All published articles of this journal are available on ScienceDirect.

Identifying Barriers to Detection of Perinatal Depression: A Qualitative Study of Midwives’ Perspectives in South African Primary Care
Authors Info & Affiliations
Abstract
Introduction
Perinatal depression is a significant global health challenge that has immense implications for maternal and child wellbeing. Despite the increasing awareness of mental health challenges surrounding pregnancy and childbirth, perinatal depression remains underdiagnosed and undertreated in many low- and middle-income countries. This study provides unique insights by applying the Theory for Health Promotion in Nursing (THPN) to comprehend midwives’ perspectives on identifying and overcoming barriers to early identification of perinatal depression within a low-resource setting.
Methods
A qualitative study, theoretically grounded by the THPN, which considers that health promotion happens through interactive processes between midwife and their environment, positioning them as therapeutic agents to promote maternal health, particularly in the external environment of midwife-led obstetric units. As such, data were collected from seventeen (17) midwives between April and May 2024 using semi-structured face-to-face interviews, and thereafter, analysed using thematic analysis.
Results
Three overarching themes emerged, namely, (1) sociocultural barriers, (2) healthcare system and provider-related barriers, and (3) proposed solutions to address barriers. A complex interplay of factors such as cultural stigma, inconsistent screening practices, and sub-optimal working conditions was identified to influence early detection.
Discussion
The findings reveal that the barriers to detecting perinatal depression are embedded in cultural, systemic, and provider interactions with the women. Through the lens of the THPN framework, the study uncovers how midwives as therapeutic agents not only encounter resource constraints, but stigma and systemic barriers hinder their ability towards early detection. There is a need for multi-level interventions to address the identified barriers to improve perinatal mental health care.
Conclusion
Both sociocultural and health care system barriers exist in the South African maternal health care settings. The results of this study suggest the need for integration of mental health services into maternal healthcare to enhance management of women who are at risk of developing perinatal depression.
1. INTRODUCTION
Perinatal depression is a significant global health challenge that has immense implications for maternal and child wellbeing. Perinatal depression, formally known as postpartum depression (PPD), is defined as depression experienced after childbirth according to the Diagnostic and Statistical Manual of Mental Disorders [1]. The use of the concept of perinatal depression recognizes that depression related to childbirth actually begins during pregnancy. According to the National Institute of Mental Health, perinatal depression includes depression that occurs during pregnancy (prenatal depression) and in the weeks after childbirth (postpartum depression), with most episodes beginning within four to eight weeks after the baby is born [2]. The symptoms present as extreme sadness, anxiety, and changes in sleeping and eating patterns, making it difficult for the mother to carry out daily tasks, including caring for her newborn baby.
While having a baby could be viewed as exciting, it could also be a daunting time for the mother, particularly because of the changes that the mother experiences during the perinatal period, such as physiological, psychological, financial, and social changes. The routine screening conducted at multiple points during the perinatal period and in intervals during the postpartum period could assist in identifying perinatal depression. However, in many instances where a routine screen is not done, perinatal depression may go unnoticed [3]. Thus, the early detection of perinatal depression becomes important in routine checkups to prevent fatalities. The knowledge and skills of midwives in screening for perinatal depression are vital. However, in most instances, midwives report low literacy about perinatal depression, leading them to miss the signs that are at times detectable [4].
Perinatal depression affects 17.22% of women globally, with varying rates across regions and populations [5]. In the American context, perinatal depression accounts for 21.71% in South America and 17.01% in Northern America %; while a variation is noted to be 16.62% in Eastern Europe compared to 17.39% in Eastern Asia. Southern Africa accounts for the highest prevalence at 39.96% compared to Northern and Western Africa at 19.83% and 13.62%, respectively [6]. Untreated perinatal depression extends beyond the affected mother’s experience but has long-term psychological impact on the mother, child's well-being, family dynamics, and socioeconomic implications linked to the increased utilization of health care services.
The literature reports risk factors for the development of perinatal depression among women, such as difficult relationships, intimate partner violence, unplanned pregnancies, loneliness, low educational level, poor economic status of families, low social support, and societal pressures [7–11]. At the same time, women with perinatal depression present with low help-seeking behaviours due to cultural beliefs and misconceptions about perinatal depression reported as the common hindrances for women to seek help [12]. A study conducted in a rural African setting reported that women with perinatal depression symptoms did not seek help as they wanted to solve the problem by themselves, while some resorted to traditional and religious interventions [13].
Additionally, women who are aware of their mental health difficulties during the perinatal period fear disclosing their symptoms due to being mocked by others (stigma), thus consider mental health as a private matter [9, 12].
While midwives play a vital role in detecting perinatal depression, there are multifaceted factors that hinder the early detection of perinatal depression. A systematic literature review revealed that midwives present with low perinatal depression literacy, particularly about the knowledge of the definition, prevalence, symptoms, risk factors, screening tools, and their treatments, which hinders the provision of care to perinatal women [14]. Furthermore, literature reveals that the training of midwives does not fully prepare them to be able to identify and manage mothers presenting with perinatal depression. A study [15] revealed that only 24.3% of midwives had formal training on perinatal depression, indicating that a gap in preparing midwives exists, while of midwives had inadequate knowledge, which impacted their confidence in detecting perinatal depression symptoms. Some factors include the notion of overlooking mental health in maternal health care [16]. Despite the increasing awareness of mental health challenges surrounding pregnancy and childbirth, perinatal depression remains underdiagnosed and undertreated in many low- and middle-income countries [17], hence the early detection of perinatal depression remains challenging owing to numerous challenges in the healthcare system and societal factors. The study aimed to uncover hindrances to the early detection of perinatal depression from the perspective of South African midwives.
2. MATERIALS AND METHODS
2.1. Purpose of the Study
The study aimed to uncover barriers to the early detection of perinatal depression from the perspective of South African midwives using an exploratory descriptive qualitative design [18].
2.2. Study Setting
The study was conducted in the Tshwane Metropolitan municipality located in Northern Gauteng, South Africa. Tshwane is South Africa’s fourth largest metropolitan area with over 3.5 million inhabitants. Four midwifery-led obstetric units (MOUs) located in Community Health Centres (CHCs) of Tshwane region one and two were chosen. These MOUs serve a diverse population, including the provision of 24-hour antenatal, intrapartum, and postnatal care services for uncomplicated pregnancies, with approximately 83.2% of the local population receiving postnatal care from these facilities. Each MOU operates with at least eight midwives during the day and four at night. The MOUs provide maternal care in the region, where midwives are responsible for both clinical care and health education, referring complicated cases to higher-level facilities; therefore, these settings are critical for understanding barriers to the detection of perinatal depression.
2.3. Study Design and Theoretical Framework
This study was theoretically grounded by the Theory for Health Promotion in Nursing (THPN) to identify barriers to early identification of perinatal depression from the perspective of South African Midwives. This theory views human beings holistically as integrated beings connected to body, mind, and soul, and they interact dynamically with their environment. Thus, health emerges from the quality of these interactions rather than merely the absence of illness. In this study, this holistic view was essential to comprehend how midwives' own well-being and professional capacities influence their ability to identify perinatal depression. Therefore, THPN assumes that midwives have the knowledge and analytical abilities to assess, judge, and manage conditions like perinatal or postpartum depression while acknowledging their spiritual dimensions that influence their worldviews and practice philosophies.
Furthermore, THPN considers that health promotion occurs through interactive processes between midwives and their environment, positioning midwives as therapeutic agents to promote maternal health, particularly within the external environment of midwife-led obstetric units where perinatal and postnatal care take place. By applying this theoretical framework, the study found that barriers to perinatal depression identification arise from a complex interplay among midwives' personal characteristics, professional knowledge, the clinical environment, and the broader healthcare system. All these factors can either facilitate or hinder effective maternal mental healthcare.
2.4. Participant Recruitment
The participants were approached directly, face-to-face, by the researchers following ethical approval and site permissions to recruit them for participation in the study. Individual appointments were then made with those who showed interest to obtain informed consent.
2.5. Sample and Procedure
Purposive sampling was used to select the participants with specific characteristics that would enable the researchers to explore the barriers to early detection of perinatal depression [19]. The sample was drawn from midwives working in midwifery-led Obstetric Units based on their involvement in providing maternal care. The inclusion criteria were as follows: (1) registration as midwife and (or) midwife specialist in line with the South African Nursing Council (SANC); (2) a minimum of 2 years’ experience in direct contact with women who are attending postnatal care; (3) employees at any of the selected MOUs and willing to participate in the study. The final sample of seventeen (17) midwives was determined using the principle of data saturation. No new thematic information emerged on the 13th interview; however, four additional interviews were conducted to confirm saturation, resulting in the final sample of 17 midwives.
2.6. Outline of the Interview Schedule
Prior to data collection, we conducted two preliminary interviews with midwives who possessed similar characteristics to be included in the study to pre-test the data collection instrument [19]. The feedback from the preliminary interviews was used to refine the data collection instrument, ensuring that the questions were clear. The formal data collection instrument included the following: (1) What are your thoughts regarding screening for perinatal depression? (2) What barriers do you experience in the identification of perinatal depression? (3) Can you describe the measures used in this facility to encourage mothers to verbalize psychological abnormalities? (4) What do you think will enable you as a midwife to perform perinatal depression screening during routine care? (5) In your view, what can be done to empower midwives in the screening and management of perinatal depression?
2.7. Data Collection
Data were collected between April and May 2024 using semi-structured face-to-face individual interviews. The interviews were conducted by the second author at the MOUs where the midwives provide maternal care. The interviewer was a female researcher with knowledge in public health, and was mindful of potential power dynamics as a researcher. To ensure reflexivity, the researcher maintained a neutral, non-judgmental, and open viewpoint to encourage honest responses from participants, and field notes were documented. The interviews lasted between 29 and 42 minutes, with a mean of 31 minutes. An audio recorder was used to capture the interviews with the participants' permission. Privacy and anonymity were ensured during the process of data collection, where no information linking to the participants was shared [20]. All interviews were conducted in English and were concluded when data saturation was confirmed, i.e., when no new themes emerged.
2.8. Data Analysis
The second author transcribed the audio-recorded interviews, while the first and third authors checked and verified the transcriptions against the recording to confirm if they captured the meaning from the participants’ perspectives. The participants also confirmed these to ensure that the transcriptions reflect what the participants shared during data collection. Thereafter, Braun and Clarke’s reflexive thematic analysis [21]. The six-step analysis method was applied by (1) familiarization with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. The three researchers independently analyzed the data, then met to reach consensus on the final themes. Finally, the researchers returned to the participants for validation of the final themes, ensuring that they reflect the participants’ views and the accuracy of the data.
2.9. Trustworthiness
To ensure credibility, interviews were conducted until the data were deemed sufficient. Additionally, the researchers independently analyzed the data, compared their analysis and discussed to reach a consensus on the final themes [22]. For dependability, an independent expert in qualitative research reviewed the transcript and the analyzed data to ensure accuracy of the data [23]. In addition, the midwives who participated in this study were given an opportunity to confirm the interpretation of the findings, ensuring that their perspectives were correctly captured. Lastly, the researchers provided detailed and comprehensive descriptions of the methods used in this study, including comprehensive descriptions of the participants and study context, thereby ensuring transferability.
2.10. Ethical Considerations
The study was approved by the Sefako Makgatho Health Sciences University Research Ethics Committee (SMUREC/H/345/2023:PG). Since the study involved human participants, the site managers of the MOUs also granted the researchers access to the participants [24]. The study was conducted in accordance with the Declaration of Helsinki [25]. The participants were then approached directly, face-to-face, to provide details of the study. Individual appointments were made with the midwives who demonstrated interest in participating in the study to obtain written informed consent. All participants gave written informed consent, and they were reassured that privacy and confidentiality would be maintained. As such, participants’ IDs were used to protect their personal information. Their right to self-determination was maintained by informing them of their freedom to withdraw anytime without consequences [19].
3. RESULTS
The characteristics of participants and the themes that emerged during data analysis are detailed below:
3.1. Characteristics of Participants
A total of 17 midwives participated in this study. The majority of participants were female (94%), and only 6% were male. This could be because nursing is still a female-dominated profession, especially in midwifery in South Africa. The majority of the midwives (53%) had basic training in midwifery during their undergraduate studies, while 47% had a postgraduate qualification in midwifery and registered as midwife specialists at the South African Nursing Council (SANC). An overview of the characteristics of participants is provided in Table 1 below. The researchers respected the right to self-determination of one participant who chose not to disclose their age. This is denoted by ‘xx’ as shown in Table 1.
| ID | Gender | Age in Years | Experience in MOU in Years | Qualifications |
|---|---|---|---|---|
| P1 | Female | 35 years | 6 years | *Advanced midwifery |
| P2 | Female | 24 years | 3 years | Basic midwifery within a degree in nursing science and art |
| P3 | Female | xx years | 5 years | Basic midwifery within the diploma in nursing science and art |
| P4 | Female | 55 years | 11 years | Basic midwifery within a degree in nursing science and art |
| P5 | Female | 30 years | 4 years | Basic midwifery within the diploma in nursing science and art |
| P6 | Female | 42 years | 9 years | *Advanced midwifery |
| P7 | Female | 62 years | 18 years | *Advanced midwifery |
| P8 | Female | 39 years | 3/5 years | Basic midwifery within the diploma in nursing science and art |
| P9 | Female | 29 years | 4 years | Basic midwifery within the diploma in nursing science and art |
| P10 | Female | 39 years | 9 years | *Advanced midwifery |
| P11 | Female | 45 years | 8 years | *Advanced midwifery |
| P12 | Female | 50 years | 11 years | *Advanced midwifery |
| P13 | Female | 46 years | 11 years | *Advanced midwifery |
| P14 | Female | 33 years | 9 years | Basic midwifery within the diploma in nursing science and art |
| P15 | Female | 44 years | 10 years | *Advanced midwifery |
| P16 | Male | 44 years | 16 years | Basic midwifery with a Postgraduate diploma in primary health care nursing |
| P17 | Female | 35 years | 3 years | Basic midwifery within the diploma in nursing science and art |
Note: Keys: xx- denotes that the participant did not disclose her age
*- denotes that the participant has a postgraduate qualification in midwifery, either a postgraduate diploma in advanced midwifery or a Master’s degree in advanced midwifery, which are registered under the same regulation in South Africa, Regulation 212 (R212).
3.2. Presentation of Key Themes
The thematic analysis resulted in three overarching themes emerging: (1) sociocultural barriers, (2) healthcare system and provider-related barriers, and (3) proposed solutions to address barriers to early detection of perinatal depression. The themes and subthemes are presented in Fig. (1) and further supported with verbatim quotes to ensure the accuracy of the results.
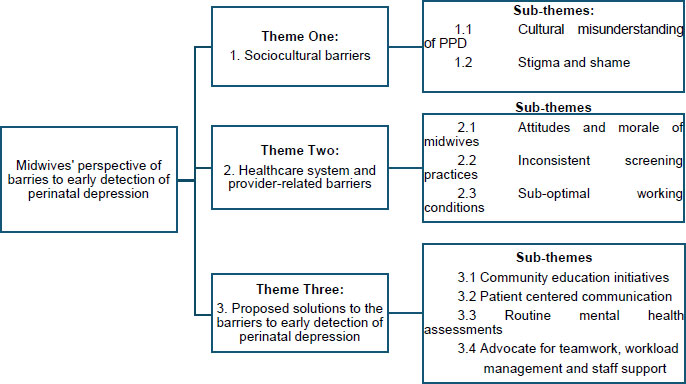
Diagrammatic representation of the themes and subthemes within the thematic framework.
3.2.1. Sociocultural Barriers
The midwives’ narratives revealed that sociocultural factors create a significant barrier to perinatal depression, mostly due to stigma around mental health issues during the perinatal period and the consequent fear of being judged experienced by the women. The midwives further reported that within their communities, particularly Black South African communities, early symptoms of perinatal depression are frequently misconstrued as personal shortcomings, as well as one's own interpretation about one's readiness to become a mother, rather than signs of medical disorders. One of the advanced midwives explained that cultural beliefs prevent recognition of perinatal depression as a health concern:
“In our Black communities, it was never recognized, and someone will be scolded and say, 'you are just afraid of being a mother'.” [Participant 10, 39-years-old, Advanced Midwife]
This remark highlights how cultural beliefs can mask normal emotional challenges, characterizing them as personal deficiencies rather than symptoms that require medical attention. The internalization of stigma leads to women experiencing mental health challenges to conceal their symptoms:
“Remember in our society......when you have a psychological challenge or a mental challenge, you are regarded by other people as like this one is... but this one.” [Participant 12, 50-years-old, Advanced Midwife]
The expression “regarded by other people” highlights how societal perception about health challenges can silence women, particularly when it comes to turning their private distress into public humiliation. Society seems quick to pass judgment, linking symptoms of distress during the perinatal period to a phase of difficulty that will pass and the women’s unpleasant attitudes towards their babies. One midwife reflected:
“Us as the Black people... we thought that maybe this woman is being unkind to the baby...” [Participant 17, 35-years-old, Midwife]
The midwives also acknowledged that their own cultural backgrounds and preconceived ideas could unintentionally reinforce these barriers, particularly their lack of understanding of symptoms of perinatal depression. One midwife said:
“At that time, I was thinking ahhh maybe these women are crazy. I didn't have much insight on it when they told me about that…that was my perception of it, postpartum depression.” [Participant 16, 44-years-old, midwife with Primary Health Care Specialty]
The midwives’ openness about their own biases arising from the relatively same preconceptions about mental health difficulties during the perinatal period can create a clinical environment where symptoms are minimized and misunderstood, leading to concealment.
“Our patients are not free most of the time. They are hiding things... I don’t know what is the reason or maybe they think we will judge them.” [Participant 11, 45-years-old, Advanced Midwife]
“Cultural aspects... personality of midwives... some are just here for income, not passionate about excellent service.” [Participant 7, 62-years-old, Advanced Midwife]
The resultant effect is that of an intimidating environment that women fear disclosing. The participants revealed that patients actively withhold information, with some midwives observing:
“They have the shame of talking about this... because when you have a psychological challenge or mental challenge, you are regarded as other people as like this one is.” [Participant 12, 50-years-old, Advanced Midwife]
“Some are afraid... the sister might judge me; the sister might shout at me. They will say, 'You guys don’t understand my situation, so there’s no need for me to explain further.'” [Participant 17, 35-years-old, Midwife]
Therefore, fear of being judged forms a significant barrier to disclosure of mental health challenges during the perinatal period, especially in an environment that is meant to provide support.
3.2.2. Healthcare System and Provider-related Barriers
Beyond cultural factors, midwives identified other significant barriers within the healthcare system and their own professional practice, characterized by inconsistent screening practices, sub-optimal working conditions, and, at times, dehumanizing provider attitudes. A recurring theme was the negative attitude and low morale among which often leads to poor interaction or engagement with the women and creates a space of avoidance, deeming midwives unapproachable. One midwife reflected:
“We are unapproachable... most nurses are... patients will not approach us. Our attitude as nurses [midwives] sometimes makes it difficult for patients to approach us. We are poorly treating them... we are not giving them holistic care.” [Participant 3, xx-years-old, Midwife]
This self-reflection indicates a professional culture in which emotional numbness may be widespread, directly affecting the quality of therapeutic engagement. These attitudes are frequently associated with inadequate working conditions. Participants in this study related their behaviour to systemic pressures, with some acknowledging:
“Our attitude is like we are always angry... We have our employment issues, but we are angry. I think we are taking our anger out on our patients.” [Participant 1, 35-years-old, Advanced Midwife]
“I think mostly it’s our attitude, ethnicities. It’s unfriendly. Obviously, not gonna show your emotions. You’re not going to show any weakness.” [Participant 8, 39-years-old, Midwife]
The above utterances indicate a worrying loop in which systemic pressures on healthcare personnel are passed on to patients, ultimately compromising the foundation of trust. Furthermore, the inconsistent application of mental health screening emerged as an operational failure during routine maternal care. Some do not consider mental health screening important during this phase, while others do not prioritize it. The midwives admitted:
We take [mental health screening] lightly... Just ask one question to the patient.” [Participant 15, 44-years-old, Advanced Midwife]
“Not every woman is actually screened for postpartum depression... It’s very overlooked.” [Participant 5, 30-years-old, Midwife]
Some midwives focus on maternal care, which directs them to physical care, and they end up overlooking the mental health of the women despite having screening tools that guide their practice. Some indicated that the current maternity guidelines do not focus on mental health screening. The participants said:
“We don’t even mention postpartum on discharge [meaning postpartum depression]... I don’t even remember telling the patient, that’s it.” [Participant 8, 39-years-old, Midwife]
“We don't dwell much on the mental well-being of the women after giving birth... We are most likely not to identify those women. There is nothing in the book [about postpartum screening]... You can skip it.” [Participant 14, 33-years-old, Midwife]
“We don’t manage it... We’re just focusing on the physical... Even if you see someone is not well emotionally, you’ll just ask what’s wrong. You’ll be fine, but you’re not going deep.” [Participant 1, 35-years-old, Advanced Midwife]
Thus, indicating that maternal mental health is systematically ignored within routine care protocols. This is worsened by time constraints and infrastructure limitations. The midwives mentioned that they do not have time or space to perform or conduct mental health screenings, as it often gets busy in the MOUs, such that they cannot prioritize mental health. One midwife said:
“Time, workload... You’ve got 10 patients to admit, you’ve got 5 to discharge, the world is full, so you just want to give a touch-up.” [Participant 8, 39-years-old, Midwife]
The statement “give touch-up” directly captures the reality of care within busy MOUs where comprehensive assessment is compromised to complete the numbers who are there to receive care. Privacy concerns in overcrowded facilities hinder disclosure, as mentioned below:
“In our facilities, it's just a small space that you see that we are in, then we work. We are two nurses working... sometimes feel shy to divulge information that is sensitive because there is another patient.” [Participant 16, 44-years-old, Midwife With Primary Health Care Specialty]
Finally, bureaucratic and referral barriers complicate care pathways. This is mentioned by one midwife who says:
“Our policies and protocols limit us... Patients suffering from depression must be referred to higher levels of care, but the system is overwhelmed.” [Participant 12, 50-years-old, Advanced Midwife]
The above means that even if the midwives are able to detect perinatal depression early, systemic barriers such as a fragmented system may prevent them from effectively intervening, therefore rendering the screening process ineffective.
3.2.3. The Proposed Solutions to Breaking the Barriers to Early Detection of Perinatal Depression
In response to these barriers, the midwives proposed practical solutions targeting individual, community, and systemic levels. Their recommendations focus on education, improved communication, standardized screening, and support for healthcare workers. One main recommendation was community and patient education to explain perinatal depression. The participants pointed out that awareness must extend beyond the clinical setting to the community, including family involvement, to improve understanding of mental health challenges during the perinatal period. They said:
“We need awareness... Let's educate them. The woman can also identify that they are not okay and will speak. Health education should emphasize... not only wait after delivery.” [Participant 14, 33-years-old, Midwife]
“Health education... You take time and speak to make sure the patient understands... If they know about this condition, they will be free. The families need to know... Others think it’s witchcraft. Health education can help.” [Participant 11, 45-years-old, Advanced Midwife]
“Educate the whole community, not just mothers... awareness helps families recognize signs early.” [Participant 7, 62-years-old, Advanced Midwife]
At the clinic level, midwives identified patient-centred communication and rapport building as necessary to improve the interaction and engagement between the midwives and the women during the perinatal period. One midwife clearly said:
“Friendliness. The approach, how we approach the patient... If I come with an attitude to a patient, definitely I won’t get anything. If you come with an attitude, the patient will also come with an attitude.” [Participant 8, 39-years-old, Midwife]
Others suggested creating a safe space for the women to open up about their challenges freely without fear of being judged:
“Establishing a good rapport is particularly important in ANC, so that during your history taking, the patient can feel free, or at least to be able to open up.” [Participant 16, 44-years-old, Midwife with Primary Health Care Specialty]
“You [the midwife] have to create a rapport between you and this woman, a good relationship, don’t be judgmental.” [Participant 4, 55-years-old, Midwife]
The midwives strongly supported the implementation of mandatory and standardized mental health screening that should be integrated into routine care to transform maternal healthcare. They emphasize the importance of mental health screenings and recommend that these should be started early in the antenatal period. They said:
“Screening is a must... Mental health problems will arise if you ask.” [Participant 15, 44-years-old, Advanced Midwife]
“They should include mental screening postpartum in the book... You have to follow it, like vitals. Screening is essential... It’s vital to identify women likely to fall into postpartum depression.” [Participant 14, 33-years-old, Midwife]
“I think, for instance... if maybe the tool can be incorporated with antenatal... maybe there's a space that we can be able to do that.” [Participant 6, 42-years-old, Advanced Midwife]
The midwives proposed that systemic support and interdisciplinary collaboration be supported, as individual effort may not be sufficient. At the same time, others pointed out the need for improved staffing and resource allocation. The midwives emphasized teamwork as a cornerstone of healthcare provision for creating comprehensive care strategies for maternal mental health:
“Perhaps the solution can come if we continue to talk about it, and then when we involve our professors and other doctors, perhaps they can, because most of our providers... If we engage them a lot, then perhaps the solution can come.” [Participant 16, 44-Years-Old, Midwife with Primary Health Care Specialty]
“Midwives and WBOT teams need a close relationship... assign a WBOT person to each mother.” [Participant 15, 44-years-old, Advanced Midwife]
“If we are well-staffed... we can treat women holistically. Management should help... if it’s something they can do to help you.” [Participant 3, xx-years-old, Midwife]
Finally, participants reinforced the need for training and psychological support for midwives. One midwife acknowledged the need for shared learning that could improve the midwives’ knowledge of maternal mental health:
“If you went to a short course, share the knowledge…” [Participant 2, 24-years-old, Midwife]
The same midwife and another were specific about the need to address the emotional toll resulting from their work, including supporting each other:
“…..Midwives need help psychologically... we need to consult because we experience a lot in the workplace” [Participant 2, 24-years-old, Midwife]
“Midwives need to build a common ground... use each other’s strengths (e.g., counseling skills. If shortage is addressed... and teams work together, holistic care improves” [Participant 9, 29-years-old, Midwife]
These practical solutions are proposed to ensure that there is close collaboration among other healthcare teams and the midwives, dedicated support to the midwives, and commitment to addressing staff shortages, which in turn will be beneficial to the mental health of women during the perinatal period.
4. DISCUSSION
Our findings reveal a complex interplay of barriers that hinder early identification of perinatal depression in South African primary care settings. These barriers are identified at sociocultural, systemic, and individual provider levels, creating a revolving cycle that leaves perinatal depression undetected and untreated. The study innovatively applies the Theory for Health Promotion in Nursing (THPN) to contextualize the role of a midwife not just as a healthcare provider but as a therapeutic agent contributing significantly to promote maternal mental health. Although their role is often constrained, it is dynamically shaped by their interactions with cultural norms, systemic pressures, and their own professional environments.
4.1. Social Creation of Silence: Stigma as a Barrier
The sociocultural barriers identified extend beyond individual beliefs to constitute a social construction of silence around perinatal mental health. In the communities served by these midwives, particularly Black South African communities, symptoms of perinatal depression are frequently reinterpreted through cultural scripts that characterize them as moral shortcomings, fear of motherhood, or even spiritual challenges rather than medical conditions. South Africa is a country with diverse cultural beliefs and practices. Therefore, cultural views shape how perinatal depression symptoms are perceived and understood. Our findings align with global research on mental health stigma, revealing that women at the postpartum stage fear being judged as ‘bad mothers or wives,’ thus preventing the women from connecting with others, including midwives [7].
In some South African communities, mental health issues are still not topics for discussion, thus making it difficult for the mothers to reveal to midwives any signs of change in mood or behaviour. Women are scolded when they present with mental or emotional distress, transforming their experience into a character deficiency. At the same time, in some South African cultural contexts, spiritual and cultural explanations of mental illness dominate, and as a result, the women may seek traditional help first before medical care, leading to delayed help-seeking behaviour. Notably, cultural differences related to the interpretation of mental illness exist worldwide and significantly influence how new mothers are expected to behave in this perinatal period, ignoring their emotional experiences [26]. The cultural interpretation of mental illness has consequences that link to dual stigma, that is, societal judgment and internalized shame. Similar findings are reported for patients with epilepsy who experience dual stigma due to the risk for developing depression as well [27].
Furthermore, stigma creates a challenge in the clinical environment, where the findings of this study reveal that the clinical environment further becomes an extension of the stigmatizing social environment. The attitudes of midwives during the perinatal period lead to the concealment of symptoms. A similar study revealed that patients who experienced self-stigma were reluctant to seek help when they experienced symptoms [28,29]. Furthermore, cultural and societal beliefs impact midwives’ care for women presenting with perinatal depression, including how the midwives understand and interpret the presenting symptoms of perinatal depression. This finding aligns with broader literature on mental health detection across various medical contexts. For instance, research on mental health morbidity following other health events, such as intestinal infectious diseases or epilepsy diagnosis, similarly highlights how stigma and diagnostic overshadowing can delay recognition of comorbid mental health conditions, regardless of the primary medical context [30]. This comparison highlights that the difficulty of identifying mental health challenges within physical care settings is a global concern, yet articulated within cultural lenses.
4.2. Systemic Pressures: Turning Compassion to Productivity
Beyond cultural factors, our study reveals how midwives’ attitudes within the healthcare system erode their capacity for early identification of mental health challenges in the perinatal period. It emerged in our study that midwives often present with negative attitudes towards the mothers, including them not being approachable. Their inapproachable attitudes influence how the mothers present to them, leaving them to mask or minimize the symptoms of perinatal depression. The midwives’ attitude and morale not only influence what the mothers report to them but also influence their mental health screening practices. A critical and contradictory observation is the disconnect between the midwives’ awareness of their own negative attitudes and their inability to translate this awareness into changed practice. This self-awareness indicates that the challenges are not predominantly at the individual level but also seem to be a sign of systemic distress. Most studies support the critical finding that this influences their screening practices [31, 32]. Furthermore, our study reveals considerable variation in screening practices by the midwives. This variation is because the midwives overlook mental health assessment during the perinatal period. Similar findings are reported in a study where persons with a pre-existing mental health condition experience diagnostic overshadowing, where the focus is shifted to physical symptoms [33].
Additionally, some midwives alluded to the unconducive working conditions and work constraints that led them to focus only on physical health and not prioritize the mental health of the mothers. The midwives described how working conditions, such as influx of patients, inadequate staffing, and infrastructural constraints, leave them with no time or space to conduct mental health screenings. The midwives' experience is noted to be similar in other contexts [34, 35]. High job stress and burnout levels lead to midwives’ inability to provide compassionate and effective care to women at risk for PPD [28]. The use of a screening tool during the perinatal period also adds to the inconsistencies as it assesses certain aspects of maternal health and, to some extent, mental health. Similarly, the findings of a scoping review by Shidende et al. [28] identified low screening for PPD by midwives, which is linked to the lack of resources and mental health coordination. Although the maternal screening tool accommodates mental health screening to some extent, it is still not incorporated early in the pregnancy, but only at the postpartum period. Additionally, time limitation and work overload were cited as obstacles for the midwives to conduct thorough mental health screenings during postpartum visits.
4.3. Moving to Ideal Maternal Mental Health Care: Evaluating Solutions
Solutions proposed by midwives, such as education, mandatory screening, and systemic support, indicate their understanding of what is required to improve maternal mental health. The feasibility of these solutions must be critically evaluated against the identified hindrances. Therefore, cultural understanding of perinatal depression should be addressed through community educational initiatives. These solutions are proposed by the midwives in this study, where they suggest that engaging with the communities, families, and mothers will assist in improving the understanding of perinatal depression. Our findings concur with those of Devi [3], who identified educational programs as beneficial in reducing stigma and raising awareness of PPD. The improved patient communication strategies emerged as key to eliminating barriers to early detection of perinatal depression. Therefore, the midwives in this study suggested that a friendly environment with approachable midwives could create a safe space for mothers to report symptoms of depression at an early stage.
The appropriate use of screening tools during the perinatal period could be beneficial. The midwives in this study suggest that mental health screening during the perinatal period should be mandatory. Similarly, Hoque and colleagues [36] in their study, following the identification of 60% prevalence of PPD in women living in KwaZulu-Natal, South Africa, recommended universal PPD screening at all primary healthcare facilities. As such, integrating mental health services into obstetric or maternal care settings and peer support has demonstrated improved outcomes for women in the perinatal period [37–40]. Teamwork and support emerged as valuable in eliminating barriers to early identification of perinatal depression. As such, supporting midwives could have a sustainable impact on the midwives’ practices. Such support could include a reduction of workload to ensure quality maternal and mental health care. Additionally, collaboration with other disciplines could support midwives to deliver comprehensive care.
5. STRENGTHS AND LIMITATIONS
The study's strength lies in its use of a qualitative approach, which captured comprehensive insights from multiple perspectives of midwives of diverse ages and educational experiences. These diverse perspectives provide rich contextual insights into the hindrances affecting the early detection of perinatal depression. Both sociocultural and health care system barriers identified through the use of thematic analysis offer a holistic understanding of the unique challenges faced by midwives in the South African maternal health care settings. However, this study had limitations, including its focus on midwives’ perspectives only, without including women in the perinatal period or other healthcare professionals involved in the provision of maternal healthcare. Furthermore, the study’s context is limited to MOUs in the Tshwane metropolitan area, limiting its transferability and generalizability. The experiences of the midwives who participated in this study may not be representative of those in rural facilities due to the varying resource levels as well as patient demographics.
Additionally, this study was conducted in a specific South African healthcare context and setting, potentially limiting the generalizability to other contexts with different healthcare systems or cultural backgrounds. Therefore, interpretation should be carefully considered. Recognizing the study’s specific context, more studies should be conducted in multiple contexts with different healthcare systems and cultural backgrounds to solicit different perspectives of maternal healthcare workers and women in the perinatal period to provide broader insights.
5.1. Implications for Practice
The results of this study suggest the need for integration of mental health services into maternal health care to enhance management of women in the perinatal period who are at risk of developing perinatal depression. The following recommendations are made:
- Screening for mental health symptoms should be made mandatory early in the antenatal period and continue during the perinatal period at different intervals during follow-up visits. Additionally, screening tools should be standardized and tailored for the detection of perinatal depression.
- Training and professional development for midwives need to focus on preparing the midwives for the detection and management of perinatal depression, including a focus on improving their perinatal mental health literacy. The curriculum for training midwives needs to be reviewed to integrate mental health content into midwifery training. This should include advanced communication skills with particular focus on cultural sensitivity to enable the midwives to respond to diverse populations, particularly in the South African context, and to create a safe space for women in the perinatal period to disclose their symptoms. Furthermore, professional development programs for midwives should be made available in the form of short learning programs to update the knowledge of midwives.
- Lastly, culturally sensitive educational programs should be developed to increase awareness about perinatal depression, address misconceptions and stigma for the women, their families, and communities.
CONCLUSION
The results of this study provide valuable insights into midwives’ perspectives. Both sociocultural and health care system barriers identified offer a holistic understanding of the unique challenges faced by midwives in the South African maternal health care settings. Future research should focus on the perspectives of the women of specific cultures with perinatal depression, their partners, families, and other healthcare professionals in maternal care to obtain a comprehensive understanding to develop specific interventions for the detection and management of perinatal depression.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: K.S.D.M.: Developed the protocol for the study and conducted the interviews; A.G.M-d-B and K.P.T.: Contributed to the conceptualization of the study and thematic analysis. All authors supported the drafting and development of the manuscript; therefore read and approved the final draft.
LIST OF ABBREVIATIONS
| CHC | = Community Health Centres |
| DHET | = Department of Higher Education and Training of South Africa |
| NESP | = Nurturing of Emerging Scholar Programme |
| MOU | = Midwifery-led obstetric units |
| PPD | = Postpartum Depression |
| SANC | = South African Nursing Council |
| THPN | = Theory for Health Promotion in Nursing |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval and consent to participate in the study were received from the Sefako Makgatho Health Sciences University Research Ethics Committee, South Africa (SMUREC/H/345/2023:PG)
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was obtained from the midwives who participated in this study.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are provided within this article. However, certain data are not publicly available due to privacy or ethical restrictions, including the Protection of Personal Information (POPI) Act of South Africa.
FUNDING
This paper presents research funded through the Nurturing of Emerging Scholar Programme (NESP) through the Department of Higher Education and Training of South Africa (DHET) for degree purposes. The views expressed are those of the authors and not necessarily those of DHET.
ACKNOWLEDGEMENTS
We would like to acknowledge the midwives who work hard to provide maternal care to women in need. We also want to extend our sincere appreciation to the study participants for their valuable contribution to this study.

