All published articles of this journal are available on ScienceDirect.

Cesarean Section Rates, Indications, and Immediate Outcomes at a National Referral Hospital in Botswana: A Retrospective Study
Authors Info & Affiliations
Abstract
Introduction
Cesarean Section (CS) is essential for saving the lives of women and their newborns from pregnancy and childbirth-related complications, but inappropriate use of CS may have potential adverse effects on maternal and neonatal health outcomes. However, there is a paucity of evidence regarding the rate, indications, and immediate outcomes of CS in Botswana. This study aimed to determine the rate, main indications, and immediate outcomes of CS deliveries conducted in Botswana.
Method
A facility-based, retrospective, cross-sectional study design was employed, including a review of total deliveries attended over 12 months at Princess Marina Hospital (PMH), a National Referral Hospital in Botswana. The rate of CS was determined from the total number of deliveries attended in 12 months. Furthermore, 794 CS deliveries were randomly selected from a registry of total CS deliveries to characterize the indications and immediate outcomes. Data extraction was conducted via structured, pretested instruments. Descriptive statistics were used and are presented in tables, charts, and figures.
Results
The rate of CS delivery among total deliveries attended for 12 months was 28.5% (1918/6737). The main indications for CS were fetal distress (23.6%, 187), one previous CS (13.7%, 109), malpresentation (11.4%, 90), two previous CSs (10.8%, 86), and Cephalopelvic Disproportion (CPD) (6.7%, 53). Adverse maternal outcomes accounted for 19 (2.4%) of the reported maternal complications; almost all (18, 95%) of these complications were related to Peripartum Hemorrhage (PPH). A total of 156, 19.6% of CS deliveries, with perinatal adverse outcomes, 3.8% stillborn, and 15.9% presented with complications, which accounted for 93,74.0% of CS deliveries due to a low APGAR score and birth asphyxia (14, 11.0%).
Discussion
The high cesarean section rate (28.5%) suggests possible overuse or a high-risk population, highlighting the need to promote safe vaginal deliveries. Common CS indications—like fetal distress and previous CS—point to challenges in labor management and the importance of considering vaginal birth after cesarean (VBAC). Maternal complications (2.4%), mainly due to hemorrhage, call for better emergency preparedness. Perinatal adverse outcomes (19.6%), including stillbirths and birth asphyxia, suggest delays in care and gaps in neonatal resuscitation. Overall, the findings emphasize improving labor monitoring, emergency response, and evidence-based CS use.
Conclusion
The CS rate identified in this study was higher than the World Health Organization (WHO) standard recommendation. The main indications for CS were fetal distress and one previous CS. Comprehensively addressing the CS issue needs attention in Botswana to improve maternal and perinatal outcomes. The Ministry of Health in Botswana and healthcare providers need to emphasize strengthening antenatal care services, ensuring that more women have access to skilled healthcare professionals during childbirth, providing appropriate interventions, and reducing the need for emergency and unnecessary CSs. The development of national guidelines on appropriate indications for CS delivery, training healthcare workers, and creating community awareness are recommended.
1. INTRODUCTION
Cesarean Section (CS) is a major life-saving obstetric operative intervention for mothers and babies that is performed globally [1-3]. Even though appropriate and effective use of CS can improve the outcomes of mothers and newborns, inappropriate and ineffective use of CS can lead to maternal and/or neonatal adverse outcomes [4, 5]. However, there are enormous disparities in access to safe and timely cesarean birth [6], and there is growing international concern over the health consequences of unnecessary or unsafely conducted operations [7]. The unsafe provision of CS and the concomitant overuse of surgical procedure drain resources increase avoidable morbidity and mortality [7, 8].
Studies have reported that common indications for CS, including fetal distress, obstructed labor, prolonged labor, previous CS, malpresentation, Antepartum Hemorrhage (APH), severe preeclampsia, failed induction of labor, fetal asphyxia, and fetal acidosis, are increasing across regions [8-11]. These indications have different rates across regions and countries [8-11]. The increase in CS rates has led to increased confrontation of myomas by obstetricians, shifting myomectomy from a contraindication to an indication for CS in recent years [12, 13]. Furthermore, CS delivery performance is also influenced by other socio demographic factors, such as wealth, social class, level of education, and maternal preference, particularly in developed countries [4, 8, 14, 15].
Cesarean section is a life-saving intervention when medically indicated, aids in the avoidance of birth trauma for the neonate, and preserves the mother’s perineum. However, this procedure can also lead to short-term and long-term health effects for women and children [16, 17]. On the other hand, compared with normal vaginal delivery, CS can cause significant complications for mothers, such as infection, disability, or death, and is costly [18, 19]. Compared with babies born via vaginal delivery, babies born via CS experience distinct hormonal, physical, bacterial, and medical exposures that impact their immunological development [16, 19, 20]. Understanding the rates, indications, short-term maternal and perinatal outcomes, patterns, and sociodemographic determinants of CS deliveries is crucial for improving maternal healthcare services and reducing unnecessary surgical interventions [21]. Additionally, it is crucial for governments to develop evidence-based guidelines and policies to evaluate progress in maternal and infant health and to monitor emergency obstetric care and resource use [22]. There is a lack of local data on the indications and immediate maternal and perinatal outcomes of Cesarean Section (CS), creating an evidence gap that limits policy formulation and clinical decision-making in Botswana. Particularly, there is a paucity of evidence regarding the rate, major indications, and immediate outcomes of CS delivery. Therefore, this study aimed to determine the rate, indications, and immediate outcomes of CS at a National Referral Hospital in Botswana [23]. The findings of this study could be leveraged to improve national maternal healthcare policies, develop training manuals, and provide practical guidance for local obstetric practices, ensuring that guidelines for maternal and child birth interventions are based on current scientific evidence and optimized for the local context.
2. METHODS
2.1. Study Setting and Design
A facility-based, retrospective, cross-sectional study design was used, including a review of 794 CS deliveries conducted over more than 12 months at Princess Marina Hospital (PMH) in Botswana. PMH is one of three tertiary and national referral hospitals in Gaborone, Southeast District, Botswana [23]. The hospital has 581 beds and serves a population of 231592 [24, 25]. The hospital provides comprehensive emergency obstetric care services, including CS interventions [23].
2.2. Study Participants
Princess Marina Hospital (PMH) was randomly selected from three National Referral Hospitals in Botswana. A total of 6737 deliveries were performed over 12 months at PMH. Among the total delivery registry, 1918 included all CS deliveries, including selective and emergency CS. A single population proportion was used for sample size calculation; n = Z2 * P (1−P) / d2, with proportion 50%, α= 0.05, 95% CI, and d=0.05, and a design effect of 2 was used to ensure national repre sentation, since Pakistan Institute of Medical Sciences Hospital (PMH) is a national referral hospital to which many pregnant women from different regions present. Additionally, an allowance of 3.5% for missing data was used to increase the sample size. The final sample of 794 randomly selected CS deliveries from the database was included to characterize indications and maternal and perinatal outcomes among the total CSs.
2.2.1. Inclusion Criteria
All women who delivered via cesarean section at Princess Marina Hospital during the 12-month study period, January to December 2024. CS delivery records that are complete and legible, with sufficient documentation of indications and immediate maternal and neonatal outcomes.
2.3. Operational Definition
2.3.1. Maternal Immediate Outcomes
Maternal outcomes of CS delivery are categorized as mothers who delivered alive or dead, or who developed complications. In the present study, immediate maternal adverse outcomes were categorized as those that developed complications (developed PPH or/or rupture of the uterus) as immediate maternal adverse outcomes since no maternal death was reported as an immediate outcome in the delivery registry. Postpartum Hemorrhage (PPH) and uterine rupture are commonly used as key maternal outcome indicators during Cesarean Section (CS) delivery because they represent major, life-threatening compli cations that strongly influence maternal morbidity and mortality.
2.4. Data Collection and Analysis
A structured, pretested data-collection tool was used to extract data from maternity registers [23]. The data collected included the mothers’ sociodemographic characteristics, such as maternal age and residence; antenatal care data, such as gravidity, parity, and gestational age; and maternal and fetal risk indications for CS deliveries, such as CPD, previous CS, fetal distress, and malpresentation. Immediate maternal and fetal out comes such as maternal death, stillbirth, maternal and fetal complications, and morbidities were also included in the data collection [23]. Data completeness and consis tency were assessed and cleaned prior to analysis. EpiData version 3.1 was used for double data entry verification, and analysis was conducted using SPSS version 25. A comprehensive data validation process was implemented to ensure dataset reliability, including checks for data integrity and logical consistency across variables. Discrepancies were resolved through data cleaning and cross-verification with source records. A pre-test was conducted to evaluate the effectiveness of the data collection instruments, leading to the identification and correction of errors, inconsistencies, and outliers.
As a retrospective study, data were extracted from maternity registers at selected health facilities. The extraction process involved reviewing records of cesarean section deliveries and entering relevant information into a pre-tested data collection tool. To minimize information bias, the tool was aligned with routinely documented variables, and cross-verification with source records was conducted during data cleaning.
The analysis focused on determining the rate of CS among total deliveries and characterizing the main indications and immediate outcomes of CS deliveries. Baseline characteristics, such as indications of CS deliveries, for example, labor-related complications, CPD, fetal distress, and malpresentation, were described via counts, frequency, proportions, means, and percentages.
2.5. Ethical Consideration
Ethical approval to conduct the study was obtained from the University of the Witwatersrand Ethics Committee. The Health Research and Development Division, Ministry of Health and Wellness, and the PMH Research and Ethics Committee, Gaborone, Botswana, granted permission to conduct the study. Confidentiality was maintained by excluding patients’ identifiers from the data extraction tool.
3. RESULTS
3.1. Sociodemographic Characteristics
For a total of 794 CS deliveries, the mean maternal age was 28.76 years, with a range of 15–45 years. More than half (50.6%) of the participants were aged 25-34 years, followed by more than a quarter (28.5%) aged 15-24 years, and one-fifth (20.9%) aged 35+ years. More than half (59.3%) of the participants were urban residents.
3.2. Prevalence of CS
The CS delivery rate among women who attended deliveries for 12 months was 28.5% (1918/6737) among total deliveries attended during that period.
3.3. Obstetric characteristics of CS deliveries
More than two-thirds (67.1%) (95% CI: 63.2 - 69.9) of the women were multigravidas, approximately two-thirds (65.1%) (95% CI: 61.3- 68.2) were multiparas, and one-fifth were less than 37 weeks of gestation (Table 1).
| Characteristic | n/N (%) | 95%: CI |
|---|---|---|
| GRAVIDITY | ||
| Primigravida (1) | 261 (32.9%) | 30.1 – 36.8 |
| Multigravida (>1) | 533 (67.1%) | 63.2 - 69.9 |
| PARITY | ||
| Primipara (1) | 277 (34.9%) | 31.8 – 38.7 |
| Multipara (>1) | 517 (65.1%) | 61.3- 68.2 |
| GESTATION (WEEKS) | ||
| <37 | 169 (21.3%) | 17.3 – 22.9 |
| ≥37 | 625 (78.7%) | 77.1 – 82.7 |
3.4. Indications for Caesarian Sections
The most frequent indication for CS was fetal distress (23.6%, 187), followed by one previous CS (13.7%, 109), malpresentation (11.4%, 90), two previous CSs (10.8%, 86), and a CPD (6.7%, 53) (Fig. 1).
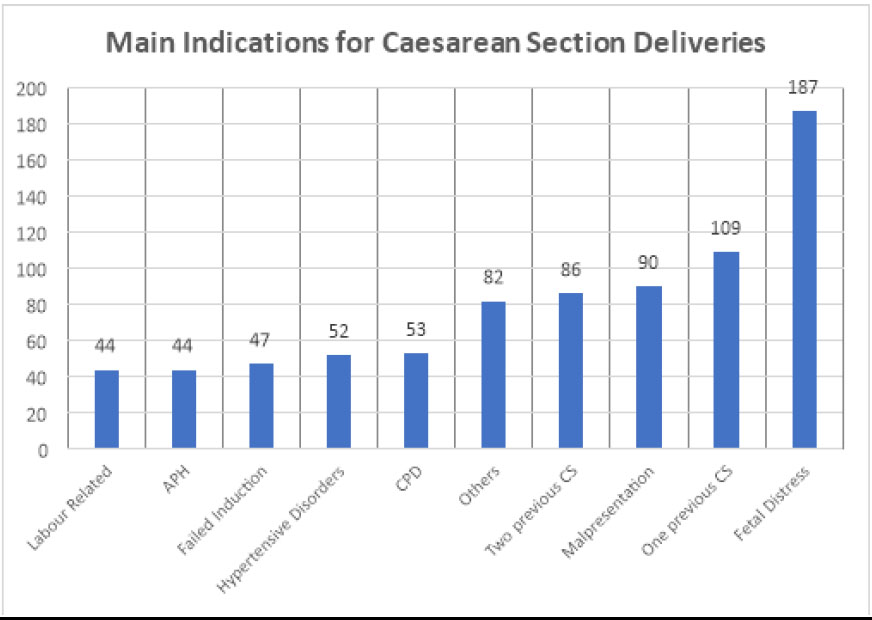
Indications for CS deliveries at Princess Marina Hospital (PMH), Gaborone, Botswana (n=794).
3.5. Maternal age Distribution and Caesarean Section Indications
One previous CS (62%) was the most frequent CS indication for the 25–34-year-old age group, followed by labor-related CS (61%) and malpresentation (59%). More than two-thirds of cases of fetal distress were reported among those aged 15–24 years (Table 2).
| Indications of CS | Age Category | N(%) | ||
|---|---|---|---|---|
| 15-24 Years | 25-34 Years | 35 + Years | ||
| Fetal distress | 68(36%) | 89(48%) | 30(16%) | 187(23.5%) |
| One previous CS | 18(17%) | 68(62%) | 23(21) | 109(13.7%) |
| Two previous CS | 10(12%) | 50(58%) | 26(30%) | 86(10.8%) |
| Malpresentations | 28(40%) | 41(59%) | 21(30%) | 70(8.8%) |
| CPD | 22(42%) | 26(49%) | 5(10%) | 53(6.7%) |
| Hypertensive disorder | 10 (24%) | 22(52%) | 20(48%) | 42(5.3%) |
| Failed inductions | 13(28%) | 26(55%) | 8(17%) | 47(5.9%) |
| Labor related | 15(34%) | 27(61%) | 2(5%) | 44(5.5%) |
| APH | 14(32%) | 19(43%) | 11(25%) | 44(5.5%) |
| Others indications | 28(34%) | 34(41%) | 20(25%) | 82(10.3%) |
3.6. Obstetric History and Indications for CS
With respect to women's obstetric history and CS, women with primigravida experienced more than two-thirds (37.6%) fetal distress as the most frequent indication for CS deliveries, followed by CPD (12.6%). Women with multigravidas with one previous CS accounted for 20.5%, followed by malpresentation (16.7%). With respect to parity, CPD (37.2%) was the most dominant indication of CS delivery for primiparas. In contrast, malpresentation accounts for 21.1% of CS indications for multiparas. With respect to gestation times of less than 37 weeks, the main indications for CS were hypertensive disorders (16%) and fetal distress (16.0%). A quarter (25.6%) of women with a gestation of 37 weeks and above reported fetal distress (Table 3).
| Gravidity | CPD | Labor Related | Failed IOL | APH | One Previous CS | Two Previous CS | HPT | Fetal Distress | Malpresentation | Others |
|---|---|---|---|---|---|---|---|---|---|---|
| Primigravida (1) | 33(12.6%) | 22(8.4%) | 22(8.4%) | 15(5.8%) | 0(0%) | 0(0%) | 15(5.6%) | 98(37.6%) | 28(10.3%) | 28(10.3%) |
| Multigravida (>1) | 20(3.8%) | 22 (4.1%) | 25(4.7%) | 29(5.4%) | 109(20.5% | 86(16.1%) | 37(6.9%) | 62(11.6%) | 89(16.7%) | 54(10.1%) |
| Total | 53(6.7%) | 44(5.5%) | 4.7(5.9%) | 44(5.5%) | 109(13.7%) | 86(10.8%) | 52(6.6%) | 160(20.2%) | 117(14.7%) | 82(10.3%) |
| Parity | - | - | - | - | - | - | - | - | - | - |
|
Primipara (1) |
03(37.2%) | 23(8.5%) | 4(8.7%) | 16(5.8%) | 0(0%) | 0(0%) | 6(5.8%) | 4(12.3%) | 30(10.8%) | 1(11.2%) |
|
Multipara (>1) |
19(4.0%) | 20(3.8%) | 4(4.6%) | 8(5.4%) | 6(16.6%) | 84(16.2%) | 36(7.0%) | 4(18.1%) | 9(21.1%) | 1(9.8%) |
| Total | 12(15.3%) | 43(5.5%) | 8(5.9%) | 4(5.5%) | 6(16.6%) | 84(16.2%) | 2(6.6%) | 163(20.5%) | 9(17.5%) | 2(10.3%) |
| <37 | 0(0%) | 2(1.2%) | 7(4.1%) | 4(14.2%) | 10(5.9%) | 6(9.5%) | 7(16.0%) | 7(16.0%) | 3(13.6%) | 33(19.5%) |
| ≥37 | 52 (8.3%) | 42(6.7%) | 1(6.6%) | 0(3.2%) | 9(15.8%) | 0(11.3%) | 25(4.0%) | 160(25.6%) | 7(10.7%) | 9(7.8%) |
| Total | 52(6.6%) | 44(5.5%) | 8(6.0%) | 4(5.5%) | 109(13.7%) | 6(10.8%) | 2(6.6%) | 187(23.6%) | 0(11.3%) | 2(10.4%) |
3.7. Maternal and Perinatal Outcomes related to CS
Maternal outcomes were classified as those mothers who were alive, died/or developed a complication. All mothers who delivered were alive. Nineteen mothers (2.4%) (95% CI: 1.4 -3.5) had a material adverse outcome (i.e., developed complications but no deaths were reported). Among mothers who developed complications (18,95%), these complications were related to Peripartum Hemorrhage (PPH), and one mother experienced uterine rupture.
Perinatal outcomes were classified as live birth, stillbirth, and/or developed complications (i.e., low APGAR score, birth asphyxia, neonatal death, and fractures).
With respect to perinatal outcomes, 764 (96.2%) (95% CI: 95-97.5) live births, thirty (3.8%) (95%:CI: 2.5 – 5.0) were stillborn, and 126 (15.9%) (95%:CI: 14.4 - 19.9) of the newborns experienced perinatal complications (i.e., low APGAR score, birth asphyxia, and neonatal death fractures).
A total of 156 (19.6%) CS deliveries with adverse perinatal outcomes were reported. Thirty (3.8%) (95%: CI: 2.5 - 5.0) newborn babies died. One hundred twenty-six (15.9%) (95%:CI: 13.7 – 19.2) newborn babies presented with complications, which accounted for 93,74.0% of all complications due to a low APGAR score, followed by birth asphyxia (14, 11.0%) and neonatal death (NND) (8, 6.0%), (11, 9%) of which were fractures, and the other compli cations were major perinatal complications (Table 4).
| - | n (%) | 95% CI | |
|---|---|---|---|
| Maternal outcome | Alive | 794 (100.0%) | - |
| Complication/morbidity | 19 (2.4%) | 1.4-3.5 | |
| Maternal adverse outcome | Yes | 19(2.4%) | 1.4 - 3.5 |
| No | 775(97.6%) | 96.5 - 98.6 | |
| Perinatal outcome | Alive | 764/794 (96.2%) | 95 - 97.5 |
| stillbirth | 30/794 (3.8%) | 2.5 - 5.0 | |
| Complication/morbidity | 126/794 (15.9%) | 13.7 - 19.2 | |
| Prenatal Adverse Outcome | Yes | 156 (19.6%) | 14.4 - 19.9 |
| No | 638 (80.4%) | 80.1- 85.6 | |
There were no significant differences in maternal or fetal outcomes between primiparas and multiparas (p=0.08). CS at a gestational age of <37 years was associated with a greater risk of adverse fetal outcomes than CS at a gestational age ≥37 years (p=0.001).
4. DISCUSSION
This study revealed that the rate of CS deliveries at PMHs was 28.5%, which is higher than that recommended by the WHO of 5–15% [10] and higher than that reported in a study covering 154 countries (2010–2018), covering 94% of the world’s live births (21.1%) and far higher than the average of 5% CS in Subsaharan Africa [7]. A study conducted in Nigeria at a referral hospital reported a rate of 25.7%, with maternal death as the outcome [26]. The CS delivery rate is higher than that reported in a study conducted in Somalia, which found an overall cesarean section rate of 21.6% over 5 years [11]. Our findings are similar to those of a study conducted in a neighboring country, South Africa, which reported CS rates of 32% [27]. This high rate of CS may be multifactorial. First, this may be due to most complicated cases being referred to PMH, thereby increasing the CS rate. Other studies also reported that high rates of CS deliveries were more evident in health facilities that have increased the accessibility and availability of CS interventions [4, 10].
On the other hand, the high CS rate in this study may also be due to missed opportunities for primary CS reduction, such as labor support, employment partograph, minimal use of instrumental vaginal delivery, and the absence of clinical practice guidelines, combined with a mandatory second opinion for CS delivery at the PMH. Low rates of instrumental vaginal deliveries are associated with an increase in CS rates [28, 29]. Inadequate and insufficient instrumental vaginal delivery may be due to a lack of policies addressing this area, and it may also be due to a lack of clinician expertise and motivation. Therefore, it is essential to develop informed policies that can effectively address the use of instrumental vaginal deliveries. Moreover, it is critical to assess doctors' skills in instrumental vaginal delivery and enhance them accordingly. The use of instrumental vaginal delivery not only significantly reduces the rate of CS deliveries but also reduces health expenditures [30]. Evidence shows that using a partograph has been associated with improved quality of care, including ease of recording, provision of a pictorial overview of progress, auditing of care, training of clinicians, and transfer of care [31, 32]. The imple mentation of clinical practice guidelines and a mandatory second opinion for CS has reduced its use as a nonclinical intervention [33]. Continuous labor support by a midwife or nurse results in less active labor and tends to lead to a high rate of vaginal delivery and a low rate of emergency CS [34]. Since CS deliveries are rarely performed in most primary and district hospitals in Botswana due to inade quate theatre facilities and medical staff (obstetricians, surgeons, neonatologists, pediatricians, and anesthesio logists), the Ministry of Health and Wellness should improve the planning of CS services across different levels of care. This can be achieved by upgrading primary and district hospitals, improving theatre facilities, and recruiting sufficient healthcare workers who can perform CS. In addition, evidence-based information is vital for assisting policymakers in planning and developing policies and guidelines to cater to women who need CS delivery and to reduce unnecessary CS deliveries.
The study findings revealed that the most frequent indication for CS delivery was fetal distress (23.6%). These findings are similar to those of other studies [11, 30]. The findings of a study from South Africa reported that fetal distress was a 40.1% indication of CS [27]. Thus, further exploration of the diagnostic accuracy of fetal distress as an indication for CS in the study setting is needed. This could be because, at the PMH, there is a lack of continuous electronic fetal monitoring systems essential for accurate diagnosis of fetal distress. As a result, doctors and midwives rely on simple measures such as fetal tachycardia and bradycardia, as well as fresh and old meconium-stained liquor, to diagnose fetal distress. This practice could, however, lead to overdiagnosis of fetal distress [30]. Moreover, Cardiotocographs (CTGs) might lead to overdiagnosis of fetal distress [30]. The mis classification of fetal distress via an imprecise methodology leads to a poor predictor of fetal outcome; the result is a tendency for unnecessary CS. Ensuring the availability of newer technologies, such as ECG, improves the predictive value of fetal monitoring, reducing operative deliveries for fetal distress [35]. This implies the need to use new and appropriate technologies for the diagnosis of fetal distress, as well as appropriate training for doctors and midwives in their use and interpretation.
This study also revealed that in primigravid and primipara patients, CPD was a frequent indication for CS. According to the literature, CPD is one of the leading indications for CS delivery for both primigravida and primiparas since these populations tend to have their first pregnancies and children at an early age and when their bodies are not yet fully mature and well developed to withstand the strenuous effects of labor and delivery [36-38]. Consequently, they experience labor-related complications such as obstructed labor, poor labor progress, and prolonged labor [36-38]. Therefore, strengthening antenatal care services for both primi gravids and primiparas by assessing pelvic adequacy is critical for early diagnosis of CPD.
4.1. Immediate Outcomes of CS Deliveries
This study revealed that PPH was the most frequent maternal complication, similar to national audit findings [39] and consistent with other studies [10, 22]. The Botswana Family Health Survey [39] revealed that most women in Botswana attend ANC and deliver in hospitals; thus, PPH is unlikely to be related to patient-related factors. More likely, they are related to key factors within the health system, such as inadequate quality of care or delays in providing the required interventions. Even though the majority of women attend ANC and deliver at health facilities, it is possible that PPH may be related to the fact that these women present late at health facilities. The current study was not designed to investigate the causes of maternal and fetal complications. However, to decrease the incidence of PPH, strengthening the capacity and training of health care workers in the provision of midwifery services, expanding community health education, and promoting early booking to enable early identification and management of this complication are critical.
This study also revealed that multiparous women had a higher rate of maternal morbidity, similar to findings in other studies [39]. It has been suggested that in this group of women, uterine muscle tone is decreased, and after delivery, uterine contractions may be ineffective and retraction may be inadequate to achieve hemostasis [39]. As most women requiring CS in this study were multiparous, the findings suggest the important role of family planning in reducing morbidity in this group [39]. Furthermore, it is essential to strengthen community health education on the importance of family planning and early ANC booking.
With respect to perinatal complications, this study revealed that a low APGAR score was the most common (74.0%) perinatal complication, which usually led to birth asphyxia and eventually NND. Although this observation is consistent with other studies, the rate is much higher than the 52% rate of low APGAR scores reported in these studies [10]. The high rate of low APGAR scores in this study could be attributed to several factors, such as a high referral number of complicated cases from lower-level health facilities, ineffective management of labor, delayed decision making, or delayed transfer of women from home or the referral of health facilities to referral hospitals [10, 40]. This study was not designed to analyze these factors, but the high rate of low APGAR scores with poor prognosis at PMH likely suggests that the neonatal intensive care unit (NICU) at this hospital lacks essential resources and is staffed by health care workers with limited expertise in neonatology. This has been documented in another study, which revealed that a lack of appropriate facilities in the NICU, an absence of neonatologists and neonatology nurses, and a shortage of pediatricians were contributing factors to high rates of low APGAR scores [10, 40]. Inadequate ANC utilization is associated with CS delivery and adverse perinatal outcomes [41], contributing to perinatal mortality [42], and ANC visits are significantly associated with lower neonatal death rates [43].
Therefore, to reduce these complications, it is critical for PMHs to institute quality antenatal care services, upscale comprehensive emergency obstetric and newborn care at lower-level health facilities, intensify neonatal resuscitative measures, and adequately train health care workers in intensive neonatal care. Furthermore, the community should be educated about the importance of early ANC booking and seeking medical help early in emergencies.
4.2. Limitations of the Study
Although a large sample size was used in this study due to its retrospective design, it has limitations such as bias from data abstraction, incomplete data, missing information on confounders (e.g., BMI, HIV, gestational diabetes, history of medical condition), record quality, lack of detail in data, lack of active follow-up, and difficulty in establishing cause‒and‒effect relationships. A regression analysis to identify factors associated with CS delivery was not conducted.
CONCLUSION
The study revealed a high CS rate (28.5%) at Princess Marina Hospital in Botswana, which is higher than the WHO's recommended rate. The high rate of CS might increase health risks for mothers and babies. An appropriate strategy should be implemented to reduce the high rate of CS, such as decreasing the overdiagnosis of fetal distress through the use of cardiotocographs and training healthcare workers in instrumental vaginal deliveries. Enhancing antenatal education to inform mothers about the risks and benefits associated with different delivery options. The study also revealed that PPH and low APGAR scores were the most common adverse outcomes associated with CS delivery. To minimize these adverse outcomes, it is important to continuously train healthcare workers in emergency obstetric and newborn care, improve neonatal facilities at tertiary hospitals, expand access to life-saving drugs and supplies, and foster community education to raise awareness and encourage the initiation of antenatal care. Further prospective studies are needed to identify predictors of adverse outcomes of CS in the study setting, to provide robust evidence to inform policy and practical implications.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: O.C.K. and J.C.Y.N.: Contributed to conceptualization, methodology, software, supervision, project administration, and funding acquisition; O.C.K., J.C.Y.N., and A.S.B.: Performed validation, formal analysis, investigation support, writing—original draft preparation, writing—review and editing, and visualization; X.X.: Contributed to investigation, resources, and data curation. All authors have read and agreed to the published version of the manuscript.
LIST OF ABBREVIATIONS
| ANC | = Antenatal Care |
| CPD | = Cephalopelvic Disproportion |
| CS | = Cesarean Section |
| NND | = Neonatal Death |
| CTGs | = Cardiotocographs |
| NICU | = Neonatal Intensive Care Unit |
| PPH | = Peripartum Hemorrhage |
| PMH | = Princess Marina Hospital |
| VBAC | = Vaginal Birth After Cesarean |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval to conduct the study was obtained from the University of the Witwatersrand Ethics Committee, reference R14/49. The Health Research and Development Division, Ministry of Health and Wellness, and the PMH Research and Ethics Committee, Gaborone, Botswana, granted permission to conduct the study. Permission was granted, and confidentiality was maintained by not including patients’ identifiers in the data extraction tool.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Permission to conduct the study was granted, and patient consent was waived to conduct review of the registry by the Health Research and Development Division, Ministry of Health and Wellness, and the PMH Research and Ethics Committee, Gaborone, Botswana.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the support of Mr. Akeem Ketlogetswe (statistical analysis), Ms. Goratileone Rapitse (coordination and data collection), and Mrs. Henrietta Thandie Matlelane. The authors would like to thank the hospital managers.

