All published articles of this journal are available on ScienceDirect.

Characteristics and Clinical Outcomes of Hospitalized COVID-19 Patients in Bojanala, South Africa
Authors Info & Affiliations
Abstract
Introduction
COVID-19 was declared a pandemic as of 23rd October 2020, followed by multiple waves, each driven by evolving SARS-CoV-2 variants. Comorbidities and age were known to influence COVID-19 outcomes adversely. This study will describe the demographic and clinical characteristics of COVID-19 patients hospitalized at public healthcare facilities.
Methods
A descriptive, analytical cross-sectional study was conducted using retrospective medical records of patients admitted with confirmed COVID-19 to five public hospitals in Bojanala District, North West Province, South Africa, from May to July 2020. All laboratory-confirmed COVID-19 patients admitted during this period were included. Descriptive statistics summarised patient profiles, while inferential analyses, including Chi-square tests, Mann-Whitney U tests, and multivariable logistic regression, were used to identify associations with mortality.
Results
Medical records of 289 patients were included; a mean age of 45 years was observed, and most were male 57.1%. Hypertension, diabetes mellitus, and HIV were the most common comorbidities. Patients with two or more comorbidities experienced significantly higher mortality 46.2% compared to those with none or one. Multivariate analysis revealed that the use of antibiotics and anticoagulants remained independently associated with increased risk of death, even after adjusting for age and comorbidity burden. Conversely, age and comorbidity count lost significance after adjustment, suggesting their predictive effect may be mediated through clinical severity and treatment intensity.
Discussion
Globally, variations in findings were noted in studies. Age, male gender, and multimorbidity were significant independent variables associated with severe COVID-19 outcomes and mortality. In most studies, older age and male gender were significant factors associated with mortality. The study reports that the correlation between the use of antibiotics, anticoagulants, and mortality was likely the result of these interventions functioning as indicators for advanced clinical severity rather than direct contributors to adverse outcomes.
Conclusion
Length of hospital stay was significantly shorter for patients who died compared to those who recovered. Emphasis on early screening of high-risk COVID-19 patients in settings with limited resources is advised, particularly older male patients with multimorbidity, including hypertension, diabetes, and HIV.
1. INTRODUCTION
Severe Acute Respiratory Syndrome (SARS-CoV-2), the virus responsible for COVID-19, emerged as a global public health challenge, placing substantial pressure on healthcare systems worldwide [1]. First identified in Wuhan, China, in December 2019, SARS-CoV-2 belongs to the coronavirus family [1, 2]. As of October 2023, the global mortality burden from COVID-19 exceeded 6 million, with over 3 million fatalities in the United States of America alone [1, 3]. As of January 2020, the World Health Organization declared COVID-19 a global pandemic following its rapid spread [4]. It was widely believed that the virus originated through zoonotic transmission from animals, most likely bats, to humans [5]. Although two competing hypotheses remain, natural zoonotic spillover versus a laboratory-associated incident, no conclusive evidence has definitively supported either [5-6]. In Africa, the spread of the COVID-19 pandemic was marked by various factors, including transmission dynamics, public health responses, and regional healthcare capacity [7]. While SARS-CoV-2 spread across nearly all African countries within three months, the continent reported lower transmission and mortality rates compared to other regions [8, 9]. South Africa, however, had the most COVID-19 cases and fatalities on the continent [8, 10].
Globally, successive waves of COVID-19 were driven by emerging viral variants, raising concerns about diagnostic efficacy, treatment responses, vaccine effectiveness, and disease severity [11, 12]. In both developed and developing countries, delayed care-seeking, limited access to healthcare, and underlying comorbidities were identified as major contributors to adverse outcomes. Studies linked conditions, including hypertension, diabetes mellitus, cardiovascular disease, chronic obstructive pulmonary disease, malignancy, and smoking history, to poorer COVID-19 outcomes [13, 14]. These comorbidities are thought to worsen disease progression through immune dysregulation, systemic inflammation, and endothelial dysfunction.
Whereas international data is abundant, there remains a lack of region-specific evidence documenting the highest incidence of COVID-19 cases and fatalities across the continent concerning clinical characteristics and outcomes of hospitalized patients in environments with limited resources. Bojanala, a district in South Africa’s North West province, exemplifies such a context. The country’s dual healthcare system, characterized by marked inequalities in access, provides a unique environment for examining the clinical burden of COVID-19 [15]. Therefore, the objectives of this study were to assess demographic characteristics, comorbidity burden, treatment interventions, and clinical outcomes of hospitalized patients with confirmed COVID-19 infection.
2. METHODOLOGY
2.1. Study Design
A retrospective analytical study was conducted across five public hospitals in the North West Province of South Africa. The data was retrieved from paper-based patient medical records for the period between May and July 2020, which corresponded to the first wave of the COVID-19 pandemic in the country. The study sought to assess demographic characteristics, comorbidity burden, treatment interventions, and clinical outcomes among hospitalized patients with confirmed COVID-19 infection.
2.2. Study Setting
The study was conducted in five public health facilities in the Bojanala district, North West Province, in South Africa. Participating hospitals in the COVID-19 response effort included a regional hospital, three district hospitals, and a field hospital, which the district mandated be responsible for the admission of patients with confirmed diagnoses. The facilities were designated to treat patients who tested positive for COVID-19, each facility playing a pivotal role in managing the healthcare demands during the pandemic. (Fig. 1) shows the map of the Bojanala District where the data were collected. There are four districts in the North West Province, with Bojanala being the largest, having a population of 1.62 million people according to the Department of Statistics 2023 Census [16]. The area of Bojanala District is 18,333 km2, and is made up of five regional governments, namely Kgetleng Rivier, Madibeng, Moses Kotane, Moretele, and Rustenburg, which have a total of 139 wards. It is situated within a mining area, along the N4 National Road, running from the Botswana border into the Mpumalanga Province. Most of the district's population is black Africans, making up 98% of the overall population, with whites making up 2% of the total population [17]. Most of the population (84%) relies on public health facilities, while roughly 16% is covered by medical schemes that provide them access to private healthcare services. A small proportion of individuals use both public and private facilities. All patients hospitalized at any of the five designated public health facilities in the Bojanala District who had a laboratory-confirmed diagnosis of COVID-19 were included in the study. The study employed a census sampling approach, capturing the entire eligible population during the enrolment period from May to July 2020, which corresponded with the peak of the first COVID-19 wave in the North West Province. This period was selected to ensure uniformity in treatment protocols and to reflect the healthcare system's response during the height of the pandemic. A total of 289 patients met the inclusion criteria and were enrolled. By including all eligible cases, the study aimed to maximize data completeness and avoid sampling bias within the defined setting. The sample size of this study was relatively small compared to studies conducted in similar regions. In South Africa, the rollout of electronic health record platforms is still under development, and public health facilities remain reliant on paper-based or partial documentation systems [18]. A recent qualitative study of the South African public health sector showed that, despite existing policy frameworks on rolling out a comprehensive national electronic health system [19]. Some barriers, including deficiencies in infrastructure, interoperability, and leadership, still exist. An integrated electronic repository for the reliable extraction of population-level clinical data is absent, and patient records are fragmented across hospitals, maintained in paper-based files, and not incorporated into any centralized system that facilitates large-scale epidemiological analysis.

Map of South Africa showing the location of hospitals in the North West Province, Bojanala District Municipality [20].
2.3. Inclusion and Exclusion Criteria
The study included medical records of both male and female patients of any age group with confirmed laboratory COVID-19 positive results between May 2020 and July 2020. The selected timeframe represents the onset and escalation of the initial COVID-19 wave in the Bojanala District. The district started reporting an ongoing increase in new infections after the initial cases were identified in late March. Bojanala district experienced a significant increase in community transmissions, reflecting the national peak, with particularly high case increases attributed to mining activities, densely populated areas, and workforce mobility. The period saw the highest number of hospital admissions in district hospitals just before the second wave, with healthcare providers working under rapidly changing national guidelines and limited resources.
The focus on this time frame provides a representative depiction of the district's early high-burden period during which systems were severely strained, and protocols were still being established. Only patients hospitalized in any of the five public health facilities in the Bojanala District were included. Patients were not considered if they were admitted to any of these health facilities, were hospitalized in private health institutions, declared dead on arrival, admitted outside the specified period, or classified as persons under investigation without confirmed test results.
2.4. Data Collection
Trained research assistants, including doctors and nurses, were assigned to each facility for data collection. A standardized data collection tool, adapted from previously published research, was used to capture demographic and clinical information [21]. The tool captured key variables, including demographic data, comorbidities, treatment measures, length of hospital stay, and clinical outcomes. Information from the literature was used to develop the tool.
A nearby hospital served as the pilot site to assess the user-friendliness of the data collection tool. The purpose of the pilot study was to identify and eliminate ambiguities, ensuring standardization and alignment with the objectives of the study. Following the pilot study, an identifying marker was added to the tool's numbering system. Additionally, each research assistant underwent separate training sessions before data collection to ensure consistency and standardization across all facilities. Patient data was obtained from admission records across various wards in each medical facility. Administrative clerks assisted in retrieving patient files, which were then assigned an identifying number. Key details, including demographic information, comorbidities, treatment, clinical outcomes, and length of hospital stay, were extracted and recorded using the standardized data collection tool.
2.5. Data Analysis
Microsoft Excel was used to input data and subsequently imported into IBM SPSS Statistics version 29 for analysis. Descriptive statistics were used to summarize demographic variables, comorbidities, treatment types, and clinical outcomes. Means and standard deviations were calculated for continuous variables, while frequencies and percentages described categorical variables. To examine associations between independent variables and in-hospital mortality, a binary logistic regression model was developed. The outcome variable was patient status: died or transferred to high care vs. recovered. Predictor variables included age, sex, length of hospital stay, comorbidity burden quantified as the count of recorded chronic medical conditions, and treatment variables, which included antibiotic use, anticoagulant therapy, corticosteroid therapy, and oxygen supplementation. Individual comorbid conditions were not analysed separately due to low frequency and incomplete severity grading; therefore, comorbidity burden was assessed as the total number of chronic conditions per patient.
Age, length of hospital stay, and comorbidities were analyzed as continuous variables. Sex and all treatment variables were analyzed as binary variables (yes/no), with the “no” category identified as the reference group. The variables were entered into the multivariable logistic regression model using the enter method, as all predictors were deemed clinically significant. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported to assess the strength and direction of associations. A p-value of <0.05 was considered statistically significant. Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test, and discrimination was evaluated using the area under the receiver operating characteristic ROC curve. This regression analysis was included to adjust for confounding factors and strengthen the causal interpretation of mortality risk factors within this non-randomized sample.
3. RESULTS
3.1. Baseline Characteristics and Clinical Outcomes
Medical records of 289 patients were included in the study. The mean age was 45 years, and the age ranged from 13 to 87 years. The large group 97 (33.6%) was over 50 years of age, followed by 79 (27.3%) in the 31–40 age group and 78 (27.0%) in the 41–50 age group. Male patients constituted nearly 60% of the cohort, slightly outnumbering females. The demographic characteristics of patients are shown in (Table 1).
| Characteristic | Frequency (%) |
|---|---|
| Age groups | - |
| 30 years and younger | 35 (12.1) |
| 31 - 40 years | 79 (27.3) |
| 41 - 50 years | 78 (27) |
| Older than 50 years | 97 (33.6) |
| Mean ± Std = 45.7 ± 13.9, Min = 13, Max = 87, Percentiles 25 = 35, 50 = 44, 75 = 54.5 | |
| Gender | - |
| Female | 124 (42.9) |
| Male | 165 (57.1) |
| Hospital | Frequency (%) |
| Field Hospital | 171 (59.2) |
| Regional Hospital | 63 (21.8) |
| Three district hospitals | 55 (19) |
| Ward | - |
| General ward | 271 (93.8) |
| High care | 11 (3.8) |
| Intensive care unit | 7 (2.4) |
| Length of hospital stay | - |
| 1 - 5 days | 74 (25.6) |
| 6 - 10 days | 137 (47.4) |
| 11 - 15 days | 64 (22.1) |
| More than 15 days | 14 (4.8) |
| Mean ± Std = 8.3 ± 4.4, Min = 1, Max = 27, Percentiles 25 = 5, 50 = 8, 75 = 11 | |
| Treatment | - |
| No treatment | 100 (34.6) |
| Drug treatment | 119 (41.2) |
| Drug and oxygen treatment | 59 (20.4) |
| Drug and NIMV/ IMV | 11 (3.8) |
| Clinical outcomes | - |
| Died or transferred to high care | 49 (17.0) |
| Recovered | 238 (83.0) |
Field hospitals accommodated most admissions, with 171 patients (59.2%) managed in these facilities. Admissions to the regional and district hospitals were nearly equal, with 63 (21.8%) and 55 (19.0%) patients, respectively. Following national COVID-19 isolation protocols at the time, all patients who tested positive were required to isolate for 14 days from the date of diagnosis [22]. Those unable to isolate safely at home were admitted to the field hospital for the duration of their isolation period. This policy was later revised, reducing the required isolation to 10 days [22]. The mean length of hospital stay was 8 days, with a minimum of 1 day and a maximum of 20 days. Nearly half of the patients, 137 (47.4%), were hospitalized for 6–10 days, followed by 74 (25.6%) who stayed for 1–5 days. A further 64 (22.1%) stayed for 11–15 days, and 14 (4.8%) remained in hospital for more than 15 days. Patients were admitted to general wards, high-care units, or intensive care units based on their clinical severity. Treatment modalities varied; notably, 34.6% of patients required no treatment, indicating an asymptomatic or mild disease course. Pharmacological treatment alone was administered to 41.2%, while 20.4% received both medication and oxygen therapy. Only 3.8% required ventilatory support. The mortality rate was 23%, while most patients, 240 (83.0%), were treated and discharged. Nine percent were moved from district or field hospitals to the regional hospital for further care. Hospital admission, treatment characteristics, and clinical outcomes are shown in (Table 1).
3.2. Patient Comorbidities
Comorbidity profiles were recorded for all admitted patients, including conditions such as hypertension, diabetes mellitus, HIV, cardiovascular disease, cerebrovascular disease, chronic renal disease, cancer, obesity, and chronic liver disease. A total of 211 patients (73.0%) had one or no comorbidities, of whom 203 (96.2%) recovered, and 8 (3.8%) died. Among those with a single comorbidity, 80 patients had hypertension, with 66 (82.5%) recovering and 14 (17.5%) dying. Thirteen patients had diabetes mellitus; five recovered, while five died, and outcome data were incomplete for the remaining cases. Of the 31 patients identified as HIV-positive, 27 (87.1%) recovered while four (12.9%) died. In contrast, patients with multiple comorbidities (n = 50; 17.3%) had poorer outcomes, with only 35 (70.0%) recovering and 15 (30.0%) dying.
3.3. Demographic, Hospital Length of Stay, Comorbidities, and Treatment versus Outcomes of Patients with COVID-19
The demographic data, clinical characteristics, and treatment modalities of patients who recovered (n = 238) and those who died or were transferred to high care (n = 49) are presented in Table 2. The mean age of patients who experienced adverse outcomes was considerably higher than that of those who recovered (43.3 ± 13.2 years; p < 0.001). There was no statistically significant difference in outcomes between male and female patients (p = 0.957). A prolonged average length of hospital stay (8.7 ± 4.0 days) was observed in recovered patients compared to those who died or were transferred (6.8 ± 5.5 days; p < 0.001). The mortality rate was highest among patients with two or more comorbidities (46.2%), compared to those with one (9.6%) or no comorbidities (7.9%) (p < 0.001). The use of analgesics, antibiotics, anticoagulants, corticosteroids, oxygen, and non-invasive mechanical respiration was significantly higher in patients who experienced adverse outcomes (all p-values < 0.001). Notably, all patients who received no treatment showed recovery.
| Characteristic | Recovered (n = 238) | Died or Transferred to High Care (n = 49) | P-value |
|---|---|---|---|
| Age (years) | - | - | - |
| Mean age | 43.3 ± 13.2 | 61.2 ± 11.1 | <0.001 |
| Gender | - | - | - |
| Male | 135 (82.8) | 28 (17.2) | 0.957 |
| Female | 103 (83.1) | 21 (16.9) | |
| Length of hospital stay | - | - | - |
| Mean days | 8.7 ± 4.0 | 6.8± 5.5 | <0.001 |
| Comorbidity | - | - | - |
| No comorbidity | 128 (92.1) | 11(7.9) | - |
| One comorbidity | 75(90.4) | 8(9.6) | <0.001 |
| Two or more comorbidities | 35 (53.8) | 30(46.2) | - |
| Treatment | - | - | - |
| No treatment | 100(100) | - | - |
| Analgesic | 137(73.7) | 49(26.3) | <0.001 |
| Antibiotic | 97(67.8) | 46(32.2) | <0.001 |
| Anticoagulants | 50(56.2) | 39(43.8) | <0.001 |
| Corticosteroids | 55(59.8) | 37(40.2) | <0.001 |
| Oxygen | 30(51.7) | 28(48.3) | <0.001 |
| NIMV | 1(10.0) | 9(90.0) | <0.001 |
3.4. Univariable and Multivariable Logistic Regression for Predictors of Mortality in COVID-19 Patients
The findings of univariate and multivariate logistic regression analyses conducted to identify predictors of death or transfer to high care among hospitalized COVID-19 patients are presented in Table 3. In univariate analysis, increasing age was significantly associated with adverse outcomes (OR = 1.07; 95% CI: 1.05–1.10; p < 0.001). However, in the multivariate model, this association was not statistically significant (aOR = 1.02; 95% CI: 0.99–1.05; p = 0.153). Gender was not found to be a significant predictor of mortality in either the univariate (OR = 1.02; 95% CI: 0.55–1.89; p = 0.957) or multivariate analysis (aOR = 1.86; 95% CI: 0.85–4.07; p = 0.118). Shorter hospital stay was significantly associated with death in the univariate model (OR = 0.88; 95% CI: 0.81–0.96; p = 0.004), but this association did not remain significant in the adjusted model (aOR = 0.94; 95% CI: 0.87–1.01; p = 0.103). The number of comorbidities showed a significant association with death in the univariate analysis (OR = 2.27; 95% CI: 1.69–3.07; p < 0.001), though it lost statistical significance after adjustment (aOR = 1.10; 95% CI: 0.73–1.66; p = 0.639). Use of antibiotics was strongly associated with mortality in both univariate (OR = 22.29; 95% CI: 6.74–73.72; p < 0.001) and multivariate analyses (aOR = 6.00; 95% CI: 1.44–25.06; p = 0.014). Patients receiving anticoagulants had significantly higher odds of mortality in the univariate analysis (OR = 14.66; 95% CI: 6.85–31.40; p < 0.001), and this association remained significant after adjustment (aOR = 7.13; 95% CI: 1.24–41.03; p = 0.028). Corticosteroid use, which was significantly associated with mortality in the unadjusted analysis (OR = 10.26; 95% CI: 5.01–21.02; p < 0.001), did not remain statistically significant in the multivariate model (aOR = 0.36; 95% CI: 0.07–1.94; p = 0.237). Lastly, oxygen therapy was associated with adverse outcomes in univariate analysis (OR = 9.24; 95% CI: 4.67–18.30; p < 0.001), but this association was not statistically significant after adjusting for confounding variables (aOR = 1.96; 95% CI: 0.81–4.71; p = 0.134).
| Univariate | Multivariable | |||
|---|---|---|---|---|
| Predictor | Crude OR (95% CI) | p-value | Adjusted aOR (95% CI) | p-value |
| Age | 1.07 (1.05-1.10) | <0.001 | 1.02 (0.99-1.05) | 0.153 |
| Gender | 1.02 (0.55-1.89) | 0.957 | 1.86 (0.85-4.07) | 0.118 |
| Length of hospital stay | 0.88 (0.81-0.96) | 0.004 | 0.94 (0.87-1.01) | 0.103 |
| Comorbidity | - | - | - | - |
| Comorbid count | 2.27 (1.69-3.07) | <0.001 | 1.10 (0.73-1.66) | 0.639 |
| Treatment | - | - | - | - |
| Antibiotic | 22.29 (6.74-73.72) | <0.001 | 6.00 (1.44-25.06) | 0.014 |
| Anticoagulant | 14.66 (6.85-31.40) | <0.001 | 7.13 (1.24-41.03) | 0.028 |
| Corticosteroid | 10.26 (5.01-21.02) | <0.001 | 0.36 (0.07-1.94) | 0.237 |
| Oxygen therapy | 9.24 (4.67-18.30) | <0.001 | 1.96 (0.81-4.71) | 0.134 |
3.5. Model Strength and Predictive Utility
The Receiver Operating Characteristic curve yielded an Area Under the Curve of 0.92, demonstrating excellent discriminatory performance. The ROC curve analysis for the final logistic regression model is provided in Fig. (2). The sensitivity was 91%, and the specificity was 78%, confirming the model's effectiveness in predicting adverse COVID-19 outcomes. The final logistic regression model exhibited high discriminatory ability with an AUC of 0.92. High sensitivity and specificity indicate clinical utility in flagging high-risk patients. The absence of significance for age and comorbidities in the adjusted model highlights the complex interaction between clinical factors, possibly due to multicollinearity or shared predictive weight with treatment indicators.
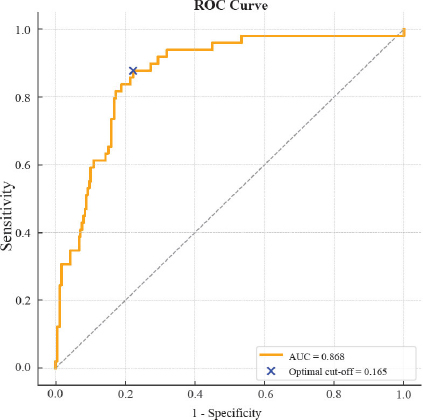
ROC curve analysis for the final logistic regression model.
4. DISCUSSION
This study was conducted in five public healthcare facilities in the Bojanala district of the North West Province in South Africa to explore the demographic profile, multimorbidity, and outcomes of admitted patients with confirmed COVID-19.
Variations in patient demographics and outcomes from this study and other regions were observed. Studies conducted in KwaZulu-Natal and Cape Town, South Africa, showed that advanced age and comorbidities were independent risk factors associated with adverse COVID-19 severity and mortality [21, 23]. The findings of this study were similar to those of studies conducted in South Africa and other regions. In studies conducted in the USA and China, older patients, male gender, and presence of multimorbidity were associated with the risk of mortality [24, 25]. There are differences noted in findings of various COVID-19 studies, possibly influenced by the methodologies used in each study, the criteria for hospital admissions, patient health-seeking behaviour, and prevalence and severity of chronic conditions in different regions [26].
Healthcare systems and utilization were affected globally by the COVID-19 pandemic due to a combination of factors. In this study, patient health-seeking behaviour, financial constraints, chronic disease burden, and lockdown regulations likely affected some patients in seeking timely medical care. The delay of regular monitoring and treatment might lead to insufficient disease management, which would eventually lead to an increase in the risk of complications, long-term impairment, and a higher cost on the healthcare system in the future [26].
In a study conducted in China on COVID-19 severity and mortality, with a focus on gender variations, found that among older patients who died, more than 70% were male [27]. Although susceptibility and ages were comparable between males and females, males were more likely to experience adverse outcomes than females. The association between male gender and mortality was linked to male health-seeking behaviour and life expectancy in China and possibly globally.
Although our findings indicate that the mean age of patients who died was significantly higher than that of patients who recovered, age was not a predictive factor for mortality. Male patients represented a larger proportion of this study; however, there were no differences in mortality between male and female patients. Similar studies in South Africa and other regions reflect that male patients were associated with severe COVID-19 outcomes and mortality; our findings reflect no age or gender differences in adverse outcomes.
South Africa has a high prevalence of HIV, diabetes, hypertension, and arthritis compared to most regions on the continent and globally [28]. Often, older populations require regular screening, given the high prevalence of multimorbidity in this population.
We studied the correlation between multimorbidity and COVID-19 outcomes. The severity and management of chronic conditions were not established due to the retrospective nature of the study design, and public health facilities rely on paper-based systems, while the rollout of electronic systems in the country is developing.
Previous studies have shown that patients with comorbidities, including diabetes, hypertension, cardiovascular disease, and kidney disease, were associated with an increased risk of adverse COVID-19 outcomes [29, 30].
We report on the association of multimorbidity in patients admitted for COVID-19, where almost half of the patients experienced severe COVID-19 outcomes and mortality. The patients were 2.3 times more likely to experience adverse outcomes than patients with one or no chronic conditions. Multimorbidity was reported as a simple count and not graded for clinical severity due to how information was recorded in the patients' files at the healthcare facilities during data collection. PLHIV with low CD4 T cell count or immunological weakness, HIV-related immunosuppression may mitigate the hyperinflammatory response that is associated with severe COVID-19, potentially protecting against a cytokine storm [31].
The susceptibility for adverse COVID-19 outcomes may increase due to the combined effect of immunosuppression and significant comorbidity, particularly when HIV was untreated or chronic immunological activation [32, 33]. However, comorbidities, immunological dysfunction, and delayed treatment continued to be significant concerns for PLHIV during the epidemic [33]
Studies suggested that PLHIV hospitalized with COVID-19 were not at an increased risk of adverse outcomes [31, 34, 35]. However, PLHIV with detectable viral loads showed less severe respiratory disease than those who were virologically suppressed, and their inflammatory responses were comparable to those without HIV. The number of PLHIV in this study was lower than in other studies. The status of their chronic condition was not known, and only a few had multimorbidity. Most of these patients recovered, and their outcomes were comparable to those without HIV.
Compared to national surveillance statistics and estimates from other studies conducted in more severely affected regions, the mortality rate was lower in our region [36]. A variety of factors could have contributed to this trend, such as differences in healthcare facility capacities, proactive quarantine measures, and earlier diagnoses. In studies conducted in similar settings in South Africa, higher mortality rates were reported linked to delays at presentation and restrictive access to medical treatment due to the high volume of patients in need of medical care during the period of the pandemic [21, 35].
Patients, particularly those with multimorbidity, were at a great risk of severe COVID-19 outcomes and mortality with every increase in age, as a result of their predisposition to organ failure, compromised immunological responses, and reduced susceptibility to viral infections [37]. This combination of factors is associated with less favourable recovery outcomes and likely necessitates longer hospital stays and more intensive treatment. While the age was a considerable indicator for adverse effects in univariable analysis, the lack of significance in multivariable regression suggests that its impact was influenced by other factors, including the severity of comorbidities, requirements for treatment, and other factors.
A young age served as a protective factor against COVID-19 complications; this beneficial effect might also be mitigated by the high prevalence of uncontrolled HIV infection and non-communicable diseases in certain geographic regions [38].
In a review on the impact of comorbidities on COVID-19 patients, PLWHIV hospitalized due to COVID-19 were noted to be younger and had a higher hospital mortality than patients without HIV [39]. Patients without comorbidities were also reported to recover with minimal intervention, while patients with multimorbidity and comorbidities often required escalation to higher care and extended treatment durations. This was also possible due to the added risk of organ support complications and acquiring secondary infections due to prolonged ventilator support.
We also report that treatment with anticoagulants and antibiotics was associated with adverse COVID-19 outcomes after adjusting for confounders, including age and chronic conditions. However, this finding should be treated with caution, as factors in policy frameworks during the early pandemic and the severity of each patient’s chronic condition may affect outcomes.
In this study, a higher mean hospital stay was noted in patients who recovered than in those who died. This was due to the recommended isolation period of 14 days for individuals with a positive COVID-19 test to limit the spread, rather than an indication for treatment of a severe medical condition. Most countries recommended that patients with COVID-19 symptoms who were not able to self-isolate at home, to go to designated healthcare facilities regardless of the severity of their symptoms during the first waves of the pandemic [22]. Our multivariable model's higher AUC (0.92) shows its predictive power in early high-risk patient identification. In the adjusted model, age, comorbidities, and steroid usage lacked statistical significance, suggesting multicollinearity or shared predictive weight.
5. STRENGTHS AND LIMITATIONS OF THE STUDY
The study was conducted at public health facilities in the Bojanala District, reflecting the clinical conditions of resource-limited settings where more than 80% of South Africans seek medical care. Using the census sampling method, all 289 confirmed COVID-19 patients hospitalized during the first pandemic period were included. This improved internal validity ensured that the results accurately represented real-world clinical practice. To address prevalent limitations of retrospective studies, standardized data collecting methods, cross-referencing records within health facilities, and trained research assistants were used to improve reliability and consistency. Several comorbid conditions presented occasionally, constraining the capacity to analyze them individually or investigate condition-specific risks. Consequently, the comorbidity load was evaluated primarily as a count of chronic diseases, potentially underrepresenting the significance of high-risk severe comorbidities. The study used applicable non-parametric tests and multivariable logistic regression, in conjunction with diagnostic evaluations, to determine the relationships between clinical variables and outcomes. The resulting model demonstrated a high discriminative ability, achieving an area under the ROC curve of 0.92, thus affirming the strength of its prediction accuracy.
However, several limitations need to be recognized. The study's exclusion of private sector facilities limits the generalizability of its results to the wider South African population or alternative healthcare systems. The use of non-random sampling, although inclusive, may increase the probability of selection bias. The limited sample size constrains the detection of lower effect sizes and results in broader confidence ranges in adjusted models. Multicollinearity among clinical factors may have reduced individual impact estimates in the multivariable study. The national policy in early 2020 mandating facility isolation for patients unable to quarantine at home may have extended hospital stays for non-clinical reasons, especially in field hospitals, complicating the interpretation of length of stay as a measure of illness severity.
Despite measures used to verify records, the research did not systematically quantify missing data. A comprehensive case analysis method was used, including only patients with complete data for each model in the studies. This strategy guaranteed consistency but might have added bias if the missing data were associated with clinical severity or other unmeasured variables. Evolving clinical guidelines and limited healthcare resources in the early months of the epidemic may have influenced treatment choices and results, hence restricting comparison with subsequent stages of the pandemic or varying health system settings.
CONCLUSION
This study showed significant associations between comorbidity burden, age, and clinical outcomes in COVID-19 patients hospitalized in public facilities. Hypertension, diabetes mellitus, and HIV were the prevalent comorbidities. Patients with multiple comorbidities had an over 50% death rate, reflecting the cumulative effect of chronic illness clustering. Older age was a significant predictor, as it correlated with higher mortality; however, its predictive value decreased in multivariate models, showing confounding by treatment intensity or comorbidity burden. Patients receiving treatment, particularly antibiotics and anticoagulants, had an increased mortality risk, independent of adjustments for other clinical and demographic variables. This suggests that these treatments may have acted more as markers for illness severity than as direct factors contributing to adverse outcomes. During the early waves of the pandemic, all COVID-19-positive individuals unable to self-isolate at home were hospitalized for a 14-day isolation period, regardless of treatment need. This approach may have led to the extended duration of hospitalization in some patients who need no active treatment, as well as to the perceived gap between hospitalization and clinical severity in low-risk populations. Patients with one or no comorbidities often achieve recovery with minimal intervention, while the occurrence of multiple chronic diseases correlated with prolonged hospitalization and increased treatment need, indicating more severe disease trajectories and reduced physiological reserve. Emerging evidence suggested positive as well as negative impacts of HIV-related immunosuppression on COVID-19 outcomes. While studies show that people using ART may evade the severe inflammatory consequences of COVID-19, poorly managed HIV with immunological impairment continues to be a substantial risk factor. This intricate interaction needs more investigation in multiple settings. Although the mortality rates in this group are modest compared to national averages, the results highlighted age, multimorbidity, and treatment intensity as fundamental predictors of adverse outcomes. Individualized risk classification and proactive clinical care are essential, especially in resource-constrained environments.
This study emphasized the importance of early identification and stratification of high-risk COVID-19 patients, especially those with multiple comorbidities such as hypertension, diabetes, and HIV, in resource-constrained settings, where advanced care is limited. Clinical decisions should rely on accessible indicators such as age, comorbidity burden, and treatment needs. Clinical protocols should incorporate comorbidity screening and severity at admission, ensure access to essential treatments, and always keep chronic disease management to reduce preventable mortality.
DECLARATION
The viewpoints and findings presented in this study are solely those of the authors and do not necessarily represent the views or policies of the Public Health Facilities, Bojanala District Health Department, any affiliated institutions, or the publisher. The views and concepts articulated are solely for research purposes and should not replace professional medical advice, diagnosis, or treatment. The views and information articulated in this study are based only on the research goals of this investigation.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: K.S.M.: Contributed to the conception and design of the study and provided the manuscript draft; C.D.K. and J.T.: Supervised the work and provided technical guidance; K.S.M.: Collected the data; J.L.M.Y. and B.M. K.S.M., C.D.K., J.T.: The manuscript was evaluated and edited; and S.A.K.: captured, cleaned, analyzed, and interpreted the data. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AUC | = Area Under Curve |
| COVID-19 | = Coronavirus Disease |
| HIV | = Human Immunodeficiency Virus |
| ROC | = Receiver Operating Characteristic |
| SARS-CoV-2 | = Severe Acute Respiratory Syndrome Coronavirus-2 |
| SMUREC | = Sefako Makgatho University Research Ethics Committee |
| TB | = Tuberculosis |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research study obtained ethical clearance from Sefako Makgatho University, Pretoria, South Africa. Ethical approval from the Research Ethics Committee (SMUREC) under reference number SMUREC/M/283/2020: PG. Authorization to examine patient records was obtained by the Bojanala district research committee. To maintain anonymity, patient identities were anonymized by the assignment of number codes to the data-gathering instrument.
HUMAN AND ANIMAL RIGHTS
All procedures undertaken during this investigation with people as subjects were in line with the ethical standards of the school and/or research committee, as well as the 2013 revision of the Declaration of Helsinki from 1975.
AVAILABILITY OF DATA AND MATERIALS
The corresponding author can provide the data that substantiates the findings of this study upon request.
ACKNOWLEDGEMENTS
The researchers extend their heartfelt gratitude to the Bojanala District Health Department and the managers of the participating facilities for their gracious cooperation and support in facilitating data collection.

