All published articles of this journal are available on ScienceDirect.

Job Stress, Fatigue, and Happiness among Iranian Nurses
Authors Info & Affiliations
Abstract
Introduction
One of the fundamental steps toward enhancing productivity in the healthcare system is identifying the causes and factors, such as fatigue, job stress, and happiness, among nursing personnel. This study was conducted to determine the relationship between job stress and occupational fatigue with happiness among nurses working in hospitals affiliated with Shahroud University of Medical Sciences in 2025.
Methods
This cross-sectional study included 178 nurses who completed the Oxford Happiness Questionnaire, the Job Stress Questionnaire, and the Occupational Fatigue Questionnaire. Participants were recruited using convenience sampling. The relationships among job stress and occupational fatigue with happiness, treated as latent variables, were examined using Generalized Structural Equation Modeling (GSEM). A significance level of 0.05 was applied for all statistical tests.
Results
The results revealed a mean fatigue score of 91.8 ± 34.1, indicating that nurses in the study experience moderate levels of fatigue. The job stress score averaged 173.8 ± 21.2, which was notably above the typical threshold. Nurses' happiness levels, with a mean score of 69.7 ± 12.9, were influenced by factors such as marital status and work experience. The analysis using a Generalized Structural Equation Model (GSEM) showed a strong positive correlation between job stress and occupational fatigue. In addition, the findings highlighted a significant negative relationship between fatigue and happiness scores, showing that higher levels of fatigue are associated with lower happiness.
Discussion
The findings reveal that nurses experience high levels of job stress, while occupational fatigue is reported at moderate levels. A significant positive correlation was observed between job stress and fatigue. Moreover, an indirect relationship was identified between these factors and nurses' happiness. These results propose that both stress and fatigue have a substantial impact on nurses' well-being, influencing their overall happiness in the workplace.
Conclusion
Given these findings, it is crucial to implement targeted educational programs aimed at reducing job stress and occupational fatigue among nurses. Such interventions could lead to substantial improvements in both the variables studied and the overall happiness of nursing staff, ultimately enhancing their professional satisfaction and well-being.
1. INTRODUCTION
Human resources are widely recognized as the fundamental drivers of organizational performance, playing a central role in sustaining operations and achieving institutional goals [1]. Among organizational assets, human capital is considered the most critical determinant of productivity, especially within healthcare systems where service quality is highly dependent on workforce performance [2, 3]. Within these systems, nurses constitute one of the largest and most essential professional groups, providing continuous and direct patient care, often under demanding and stressful conditions. Prolonged exposure to such conditions may result in a range of physical and psychological consequences, including gastrointestinal disorders, cardiovascular complications, neurological fatigue, impaired concentration, maladaptive behaviors, emotional dysregulation, aggression, job stress, and occupational fatigue [4]. Job stress and fatigue represent significant problems that affect not only nurses’ professional functioning, but also their personal and family lives [5]. Consequently, improving productivity and care quality in healthcare organizations requires careful identification and management of key contributing factors, including job stress, fatigue, and overall well-being among nurses, who serve as the cornerstone of hospital-based care delivery [6].
Happiness, as a positive psychological state and an important indicator of mental health, arises from individuals’ cognitive and emotional evaluations of their lives and has a direct influence on physical and psychological well-being [7, 8]. In nursing, happiness has a meaningful role in shaping work performance, resilience, and the quality of patient care. Conceptually, happiness reflects an individual’s overall appraisal of life satisfaction and is shaped by personal attitudes, perceptions, and positive life experiences [9]. It is a multidimensional construct encompassing emotional components (such as positive affect and joy), social components (including supportive interpersonal relationships), and cognitive components (related to optimistic interpretation and information processing) [10]. Higher levels of happiness have been associated with improved workplace relationships and may contribute to reductions in job stress and occupational fatigue among nurses [11, 12].
Occupational factors are among the most prominent environmental stressors contributing to chronic psychological strain and job stress [13, 14]. Job stress is defined as a harmful physical and emotional response that occurs when job demands exceed an individual’s abilities, resources, or needs. It is recognized as one of the most common work-related health problems, second only to musculoskeletal disorders, and is strongly influenced by working conditions and organizational factors [15-17]. Such responses may manifest as maladaptive behaviors, interpersonal conflict, workplace violence, occupational accidents and injuries, or a range of physical health complaints, and are considered among the most influential contributors to psychological, physical, and behavioral disorders within organizational settings [18]. Job stress comprises several dimensions present in the work environment, including physical environmental stress, role ambiguity, and role conflict, which together reflect the overall level of occupational stress experienced by employees [19]. Both demographic and occupational characteristics have been shown to influence work-related stress among nurses. Demographic factors such as age, gender, marital status, and nationality, as well as work-related variables including job position, average weekly working hours, clinical setting, inadequate staffing levels, and shortages of essential medications and nursing equipment, have been identified as key contributors to occupational stress [20, 21]. When psychological pressure originating from the workplace becomes excessive or prolonged, it may lead to physical and mental health complications, undermine individual well-being, hinder the achievement of organizational goals, and ultimately result in reduced job performance and quality of care.
Employees exposed to such occupational stressors are at increased risk of developing occupational fatigue and burnout [14]. As noted previously, job-related stress is associated with a wide range of physical, psychological, and behavioral consequences. When stress is prolonged or intensified, individuals may develop clinically evident conditions, including depression, anxiety disorders, psychosomatic symptoms, chronic pain, reduced life satisfaction, and diminished overall well-being. Behavioral outcomes linked to job stress include occupational fatigue, absenteeism, tobacco use, sleep disturbances, inappropriate medication use, alcohol consumption, and substance dependence [22, 23].
Occupational fatigue is a condition that develops during the work period and is characterized by reduced mental and physical capacity, diminished motivation to perform tasks, a subjective sense of heaviness, slowed task performance, and decreased efficiency [24, 25]. Prolonged exposure to stress is recognized as one of the principal contributors to occupational fatigue among otherwise healthy working individuals [16].
Occupational stress, shift work, and physical workload have been consistently associated with occupational fatigue [26, 27]. In healthcare settings, occupational fatigue among nurses may lead to diminished work performance, reduced capacity to perform physical and cognitive tasks, and increased risks to patient safety and overall care quality [4, 28, 29]. Evidence from multiple studies implies that more than half of nurses experience some degree of occupational fatigue during their professional practice [30, 31]. Given the clinical and organizational importance of these issues, as well as the need to identify factors predicting job stress, occupational fatigue, and happiness among nurses, and considering the lack of region-specific evidence, the present study was designed to evaluate the levels of job stress and occupational fatigue and to examine their association with happiness among nurses working in hospitals affiliated with Shahroud University of Medical Sciences in 2025.
2. METHODS
This cross-sectional study was conducted on nurses working in Shahroud, northeast of Iran. Shahroud is a city with three general hospitals with 800 nurses (Imam Hossein, Bahar, and Khatam). Based on similar conducted studies [32] and considering a regression coefficient between happiness and job stress of 0.38, a correlation between happiness and job stress of -0.42, statistical power of 80%, and type I error of 5%, the required sample size was calculated to be 174 participants. In implementation, 178 nurses employed in hospitals affiliated with the university (Imam Hossein and Bahar hospitals) were studied in 2025. Nurses working at Khatam Hospital, affiliated with Islamic Azad University, were not included. The sampling method employed was convenience sampling. Questionnaires were distributed to all employed nurses, and those who provided consent to participate in the study and completed the questionnaires entirely totaled 178 participants. Nurses who were on maternity leave, unpaid leave, or medical leave exceeding one month were excluded from the study according to the established exclusion criteria.
2.1. Measurement Instruments
This study employed three standardized questionnaires: the Oxford Happiness Questionnaire, the Job Stress Questionnaire, and the Occupational Fatigue Questionnaire. In addition, a sociodemographic form was used to collect information on age, sex, work shift, work experience, educational level, marital status, number of children, spouse’s occupation and educational level, income satisfaction, occupational interest, place of residence, and hospital department of employment, along with other relevant demographic characteristics.
2.1.1. Job Stress Questionnaire
This instrument consists of 60 items distributed across six dimensions: role workload, which assesses the extent to which workplace demands exceed an individual’s capacity; role inadequacy, which evaluates the alignment between an individual’s skills, education, training, and experience and job requirements; role ambiguity, which measures clarity regarding job priorities, expectations, and performance evaluation criteria; role boundary, which examines conflicts between professional values and organizational role expectations; responsibility, which assesses the perceived responsibility for the performance and well-being of others in the workplace; and physical environment, which evaluates exposure to unfavorable physical working conditions. Each of the six aforementioned dimensions is evaluated through 10 items based on a five-point Likert scale (never=1, sometimes=2, often=3, usually=4, and most of the time=5). The questionnaire score range is between 60 and 300 points. Higher scores indicate greater levels of stress. Overall stress scores were categorized into four levels: low stress (score less than 99), low to moderate stress (score 100-149), moderate to severe stress (score 150-199), and severe stress (score 200 and above). The validity of the Iranian version of the questionnaire (Farsi version) was confirmed in the research by Sharifian and colleagues, and its reliability using Cronbach's alpha was 0.89 [33]. In the study by Heidari and colleagues, reliability assessment of the questionnaire using Cronbach's alpha coefficient demonstrated that the alpha coefficient for the overall job stress questionnaire score was 0.89, and for other dimensions ranged from 0.63 to 0.89 [17]. In the present study, the instrument's reliability was calculated with a Cronbach's alpha of 0.85.
2.1.2. Occupational Fatigue Questionnaire
This questionnaire contains 20 questions across five dimensions (lack of energy, physical effort, physical discomfort, lack of motivation, sleepiness), with each dimension measured by 4 questions on a 10-point Likert scale (not at all=1 to very high agreement=10). The score range for this questionnaire is between 20 and 200, where higher scores indicate greater levels of fatigue. The validity of the Farsi version of the questionnaire has been confirmed in Iran, and its reliability has been reported with a Cronbach's alpha coefficient of 0.94 [34]. In the study conducted by Heidari et al., the internal consistency of the Occupational Fatigue Questionnaire was assessed using Cronbach’s alpha, yielding a coefficient of 0.94 for the total scale and values ranging from 0.70 to 0.84 across its subscales [17]. In the present study, the reliability of the instrument was confirmed, with a Cronbach’s alpha coefficient of 0.92.
2.1.3. Oxford Happiness Questionnaire
The Oxford Happiness Questionnaire consists of 29 items encompassing five dimensions: satisfaction, positive mood, health, efficacy, and self-esteem. Each item includes four statements scored on a 4-point scale, with scores ranging from 0 to 3, where higher scores reflect greater levels of happiness. The total score ranges from 0 to 87, with higher scores indicating higher overall happiness [35]. The validity of the Persian version of the questionnaire has been established in previous studies conducted in Iran, and its reliability has been reported as 0.93 [36, 37]. In the present study, internal consistency reliability was assessed using Cronbach’s alpha, yielding a coefficient of 0.940. Based on the classification proposed by Vakili et al. [11]. Overall happiness scores were categorized into four levels: low happiness (scores < 22), moderate happiness (scores 23–44), high happiness (scores 45–66), and very high happiness (scores ≥ 67).
2.2. Ethical Considerations
All questionnaires were completed anonymously, and no identifying information was collected. Participation in the study was entirely voluntary, and informed consent was obtained from all participants prior to data collection. The study protocol was reviewed and approved by the Research Ethics Committee of Shahroud University of Medical Sciences (approval code: IR.SHMU.REC.1402.177).
2.2.1. Statistical Analysis
After data collection, analyses were performed using SPSS and Stata software. Descriptive and inferential analyses included Analysis of Variance (ANOVA), chi-square tests, and Pearson’s correlation coefficient. Generalized Structural Equation Modeling (GSEM) was applied to examine the relationships among latent variables, occupational fatigue, job stress, and happiness, as well as their associations with observed variables. A two-tailed significance level of 0.05 was considered statistically significant for all analyses.
3. RESULTS
Analysis of demographic characteristics showed that 178 nurses participated in the study and completed the questionnaires. The sample included 125 women and 53 men, with a mean age of 30.0 ± 6.3 years. Of the participants, 101 (56.7%) were single, and the remaining were married. Thirty-six nurses (20.2%) reported concurrent employment outside of nursing. Most participants held a bachelor’s degree (n = 158; 88.8%), and 104 nurses (58.4%) had more than five years of work experience. Regarding work schedules, 39 participants (21.9%) worked fixed shifts, whereas 139 (78.1%) worked rotating shifts. With respect to income satisfaction, only 17 nurses (9.6%) reported being satisfied, 83 (46.6%) reported dissatisfaction, and the remaining participants reported moderate or relative satisfaction.
Tables 1 and 2 show the total mean scores of occupational fatigue, job stress, and happiness. The mean occupational fatigue score was 91.9±34.1. The mean job stress score was 173.8±21.2, with the majority of nurses (158 participants, 88.8%) experiencing severe to very severe job stress. The mean happiness score was 69.7±12.9. The outcomes revealed that 38 nurses (21.3%) had low interest in their profession, 93 participants (52.2%) had moderate interest, and 48 participants (26.4%) had high interest in their profession. Among the job stress dimensions, role overload and role ambiguity received the highest scores in job stress. The means and standard deviations of job stress, occupational fatigue, and happiness, along with their subscale scores, are presented in Tables 1 and 2.
To examine the relationship between occupational fatigue and job stress, the mean fatigue scores across three levels of job stress were compared using analysis of variance, with results presented in Table 1. The results demonstrated that mean age, occupational fatigue, and its dimensions (lack of energy, physical effort, physical discomfort, lack of motivation, and sleepiness) showed significant differences across job stress levels (Table 1).
| Variable | Job Stress Mean±SD | Total | F | p-value | ||
|---|---|---|---|---|---|---|
| Moderate | Severe | Very Severe | ||||
| Age (year) | 28.4±5.9 | 30.56±6.28 | 27.59±5.92 | 30.0±6.3 | 2.48 | 0.09 |
| Occupational Fatigue | 78.1±30.9 | 90.7±32.6 | 118.2±37.5 | 91.9±34.1 | 7.27 | 0.001 |
| Lack of Energy | 18.8±9.7 | 23.1±9.51 | 28.6±9.2 | 23.1±9.8 | 4.83 | 0.009 |
| Physical Exertion | 13.0±6.3 | 14.1±6.5 | 21.1±10.9 | 14.6±7.26 | 8.17 | <0.001 |
| Physical Discomfort | 14.9±6.8 | 17.4±8.3 | 22.4±9.9 | 17.6±8.5 | 3.81 | 0.02 |
| Lack of Motivation | 15.4±6. 9 | 13.9±7.2 | 19.2±7.2 | 14.6±7.3 | 4.38 | 0.01 |
| Drowsiness | 15.9±7.9 | 22.2±9.4 | 26.9±9.9 | 21.9±9.6 | 6.72 | 0.002 |
| Happiness | 65.6±11.6 | 70.9±12.1 | 64.9±19.1 | 69.7±12.9 | 2.83 | 0.06 |
| Satisfaction | 12.7±3.8 | 13.7±2.97 | 12.4±4.2 | 13.5±3.2 | 1.85 | 0.16 |
| Positive Mood | 13.6±3.0 | 14.5±3.1 | 13.5±4.1 | 14.3±3.2 | 1.35 | 0.26 |
| well-being | 13.4±2.5 | 14.6±2.6 | 12.6±4.5 | 14.3±2.9 | 4.68 | 0.01 |
| Efficacy | 14.0±3.1 | 14.9±2.9 | 13.9±4. 8 | 14.8±3.2 | 1.36 | 0.26 |
| Self-esteem | 11.7±2.2 | 13.1±2.6 | 12.4±3.1 | 12.9±2.6 | 2.64 | 0.07 |
| Variable | Happiness (Mean ± SD) | F | p-value | |||
|---|---|---|---|---|---|---|
| Moderate | High | Very high | Total | |||
| Age | 27.6±5.6 | 28.4±6.5 | 31.1±5.9 | 30.0±6.3 | 4.29 | 0.02 |
| Occupational Fatigue | 112.3±38.8 | 101.6±33.8 | 85.2±32.3 | - | 6.32 | 0.002 |
| Lack of Energy | 27.88±8.98 | 25.08±8.9 | 21.8±9.9 | - | 3.33 | 0.04 |
| Physical Exertion | 19.4±11.9 | 16.5±7.8 | 13.3±6.2 | - | 5.79 | 0.004 |
| Physical Discomfort | 20.8±10.8 | 19.6±7.9 | 16.4±8.4 | - | 3.29 | 0.04 |
| Lack of Motivation | 17.8±2.9 | 17.4±8.9 | 12.8±6.0 | - | 9.22 | 0.000 |
| Drowsiness | 26.50±10.51 | 23.2±9.2 | 21.0±9.6 | - | 1.97 | 0.14 |
| Job stress | 178.5±32.4 | 177.5±24.9 | 171.5±17.7 | 173.8±21.2 | 1.79 | 0.17 |
| Role Workload | 33.9±8.6 | 31.6±5.5 | 32.2±5.1 | 32.1±5.40 | 0.66 | 0.52 |
| Role Inadequacy | 29.4±10.1 | 29.1±5.7 | 27.7±5.4 | 28.2±5.8 | 1.34 | 0.26 |
| Role Ambiguity | 30.5±9.0 | 30.6±5.7 | 31.8±5.2 | 31.4±5.5 | 0.97 | 0.38 |
| Role Boundary | 34.3±9.9 | 29.1±4.9 | 28.9±3.9 | 29.2±4.8 | 5.04 | 0.007 |
| Responsibility | 28.5±10.5 | 31.0±5.3 | 28.7±4.6 | 29.4±5.3 | 3.81 | 0.02 |
| Physical Environment | 22.0±7.3 | 26.1±8.0 | 22.2±5.9 | 23.5±6.95 | 6.40 | 0.002 |
The examination of the relationship between happiness and job stress and fatigue through comparison of mean stress and occupational fatigue scores across happiness levels is presented in Table 2. The results indicated that mean age, occupational fatigue, and its dimensions (lack of energy, physical effort, physical discomfort, and lack of motivation) showed significant differences among the three happiness levels. Comparison of job stress scores revealed differences only in three dimensions: role boundary, responsibility, and physical environment (Table 2).
Comparison of happiness and job stress according to demographic variables in Table 3 demonstrated that there were no significant differences in happiness levels based on gender, hospital department, work shift, income satisfaction, interest in the nursing profession, and hospital name. However, significant relationships existed between happiness levels and marital status and work experience variables. Additionally, significant relationships were found between job stress and work experience, as well as between job stress and happiness. Specifically, the frequency of very severe job stress was higher among individuals with less than five years of work experience compared to other groups. Furthermore, very severe job stress was lower among individuals with higher happiness levels compared to other groups (Table 3).
Based on the results of the examination among these three variables in Tables 1 and 2, a conceptual model of the relationship between the three latent variables was investigated using Generalized Structural Equation Modeling (GSEM). As observed in Fig. (1), the standardized coefficients of relationships between latent variables of happiness using structural equation modeling demonstrated a significant positive relationship between job stress and occupational fatigue (standardized beta coefficient =0.99). Additionally, a significant negative relationship existed between occupational fatigue scores and happiness scores (standardized beta coefficient= -0.059). Fit model criteria included Akaike's Information Criterion (AIC= 16279.8) and Bayesian Information Criterion (BIC= 16442.1). In the final model, only the sex variable was significant.
| Variable | Happiness; n (%) | Job Stress; n (%) | ||||
|---|---|---|---|---|---|---|
| Moderate (n=8) | Severe (n=59) | Very severe (n=111) | Moderate (n=20) | Severe (n=141) | Very severe (n=17) | |
| Gender | ||||||
| Male | 1(1.9) | 12(22.6) | 40(75.5) | 3(5.7) | 47(88.7) | 3(5.7) |
| Female | 7(5.6) | 47(37.6) | 71(56.8) | 17(13.6) | 94(75.2) | 14(11.2) |
 2 (p-value) 2 (p-value) |
5.74(0.05) | 4.13(0.13) | ||||
| Marital Status | ||||||
| Single | 6(5.9) | 42(41.6) | 53(52.5) | 12(1.9) | 77(76.2) | 12(11.9) |
| Married | 2(2.6) | 17(22.1) | 58(75.3) | 8(10.4) | 64(83.1) | 5(6.5) |
|
2 (p-value) |
9.76(0.008) | 1.68(0.43) | ||||
| Work Experience | ||||||
| <5 | 6(8.1) | 39(52.7) | 29(39.2) | 11(14.9) | 51(68.9) | 12(16.2) |
| 5-10 | 2(3.1) | 13(20.3) | 49(76.6) | 6(9.4) | 56(87.5) | 2(3.1) |
| >10 | 0(0) | 7(17.5) | 33(82.5) | 3(7.5) | 34(85.0) | 2(7.5) |
|
2 (p-value) |
29.92(<0.001) | 9.66(0.04) | ||||
| Hospital Department | ||||||
| Internal Medicine | 3(4) | 20(26.7) | 52(69.3) | 3(4) | 53(84) | 9(12) |
| Surgery | 3(7.7) | 14(35.9) | 22(56.4) | 7(17.9) | 29(74.4) | 3(7.7) |
| ICU | 2(3.1) | 25(39.1) | 37(57.8) | 10(15.6) | 49(76.6) | 5(7.8) |
|
2 (p-value) |
3.92(0.42) | 7.36(0.12) | ||||
| Work Shifts | ||||||
| Rotating | 6(4.3) | 46(33.1) | 87(62.6) | 14(10.1) | 112(80.66) | 13(9.4) |
| Fixed | 2(5.1) | 13(33.3) | 24(61.5) | 6(15.4) | 29(74.4) | 4(10.3) |
|
2 (p-value) |
0.05(0.98) | 0.94(0.63) | ||||
| Income Satisfaction | ||||||
| Satisfied | 1(5.9) | 6(35.3) | 10(58.8) | 5(29.4) | 10(58.8) | 2(11.8) |
| Somewhat Satisfied | 3(3.8) | 27(34.6) | 48(61.5) | 6(7.7) | 62(79.5) | 10(12.8) |
| Dissatisfied | 4(4.8) | 26(31.3) | 53(63.9) | 9(10.8) | 69(83.1) | 5(6) |
|
2 (p-value) |
0.40(0.98) | 8.98(0.06) | ||||
| Job Interest | ||||||
| Low | 4(10.5) | 14(36.8) | 20(52.6) | 6(15.8) | 28(73.7) | 4(10.5) |
| Moderate | 3(3.2) | 29(31.2) | 61(65.6) | 7(7.5) | 78(83.9) | 8(8.6) |
| High | 1(2.1) | 16(34) | 30(63.8) | 7(14.9) | 35(74.5) | 5(10.6) |
|
2 (p-value) |
5.74(0.05) | 4.13(0.13) | ||||
| Hospital name | ||||||
| Imam Hossein | 5(4.1) | 40(33.1) | 76(62.8) | 14(11.6) | 98(81) | 9(7.4) |
| Bahar | 3(5.3) | 19(33.3) | 35(61.4) | 6(10.5) | 43(75.4) | 8(14) |
|
2 (p-value) |
0.12(0.94) | 1.95(0.28) | ||||
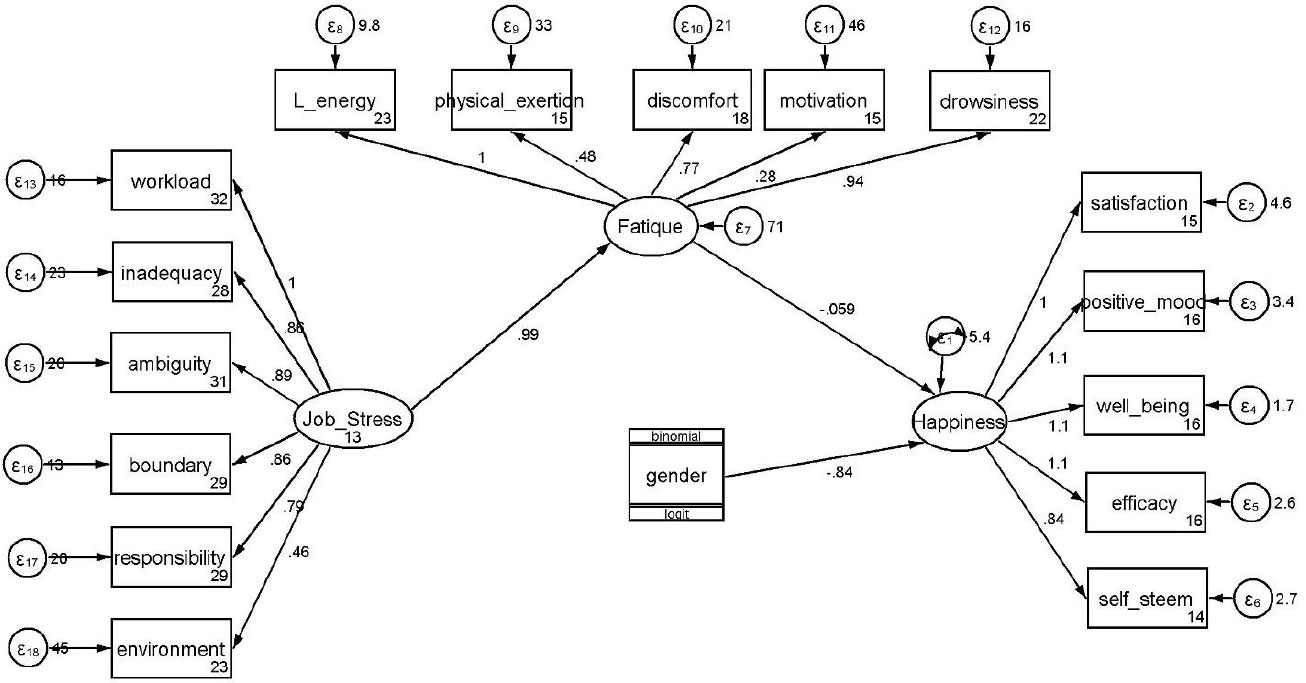
Relationships between latent variables of happiness, job stress, and fatigue using structural equation modeling.
4. DISCUSSION
The results of the present study indicate that job stress was prevalent among the majority of nurses, with workload emerging as one of the most prominent dimensions of occupational stress. Mean occupational fatigue scores among nurses experiencing severe and very severe levels of job stress were significantly higher than those observed among nurses with moderate stress levels. In contrast, no significant differences were found in mean happiness scores across different levels of job stress. While occupational fatigue demonstrated a significant inverse relationship with happiness, job stress itself did not show a significant direct association with happiness. The mean job stress score in this study was 173.8 ± 21.2, and most nurses (158 participants, 88.8%) experienced severe to very severe levels of job stress. In comparison, an Iranian study using a different measurement instrument reported a mean job stress score of 169.3 ± 14.2, with 99.5% of nurses classified as having moderate job stress, which is inconsistent with the achieved results [14]. Conversely, another Iranian study employing the same questionnaire reported a mean job stress score of 180.0 ± 23.4, which is slightly higher than that observed in the current study; however, the difference between the two studies was not statistically significant [17].
Previous studies conducted in Iran and other countries have generally reported moderate levels of job stress among nurses. In contrast, the consequences of the present study indicate high levels of job stress, with the majority of nurses experiencing elevated stress. Therefore, the moderate stress levels reported in earlier studies are not consistent with our results [16, 28, 38]. Similarly, an Iranian study using a comparable instrument reported that 22.8% of nurses experienced severe to very severe job stress, which is notably lower than the proportion observed in the present study [39].
Nursing is inherently associated with multiple occupational stressors that can adversely affect nurses’ health and contribute to heightened job stress. Given the critical role of nurses and the importance of maintaining their health, along with the well-documented impact of stress on the quality of nursing care, it is essential for healthcare administrators to implement supportive interventions. These may include counseling services, stress management programs, and opportunities for nurses to participate in decision-making processes. Among the dimensions of job stress assessed in this study, role workload had the highest mean score, whereas the physical environment had the lowest. This pattern is consistent with results from another study conducted in Iran [17].
In addition, significant associations were identified between job stress and age, work experience, and happiness levels. In contrast, a study among nurses in Saudi Arabia found no significant relationship between job stress and age or work experience, but did report significant associations with gender and educational level, which differs from the findings of our study [16].
Given the elevated scores in the workload domain, nursing managers should place particular emphasis on workload management by optimizing shift schedules and ensuring adequate staffing levels. Analysis of occupational fatigue demonstrated statistically significant differences in mean fatigue scores and their dimensions, including lack of energy, physical effort, physical discomfort, lack of motivation, and sleepiness across different levels of job stress. Nurses experiencing severe and very severe job stress reported higher fatigue levels than those with moderate stress. These conclusions are consistent with previous studies conducted in Iran, which have similarly reported significant relationships between job stress and occupational fatigue [5, 17, 40].
Nurses are frequently exposed to demanding working conditions that predispose them to fatigue, which can disrupt physical and psychological balance and increase vulnerability to mental distress.
Fatigue may also impair concentration and attention, thereby intensifying mental strain. In the present study, the mean occupational fatigue score was 91.9 ± 34.1, which is higher than that reported in another Iranian study using the same questionnaire (53.2 ± 22.5) [17]. In contrast, a study employing a fatigue questionnaire with a scoring range of 20–100 reported a mean score of 50.5 ± 12.8. Despite these variations, the present study and several others have classified occupational fatigue among nurses as moderate, which aligns with previous results [28, 40-44]. However, studies conducted in Greece have reported low levels of occupational fatigue among nurses, which is inconsistent with our results [45]. Studies from Korea and the United States, reporting moderate fatigue levels, are more closely aligned with our outcomes [4, 46].
Among the dimensions of occupational fatigue, lack of energy was the most prominent, while lack of motivation had the lowest score. A similar pattern was reported in another Iranian study using the same measurement tool, although physical effort was identified as the lowest-scoring dimension in that study [17]. Even moderate levels of fatigue may negatively affect healthcare quality, patient safety, and nurses’ well-being, while also reducing productivity and increasing organizational costs.
Accordingly, interventions aimed at reducing nursing fatigue should consider multiple factors, including organizational conditions, physical work environments, caregiving demands, available tools and technologies, and nurses’ psychological and physiological characteristics. The mean happiness score in the present study was 69.7 ± 12.9, which is above the midpoint of the scale. Previous Iranian studies using similar instruments reported mean happiness scores ranging from 64.2 to 74.4, which are comparable to the results of our research [6, 46-48]. Other studies conducted in Iran have similarly reported moderate levels of happiness among nurses [11, 49, 50]. A study conducted in Turkey using a different scale (range: 7–35) also reported moderate happiness levels among nurses (23.1 ± 5.1) [51].
Variations across studies may be attributed to differences in work environments, cultural and social contexts, organizational structures, and measurement instruments. No significant differences in happiness levels were observed with respect to gender, hospital ward, work shift, income satisfaction, interest in the nursing profession, or hospital affiliation, which is consistent with results reported in previous studies [47]. In contrast, significant associations were identified between happiness and marital status as well as work experience. Similarly, another study reported no significant relationships between happiness and gender, marital status, or educational level, which partially supports the achieved results of this study [50].
A study conducted in teaching hospitals in northwest Iran reported significant relationships between happiness and employment status, work experience, and work shift, while no associations were observed with gender, having a second job, marital status, hospital ward, or educational level. These findings partially align with this research, particularly regarding the absence of associations with gender and hospital ward [48]. In another study conducted in hospitals in Kashan, happiness was significantly associated with marital status, age, hospital ward, interest in the nursing profession, and work shift, which is consistent with the current consequences concerning the association between happiness and marital status [49].
In the final analytical model of the present study, job stress did not demonstrate a direct association with happiness; rather, its effect on happiness was mediated through occupational fatigue. In contrast, a study conducted in China reported a direct negative relationship between job stress and happiness, which is inconsistent with the present results [52].
Nurses are routinely exposed to patient suffering, demanding work environments, long working hours, and substantial emotional challenges. Prolonged exposure to these stressors may result in adverse physical and psychological outcomes. Therefore, greater attention to factors such as job satisfaction, work-life balance, and support from colleagues and supervisors may play a critical role in enhancing nurses’ happiness and should be considered at multiple managerial levels within healthcare systems [53].
5. LIMITATIONS
The relationships between latent variables in this study were examined using a cross-sectional research design, which may be subject to reverse causality bias. Also, the relationship between variables should be understood as association, not causation. Furthermore, the study sample comprised nurses working in hospitals affiliated with Shahroud University of Medical Sciences, the region's main healthcare providers; therefore, generalization of results to nurses working in private hospitals and those under the coverage of Social Security Organization and military forces is limited due to the restriction of the study to a single university. Due to this limitation, most Iranian nurses work in hospitals affiliated with medical universities. The robust study design, adequate sample size, diverse selection of nurses from different hospital departments, and utilization of standardized questionnaires constitute the strengths of this study.
CONCLUSION
Job stress levels among nurses were high, while occupational fatigue was at a moderate level. Given the significant positive relationship between job stress and occupational fatigue, and the significant negative relationship between occupational fatigue scores and happiness scores, developing educational programs to reduce job stress (reducing workplace discrimination and improving wages, enhancing working conditions and communication between staff and supervisors, training conflict management skills, improving social and managerial support in the workplace, staff empowerment and continuous personnel training to update scientific and practical knowledge, reducing role workload, and moderating working hours and shift schedules) and reducing occupational fatigue (establishing more flexible work shifts, providing supportive services such as psychological counseling, nutrition and exercise programs for nurses, improving workplace environmental conditions, and promoting a culture of health) can contribute significantly to improving the studied variables and enhancing nurses' happiness.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.A., H.V.: Study conception and design; H.V.: Data collection; A.Kh., M.B.S.: Analysis and interpretation of results; M.A., E.S.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| SEM | = Structural Equation Modeling |
| ANOVA | = Analysis of Variance |
| SPSS | = Statistical Package for the Social Sciences |
| ICU | = Intensive Care Unit |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study received ethical approval from the Institutional Review Board of Shahroud University of Medical Sciences Iran, Ethics Committee approval number: IR.SHMU.REC.1402.177.
HUMAN AND ANIMAL RIGHTS
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
AVAILABILITY OF DATA AND MATERIALS
The data sets used and/or analyzed during the study will be available from the corresponding author [A.K] upon reasonable request.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to all nursing staff at hospitals affiliated with Shahroud University of Medical Sciences who participated in this study. Special appreciation is extended to the Research Deputy of Shahroud University of Medical Sciences, Iran for their support and facilitation of this research.

