All published articles of this journal are available on ScienceDirect.

Fibular Hemimelia in a Young Boy with Delayed Diagnosis and Challenging Parental Decision: A Case Report and Review
Authors Info & Affiliations
Abstract
Background
Fibular hemimelia (FH) is a rare congenital limb deficiency defined by partial or complete absence of the fibulae bone, often associated with other limb deformities. Here, we present the case of a 2-year-old male who presented late with right femoral head (Rt FH) and proximal femoral deficiency, and whose family faced the challenging decision to decline therapy.
Case Presentation
A two-year-old baby boy was presented with delayed ambulation and a history of Rt lower limb deformity discovered since birth, yet no medical advice was sought due to parental reluctance. Examination revealed typical developmental milestones. The affected limb was 3 cm shorter than the contralateral limb, with evidence of muscle wasting, and there were no associated knee joint or toe deformities. A plain X-ray confirmed the absence of Rt fibula and shortened bowed tibia alongside proximal femoral focal deficiency (PFFD), and a CT scan classified it as type II FH with PFFD. After discussing the available therapeutic options, the parents declined any intervention and acknowledged their responsibility in the decision.
Conclusion
Early diagnosis and timely intervention are key factors for enhancing mobility. The late presentation of the case, coupled with the additional ethical challenge posed by the parents’ decision to forgo treatment, highlights the importance of real-time ethical considerations in managing congenital malformations.
1. INTRODUCTION
Fibular hemimelia (FH) is a rare congenital limb anomaly defined by the partial or complete absence of the fibulae. The disease exhibits diverse severity, ranging from mild FH, where the fibulae are hypoplastic, to severe FH, where the fibulae are completely absent. Its incidence ranges from 5.5 to 20 cases/1 million live births. FH tends to affect the right side more often, which is unilateral in ¾ of the cases [1].
The condition has a 2:1 predilection for males and is usually present at birth, with limb length discrepancy and joint deformity, and may be associated with toe abnormalities. However, the case may be accidentally discovered antenatally during an obstetrical ultrasound examination (US) of the fetus [2, 3]. Although the exact cause of fibular hemimelia is not yet defined, several etiological factors have been proposed to help understand why it occurs and how to prevent it among high-risk women. Although most cases are sporadically presented, some suggest a genetic predisposition in the affected limb. Teratogen exposure during antenatal development [4], maternal hyperpyrexia, and environmental toxins early in pregnancy (including smoking) have been linked to FH [5-7].
Abnormality in the vascular supply of the limbs can disrupt limb budding and development [8]. Amniotic bands syndrome during intrauterine life may cause direct compression of the limb, interrupting its growth [9, 10]. There are several classifications of FH based on severity and anatomical involvement to help guide therapeutic strategies, particularly in distinguishing cases eligible for limb lengthening from those requiring prosthetic management (Fig. 1).
First, there was the Achterman and Kalamchi classification (1979), which subclassified cases based on the partial or complete absence of the fibula [10]. Second, Stanitski and Stanitski 2003 relied on the shortened bone to determine whether ankle joints were involved. Finally, Paley's classification in 2016 focused on associated femoral, tibial, and foot deformities [11, 12]. Here, we present a case of a 2-year-old baby boy who presented with FH, proximal femoral focal deficiency, discussing presentation, diagnostic test, and management challenges that stem from parental refusal to treatment.
2. CASE PRESENTATION
A 2-year-old male child was brought to the outpatient department of Children Central Hospital, Baghdad, Iraq, with a chief complaint of delayed walking and shortened Rt leg. The parents noticed that their child was significantly behind his peers in achieving independent ambulation while other developmental milestones were within normal limits. As the child aged, there was progressive limb length discrepancy, with the right leg appearing shorter than the left, alongside muscle wasting in the affected limb; no pain, swelling, or gait instability was reported.
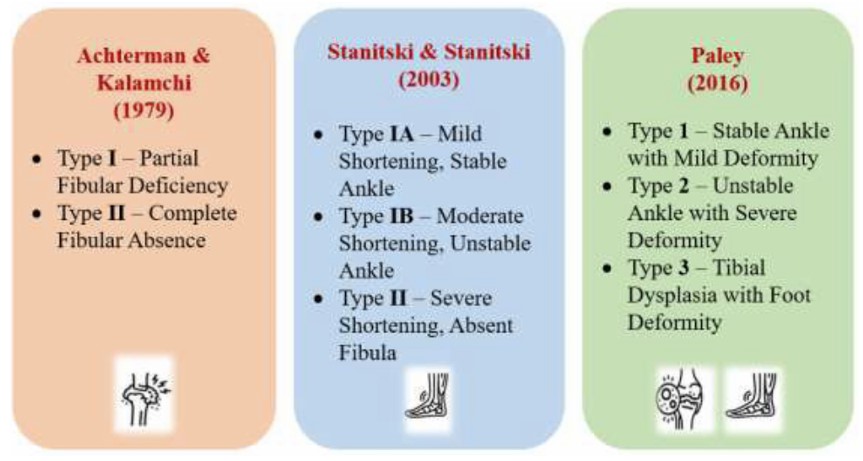
Different classification systems for FH.
The child was the third of five children in the family. The pregnancy was naturally conceived and went uneventfully; the mother reported no exposure to teratogenic agents, infections, or substance abuse, including smoking. The child was delivered vaginally at term with no reported complications.
The family lived in a rural area and had no history of similar cases in the family with unremarkable past medical, surgical histories, and hereditary diseases. The parents did not seek medical advice until the child reached the age of two and remained unable to walk independently.
The examination of the child appeared active and alert with age-appropriate growth parameters. The Rt leg appeared shorter by 3 cm from the left, with mild muscle wasting without tenderness; there were no signs of ankle joint deformity or restricted mobility, nor restricted joint motion, and no foot abnormality. Neurological examination and tendon reflexes were normal too.
The differential diagnosis included congenital conditions, such as fibular or tibial hemimelia, amniotic band syndrome, and proximal femoral focal deficiency. Other possible differential diagnoses were acquired conditions, including post-traumatic or post-infectious growth arrest, bone dysplasia, and neuromuscular disorders [1, 3, 6]. Given the progressive nature of limb length discrepancy, congenital causes seem to fit the case.
Imaging study, including X-rays (Figs. 2 and 3) and CT scans, confirmed the FH diagnosis and defined its severity. The case involved fibular hemimelia, characterized by fibular hypoplasia, a bowed tibia, and limb shortening, combined with proximal femoral focal deficiency (PFFD), in which the femur is shortened, angulated, or bowed, but demonstrates normal mineralization. PFFD tends to associate with FH in 50% of the cases [13, 14]. The ankle joint, foot, and tibia bone were unaffected. The diagnosis was consistent with type II FH with PFFD.
The parents were counselled regarding the variable treatment options, including the following:
- Surgical limb lengthening, including the Ilizarov method or precise deformity correction through staged procedures for improved functional mobility [15].
- Prosthetic fitting or amputation with prosthetic use was the other option for better mobility and quality of life for the case [16].
- Orthotic support: if both options were declined, a custom orthotic could assist with gait and alignment, including custom braces or a prosthetic device designed according to the child's needs [17].
The long-term implications of untreated FH were discussed with the family, including challenges imposed on functional mobility, gait abnormality, and psychosocial impacts. After discussing the available options, the parents declined surgical intervention, opting for non-intervention at this stage, and signed an informed refusal acknowledging the potential risks and consequences of their decision.
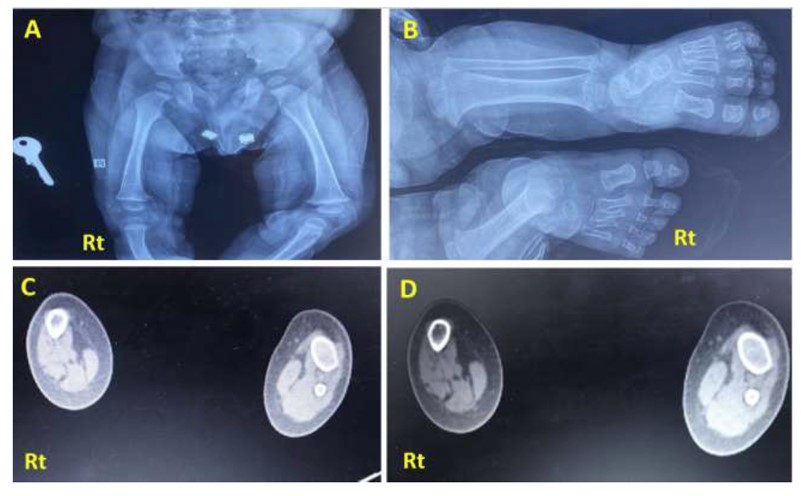
X-ray of the presented case. (A) Anteroposterior projection of both legs showing a completely absent Rt fibula with limb shortening and limb length discrepancy compared to the Lt side. The tibia is foreshortened, thickened, and bowed with medial rotation. (B) X-ray frontal view of Rt and Lt femur showing underdeveloped Rt femoral head compared to the Lt side, consistent with mild Rt proximal femur deficiency. (C, D): CT scan of both legs (axial section view) showing absent Rt fibula with deficiencies of the related muscular component, with the Rt tibia showing reduced radius compared to the Lt side.
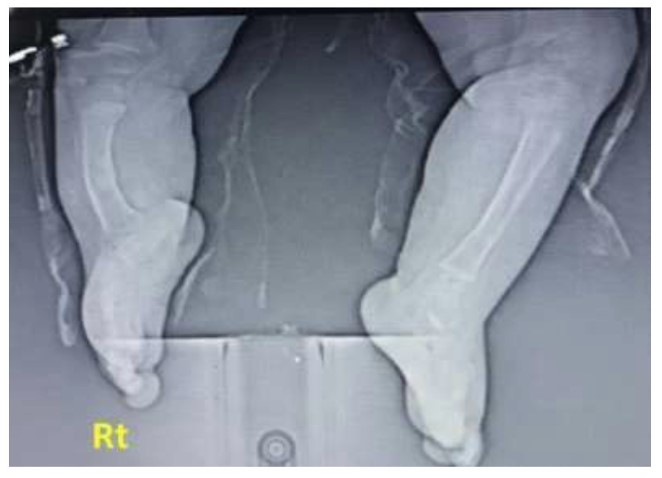
X-ray posteroanterior projection of both Rt and Lt legs; the Rt leg is shortened with thickened bowing of tibial bone, thickened cortex borders, and irregular bony marrow trabeculation compared with the normal Lt leg. Fibula is absent, associated with a hypoplastic, deformed attachment of the distal tibia to the ankle region, and later showing irregular hypoplastic carpal bony fusion.
| - | Age/sex | Presenting Symptom | Imaging Studies | Reference |
|---|---|---|---|---|
| 1. | 6-year male | Short Rt-leg Rt equinovalgus deformity of the foot |
Absent fibulae Shortened bowed tibia Hypoplastic lateral femoral condyle Subtalar coalition and absent lateral ray |
Sisay et al. (2015) [18] |
| 2. | 6-year female | Lt short leg, unstable knee | Absent Lt fibulae Absent anterior cruciate ligament (ACL) |
Tate and Wojtys et al. (2019) [19] |
| 3. | Male | Mild length discrepancy, extensive tarsal deformity and oligodactyly | Absent fibulae Extensive hindfoot coalition of multiple bones |
Özdemir et al. (2019) [20] |
| 4. | 23-year-old female | Rt leg shortened; equinovalgus foot; malformed foot and toes | Rt fibulae absent Bowed shortened tibia Equinovalgus position of the foot Diffuse alteration in the trabecular pattern of tibial and foot bones. Astragalus-calcaneal dysmorphia and syndactyly |
Raposo et al. (2022) [21] |
| 5. | 4-year-old female | Rt hemimelia and shortened limb Deformed Rt ankle and valgus foot |
Limb shortening Lateral rays were absent A unique anomaly was diagnosed at the age of 3 years: a spina bifida |
Manasra et al. (2025) [4] |
3. DISCUSSION
FH is a rare congenital condition; despite its rarity, it is the most frequently reported type of long bone deformity. Table 1 lists some of the cases reported in the last decade.
Diagnosing FH is mainly clinical and confirmed by imaging studies. The clinical picture is provided as follows:
The affected limb can be shortened with a discrepancy in limb length.
- The affected limb can be shortened with a discrepancy in limb length.
- Associated foot deformities may occur, such as equinovalgus ankle joint position.
- Toe abnormalities include syndactyly, oligodactyly, or polydactyly [22].
Imaging studies, on the other hand, such as plain radiographic tests, are essential to confirm the state of the fibular bone, whether it is partially or completely absent, its degree of shortening, and to define if lateral ray anomalies are present.
A CT scan gives an accurate 3-dimensional reconstruction of the actual limb length discrepancy and defines associated joint defects as club foot [23]. An MRI scan assesses associated muscle agenesis, wasting, pseudoarthrosis, and if there is a proximal femoral deficiency [1].
The management strategy is challenging and depends on the case severity and associated deformities [24]. The surgical option includes either limb lengthening surgery, the Ilizarov technique (reserved for mild-moderate cases), or amputation and prosthetic fit, offered for severe cases with significant functional impairment [25]. Associated ankle joint deformities are also managed surgically and are needed to improve the weight-bearing function [24, 25].
The prosthetic has evolved significantly during the last few years, improving patients' quality of life by improving mobility and gait efficiency. It is recommended that these cases be followed up to evaluate bone, joints, and overall functional outcomes [26].
There are other reports of FH among the Iraqi population; a case series, including 8 cases, was reported in Erbil, discussing the use of surgery, i.e., the Ilizarov technique, in managing FH cases.
Another case was reported in Fallujah General Hospital, where a newborn was suffering from fibular hemimelia associated with tracheoesophageal fistula [27, 28].
Many points seen in this case deserve to be highlighted. This case is unique because it involved fibular hemimelia (FH) with proximal femoral focal deficiency, while sparing the ankle joints, foot, and toes, accounting for a rare combination [13], which further highlights the clinical diversity of FH [29]. An Egyptian case report discussed fibular aplasia, tibial cacomelia, and oloigososyndactyly syndrome [30].
There are innovative management options for this disorder, including the use of autologous osteoblast cell therapy, which represents one of the innovative treatments for FH by offering shorter therapy duration and improved patient outcomes compared to traditional therapeutic strategies [31, 32]. The use of patient-specific 3D-printed knee joint models offers precise pre-operative planning for a tailored graft placement; this optimizes surgical accuracy and outcome [33]. Advanced biologic grafts integrating tissue-engineered scaffolds and bio-enhanced grafts allow better healing and reduced failure rates [34, 35].
Finally, applying AI (artificial intelligence) in ACL reconstruction is an innovative approach to guiding surgical decision-making. The AI algorithm helps optimize graft selection and refine rehabilitation protocols [36, 37].
It is worth mentioning that all cases need multidisciplinary rehabilitation to optimize limb mobility and function. Ideally, these cases should be managed by a multidisciplinary approach, including a pediatric orthopedic, a physiotherapist, who will design a tailored rehabilitation program to enhance limb function, and a psychosocial therapist for the child and the family [38]. The child is likely to face issues concerning the social implications of the condition that can affect his/her self-esteem. As for the family, they need to cope with the challenges faced as the child grows older [39, 40].
The FH prognosis relies on how early the presentation was, the case severity, and the success of the surgery. Some of the cases managed by surgery require multistage operations and sometimes revisions [1, 25]. It is unusual for such cases to present late; however, in this instance, the delay resulted from the parents’ refusal to pursue corrective interventions. The ethical aspects of patient care have been emphasized in this case, providing a deeper insight into the challenges faced by physicians in the real world, where a critical balance needs to be maintained between treatment options and parental autonomy.
Delayed treatment of fibular hemimelia is likely to cause multiple musculoskeletal and rheumatic complications [33], not to mention the psychosocial complications. Thus, timely intervention is vital to prevent long-term disability and inflammatory complications [25].
CONCLUSION
Fibular hemimelia is a rare complex anomaly that requires a multidisciplinary approach. Earlier diagnosis and personalized management are key factors to improve FH outcomes as they enable timely intervention. At the same time, a multidisciplinary approach enhances mobility and reduces psychosocial impact. Advancements in surgical techniques and prostheses continue to improve the function of limbs, gait stability, and patients' quality of life. Further research is warranted to refine treatment selection, which can improve the patient’s quality of life and assess the long-term outcome for this rare limb anomaly.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: M.A.G.Z.: Data collection; S.A.: Methodology; S.K.A.: Visualization; W.N.M.H.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| FH | = Fibular hemimelia |
| PFFD | = Proximal femoral focal deficiency |
| ACL | = Anterior cruciate ligament |
| AI | = Artificial intelligence |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Mustansiriyah University ethics committee issued approval for publication with IRB 73 (dated 21/3/2024).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The patient's parents signed informed consent for the publication of this case and the related data.
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting material are available within the article.
ACKNOWLEDGEMENTS
The authors thank Mustansiriyah University for continuous support.

