All published articles of this journal are available on ScienceDirect.

A Cross-Sectional Study on the Competency in Delivering Health Services among Barangay Health Workers in Metro Vigan: Basis for the Conduct of a Competency-based Training Program
Abstract
Introduction
This study assessed the proficiency of Barangay Health Workers (BHWs) in providing fundamental health services in Metro Vigan, Philippines. Barangay Health Workers (BHWs) are essential to the nation's primary healthcare framework, delivering services related to health education, illness prevention, maternity and child health, and health surveillance. Notwithstanding their essential function, apprehensions regarding their proficiency arise from insufficient training and resources. This study evaluates BHW competencies in five fundamental domains: health promotion, health education, station maintenance, health status monitoring, and record-keeping. It also examines the correlation between the demographic parameters of BHWs, including age, education, and marital status, and their degrees of competency. Furthermore, this study proposes a comprehensive competency-based training program for BHWs in Metro Vigan to sustain and improve their competency in delivering health services.
Methods
A descriptive-correlational study approach was utilized, employing a questionnaire derived from the TESDA Self-Assessment Guide for Barangay Health Services.
Results
The findings reveal that although BHWs typically exhibit considerable proficiency, their civil status influences their performance, especially in health monitoring and record-keeping.
Discussion
Training programs were deemed inadequate, exhibiting deficiencies in cultural awareness and communication abilities.
Conclusion
The report recommends establishing a TESDA certification program, creating targeted training initiatives, and improving feedback systems to enhance the performance of BHWs and ensure the sustainability of primary health services. This study supports the United Nations’ Sustainable Development Goals 3, 8, and 16 by encouraging skill-based programs to improve how well BHWs perform their important roles.
1. INTRODUCTION
The 1979 Alma-Ata Declaration on Primary Health Care (PHC), advocating for an increase in health personnel and enhanced community involvement, facilitated the expansion of Community Health Workers' responsibilities, encompassing health promotion and case management, supported by mounting evidence of their effective execution and cost-efficiency [1].
In the Philippines, Barangay Health Workers are authorized to operate as such by the local health board in compliance with the regulations established by the Department of Health [2]. Republic Act 7883, titled “Barangay Health Workers' Benefits and Incentives Act of 1995,” acknowledges the necessity for primary health care and organizes health workers to enhance health empowerment. The Barangay Health Worker program was initiated in the early 1980’s as part of the Philippines' strategy to implement the community health worker model for primary health care provision. This effort sought to enhance health outcomes by utilizing local volunteers to deliver basic health services and education within their communities [1].
A barangay health worker is someone who has completed training programs from recognized government or non-government organizations and voluntarily provides primary health care services in the community. They have also received accreditation from the local health board in line with the rules set by the Department of Health (DOH) [2].
Barangay health workers are a kind of community health worker who serve as health advocates and educators in their respective areas. In the Philippines, barangay health workers (BHWs) are essential in coordinating mass drug administration (MDA) as advocates, implementers, and educators [3]. They reside in the communities they serve and undergo around five weeks of training, which includes administering vaccines, measuring children's weight, and providing birthing services, among other tasks. They offer information, educational resources, and motivational services regarding basic health care, maternity and child health, child rights, family planning, and nutrition.
The Department of Health establishes the optimal ratio of barangay health workers to homes, ensuring that the total number of barangay health workers nationally does not surpass one percent (1%) of the total population [2]. Each volunteer is anticipated to assist approximately 20 families within their community. The shortage of trained personnel has reduced the number of volunteers, particularly in isolated places, where only one or two volunteers served a whole barangay [4].
Most barangay health professionals are female. They are classified as “volunteers” due to the non-permanent nature of their positions, rendering them more susceptible to the demands of the barangay captain or other important leaders who possess the authority to appoint them. They often receive an allowance and a limited array of benefits, including training, medical assistance, and groceries on special occasions [5].
Barangay Health Workers (BHWs) assume a vital role during this health crisis. Consequently, they are crucial in the endeavors of health advocates to halt the transmission of the coronavirus. At the grassroots level, they constitute the primary line of defense and serve as the connection between community members and health practitioners and institutions.
Barangay Health Workers (BHWs) have been present in the Philippines for nearly four decades and have frequently received commendations in assessments of local health systems and community engagement. However, there is insufficient comprehension of the factors that drive and sustain their engagement as community volunteers. This comprehension is essential, as the program's ongoing effectiveness and longevity depend on its capacity to inspire and engage community members to serve as peer health advocates, which is a challenge that has been acknowledged [1]. Notwithstanding the essential function of Barangay Health Workers (BHWs), the execution of measures intended to assist them, including the Barangay Health Workers' Benefits and Incentives Act (2), has been inadequate. This oversight has resulted in difficulties in maintaining the program, as BHWs frequently lack adequate assistance, compensation, and training opportunities, which undermines their motivation and capacity to execute their responsibilities efficiently [6-8]. The politicization of the BHW program via patronage politics has engendered inefficiencies that obstruct the program's objectives [6].
Certain health workers, including health professionals and Barangay Health Workers (BHWs), contend that the training provided for BHWs is inadequate, necessitating additional training. Transportation expenses to the primary health center may dissuade BHWs from participating in training [9]. The political authority of local government entities limits the efforts of barangay health volunteers [10]. There exists a belief that barangay health stations deliver subpar health services and exhibit low client satisfaction. Due to funding constraints, barangay health stations face shortages of medical supplies, prolonged wait times, deterioration of facility infrastructure, and insufficient training and staffing. The rural impoverished are the most vulnerable to inadequate sanitation, malnutrition, and insufficient hygiene initiatives. Local authorities' political, social, and economic decisions influence communities’ reliance on barangay health care.
Volunteers may frequently possess a poor understanding due to recent advancements in medicine and insufficient training. Training is essential for barangay health workers to enhance their health knowledge and proficiency, hence delivering optimal quality treatment.
The cultivation of proficiency in healthcare professions is a multifaceted process, adeptly articulated by Patricia Benner in her foundational text, “From Novice to Expert.” This paradigm, based on the Dreyfus paradigm of skill acquisition, delineates the progression of humans through five distinct degrees of proficiency: novice, advanced beginner, competent, proficient, and expert [11-13]. Benner's methodology is particularly pertinent to the examination of Barangay Health Workers (BHWs) in Metro Vigan, as it provides a significant framework for evaluating their competency and guiding the creation of specialized training programs.
Benner's paradigm fundamentally recognizes the acquisition of clinical skill not only through formal education but also through experiential learning and practical application. The inexperienced BHW, akin to any neophyte, significantly depends on regulations and procedures, devoid of the contextual insight acquired via experience. Upon reaching the advanced beginner stage, BHWs start to identify patterns and utilize their knowledge in particular contexts. The competent level is characterized by the capacity to prioritize duties and make educated judgments, whilst the proficient BHW exhibits a comprehensive awareness of patient needs and can adjust their approach accordingly. Ultimately, the professional BHW demonstrates an innate comprehension of intricate scenarios, allowing for swift and precise decision-making grounded in profound knowledge and experience [11-13].
The model's foundation in qualitative research and nursing narratives offers a pragmatic and accessible framework for comprehending skill learning in healthcare [11, 14]. This is especially significant regarding BHWs, who frequently operate in varied and demanding community environments. The model emphasizes the value of experiential learning, acknowledging that BHWs cultivate their abilities via direct engagement with community members and exposure to many health-related scenarios.
Diverse clinical environments have extensively utilized Benner's concept, demonstrating its adaptability and significance. Research indicates that the proficiency of nurses affects their roles and duties in the management of patients with congestive heart failure (CHF) and stroke [12, 15]. Expert nurses are essential for delivering high-quality patient care and results, acting as clinical role models and leaders [16].
Benner's paradigm, in addition to conventional nursing practice, guides the creation of curriculum in nursing education. The University of Liverpool's Diploma in District Nursing employed the model to amalgamate skills acquisition and clinical knowledge within post-registration courses [13]. Similarly, faculty development within healthcare simulation education has employed the concept, emphasizing the importance of structured training and mentorship [17].
Despite its extensive utilization, Benner's paradigm has encountered criticism, chiefly over its philosophical foundations. Some contend that it is more philosophical than theoretical because of its interpretive character and dependence on qualitative data [14, 18]. Nevertheless, these criticisms frequently arise from misinterpretations of the model's philosophical basis, which is grounded in interpretative and Heideggerian phenomenology [18]. This philosophical underpinning is especially pertinent to the context of BHWs, since comprehending the lived experiences of community members is essential for delivering effective care.
Although Benner's approach provides a significant framework for comprehending BHW competency, it is crucial to recognize the distinct issues and criticisms that may emerge in this setting. The model emphasizes intuitive knowledge and experiential learning, thereby challenging traditional cognitive and positivist approaches [19]. Resource-limited environments, where BHWs may lack formal training and oversight, make this aspect especially pertinent.
Furthermore, the model's emphasis on individual skill development may require modification to account for the collaborative aspects of BHW work. Community health workers frequently collaborate in teams and depend on communal support, which emphasizes the value of collective skills and shared information.
This study evaluated the proficiency of BHWs in delivering health services within the community. The findings of this study will provide a foundation for the implementation of competency-based training for Barangay Health Workers. The knowledge and skills acquired from the training can be employed to enhance health, avert diseases, and provide care to ill individuals within the community.
Ultimately, this study facilitates the achievement of the United Nations’ Sustainable Development Goal 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages, as it has the potential to address universal health care, particularly for disadvantaged populations. Barangay health workers are crucial in advancing equitable health coverage, which is vital for attaining Sustainable Development Goal 3: Good Health and Well-being. They offer various preventative, promotive, and treatments, encompassing maternity, infant, and child health care, in addition to tackling infectious and non-communicable diseases [20, 21]. Elevated moral sensitivity and work values substantially affect work engagement, corresponding with Sustainable Development Goals 3, 8, and 16, which emphasize health, decent employment, and robust institutions, respectively [22].
1.1. Objectives of the Study
This study sought to evaluate the proficiency of Barangay Health Workers (BHWs) in Metro Vigan in providing essential health services to guide the development of a competency-based training program. Specifically, it aimed to:
- Characterize the demographic and professional profile of Barangay Health Workers (BHWs), encompassing age, gender, marital status, educational qualifications, duration of service, and previous training or seminars participated in.
- Assess the proficiency of Barangay Health Workers in essential health service domains: health promotion, health education, station maintenance, health status monitoring, and record keeping.
- Analyze the correlation between the profiles of BHWs and their levels of competency.
- Propose a training program based on competencies, informed by the research findings.
1.2. Conceptual Framework
This study revolved around the paradigm presented as shown in Fig. (1), which indicates that the competencies of BHWs in Metro Vigan are influenced by their profiles.
The research paradigm shows that the competencies of the BHWs in Metro Vigan are dependent on their profile.
The research paradigm.
2. METHODOLOGY
2.1. Research Design
The study employed the descriptive-correlational method of research to describe the variables under study and determine the relationships that naturally occur between them. The descriptive correlational research design seeks to delineate the current condition of variables and investigate the interrelations among them. It does not entail experimental manipulation, rendering it appropriate for the observation of natural phenomena and correlations [23-25].
2.2. Population and Sample
The study included Metro Vigan Barangay Health Workers from Vigan City, Bantay, Caoayan, San Vicente, and Sta. Catalina. Numerous studies highlight Metro Vigan's diverse socio-demographic profile. A study of diabetes mellitus patients found that most were 50 or older, female, married, and high school graduates. Unskilled laborers with monthly family incomes of Php 5,000.00 or less predominated [26]. This demographic has limited financial means and educational attainment, which may impair health awareness and healthcare access.
A separate study of the Katarungang Pambarangay system found that most respondents were 31–40, male, married, and college-educated. These participants had lived in their barangays for over nine years, suggesting a more stable and educated demographic than the diabetic study [27]. This educational and age disparity highlights Metro Vigan's socio-demographic diversity.
Table 1 presents the distribution of respondents across the five municipalities: Bantay, Caoayan, San Vicente, Sta. Catalina, and Vigan City. The study population included all BHWs in Metro Vigan, and total enumeration was employed to include all eligible participants. A total of 884 BHWs were initially approached for participation in the study.
| Municipality | N |
|---|---|
| Bantay | 237 |
| Caoayan | 128 |
| San Vicente | 66 |
| Sta. Catalina | 123 |
| Vigan City | 330 |
| Total | 884 |
Inclusion criteria were:
(1) The Municipal Health Office (MHO) officially recognized them as Barangay Health Workers.
(2) The individual must actively engage in health service duties under the direct supervision of the Municipal Health Office (MHO).
(3) The participants must provide informed consent before participating in the study.
Exclusion criteria were:
(1) BHWs are not currently engaged in healthcare duties.
(2) The criteria also included individuals who did not possess official identification from the Municipal Health Office (MHO).
(3) Those unwilling to provide informed consent.
Eligibility was determined based on official identification by the Municipal Health Office (MHO) and active engagement in health service duties under the direct supervision of the MHO. Of those approached, all 884 met the eligibility criteria, provided informed consent to participate, and completed the survey, resulting in a 100% response rate. The final analysis included data from all participants who finished the survey. This structured recruitment and inclusion process ensures transparency in participant flow and provides a clear denominator for the study findings.
Figure 2 presents the flowchart that illustrates the recruitment process of 884 Barangay Health Workers (BHWs) in Metro Vigan.
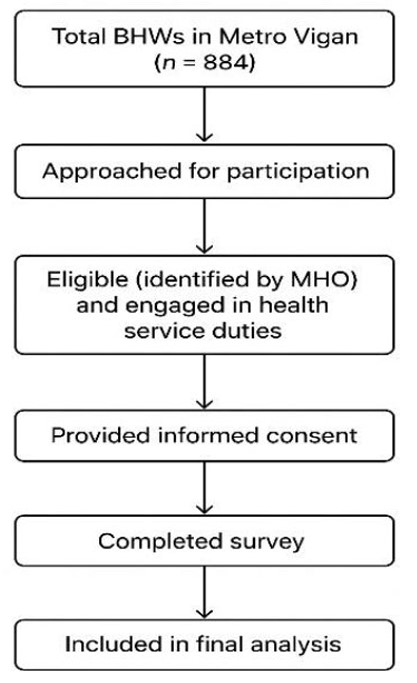
Participant recruitment flowchart.
This flowchart shows the recruitment process of 884 Barangay Health Workers (BHWs) from Metro Vigan. All were verified by the Municipal Health Offices (MHOs) as eligible, provided informed consent, completed the survey, and were included in the final analysis, yielding a 100% response rate.
2.3. Data Gathering Instrument
In gathering the data for the study, the researcher used a questionnaire checklist based on TESDA’s Self-Assessment Guide for Barangay Health Services NC II, which was translated into Iloko. The questionnaire checklist includes the following parts: Part I gathered information about the socio-demographic variables, which include age, sex, civil status, educational attainment, number of years as a BHW, and trainings and seminars attended. Part II is on the level of competency of the respondents in the delivery of barangay health services along with assisting the household to identify health problems to promote health and well-being; sharing knowledge and skills among members to provide information, education, and communication (IEC) and household teaching in disease prevention and control; ensuring the proper maintenance of the health station and safe custody of its equipment, medical supplies, materials, and health; monitoring the health status of household members under his/her area of service coverage; and maintaining updated lists/records of health activities. The following norms for interpretation were used to interpret the data:
| Range | Item DR | Overall DR |
| 4.21 – 5.00 | Always (A) | Very High (VH) |
| 3.41 – 4.20 | Often (O) | High (H) |
| 2.61 – 3.40 | Sometimes (So) | Fair (F) |
| 1.81 – 2.60 | Seldom (Se) | Low (L) |
2.4. Data Gathering Procedures
We first sought permission and approval from the university's Ethics Committee to conduct the study. After the approval, the researcher forwarded a letter to the city mayor and municipal mayors asking for permission to conduct the study in the selected study sites. After granting permission, the researcher met the respondents and explained the objectives of the study and their involvement. Upon signing the informed consent form, questionnaire checklists were distributed among the chosen respondents. The respondents were given ample time to answer the questionnaire checklist and retrieved it thereafter.
2.5. Availability of Data and Research
The data supporting the findings of this study are available at the University of Northern Philippines. Due to ethical considerations and the necessity of preserving respondent confidentiality, the raw data will not be publicly accessible. However, anonymized datasets and relevant materials may be obtained from the corresponding author upon a reasonable request and with the approval of the University of Northern Philippines.
2.6. Ethical Considerations
Before data collection, stringent ethical processes were followed. The research involving human subjects was carried out in compliance with the ethical guidelines established in the Declaration of Helsinki. The study underwent review by the University of Northern Philippines Ethics Review Committee of the university with approval number A-2022-127. Consent was secured from all relevant institutions, and participants were comprehensively briefed on the study's aims and possible advantages. To guarantee secrecy and anonymity, all data was encoded and securely stored.
2.7. Conflict of Interests
The researchers contend that there were no conflicts of interest, as the sole objective of the study was to assess the competence of Barangay Health Workers (BHWs) in delivering health services. All participants provided informed consent and were made aware of their right to withdraw from the study at any time without repercussions. Participants were promised they could refuse to answer any questions they deemed uncomfortable. Although all participants were of legal age, the researchers implemented extensive precautions to ensure their well-being during the study. The study may offer a foundational framework for the establishment of competency-based training for BHWs. Participants received no remuneration or incentives for their participation.
2.8. Statistical Treatment of Data
The following statistical tools were used to analyze and interpret the data gathered for this study:
(1) Frequency count and percentages described the socio-demographic profile of the respondents.
(2) Mean described the level of competency in the delivery of barangay health services for the respondents.
(3) Simple correlational analysis determined the relationship between the level of competency in the delivery of barangay health services and the profile of the respondents.
3. RESULTS AND DISCUSSION
This section presents, interprets, and analyzes the data gathered in the study. This study utilized the tabular and textual modes of presentation.
3.1. Personal-Related Profile of the Respondents
The distribution of the respondents in terms of the above-mentioned variables is presented in Table 2.
| Variables | f | % |
|---|---|---|
| Age | - | - |
| 60 and above | 121 | 13.69 |
| 50-59 years old | 167 | 18.90 |
| 40-49 years old | 306 | 34.61 |
| 30-39 years old | 234 | 26.47 |
| 20-29 years old | 55 | 6.22 |
| Below 20 years old | 1 | 0.11 |
| Total | 884 | 100.0 |
| Sex | - | - |
| Female | 864 | 97.7 |
| Male | 19 | 2.1 |
| No response | 1 | 0.1 |
| Total | 884 | 100.0 |
| Civil Status | - | - |
| Married | 663 | 75.0 |
| Single | 113 | 12.8 |
| Widowed | 84 | 9.5 |
| Separated | 13 | 1.5 |
| No response | 11 | 1.2 |
| Total | 884 | 100.0 |
| Educational Attainment | - | - |
| College graduate | 318 | 36.0 |
| College undergraduate | 163 | 18.4 |
| High school graduate | 292 | 33.0 |
| High school undergraduate | 64 | 7.2 |
| Elementary graduate | 47 | 5.3 |
| Total | 884 | 100.0 |
| Length of Experience as BHW | - | - |
3.1.1. On Age
The ages of the respondents varied from under 20 to over 60, with the largest proportion (34.61%) in the 40-49 age bracket. The lowest percentage (0.11%) pertains to those under 20 years of age, signifying that BHWs are primarily middle-aged adults. This number indicates that the workforce predominantly comprises seasoned persons who are presumably mature and proficient, although they may necessitate targeted treatments to sustain or augment their skills as they age.
3.1.2. On Sex
The overwhelming majority of replies are female (97.7%), and only 2.1% are male. This discovery demonstrates the gendered makeup of the BHW workforce, aligning with broader societal norms that predominantly involve women in caring tasks.
3.1.3. On Civil Status
Seventy-five percent of respondents are married. A minor percentage of the respondents are separated (1.5%). This profile indicates that most BHWs possess stable family structures, perhaps affecting their capacity to balance work and personal obligations.
3.1.4. On Educational Attainment
The predominant group of responders consists of college graduates, making up 36% of the total, while only 5.3% are elementary school graduates. The data indicate that the majority of BHWs have attained at least a secondary education, with a considerable percentage having higher educational qualifications. Educational attainment may be a pivotal determinant in their capacity to comprehend and provide health care efficiently.
3.1.5. On Length of Experience as a BHW
The largest proportion of respondents (32.4%) possess 1-4 years of experience, and 16.7% have less than one year of experience. This distribution reflects a harmonious blend of experienced and relatively novice BHWs, facilitating chances for mentorship and skill transfer within the workforce.
3.1.6. On Trainings and Seminars Attended
A notable percentage (36.9%) of participants have attended 1–4 trainings or seminars, and the fewest are those attending more than 10 (16.6%). This finding indicates that most respondents have engaged in some type of training or seminar, which illustrates the importance of ongoing professional development in improving their skills.
3.2. Core Competencies of the Respondents
3.2.1. On Health Promotion
Table 3 presents the level of competence of the BHWs in health promotion.
| Item | Items | Mean | DR |
|---|---|---|---|
| - | As a BHW, I perform the following barangay health services… | ||
| 1 | Facilitate individuals’ understanding of health services provided by agencies through use of appropriate interpersonal communication skills. | 4.34 | Always |
| 2 | Communicate the culture, practices/beliefs, needs, issues, feedback of individuals/community to service providers | 4.24 | Always |
| 3 | Identify support needed by individuals to access health services | 4.31 | Always |
| 4 | Identify aftercare/follow-up support needed by individuals | 4.23 | Always |
| 5 | Document health activities and related information | 4.33 | Always |
| 6 | Identify advice or health intervention for individual/family/household based on a given scenario | 4.26 | Always |
| 7 | Give advice to seek consultation or referral to rural health units, based on identified health symptoms | 4.29 | Always |
| 8 | Provide culturally sensitive inputs/information as guidance in health planning/intervention, following standard operating procedure | 4.16 | Often |
| - | Overall | 4.27 | Very High |
Table 3 assesses the proficiency of barangay health workers (BHWs) in health promotion. The average score of 4.27, classified as “Very High,” indicates a consistently robust performance by the BHWs in providing basic health services to their communities. This demonstrates their capacity to perform essential health-related functions proficiently, guaranteeing efficient service provision and meeting the health requirements of their local barangays.
The highest-rated competency is “Facilitate individuals’ understanding of health services provided by agencies through appropriate interpersonal communication skills” (mean = 4.34, “Always”), highlighting the BHWs' remarkable proficiency in effectively conveying health-related information. Communication is fundamental to health education, and this outcome highlights their importance as essential intermediaries between health organizations and the community. The competency with the lowest ranking is “Provide culturally sensitive inputs/information as guidance in health planning/intervention, following standard operating procedure” (mean = 4.16, “Often”). This result, although elevated, indicates a relative deficiency in the BHWs' capacity to comprehensively incorporate cultural concerns into health planning and interventions, which is essential for customizing health care to meet various community requirements.
The results indicate that, although BHWs are generally performing satisfactorily, initiatives should be undertaken to improve their cultural competence. Culturally sensitive approaches are essential for enhancing health and well-being; thus, specialized training programs that emphasize the comprehension and incorporation of cultural beliefs and practices into health interventions may enhance their efficacy. Moreover, the elevated overall competency level indicates that BHWs are strategically positioned to enhance community health outcomes; nonetheless, ongoing professional development is essential to sustain and augment their skills.
Training is an essential technique for enhancing cultural competence among healthcare professionals. It improves practitioners' knowledge, abilities, and attitudes; however, the effect on healthcare outcomes remains ambiguous. Diverse interventions, such as training and mentoring, exist to enhance cultural competency; nevertheless, further data is required to evaluate their effect on healthcare outcomes [28]. BHWs are driven by both financial and non-financial incentives, the prospect of acquiring technical expertise, and the aspiration to enhance community health and social status. Ensuring sufficient assistance and resources, including allowances and medical supplies, is essential for BHWs to fulfill their responsibilities and improve community engagement [1].
The findings illustrate the strengths of BHWs in promoting health communication, recording activities, and guiding individuals in obtaining suitable health care, as indicated by continuously elevated mean scores. Their capacity to assist clients in obtaining referrals (mean = 4.29) and recognizing health interventions (mean = 4.26) underscores their critical function in addressing disparities in primary healthcare access. The comparatively lower score in delivering culturally sensitive inputs (mean = 4.16) indicates possible constraints in tailoring health services to the distinct needs and practices of the communities served. This disparity may arise from inadequate training or insufficient exposure to culturally varied health contexts.
Improving the cultural competence of BHWs could substantially enhance their capacity to provide inclusive health services. Furthermore, the results underscore the necessity of maintaining their expertise in communication, documentation, and health guidance via frequent capacity-building initiatives. The table indicates that although BHWs exhibit high competence in their responsibilities, ongoing enhancement initiatives targeting cultural sensitivity and inclusivity could further augment their contributions to community health and well-being.
Cultural competence in healthcare means respecting and tailoring care to fit the values, needs, and behaviors of clients. This leads to better health outcomes and higher satisfaction with care [29]. Engaging effectively with ethnic minority groups is crucial for promoting fair healthcare quality and minimizing barriers to service access [30].
3.2.2. On Health Education
Table 4 presents the level of competence of the BHWs in health education.
Table 4 evaluates the competency of Barangay Health Workers (BHWs) in health education. The overall mean of 4.22, categorized as “Very High,” indicates that BHWs consistently demonstrate exceptional proficiency in providing health education and promoting awareness within their communities. This illustrates their ability to serve as efficient channels for health-related information and their dedication to disease prevention and control initiatives.
| Item | Items | Mean | DR |
|---|---|---|---|
| - | As a BHW, I perform the following barangay health services… | ||
| 1 | Identify community beneficiaries of health programs and services | 4.31 | Always |
| 2 | Discuss how to organize the network or linkages of beneficiaries to health programs/services | 4.15 | Often |
| 3 | Discuss how to establish a community relationship in accordance with the Department of Health’s objectives | 4.16 | Often |
| 4 | Demonstrate how to share knowledge or updates with fellow Barangay Health workers to provide updates on health programs/projects | 4.28 | Always |
| 5 | Present information on DOH programs, policies, infection control measures, and practices through the guidance of rural health midwife and/or nurse | 4.28 | Always |
| 6 | Observe culturally sensitive health strategies according to the needs of the individual/family/household | 4.22 | Always |
| 7 | Gather feedback on needed improvement for promotional activities | 4.12 | Often |
| - | Overall | 4.22 | Very High |
The top-rated competencies, each with a mean score of 4.28 (“Always”), are “Demonstrate how to share knowledge or updates with fellow Barangay Health Workers regarding health programs/projects” and “Present information on DOH programs, policies, and infection control measures and practices under the guidance of a rural health midwife and nurse.” These results highlight their effectiveness in doing so for the broader community. The capacity to convey information under professional supervision guarantees precision and compliance with the Department of Health (DOH) regulations.
The ability with the lowest rating is “Gather feedback on needed improvement for promotional activities,” which has a mean score of 4.12 (“Often”). Although still in the “Very High” bracket, this indicates that BHWs may face difficulties in systematically gathering and employing feedback to enhance their promotional methods. A comparatively lower score is observed in “Discuss how to organize network or linkages of beneficiaries to health programs/services” (mean = 4.15, “Often”), indicating a potential requirement for more systematic training in establishing community ties.
The findings highlight the critical role of BHWs in preventing illness and promoting health. The diminished ratings in feedback collection and network organization suggest potential for improvement in community participation and evaluation skills. Organized seminars or training sessions centered on feedback acquisition, network structuring, and connection establishment could enhance their efficacy. Moreover, formulating culturally relevant and community-focused promotional tactics might enhance their capacity to address the distinct demands of varied groups.
Structured workshops and training programs are necessary to enhance BHWs' competencies in feedback gathering, network organization, and linkage development. Proper training and assistance are essential for improving their functions in illness prevention and management [3, 31, 32]. Community health workers necessitate additional training in community participation and assessment to enhance their efficacy. This entails the formulation of culturally relevant and community-centered promotional techniques [1, 3, 6].
The results indicate that BHWs excel in essential abilities, including knowledge dissemination, providing updates, and articulating DOH policies and infection control protocols, hence underscoring their dependability in IEC activities. These qualities are essential for sustaining informed communities and bolstering public health programs. Nonetheless, the marginally reduced scores in establishing linkages and collecting feedback indicate a deficiency in including beneficiaries and assessing the efficacy of their initiatives. These duties necessitate strategic planning and systematic methodologies, which may not yet be completely cultivated among the BHWs.
Enhancing competencies in obtaining meaningful feedback and establishing networks would enable BHWs to optimize their promotional tactics and augment their outreach initiatives. Moreover, equipping them with instruments and methodologies for community evaluation and relationship cultivation could enhance their capacity to implement focused and efficient health interventions. Although BHWs demonstrate considerable skill, ongoing capacity-building initiatives are crucial to enhance their effectiveness in disease prevention and control.
Training interventions can enhance the confidence, competence, and intention of BHWs to employ behavior change approaches. Ongoing training and assessment are essential to sustain these enhancements [33]. Furthermore, effective, and advantageous supervision is essential for enhancing the performance of healthcare professionals. The most successful supervision methods remain ambiguous, highlighting the necessity for additional research and standardization [34, 35].
3.2.3. On-station Maintenance
Table 5 presents the level of competence of the BHWs in station maintenance.
Table 5 evaluates the competency of Barangay Health Workers (BHWs) in maintaining health stations and safeguarding their equipment, medical supplies, and materials. The average score of 4.31, classified as “Very High,” signifies that BHWs have considerable competence in this domain. This underscores their unwavering compliance with standards in preserving the functionality, organization, and safety of the health station and its resources.
| Item | Items | Mean | DR |
|---|---|---|---|
| - | As a BHW, I perform the following barangay health services… | ||
| 1 | Demonstrate physical inventory of equipment and medical supplies | 4.15 | Often |
| 2 | Practice proper storage of equipment and medical supplies in a designated place | 4.30 | Always |
| 3 | Demonstrate the maintenance of the cleanliness and orderliness of the Barangay health center catchment area | 4.46 | Always |
| 4 | Orient fellow health workers on the proper use and storage of equipment | 4.27 | Always |
| 5 | Practice proper filing of records for accessibility and completeness | 4.36 | Always |
| 6 | Practice proper disposal of damaged records according to the protocol of record management systems | 4.33 | Always |
| - | Overall | 4.31 | Very High |
The top-rated skill is “Exhibit the upkeep of cleanliness and orderliness of the barangay health center catchment area,” with a mean score of 4.46, translated as “Always.” This indicates that BHWs prioritize a clean and ordered environment, which is crucial for enhancing health and guaranteeing patient safety. In contrast, the competency with the lowest rating is “Demonstrate physical inventory of equipment and medical supplies,” which has a mean score of 4.15, read as “Often.” This suggests that, although BHWs acknowledge the significance of inventory management, they may not execute this duty as consistently as others, likely due to time limitations or the intricacies of inventory processes.
The results indicate that BHWs are proficient at managing health stations and protecting the resources under their stewardship. Their exceptional performance in activities such as efficient storage, meticulous record-keeping, and sanitation guarantees the efficiency and accessibility of the health station for the community. The marginally reduced score for physical inventory indicates a requirement for more systematic training or consistent scheduling for inventory management. This would enhance resource oversight, avert inventory deficits, and guarantee the accessibility of critical medical supplies.
Although BHWs excel in most domains, a significant shortcoming exists in physical inventory management. This indicates a necessity for enhanced training protocols or consistent inventory schedules to optimize resource oversight and eliminate stock deficiencies [36, 37].
The results underscore the BHWs' dedication to maintaining the efficacy and safety of the barangay health station. Activities like upholding cleanliness and accurately filing documents illustrate their recognition of the influence that organized and sanitary settings have on the efficacy of health service delivery. The diminished score in inventory management may signify a deficiency in systematic protocols or a requirement for instruments that streamline the process. Regular inventory assessments are crucial to ensure the proper stocking and operation of medical supplies and equipment, which in turn directly impacts the delivery of health services.
To rectify the deficiencies, interventions like the implementation of inventory management training and the introduction of standardized checklists may prove advantageous. Furthermore, fostering collaboration among BHWs for activities such as inventory management and storage may improve efficiency and accountability. Although the BHWs demonstrate robust skills in managing health stations, targeted initiatives to enhance specific aspects, such as inventory management, would further augment their capacity to provide effective and sustainable health services to the community. The integration of contemporary technologies, the 5S methodology, and training initiatives for inventory staff can augment efficiency and elevate service quality in medical stores [38]. Enhancing inventory management techniques is essential to keep health stations well-stocked and able to provide uninterrupted service. This process entails improved monitoring of inventory and guaranteeing prompt restocking [36].
3.2.4. On Health-status Monitoring
The level of competence of the BHWs in health status monitoring is presented in Table 6.
| Item | Items | Mean | DR |
|---|---|---|---|
| - | As a BHW, I perform the following barangay health services… | ||
| 1 | Identify the priority individual/family/household for consultation | 4.41 | Always |
| 2 | Get health data information through an interview, including vital signs and anthropometric measurements of the individual/family/household. | 4.39 | Always |
| 3 | Identify health and health-related information that needs to be monitored | 4.34 | Always |
| 4 | Identify necessary medical documents/records required by health facilities | 4.31 | Always |
| - | Overall | 4.36 | Very High |
Table 6 evaluates the competency level of Barangay Health Workers (BHWs) along with health-status monitoring. The average score of 4.36, classified as “Very High,” signifies that BHWs continuously exhibit robust competencies in health status monitoring, underscoring their dedication to the welfare of individuals, families, and households in their vicinity.
The highest-rated ability is “Identify the priority individual/family/household for consultation,” with a mean score of 4.41, interpreted as “Always.” This indicates that BHWs are proficient in prioritizing individuals or groups in need of urgent medical care, which is essential for effective health service delivery and resource distribution. The competency with the lowest rating is “Identify necessary medical documents/records required by health facilities,” which has a mean score of 4.31, interpreted as “Always.” Although still elevated, this competency suggests that BHWs may face minor difficulties in regularly recognizing or generating medical papers, potentially due to discrepancies in documentation requirements among health facilities.
The findings underscore the crucial function of BHWs in overseeing the health of their communities. Their capacity to prioritize consultations, collect health data, and manage pertinent health information guarantees prompt interventions and efficient health management. Community health workers (BHWs) are crucial in the prevention of noncommunicable diseases (NCDs) through the screening of these conditions, aiding patients in health management, and advocating for healthy habits [39]. Insufficient training and funding constrain their effectiveness, despite their contribution to malaria control initiatives [31]. The somewhat reduced score in medical documentation indicates a viable requirement for standardized protocols or supplementary training to improve their proficiency in document creation and submission procedures. These steps will enhance the efficacy of referrals and coordination with healthcare facilities.
The exceptional proficiency exhibited by BHWs in health status monitoring underscores their essential function in basic health care provision. Their proficiency in prioritizing consultations guarantees that scarce resources are allocated to those in most need, while their capability to collect and analyze health data facilitates evidence-based decision-making. The minor deficiency in document-related abilities may arise from disparate standards or a lack of consistency in health facility procedures, perhaps causing confusion among BHWs or resulting in delays in patient processing.
To resolve this, we might implement specific interventions, such as training on health documentation and partnerships with health facilities to optimize record-keeping protocols. Furthermore, providing BHWs with instruments like standardized forms or checklists for medical recording could significantly enhance their efficiency. Although the BHWs in Metro Vigan demonstrate exceptional proficiency in health status monitoring, rectifying small deficiencies in documentation procedures will enhance their contributions to the healthcare system and improve service delivery outcomes. To resolve this, specific interventions, such as training on health documentation and partnerships with health facilities to optimize record-keeping protocols, might be implemented. Furthermore, providing BHWs with instruments like standardized forms or checklists for medical recording could augment their efficiency. Although the BHWs in Metro Vigan demonstrate exceptional proficiency in monitoring health status, rectifying small deficiencies in documentation processes will enhance their contributions to the healthcare system and improve service delivery outcomes. The shift from manual to digital systems can markedly enhance the efficiency, precision, and accessibility of health-related information. This methodology can facilitate enhanced data-driven decision-making at the barangay level [40].
3.2.5. On Record Keeping
Table 7 presents the BHWs' level of competence in record keeping.
Table 7 evaluates the competency level of Barangay Health Workers (BHWs) in maintaining current lists and records of health activities, a crucial element for guaranteeing systematic and effective health care delivery. The total mean assessment of 4.31, classified as “Very High,” indicates that BHWs routinely exhibit proficient skills in recording, arranging, and reporting health data in accordance with established norms.
The top-rated competency is “Record and sort the socio-demographic data and health condition of individual/family/household according to standard protocol,” with a mean score of 4.33, interpreted as “Always.” This underscores the BHWs' remarkable capacity to gather and structure essential data that underpins community health planning and actions.
| Item | Items | Mean | DR |
|---|---|---|---|
| - | As a BHW, I perform the following barangay health services… | ||
| 1 | Record and sort the socio-demographic data and health condition of the individual/family/household based on the standard protocol | 4.33 | Always |
| 2 | Fill out applicable/standard forms to report collected data | 4.32 | Always |
| 3 | Identify specific cases that need to be reported to the supervisor. | 4.30 | Always |
| 4 | Fill out applicable/standard forms to report specific cases for the supervisor | 4.29 | Always |
| - | Overall | 4.31 | Very High |
The competency with the lowest rating is “Complete applicable/standard forms to report specific cases for the supervisor,” which has a mean score of 4.29, read as “Always.” The minor difference indicates a marginally reduced consistency in completing standardized case reporting forms, suggesting a potential need for improved familiarity with reporting procedures or form templates.
The results emphasize the significance of precise and prompt data management in community health care. Through keeping current records, BHWs guarantee that health programs and interventions are informed by data and customized to the needs of their communities. The marginally lower ranking in case reporting indicates a possible area for enhancement, as efficient reporting systems are essential for good coordination between BHWs and their supervisors. Offering supplementary training or standardized instruments could mitigate this disparity by streamlining the reporting of specific situations.
For superior healthcare, strategic planning, and policy formulation, effective data management is crucial. It ensures the efficient gathering, preservation, and utilization of data to improve care outcomes and overall well-being [41, 42]. Efficient data management systems improve transparency and facilitate data-driven decision-making, essential for community health initiatives [42, 43].
The elevated competency ratings indicate that BHWs in Metro Vigan possess proficiency in managing health-related data, essential for monitoring community health trends and pinpointing areas necessitating intervention. The capacity to document and categorize socio-demographic and health information corresponds with the increasing focus on evidence-based decision-making in public health. The marginally lower score for reporting incidents may indicate difficulties such as disparate supervisor expectations or an absence of user-friendly reporting options.
Mitigating these issues would improve the efficacy and precision of health data reporting. Training sessions emphasizing accurate form-filling methodologies, coupled with the implementation of digital tools or templates, could markedly enhance BHWs' confidence and proficiency in this domain. Utilizing digital tools in healthcare systems can enhance data collection efficiency and accuracy. Digital health interventions have demonstrated the capacity to improve the quality and efficiency of primary health care services through the provision of flexible and interoperable digital technologies [44, 45]. These instruments can enhance data management and diminish inaccuracies in health data reporting [46]. The findings highlight the critical role of BHWs in the maintenance of health records and pinpoint specific strategies to improve their effectiveness in data management and reporting.
3.3. The Correlation between the Respondents' Profiles and their Level of Competency in Delivering Barangay Health Services
Table 8 reveals the relationship between the level of competency in delivering health services among the Barangay Health Workers (BHWs) and their personal-related profiles. The overall results indicate that most of the personal-related factors have a minimal or no significant impact on BHWs' overall competency. Only civil status exhibits a significant correlation, while other variables such as age (r=-0.012), sex (r=0.010), education (r=0.005), experience (r=-0.021), and training (r=0.012) do not show any statistically significant relationships with the overall competency in delivering health services. Specifically, civil status shows a weak but significant negative correlation with the overall competency (-0.079*), suggesting that the civil status of BHWs may influence their overall performance, although the effect is small.
| Variables | Core Competencies | |||||
|---|---|---|---|---|---|---|
| Health Promotion | Health Education | Station Maintenance | Health-Status Monitoring | Record Keeping | Overall | |
| Age | 0.024 | -0.002 | -0.045 | -0.021 | -0.025 | -0.012 |
| Sex | 0.032 | -0.006 | 0.022 | -0.006 | -0.012 | 0.010 |
| Civil Status | -0.077* | -0.061 | -0.060 | -0.104** | -0.067* | -0.079* |
| Education | 0.026 | 0.004 | 0.006 | -0.010 | -0.019 | 0.005 |
| Experience | 0.013 | -0.024 | -0.049 | -0.017 | -0.030 | -0.021 |
| Trainings | 0.052 | -0.007 | -0.032 | -0.011 | 0.046 | 0.012 |
When examining the core competencies individually, civil status stands out as the most significant variable. It demonstrates significant negative correlations with several key competencies, such as “health-status monitoring” (-0.104**) and “health promotion” (-0.077*). Additionally, civil status has a negative correlation with “record keeping” (-0.067*). These negative correlations suggest that certain marital statuses, especially being married or widowed, may pose challenges for BHWs in these areas. It is possible that personal responsibilities associated with marriage or widowhood could limit the time and resources available to perform these tasks, while being single allows the respondents to focus more on carrying them out, affecting their competency in monitoring health, identifying problems, and maintaining accurate records.
The findings indicate that civil status is the most significant personal-related factor affecting the competency of BHWs in specific areas, such as health monitoring, health promotion, and record-keeping. The lack of significant correlation with training suggests that interventions focused on improving training programs may need to be reevaluated to ensure that they address the specific needs of BHWs in these areas. Furthermore, the absence of significant relationships with other personal factors, such as age, sex, education, and experience, implies that BHW performance in delivering health services may be influenced more by contextual factors like civil status than by these demographic characteristics. Therefore, any competency enhancement efforts should consider the personal circumstances of BHWs, with particular attention to those whose civil status may affect their ability to perform specific tasks.
Literature indicates that personal factors, including age, sex, education, and experience, frequently exert low or no influence on the skills of health workers, consistent with evidence that these variables do not robustly forecast overall performance in health care delivery [47]. Conversely, contextual, and psychosocial factors-such as personal obligations and living situations-may significantly influence competences, including health-status monitoring and health promotion [47]. Behavioral variables such as self-efficacy, outcome expectations, and normative attitudes are emphasized as more malleable and influential on performance than fixed demographic characteristics [47]. This corroborates the notion that civil status, which might impact personal obligations and accessible resources, may exert a distinct influence on specific competences, albeit with a minimal effect size. The absence of a substantial link with training indicates that merely augmenting training may not fulfill the specific requirements of health workers; thus, interventions must be customized to address conditions and obstacles [47].
3.4. Comprehensive Competency-Based Training Program for Barangay Health Workers in Metro Vigan
Based on the findings of the study, the following comprehensive competency-based training program has been created to further enhance the competency of the Barangay Health Workers in Metro Vigan in delivering healthcare services.
3.4.1. Program Overview
3.4.1.1. Objective
To improve the proficiency, sustainability, and efficacy of Barangay Health Workers (BHWs) in Metro Vigan, thereby ensuring the provision of high-quality primary healthcare to their communities.
3.4.1.2. Target Participants
All Barangay Health Workers in Metro Vigan (Vigan City, Bantay, Caoayan, San Vicente, and Sta. Catalina).
3.4.2. Training Modules
3.4.2.1. Succession Planning and Recruitment Module
Objective: To cultivate a sustainable workforce of proficient Barangay Health Workers by enticing younger individuals to the profession.
Table 9A presents the succession planning and recruitment model for Barangay Health Workers as the initial module of the training program. Recruitment strategies that involve youth organizations and collaborate with local educational institutions effectively broaden the pool of potential Barangay Health Workers (BHWs), as community-based recruitment and partnerships with educational sectors have demonstrated the ability to enhance the sustainability and reach of health worker programs in the Philippines and comparable contexts [48-50]. Promotional materials emphasizing the essential functions and community influence of BHWs can enhance awareness and draw new members, particularly when customized to local contexts and requirements [49, 51]. Mentorship programs, wherein seasoned BHWs mentor novices through organized meetings and protocols, have shown beneficial impacts on health worker proficiency, care quality, and institutional efficacy, with evidence indicating enhancements in both clinical and managerial results [52, 53]. Ongoing mentorship and the creation of explicit mentorship resources facilitate the incorporation and retention of new BHWs, cultivating a supportive atmosphere that promotes motivation and skill enhancement [52, 53]. Recommended evaluation approaches for assessing the efficacy of recruiting and mentorship activities include monitoring the number of recruits, collecting feedback from mentors and mentees, and administering community awareness surveys [48, 53].
| Components | Activities |
|---|---|
| Recruitment Strategies | Community engagement initiatives aimed at youth organizations. Collaborations with local educational institutions and colleges. Creation of promotional materials emphasizing BHW roles. |
| Mentorship Programs | Pairing seasoned BHWs with novice recruits. Consistent mentorship meetings and assistance. Creation of mentorship protocols and materials. |
Note: Duration: 1-2 months.
Evaluation: Quantity of recruits, evaluations from mentors and mentees, and community awareness survey.
3.4.2.2. TESDA Assessment and Certification Module
Objective: To standardize the competencies of BHWs and augment their professional credibility via national certification.
Table 9B displays the second module of the training program, which is the TESDA assessment and certification. The standardized evaluation and certification of Barangay Health Workers (BHWs) is essential for maintaining uniform quality and professional integrity within decentralized health systems. The accreditation and certification systems, particularly those associated with TESDA, can bolster the legitimacy, job security, and career prospects of BHWs, while simultaneously enhancing oversight and standardization of their performance across the nation [54]. The absence of standardized competency assessments in the Philippines has resulted in inconsistencies in BHW training and employment stability, frequently swayed by local political dynamics rather than professional credentials [1, 54]. Establishing a national certification module can mitigate these anomalies, enhance accountability, and raise awareness about BHWs as vital frontline health workers [1, 54]. These measures are acknowledged as essential for enhancing the capacity and stability of community health programs; hence, they promote improved health outcomes and professional advancement for BHWs [1, 54].
| Components | Activities |
|---|---|
| Formulation of TESDA-aligned Competency Standards | Partnership with TESDA to create uniform competency evaluations. Evaluation of current BHW job descriptions and duties. |
| Certification Procedure | Evaluation of practical abilities (e.g., vital signs, first aid). Evaluation of knowledge (e.g., health promotion, disease prevention). Evaluation of ethical behavior (e.g., secrecy, respect). |
Note: Duration: 2 Months.
Evaluation: Quantity of qualified BHWs, evaluations from assessors and candidates, and influence on professional progression.
3.4.2.3. Enhanced Training Modules
Objective: To rectify recognized shortcomings in cultural sensitivity and communication competencies.
Table 9C demonstrates the enhanced training modules for Barangay Health Workers as the third module of the training program. Augmented training modules emphasizing cultural sensitivity and communication skills have demonstrably enhanced health workers' capacity to serve different populations. Cultural sensitivity training improves and develops open-mindedness, cultural knowledge, and effective communication with minority groups, resulting in improved patient outcomes and satisfaction [55, 56]. Training in communication skills-particularly through seminars, role-playing, and case studies-enhances active listening, empathy, and conflict resolution, with role-playing techniques proving more effective than conventional lectures in cultivating verbal, listening, and feedback abilities [57-59]. Training programs that include community engagement strategies and simulations help health workers feel more confident and capable in real-life situations, which builds trust and rapport with community members [60-62]. Evaluations conducted before and after training consistently demonstrate significant enhancements in communication skills and cultural competence, thereby endorsing the incorporation of these modules into the development of health workers [55-58, 62].
| Components | Activities |
|---|---|
| Training in Culturally Sensitive Communication | Seminars on active listening, empathy, and conflict resolution. Case studies and role-playing scenarios of various groups. Instruction on regional cultural conventions and ideologies. |
| Strategies for Community Engagement | Instruction on performing community needs assessments. Methods for establishing trust and rapport with community members. Methods for conducting community gatherings and debates. |
| Role-Playing and Simulation Exercises | Simulated domestic visits and community health initiatives. Role-playing scenarios that encompass difficult communication circumstances. |
Note: Duration: 2 Months.
Evaluation: Pre- and post-training evaluations, observation of communication competencies during practical activities, and community comments.
3.2.2.4. Module on Feedback and Communication Systems
Objective: To implement structured feedback systems for ongoing enhancement.
Table 9D depicts the fourth module of the training program, which focuses on the feedback and communication systems of the BHWs. The research underscores several critical aspects that facilitate the establishment of a structured feedback and communication systems module for Barangay Health Workers (BHWs). Consistent feedback sessions and organized supervision, incorporating performance dashboards and individual discussions, have demonstrated a substantial enhancement in the productivity of community health workers and their motivation, particularly when feedback is precise and actionable [63-66]. The incorporation of digital communication tools, including mobile applications and web-based platforms, augments the efficiency of feedback mechanisms, facilitates prompt data sharing, and promotes peer-to-peer communication, thereby enhancing service delivery and responsiveness to community requirements [65, 67-70]. Implementing feedback methods that encompass both in-person and digital channels guarantees that feedback is of superior quality, timely, and actionable, effectively reaching both supervisors and frontline workers, thus reinforcing standards and accountability [65, 71]. Ultimately, the ongoing assessment and modification of feedback mechanisms, encompassing the analysis of feedback data and progressive refinements, are important for sustaining advancements in BHW performance and confirming that communication systems stay effective and pertinent to local contexts [63, 65, 71].
| Components | Activities |
|---|---|
| Regular Feedback Sessions | Planned meetings with BHWs, community people, and health officials. Creation of feedback forms and protocols. |
| Digital Communication Tools | Instruction on utilizing mobile applications and web platforms for communication purposes. Formation of a BHW communication network. |
| Feedback Loop | Establishment of a mechanism for monitoring and responding to feedback. Consistent evaluation of feedback data and execution of enhancements. |
Note: Duration: 1 Month.
Evaluation: Frequency of feedback sessions, utilization of digital communication technologies, and monitoring of feedback answers.
3.2.2.5. Inventory and Resource Management Module
Objective: To improve the capacity of BHWs to handle resources efficiently.
The fifth training module, as illustrated in Table 9E shows how to develop the inventory and resource management of the BHWs. Efficient inventory and resource management is crucial for Barangay Health Workers (BHWs) to guarantee the effective provision of health services. Digital inventory management systems can enhance workflow and resource organization; nevertheless, effective deployment necessitates sufficient training and user-friendly technology to mitigate constraints, including insufficient digital skills and technical support [72]. Divergences in resource distribution and training efficacy among local contexts can affect BHWs' proficiency in managing supplies and equipment, underscoring the necessity for standardized protocols and local capacity enhancement [54]. Active, experiential training techniques-such as behavioral modeling and practice-are superior to passive methods for enhancing knowledge and performance in resource management activities [73]. Moreover, well-structured inventory management systems in healthcare can curtail expenses, diminish resource wastage, and enhance service levels, hence bolstering the overarching goals of BHW programs [74].
| Components | Activities |
|---|---|
| Digital Inventory Management Systems | Instruction on utilizing inventory management software and applications. Formulation of standard operating procedures for inventory management. |
| Procurement and Distribution | Instruction on procurement protocols and supply chain administration. Strategies for the equitable allocation of medical supplies. |
| Maintenance and Storage of Equipment | Instruction on the appropriate utilization and upkeep of medical equipment. Protocols for the secure storage and disposal of materials. |
Note: Duration: 1 Month.
Evaluation: Precision of inventory documentation, efficacy of supply distribution, and equipment maintenance records.
3.2.2.6. The Community Engagement and Partnership Module
Objective: To enhance partnerships with community stakeholders.
The final module, which is the community engagement and partnership module for BHWs, is depicted in Table 9F Community health partnerships are acknowledged as vital for effective health promotion, as they facilitate the aggregation of resources and expertise from various sectors, enhancing empowerment and promoting a feeling of community among stakeholders [75, 76]. Strategic collaboration among community health workers (CHWs), local organizations, and government agencies enhances the design, implementation, and sustainability of health initiatives, with joint program planning and resource sharing demonstrated to improve program outcomes and community engagement [50, 71, 77]. Consistent communication, consensus-building, and written agreements-such as memoranda of understanding-are essential activities that facilitate the effective implementation and execution of community-based health programs [77, 78]. Additionally, community outreach and advocacy efforts, which include training for mobilization and the development of resources for engagement, are crucial for building trust, increasing participation, and achieving measurable improvements in health behaviors and outcomes [79-81].
| Components | Activities |
|---|---|
| Partnership Development | Workshops focused on establishing and sustaining relationships. Formulation of collaboration agreements and memoranda of understanding. |
| Implementation of Joint Program | Cooperative strategizing and execution of community health initiatives. Collaboration in resource allocation and collective training initiatives. |
| Community Outreach and Advocacy | Instruction on community mobilization and advocacy methodologies. Creation of community engagement resources. |
Note: Duration: 1 Month. Evaluation: Quantity of partnerships formed, reports on collaborative program execution, and rates of community engagement.
4. LIMITATIONS OF THE STUDY
This study focused exclusively on Barangay Health Workers (BHWs) in Metro Vigan, potentially limiting the generalizability of the results. The unique socio-cultural dynamics, economic conditions, and local health system structures in Metro Vigan may have influenced the participants' experiences and competencies in ways that are distinct from other geographic contexts. Consequently, the findings may indicate context-specific patterns rather than nationally representative trends.
The collection of data depended mainly on self-reported answers, which are naturally prone to recall bias and social desirability bias. Participants may have inadvertently exaggerated their abilities or minimized their shortcomings to conform to perceived expectations. This inclination may have resulted in a slight inflation of the competency ratings, thereby influencing the accuracy of the findings and the robustness of the observed correlations.
Furthermore, the lack of direct observation constrained the study's ability to correlate self-reported data with objective evaluations of actual practice. Because of this, the assessment of BHW proficiency was mostly based on opinion rather than actual performance, which may have made the competency assessment less valid.
The study also limited its focus to five areas of competence: health promotion, health education, station maintenance, health status monitoring, and record keeping. The study did not explore other important areas, such as getting people in the community involved, working with other health professionals, and responding to emergencies. While essential for analytical clarity, this limitation may have restricted the thoroughness of the acquired competency profile.
When observed in overall, these limitations may have affected how the results were understood by making self-perceived competence levels seem higher than they really were and by limiting the findings' generalizability and external applicability. However, the gathered insights establish a crucial basis for future research that employs wider sampling, multi-method assessment, and direct observational techniques.
CONCLUSION
This study underscores the crucial function of Barangay Health Workers (BHWs) in providing important health services in Metro Vigan, accentuating their fundamental role within the primary health care system.
The demographic profile of the BHWs, predominantly middle-aged women with secure marital and educational backgrounds, indicates a dedicated and resilient workforce. Demographic considerations, especially civil status, may affect their capacity to address future health requirements, indicating the necessity for proactive workforce planning.
The study reveals that most personal-related factors-namely age, sex, education, experience, and training-exhibit negligible influence on the overall competency of BHWs. Civil status relates to BHW competency, with negative correlations indicating that marital obligations may restrict the time and resources allocated for health service provision. Civil status specifically affects essential abilities, including health status monitoring, health problem identification, and health record maintenance, indicating the necessity for focused assistance for BHWs with caregiving duties.
The findings indicate that existing training programs may inadequately address the specific issues encountered by BHWs, especially in managing personal and professional responsibilities. Furthermore, while BHWs demonstrate considerable competence in the implementation of health programs, challenges related to cultural sensitivity, communication, and operational procedures highlight systemic issues that require structural support.
The study emphasizes the significance of incorporating civil status in competency development initiatives and advocates for a reassessment of training programs to more effectively address the special needs of BHWs. Enhancing individual competencies and the organizational frameworks supporting BHWs can maximize primary health care delivery, ensuring BHWs remain effective contributors to community health.
RECOMMENDATIONS
Based on the conclusion, the following solutions are proposed to enhance the effectiveness and sustainability of Barangay Health Workers (BHWs) in delivering primary health care in Metro Vigan:
(1) Implement the Comprehensive Competency-Based Training Program for Barangay Health Workers in Metro Vigan. Metro Vigan should implement a phased approach to the 10-month BHW training program to guarantee precise delivery of each module and facilitate ongoing enhancement. Systematic assessments must be performed to gauge efficacy and implement requisite modifications, confirming that the program adapts to the changing requirements of the BHWs and the community. This strategy will optimize the program's efficacy and longevity.
(2) Form a Multi-Stakeholder Steering Committee and Obtain Funding. A comprehensive steering committee, including representatives from the Department of Health (DOH), Technical Education and Skills Development Authority (TESDA), Local Government Units (LGUs), University of Northern Philippines (UNP), Non-Governmental Organizations (NGOs), and Barangay Health Workers (BHWs), should be established to deliver strategic oversight and facilitate interagency collaboration. We must concurrently create a comprehensive funding strategy that engages local government units, the Department of Health, and external funders to ensure long-term sustainability. It is essential to allocate adequate resources for training materials, equipment, transportation, and incentives to ensure program effectiveness.
(3) Emphasize Youth Recruitment and TESDA Certification. Implement targeted outreach methods in local educational institutions to attract prospective BHWs, paired with a formal mentorship program. Accelerate the creation of a fully equipped TESDA assessment center and guarantee that assessors undergo standardized training. Clear career progression pathways must be established and conveyed to promote TESDA accreditation and professional development.
(4) Augment Training with a Needs-Based Curriculum and Interactive Techniques. Create training modules informed by comprehensive needs assessments to personalize content for the distinct needs of BHWs. Integrate interactive pedagogical techniques, like role-playing and simulation exercises, to augment practical competencies. Consistently seek feedback from BHWs and community people to assess the efficacy of training programs and implement requisite modifications.
(5) Establish Comprehensive Feedback and Communication Systems. Implement an intuitive digital communication platform to enable seemless interaction among BHWs, the community, and health authorities. Establish standardized feedback systems and implement a transparent feedback loop to guarantee prompt replies and enhancements. Training in digital inventory and supply chain management should be implemented, with regular inventory audits, to improve resource management.
(6) Enhance Community collaboration and Facilitate Continuous Professional Development. Conduct partnership-building workshops to improve collaboration with community stakeholders and promote cooperative program planning. Form alliances with educational institutions to provide advanced certification programs and scholarships for Barangay Health Workers (BHWs). Conduct monthly seminars and workshops on emerging health challenges and establish peer-to-peer learning platforms to promote ongoing professional growth.
(7) Promote BHW Advantages and Guarantee Program Viability. Promote enhanced allowances and benefits for Barangay Health Workers (BHWs), including the examination of health insurance initiatives, and establish formal recognition programs. Deliver psychosocial support services to meet the emotional requirements of BHWs. Collaborate with local government units to include the training program in their standard health service plans, enhance local training capabilities, and record best practices to guarantee long-term sustainability.
AUTHOR'S CONTRIBUTIONS
The author confirms sole responsibility for the following: Study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| BHWs | = Barangay Health Workers |
| MDA | = Mass Drug Administration |
| CHF | = Congestive Heart Failure |
| MHOs | = Municipal Health Offices |
| IEC | = Information, Education, and Communication |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This research was approved by the University Ethics Review Committee of the University of Northern Philippines, Vigan City, Philippines. The study involved human respondents who completed a questionnaire checklist.Ethical clearance was granted under Approval Number A-2022-127.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The dataset supporting the findings of this study has been deposited in the Zenodo Repository. It can be accessed through the following DOI: https://doi.org/ 10.5281/zenodo.18050923. The data includes the SPSS output generated from the research and is available for review and verification of the reported results.
FUNDING
This study was funded by the University of Northern Philippines, Vigan City, Philippines. The funding covered theessential requirements for conducting the research, including office supplies, compensation for encoders and datagatherers, and the publication fee. No specific grant or award number was issued for this project. The researcher is a faculty member of the University of Northern Philippines, which provided institutional support for the completion of the study.
ACKNOWLEDGEMENTS
Declared none.
ARTIFICIAL INTELLIGENCE (AI) DISCLOSURE
This study employed artificial intelligence (AI) tools to assist with specific research-related tasks. ChatGPT was utilized to facilitate picture development or editing, aid in data organization and preliminary analysis, and improve the article's clarity. Consensus was utilized to aid in the literature search and evaluation by enabling the discovery and synthesis of pertinent scholarly materials. Grammarly was employed to enhance language, augment clarity, and rectify grammatical and stylistic deficiencies in the manuscript. QuillBot was employed to aid in the paraphrasing and summarization of chosen paragraphs to improve readability and coherence. All stages of the research-encompassing study idea, design, data collection, analysis, interpretation of results, and validation of findings-were executed under the direct supervision of the researchers. The researchers' experience informed all methodological choices and guaranteed the study's rigor, correctness, and ethical integrity. AI technologies functioned exclusively as auxiliary instruments and did not supplant essential scholarly discernment, intellectual input, or authorship accountability. All findings, interpretations, and conclusions articulated in this paper represent the authors' individual intellectual endeavours.

