been noted in some studies between conservative religious backgrounds and vaccination hesitancy, we explored the value of integrating religion-focused inquiries into the original set of 12 VAX questions. This was done to investigate whether religious beliefs constitute a distinct sub-scale influencing vaccination attitudes [17].
2. MATERIALS AND METHODS
2.1. Study Design, Area, and Settings
This was a cross-sectional survey-based study utilizing a translation of the VAX questionnaire to the Arabic language (VAX-AR) that was produced as part of this effort. Arabic translation, piloting, and reliability testing of the VAX-AR were conducted between November 2020 – January 2021. Subsequently, validation was performed between March 2021 to August 2021 through a cross-sectional study among undergraduate students from governmental universities in Riyadh, Saudi Arabia. (Fig. 1). The study underwent three phases: Phase 1: adaptation, translation from English to Arabic, and content validation of the translated Arabic VAX questionnaire (VAX-AR). Phase 2: a pilot study of the VAX-AR version. Phase 3: psychometric evaluation of the VAX-AR version. Sample size calculation was performed Using the Roasoft online sample size calculator (roasoft.com) for a population size of more than 200,000 and an estimated response distribution of 30% [5]; yielding a needed sample of 318 participants to achieve prevalence inference with a 5% margin of error and 95% confidence interval.
2.2. Adaptation, Translation of the Questionnaire, and Content Validation
The original English VAX questionnaire was adopted [10]. The VAX is a 12-item questionnaire categorized into four different domains; 1) Mistrust/trust in vaccine efficacy, 2) Worries about unforeseen effects, 3) Concerns about commercial profiteering, and 4) Natural immunity preference. Each item was scored from 1 to 6, where one means strongly disagree, and six means strongly agree. A higher score reflects stronger beliefs in anti-vaccination ideology. Notably, the first domain had a reverse direction; hence a reverse code adjustment of its score was performed for ease of understanding and analysis. Afterward, the translation of the original English questionnaire into the Arabic language was performed. Utilizing the forward-backward translation method, one of the research team members (M.F.S) translated the questionnaire to the Arabic language and then it was subsequently translated back to English and reviewed by two other personnel - a language and medical experts - that were blinded to the initial translation process to obtain face validity (Appendix 1).
The authors added two novel religious questions to capture and assess the relevance of the religious anti-vaccination beliefs dimension, given the conservative religious views of the Saudi population. The two questions were: 1. I am concerned that vaccines may contain religiously forbidden materials. 2. Vaccinations contradict the belief that Allah (God) is the ultimate protector, so they are not needed. All questions have Likert-scale answers 1-6 (strongly disagree – strongly agree), similar to the rest of the 12 original questions (Appendix 2).
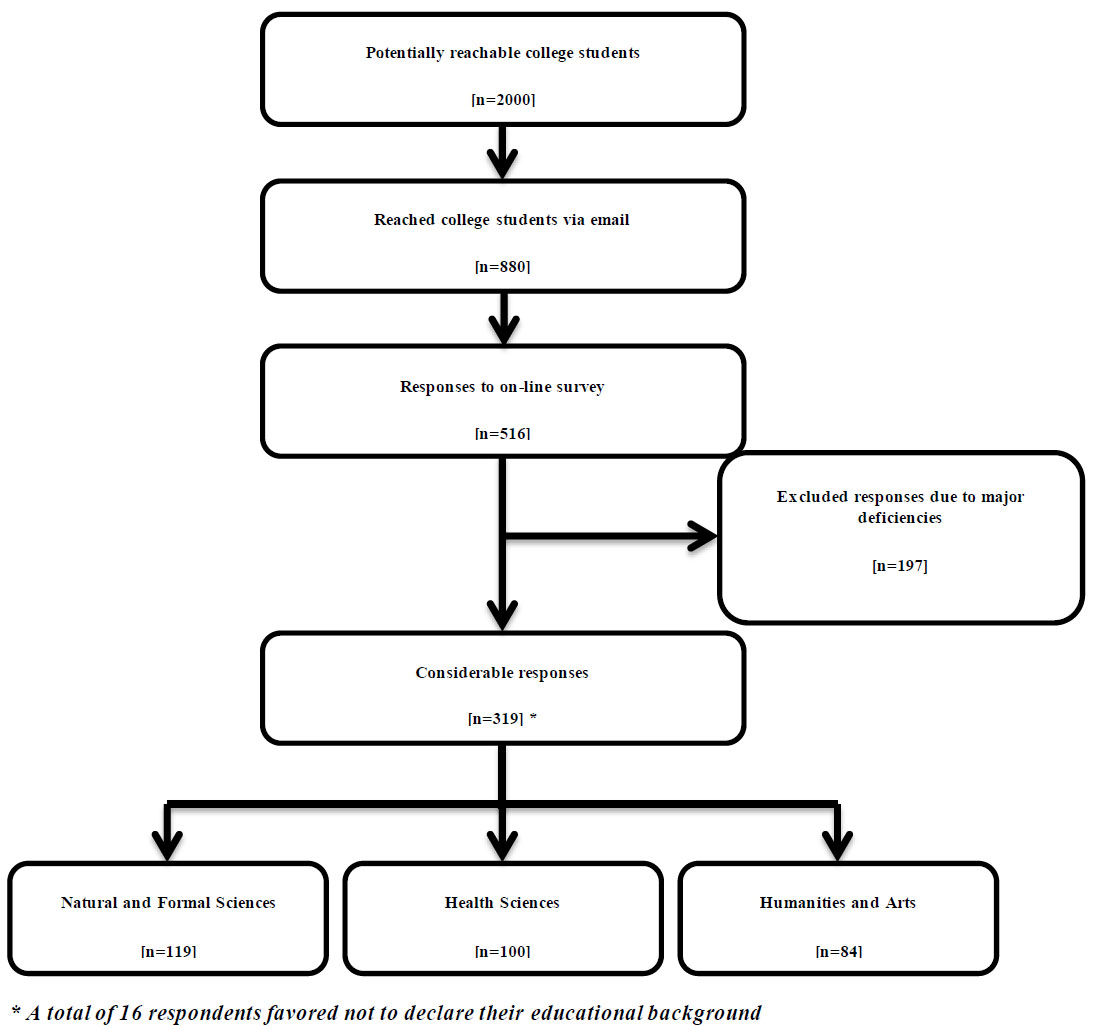
Population flowchart.
2.3. Piloting, Field Testing, and Psychometric Evaluation of the VAX-AR
The VAX-AR was first piloted to ensure its validity and readability. An online version of the questionnaire was made available. A convenient sample of undergraduate medical students studying at different governmental universities was approached and asked to fill out and distribute the questionnaire to friends and family to allow for snowball recruitment. A target of 30 responses was desired, corresponding to about 10% of the needed sample size.
After finalizing the VAX-AR, undergraduate students in three public governmental universities in Riyadh, Saudi Arabia, were targeted. The included universities were [1] Princess Nourah bint Abdul Rahman University (PNU) [2], King Saud University (KSU), and [3] Imam Mohammad Ibn Saud Islamic University (IMSIU). Three colleges were purposefully selected per discipline. College of Engineering, College of Basic Sciences, and College of Computer Science to represent the discipline of Natural and Formal Sciences. College of Law, College of Media, and College of Business to represent the disciplines of Humanities and Arts. College of Medicine, College of Nursing, and College of Applied Medical Sciences to represent the discipline of Health Sciences. At the time of sampling, national restrictions related to the Coronavirus (COVID-19) pandemic continued to take effect in public universities. Principally, all classes were held virtually with minor exceptions. Hence, all communications were done through emails, which included the initial request to participate in the study, fill the survey and subsequent two reminders. The following data were asked from all respondents [1]: age and gender [2], current college [3], time spent reading the daily news [4], flu vaccination status [5], COVID-19 vaccination status [6], VAX-AR questionnaire with the addition of the two novel questions (Appendix 1 and 2).
2.4. Statistical Analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) v. 27 and AMOS v26 for structural modeling (Chicago, IL, USA). The data were screened for missing answers, and only responses with complete VAX-AR responses were considered. The descriptive data were presented as mean ± standard deviation for continuous variables and categorical variables as counts and percentages.
Principal factor analysis was used to examine the scale's construct, validity, and dimensionality. Promax rotation was utilized to tease out the dimensions/domains. Confirmatory analysis was performed using structural modeling. The Kaiser-Meyer-Olkin (KMO) measure value was used to determine sampling adequacy, and Bartlett's test of sphericity was used to assess data suitability. A KMO of at least 0.6 and a significant Bartlett's test of sphericity with a p-value of 0.05 indicated that factor analysis is appropriate. Next, the Eigenvalue was calculated, and a cut-off value of 1 was used after approximating the first decimal point. Model fit was determined utilising chi square test and Root Mean Square Error of Approximation (RMSEA). Convergent and divergent validity testing was performed. Lastly, the internal consistency and Cronbach alpha were used to measure the reliability of the constructs; a Cronbach alpha of 0.6 or greater was considered reliable.
To compare means of scores between groups with different attitudes and behaviors toward vaccines and demographic characteristics t-test was utilized. An analysis of covariance was used to control for potential confounding variables.
3. RESULTS
3.1. Pilot
Thirty-nine Arabic-speaking participants answered the VAX-AR questionnaire; after excluding incomplete responses, 33 eligible responses were included for analysis.
The mean age of participants was 37.1 ± 9.8 years, with the majority being females (n=28, 84.8%), married (n=25, 75.8%), and having children (n=27, 81.8%). Regarding the reported educational level, most of the participants (n=28, 84.8%) reported having an undergraduate degree, whereas the others reported finishing school education (n=3, 9.1%) or having obtained a post-graduate degree (n=2, 6.1%). Most participants identified as students (n=22, 66.7%) and some identified as employees (n=5, 15.2%).
The average subscale scores, as well as the internal consistency of each domain, were as follows:
1. Mistrust of vaccine benefit domain consisted of three questions and the average score of 4.3 with a Cronbach alpha of 0.94 and inter-item correlation of 0.84.
2. Worries about unforeseen future effects domain consisted of three questions and had an average score of 2.61 with a Cronbach alpha of 0.88 and inter-item correlation of 0.72.
3. Concerns about commercial profiteering consisted of three questions and had an average score of 3.77 with a Cronbach alpha of 0.91 and inter-item correlation of 0.77.
4. Preference for natural immunity domain consisted of three questions and had an average score of 3.2 with a Cronbach alpha of 0.74 and inter-item correlation of 0.49.
Lastly, the novel anti-vaccination religious beliefs domain consisted of two questions with an average score of 4.5 with a Cronbach alpha of 0.56 and an inter-item correlation of 0.43. (Table 1).
| Variable | Statistics |
|---|---|
| Mean age, years ± SD | 21.6 ± 2.7 |
| Female gender, n (%) | 221 (69) |
| College, n (%) | - |
| - Science | 119 (37.3) |
| - Health Sciences | 100 (31.3) |
| - Art | 84 (26.3) |
| - Not declared | 16 (5) |
| Time spent reading daily news, n (%) | - |
| - 1 Minute – 1 Hour | 163 (51.1) |
| - 1 Hour – 2 Hours | 74 (23.2) |
| - More than 2 hours | 35 (11) |
| - None | 37 (11.6) |
| Attitude towards compulsory vaccination (answered NO), n (%) | - |
| - Would you ever decline receiving compulsory vaccination | 255 (81) |
| Attitude towards Flu vaccine (answered YES), n (%) | - |
| - I got a flu shot this year | 70 (22.2) |
| - I will get the flu vaccine next year | 136 (43.3) |
| Attitude towards COVID-19 vaccine (answered YES), n (%) | - |
| - I received the COVID-19 vaccine. | 230 (73.2) |
| - I will follow health recommendations regarding COVID-19 vaccines. | 213 (67) |
| - I have worries regarding the COVID-19 vaccine. | 105 (33) |
| - Worried about its safety level. | 56 (17.6) |
| - Believe that COVID-19 infection is mild / not dangerous. | 32 (10) |
| - Believe that COVID-19 vaccine is part of a bigger conspiracy. | 29 (9.1) |
| - Already got natural immunity from previous COVID-19 infection. | 29 (9.1) |
| - Worried about its low / no efficacy. | 20 (6.3) |
| - Lack of trust in the vaccine industry. | 18 (5.6) |
| - Worried about common side effects disrupting work/study. | 14 (4.4) |
| - Worried about undiscovered complications to the unborn child. | 1 (0.3) |
| - Family pressure against receiving it due to beliefs of harm. | 1 (0.3) |
3.2. Exploratory Factor Analysis, Confirmatory Factor Analysis, Discriminate Validity and Reliability
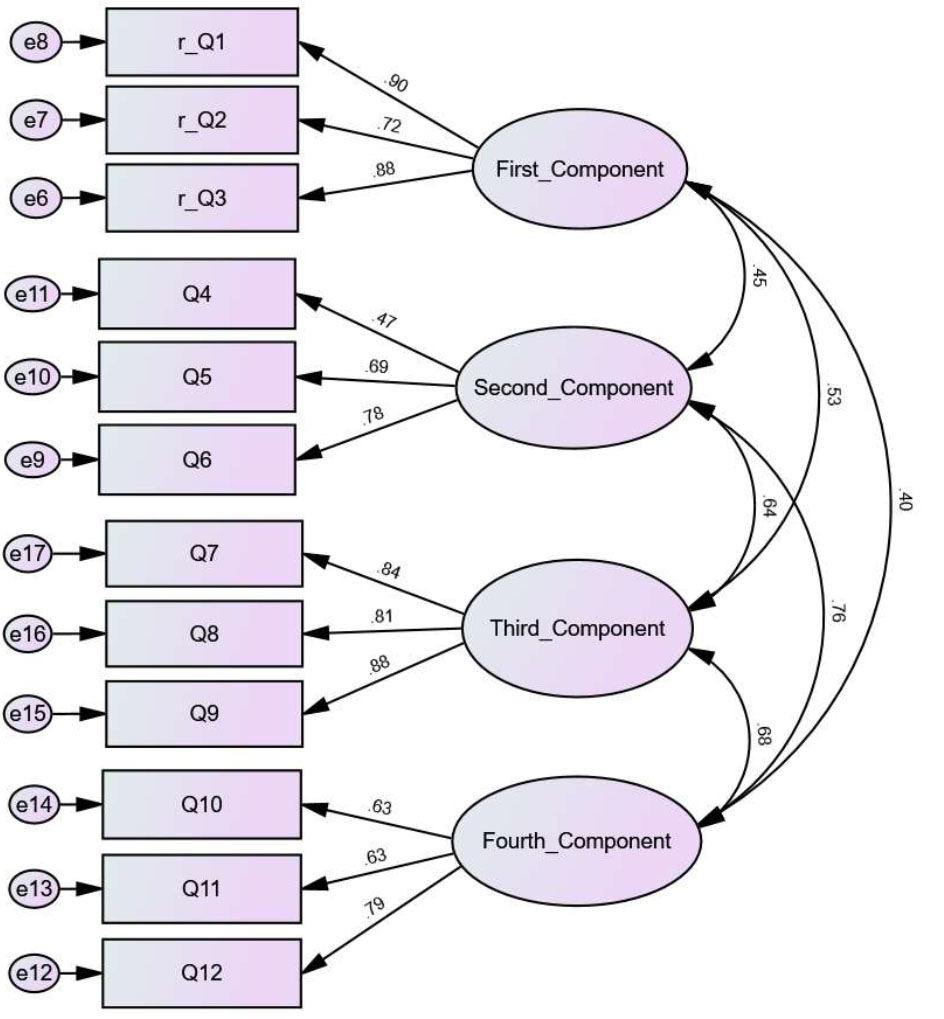
Exploratory factor analysis was performed for the VAX-AR scale, followed by tests to examine its reliability and validity. First, data suitability was measured using Kaiser-Meyer-Olkin (KMO) and Bartlett's Test of Sphericity. The KMO value was 0.88, and Bartlett's was significant (p<0.001). Next, exploratory factor analysis utilizing oblique-ProMax rotation was utilized. The scree plot illustrated the presence of four relevant components, as suggested by the curve's elbow, explaining 70.2% of the variance, with the fourth component having an Eigenvalue of 1 (Table 2A). The emerging four components correspond to the four components present at the original VAX scale, each harboring three items. The two added novel questions to the 12-item VAX scale did not force a fifth component/domain but instead seemed to load with the items under the domain titled (“Concerns about commercial profiteering”). The two added items did not improve the domain's reliability but were redundant. Hence, they were excluded from further analysis, and the 12-item VAX-AR was deemed sufficient. The internal consistency of the four identified components was measured by Cronbach α analysis and ranged from 0.70 – 0.88 (Table 2B).
Confirmatory factor analysis was conducted (Appendix 3). The fit indices of the model ranged from acceptable to excellent, as indicated by a chi-square/degrees of freedom ratio of 2.6 and a RMSEA value of 0.07. Evaluation of the reliability, along with convergent and discriminant validity revealed some concerns. Although the composite reliability for three of the constructs was robust, each exceeding the 0.7 threshold, the construct concerning worries over unforeseen future effects of vaccines yielded a slightly lower reliability score of 0.69. Additionally, the second and fourth constructs —pertaining to concerns about unforeseen vaccine effects and a preference for natural immunity—demonstrated weaker convergent and discriminant validity. The two items that contributed to the weaker scores were, items 5 (“Vaccines can cause unforeseen problems in children”) and 12 (“Being exposed to diseases naturally is safer for the immune system”), as depicted in Table 2A, despite this, attempts to improve the model by excluding these items were counterproductive, as their removal detrimentally impacted the overall integrity of the model. This suggests that while these items may have psychometric limitations, they capture essential facets of the constructs being measured, warranting their retention for the substantive value they contribute to the model.
2A. Exploratory factor analysis for the Modified Arabic (VAX-AR) Subscales*.
| - | Component | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| 1. I feel safe after being vaccinated. | 0.92 | - | - | - |
| 2. I can rely on vaccines to stop serious infectious diseases. | 0.83 | - | - | - |
| 3. I feel protected after getting vaccinated. | 0.95 | - | - | - |
| 4. Although most vaccines appear to be safe, there may be problems that we have not yet discovered. | - | 0.97 | - | - |
| 5. Vaccines can cause unforeseen problems in children. | - | 0.57 | - | - |
| 6. I worry about the unknown effects of vaccines in the future. | - | 0.61 | - | - |
| 7. Vaccines make a lot of money for pharmaceutical companies but do not do much for regular people. | - | - | 0.76 | - |
| 8. Authorities promote vaccination for financial gain, not for people's health. | - | - | 0.88 | - |
| 9. Vaccination programs are a big con. | - | - | 0.89 | - |
| 10. Natural immunity lasts longer than a vaccination. | - | - | - | 0.82 |
| 11. Natural exposure to viruses and germs gives the safest protection. | - | - | - | 0.85 |
| 12. Being exposed to diseases naturally is safer for the immune system than being exposed through vaccination. | - | - | - | 0.62 |
| • Added questions | - | - | - | - |
| 13. I am afraid that vaccinations contain prohibited substances | - | - | 0.70 | - |
| 14. Vaccinations are against the belief that Allah is the protector, and therefore they are not needed. | - | - | 0.84 | - |
Extraction Method: Principal Component Analysis.
| Domain | Mean ± SD | Cronbach's α | Inter-item Correlation |
|---|---|---|---|
| 1. Trust/mistrust of vaccine benefit (reversed) | 2.27 ± 1.17 | 0.87 | 0.69 |
| 2. Worries over unforeseen future effects | 4.38 ± 1.09 | 0.70 | 0.44 |
| 3. Concerns about commercial profiteering** | 2.3 ± 1.24 | 0.88 | 0.71 |
| 4. Preference for natural immunity | 3.47 ± 1.25 | 0.73 | 0.47 |
b. Items with factor loading less than 0.3 and more than -0.3 were not typed in the table.
** **The added questions - numbered 13 and 14 - were excluded from the analysis considering the absence of added value in the reliability score of the domain.
3.3. Response Analysis
Field testing of the VAX-AR scale was performed targeting undergraduate students at three public universities in Riyadh. An estimated 2000 students were reached via email, which included an online link directing to the survey. A total of 401 responses were received. After excluding ineligible responses, a total of 319 eligible responses were analyzed. The demographic data of all participants and a flowchart of response distribution are presented in Table 1 and Fig. (1). The mean age of the participants was 21.6 ± 2.7 years, and more than half were females (n= 221; 69.3%. All participants were undergraduate students in either the Natural and Formal Sciences discipline (n=119, 37.3%), Health Sciences discipline (n=100, 31.3%), Humanities and Arts discipline (n=84, 26.3%) or an undisclosed discipline (n=16, 5%).
All items of the VAX-AR questionnaire were scored from 1 to 6, where one reflects low anti-vaccination beliefs and six indicates strong ones. The average VAX-AR score of the study sample was 3.1 ± 0.9. When analyzing domains separately, which are: 1- Mistrust about vaccine benefits, 2- Worries over unforeseen future effects, 3- Concerns about commercial profiteering, 4- Preference for natural immunity, the mean scores were 2.3 ±1.2, 4.8 ±1.1, 2.3 ±1.6, 3.4 ±1.3, respectively (Table 3).
| Item number | Item | Strongly Disagree | Disagree | Slightly Disagree | Slightly Agree | Agree | Strongly Agree | |
|---|---|---|---|---|---|---|---|---|
| N (%) | ||||||||
| Q1 | I feel safe after being vaccinated* | 18 (5.6) | 16 (5) | 11 (3.4) | 58 (18.2) | 128 (40.1) | 88 (27.6) | |
| Q2 | I can rely on vaccines to stop serious infectious diseases* | 7 (2.2) | 18 (5.6) | 12 (3.8) | 26 (8.2) | 124 (38.9) | 132 (41.4) | |
| Q3 | I feel protected after getting vaccinated * | 11 (3.4) | 35 (11) | 9 (2.8) | 60 (18.8) | 128 (40.1) | 76 (23.8) | |
| Q4 | Although most vaccines appear to be safe, there may be problems that we have not yet discovered. | 8 (2.5) | 14 (4.4) | 24 (7.5) | 31 (9.7) | 147 (46.1) | 95 (29.8) | |
| Q5 | Vaccines can cause unforeseen problems in children. | 16 (5.0) | 31 (9.7) | 27 (8.5) | 97 (30.4) | 106 (33.2) | 42 (13.2) | |
| Q6 | I worry about the unknown effects of vaccines in the future. | 17 (5.3) | 61 (19.1) | 12 (3.8) | 71 (22.3) | 86 (27.0) | 72 (22.6) | |
| Q7 | Vaccines make a lot of money for pharmaceutical companies but do not do much for regular people. | 64 (20.1) | 115 (36.1) | 71 (22.3) | 12 (3.8) | 34 (10.7) | 23 (7.2) | |
| Q8 | Authorities promote vaccination for financial gain, not for people's health. | 121 (37.9) | 105 (32.9) | 37 (11.6) | 21 (6.6) | 25 (7.8) | 10 (3.1) | |
| Q9 | Vaccination programs are a big con. | 148 (46.4) | 107 (33.5) | 18 (5.6) | 26 (8.2) | 9 (2.8) | 11 (3.4) | |
| Q10 | Natural immunity lasts longer than a vaccination. | 16 (5.0) | 41 (12.9) | 82 (25.7) | 40 (12.5) | 82 (25.7) | 58 (18.2) | |
| Q11 | Natural exposure to viruses and germs gives the safest protection. | 44 (13.8) | 74 (23.2) | 48 (15.0) | 59 (18.5) | 63 (19.7) | 31 (9.7) | |
| Q12 | Being exposed to diseases naturally is safer for the immune system than being exposed through vaccination. | 64 (20.1) | 76 (23.8) | 38 (11.9) | 75 (23.5) | 44 (13.8) | 22 (6.9) | |
| Added questions | - | |||||||
| Q13 | I am afraid that vaccinations contain prohibited substances. | 123 (38.6) | 94 (29.5) | 50 (15.7) | 7 (2.2) | 29 (9.1) | 16 (5.0) | |
| Q14 | Vaccinations are against the belief that Allah is the protector, and therefore they are not needed. | 249 (78.1) | 40 (12.5) | 9 (2.8) | 9 (2.8) | 4 (1.3) | 8 (2.5) | |
| A- Behavior towards vaccination | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain score / Vaccination status | Flu vaccine | P-value | Covid-19 vaccine | P-value | ||||||||||
| - |
Vaccinated (n=70) |
Not vaccinated (n=245) |
- |
Vaccinated (n=230) |
Not Vaccinated (n=84) |
- | ||||||||
| Mistrust of vaccine benefit* | 1.9 ± 1.0 | 2.4 ± 1.2 | 0.001 | 2.0 ± 1.0 | 2.9 ± 1.3 | <0.001 | ||||||||
| Worries over unforeseen future effects | 4.1 ± 1.3 | 4.4 ± 1.0 | 0.037 | 4.2 ± 1.1 | 4.7 ± 1.1 | <0.001 | ||||||||
| Concerns about commercial profiteering | 2.1 ± 1.2 | 2.3 ± 1.2 | 0.127 | 2.1 ± 1.1 | 2.9 ± 1.4 | <0.001 | ||||||||
| Preference for natural immunity | 3.3 ± 1.3 | 3.5 ± 1.2 | 0.132 | 3.3 ± 1.5 | 4.0 ± 1.1 | <0.001 | ||||||||
| VAX-AR total score (all domains) | 2.9 ± 0.9 | 3.2 ± 0.9 | 0.01 | 2.9 ± 0.8 | 3.6 ± 0.9 | <0.001 | ||||||||
| B- Attitude towards vaccination | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain score / Attitude towards vaccines | Flu vaccine | P-value | Covid-19 vaccine | P-value | Compulsory vaccines | P-value | ||||||||
| - |
Positive (n=136) |
Negative (n=178) |
- |
Positive (n=213) |
Negative (n=105) |
- |
Positive (n=255) |
Negative (n=60) |
- | |||||
| Mistrust of vaccine benefit* | 2.0 ± 0.9 | 2.5 ± 1.3 | <0.001 | 1.9 ± 0.8 | 3.0 ± 1.4 | <0.001 | 2.2 ± 1.1 | 2.8 ± 1.4 | 0.001 | |||||
| Worries over unforeseen future effects | 4.2 ± 1.2 | 4.5 ± 1.0 | 0.004 | 4.1 ± 1.0 | 4.9 ± 1.0 | <0.001 | 4.3 ± 1.1 | 4.9 ± 1.0 | <0.001 | |||||
| Concerns about commercial profiteering | 2.1 ± 1.1 | 2.5 ± 1.3 | 0.003 | 1.9 ± 0.9 | 3.1 ± 1.5 | <0.001 | 2.2 ± 1.1 | 2.8 ± 1.5 | 0.002 | |||||
| Preference for natural immunity | 3.2 ± 1.2 | 3.7 ± 1.2 | <0.001 | 3.2 ± 1.2 | 4.0 ± 1.2 | <0.001 | 3.3 ± 1.2 | 4.1 ± 1.1 | <0.001 | |||||
| VAX-AR total score (all domains) | 2.8 ± 0.8 | 3.3 ± 0.9 | <0.001 | 2.8 ± 0.7 | 3.8 ± 0.9 | <0.001 | 3.0 ± 0.8 | 3.7 ± 1.0 | <0.001 | |||||
Responders who were enrolled in health-related colleges scored lower across all domains, with a difference in the score that ranged from -0.34 in the mistrust in vaccines domain to -0.79 in the preference of natural immunity domain (p<0.015). Females tended to score lower than males in all domains as well. However, after controlling for the type of college, statistical significance was only retained in the domain of concerns of commercial profiting, accounting for 15% of the variance difference (p=0.027). Age and reported time of reading daily news were not associated with significant changes in VAX-AR scores.
All participants were asked about their flu and COVID-19 vaccination status since the study was performed during the period of the COVID-19 pandemic. The reported vaccination status was used as a surrogate for the responder's behavior towards vaccination. As for attitude, questions about the likelihood of following health recommendations for the Flu, COVID-19, and compulsory vaccines were used. Higher VAX-AR scores were significantly associated with lower rates of vaccination and likelihood to follow healthcare advice (Table 4A and 4B) which jointly reflect the VAX-AR validity.
4. DISCUSSION
The VAX scale has been developed to enhance our understanding of the prevalence of anti-vaccination attitudes across various demographics. In addition to its original English form, the tool has undergone numerous validations in different populations [12, 16, 18, 19].
Compared to the current literature, two validation studies of Italian and Spanish languages have the same factor loading matrix as shown in the study by Martin et al. [10, 17, 18].
To our knowledge, our study represents a pioneering effort to translate the VAX scale into Arabic — VAX-AR — and to evaluate its validity and reliability within an Arabic-speaking context. The demographic characteristics, along with the reliability and validity metrics of our study, are consistent with those observed in other international studies, reinforcing the robustness of the VAX scale across cultural boundaries. Adopting the VAX-AR is particularly significant for public health efforts in the approximately 25 Arabic-speaking nations. The translation process employed the forward-backward method and engaged experts in both linguistics and subject matter, ensuring a precise and culturally relevant Arabic version of the scale.
One of the study's major limitations was the restricted access to the targeted sample due to the COVID-19 pandemic, which imposed limitations on the sampling technique and number of participants. Although online surveys, such as the one used in our study, typically suffer from lower participation rates, the sample size obtained was in line with our power analysis, guaranteeing robust statistical analysis despite a modest cohort size. The timing of the study, coinciding with the rollout of COVID-19 vaccines, heightened the pertinence and likely accuracy of participants’ responses, as the topic was at the forefront of public consciousness.
Our research utilized the VAX-AR to investigate vaccine attitudes among young, educated Saudis — a demographic pivotal to the region's health dynamics. The VAX-AR scores correlated appropriately with behaviors related to Flu and COVID-19 vaccinations, drawing parallels with a similar investigation in Italy [18]. The association between vaccine hesitancy, as measured by the VAX-AR, and COVID-19 vaccination status was particularly pronounced. Consistent with findings from other research, the predominant concern among the participants centered on the potential long-term effects of vaccines, a worry likely intensified by the concurrent unfolding of the COVID-19 pandemic and the public discourse surrounding the emergent vaccines [20, 21]. Notably, our participants exhibited higher mean scores of vaccine hesitancy than those in similar studies, suggesting a need for improved access to reliable vaccine information [22, 23]. Addressing these gaps through enhanced educational outreach is essential.
Besides the domains covered in the original VAX scale, there remain sub-optimally investigated dimensions that could potentially affect individuals' vaccination beliefs [19]. Religious belief and conservatism have been identified as factors affecting vaccine refusal and hesitancy [17, 24, 25]. Since the Islamic religion is intertwined within the fabric of Saudi society, affecting peoples' attitudes and behaviors, the authors opted to test this dimension by adding items to the original 12-item VAX (Appendix 2). Most Saudi youths had a negative response to the 2-item religion domain, which proves that their religious beliefs did not relate to their anti-vaccination attitudes. This can be explained by the Quran and Islamic teaching of promoting health and sustaining a healthy life. At the same time, two studies reported that Jewish and Christian communities had positive attitudes toward vaccination, and their religions similarly support health promotion and even to the level of mandating vaccines [19, 20]. On the contrary, Khan et al. stated that Pakistan had a higher vaccine hesitancy due to the belief that COVID-19 is a conspiracy against Islamic countries [21]. Moreover, a systematic review included multiple religions, including Jewish and Christian religions, and found that under-vaccinated individuals in these communities were influenced mainly by religious-related beliefs and myths [22]. Upon analysis, those items were associated positively with items in the domain of beliefs of commercial profiting yet failed to add value to the overall model. A potential explanation for this phenomenon is that both beliefs share the same sources spreading anti-vaccination misinfor- mation [26-29].
CONCLUSION
In conclusion, the translated Arabic VAX scale has good validity and reliability scores. Therefore, VAX-AR can easily be applied to assess Arabic-speaking populations' negative attitudes toward vaccination. The widespread anti-vaccination attitude observed among educated youths in Saudi Arabia reflects the need for targeted and tailored public health education campaigns and the establishment of reliable health information resources. In addition, a broader study including different community members to measure anti-vaccination attitudes and their roots in Saudi Arabia and the Middle East is highly encouraged as the limited geographic focus and the relatively low sample size may affect generalizability.
AUTHORS’ CONTRIBUTION
MA and GA contributed to the design and implementation of the research and the writing of the manuscript. MA and MFS analyzed the data and wrote the methodology. AA, GA, and MA collected the data and co-wrote the manuscript. MFS reviewed and edited the final manuscript. MFS supervised the project. All authors agreed on the final manuscript.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| PACV | = Parent Attitudes about Childhood Vaccines |
| VAX | = Vaccination Attitude Examination |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study received approval from the Institutional Review Board (IRB) committee of King Abdullah International Medical Research Center, Kingdom of Saudia Arabia (RC20/560/R).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The raw data supporting the conclusions of this article will be made available by the authors [M.F.S] without undue reservation.
CONFLICT OF INTEREST
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to Dr. Mohammed Al-Shaalan, Pediatric Infectious Diseases Consultant, Dr. Sami Mahmoud, Pediatric Psychiatry Consultant, and Dr. Fareeda Mukhtar, Lecturer in Medical Education, for their review of the translation process regarding the linguistic and scientific content of the questionnaire.