All published articles of this journal are available on ScienceDirect.

Understanding and Preventing Gender-based Intimate Partner Violence among West African Immigrants of Washington State, USA Community-based Participatory Research
Authors Info & Affiliations
Abstract
Introduction/Objective
A community health assessment conducted with the Washington West Africa Center identified ending domestic violence (DV) as a priority within the West African immigrant population in the greater Seattle area. This study seeks to understand the intersecting factors that increase the risk of DV and identify strategies to inform prevention and policy.
Methods
This cross-sectional qualitative study utilized the principles of community - based participatory research, involving in-depth interviews with 32 immigrant African women who survived DV from male intimate partners in Washington state (n=31) or acted as a key informant of DV (n=1). The interview transcripts were analyzed using descriptive thematic analytical methods.
Results
All participants experienced their first DV episode before age 26, typically during cohabitation, pregnancy, or childrearing with partners aged 26–30 years. Duration of DV ranged from 3 to 36 months. Key facilitators for exiting DV relationships included social support (50%), safety concerns for self or children (31.6%), economic empowerment (~8%), and DV education (5.3%). Perceived love by survivors was the most common reason for remaining in abusive relationships (58%), followed by fear of law enforcement involvement (18%). Stigma and shame were major barriers to seeking help.
Discussion
Study findings were similar to the regional existing literature of risk factors and common stressors that increase DV, but strategies to prevent it were distinct to this demographic.
Conclusion
Interventions leveraging cultural values like community networks of social support, empowerment and family values should be prioritized for effective DV prevention in close-knit African immigrant communities.
1. INTRODUCTION
1.1. Background
Sexual and gender-based violence (GBV) is defined as any act that is perpetrated against a person’s will and is based on gender norms and unequal power relationships. Most victims of sexual and gender-based violence are women and girls; most perpetrators are or have been intimate partners of victims and survivors [1]. Intimate partner violence (IPV) refers to behavior by an intimate partner or ex-partner that causes or is intended to cause physical, sexual, or mental or psychological harm, including physical aggression, sexual coercion, psychological abuse, and control [1, 2].
Globally, nearly 1 in 3 women have been subjected to physical and or sexual violence, and 26% of ever-married/partnered women aged 15 years and older have been subjected to physical and/or sexual violence from a current or former husband or male intimate partner at least once in their lives [1-3]. Other documented forms of violence against women worldwide include cyberviolence, acid throwing, deliberate marking, deprivation (food, resources, social), forced marriage (dowry deaths, honor killings), sexual trafficking, slavery, and rape [3-6].
From 2011-2015, data from the Washington Department of Health indicated that reported DV offenses in King County were common at 450 cases per 100,000 persons [7]. In 2016, Washington State also reported that 19.7% of DV homicide victims were born outside the United States [8].
From 1997 through 2009, there were 61 confirmed fatalities from DV in Washington State for which the victims were identified to be immigrants or refugees [9, 10]. There is no data available on the geographical demographic or ethnic origins of the homicide victims.
The African immigrant community in Washington state, started growing in the 1990s following socio-political crises on the continent of Africa [11]. In 2024, of the about 8 million residents of WA state, only about 4% or ~346,000 identified as black/ African American, whether domestic or foreign-born African immigrants [12]. Of this number, the foreign-born Africans make up just over 78,000 people. Because the East African immigrant population who migrated following the wars in Somalia and the Horn of Africa in the early 1990s constitutes a much longer and larger presence in Washington state, it is estimated that the West African diaspora is much smaller in number. The community organization Washington West African Center WAWAC reports serving more than 20,000 people of West African descent in Snohomish, Pierce, and King counties, identifying many barriers to achieving optimum health for this community, many amplified during the COVID-19 pandemic [13, 14].
Historically, most of the early West African immigrants came from The Gambia, seeking political asylum following decades of the brutal, repressive military regime of then President Yahya Jammeh [15, 16].
The Washington West African Center (WAWAC) was initially conceived to address the need gap for the Gambian community who survived that trauma. With time, WAWAC was expanded to include other West African immigrant people from other West African countries - Senegal, Mali, Ivory Coast, Nigeria, Ghana, Gabon, Togo, and Cameroon [14]. WAWAC reports that the community it cares for is predominantly family-oriented, majority Muslim, and conservative. The members of the WAWAC community largely hold conservative views on traditional gender roles, with men as providers/decision-makers and women as homemakers and mothers [14].
In addition to these cultural norms, members of the West African community also embody other intersecting identities that marginalize them and make them more vulnerable to systemic and structural harm. Those intersecting identities include being black/ black race, immigrant or undocumented status, non-native English speaking, unemployed or underemployed, being poor, culture of patriarchy, traditional gender roles, and other factors that make them more likely to suffer DV and ill health [17-21]. Other US and regional studies have revealed how the immigrant status confounds with other negative socioeconomic factors like poverty, overworking, or low employment to exert negative pressures on marital and other intimate relationships that can lead to DV that harm children and families [21-29]. According to WAWAC, the community they serve exists in mostly close-knit, culturally conservative heterosexual families, with DV being gender based, and perpetrated by men on women [30]. Therefore, throughout this study, we will refer to IPV as DV against women or DV.
1.2. Rationale/ Justification for Study
A prior community health assessment conducted by WAWAC in partnership with the University of Washington’s School of Public Health in 2022 identified DV against women (DV) as a key concern of the community, undermining the health of families [21].
WAWAC had provided anecdotal evidence gathered through interactions with community members supporting families through their programs, such as the Grandma Association's traditional marriage counseling that has been utilized by many couples to resolve conflict, including those that qualify by definition as DV against women or DV. Those anecdotes have documented DV against women and girls, which is prevalent in the West African immigrant community of the greater Seattle area. WAWAC therefore reached out to the study team to collaborate in gathering scientific evidence of the public health problem, its impact on families, how best to support survivors, and prevent its recurrence. In doing so, the researchers used a Constructivist stance to co-create a truly collaborative study that seeks to build understanding and knowledge from the perspective of the survivors of DV in this community. In the same paradigm, the study findings are also expected to improve WAWAC’s programs and services to families experiencing DV. WAWAC collaborated with the study team from conceptualization to the end of the study with the collective goal of ending the root causes of DV and IPV that are harming the families and communities they serve and identify with in a culturally acceptable way.
The results from the study are expected to contribute to generalizable knowledge of preventing IPV and DV in similar culturally conservative immigrant communities and possibly inform future culturally acceptable policy on public health that centers on and protects women, children, and families surviving DV in this demographic.
1.3. Objectives
This study aims to answer the research questions of how immigrant West African women experience DV in their community and how the community can work together to end it. The study will assess the experience and forms of DV in this community, assess the strategies for survival or resilience, and include the community’s knowledge of resources available in the community to support survivors of DV.
The specific study objectives were to assess/ determine:
(1) Risk factors for DV among the WA immigrant community
(2) Strategies for survival/resilience by DV survivors
(3) Explore policy recommendations to help prevent DV in West African immigrant communities
(4) Knowledge of resources available in the community to support survivors of DV
1.4. Definition of Terms
1.4.1. Intimate Partner Violence/ Domestic Violence/ Domestic Abuse
Intimate partner violence, also known as domestic violence or domestic abuse, is a pattern of behavior in any relationship that is used to gain or maintain power and control over an intimate partner. Abuse is physical, sexual, emotional, economic, or psychological actions or threats of actions that influence another person. This includes any behaviors that frighten, intimidate, terrorize, manipulate, hurt, humiliate, blame, injure, or wound someone.
1.4.2. Gender-based Violence (GBV)
Gender-based violence is defined as all forms of violence committed against a person because of his or her sex or gender. It is forcing another person to do something against his or her will through violence, coercion, threats, deception, cultural expectations, or economic means.
2. METHODOLOGY
2.1. Study Design
This descriptive cross-sectional study was designed as a qualitative community-based Participatory Research (CBPR) study where academic researchers collaborated with a community partner (WAWAC) and its program participants to conceptualize and conduct the study. University of Washington Institutional Review Board approved the study on July 11, 2023; recruitment of participants and data collection were completed on September 18th, 2023.
2.1.1. Study Research Team and Positionality
The research team consisted of public health professionals, academics, and community partners with varying degrees of exposure to trauma-informed qualitative methods and work involving domestic violence. Team members approached the work with care and sensitivity to the cultural and linguistic background of the study participants. See Table 1 below for detailed research team positionality, reflexivity, and credentials in relation to DV work and proximity to the study population.
2.2. Study Setting
The study was designed and conducted as a collaborative effort between academic researchers and a local community organization (WAWAC) that served primarily West African immigrant residents of Snohomish and King counties. An earlier community health assessment conducted by University of Washington students identified addressing DV against women as a major health concern for WAWAC’s community. WAWAC already had programs in place to tackle the issue of DV, but needed to scientifically understand what was driving the problem, how the community was responding to their program, how to better serve survivors of DV, and any ideas to help prevent future violence and improve outcomes for survivors and their families.
WAWAC’s programs included: (1) emergency food and housing for survivors to escape DV, (2) food for families and afterschool programs for children to prevent future DV by reducing known financial stressors and aggravators of DV, and (3) Grandma association marriage counselling service to help resolve couples’ conflict and DV issues in a culturally acceptable way.
Interviews were conducted in three settings based on participant preference: (1) a private room at the WAWAC office, (2) participants’ homes when deemed safe, and (3) Zoom for individuals who preferred remote participation or faced childcare/transportation barriers. Privacy was prioritized by ensuring that no partners or family members were present; participants were reminded to choose a safe, uninterrupted space for Zoom interviews. When safety concerns arose, interviews were paused or rescheduled. Participants were recruited from all of Washington State as long as they satisfied our inclusion criteria.
Interview questionnaires were designed in English and French in anticipation of the anglophone and francophone languages of West African people. Interviews were conducted in English, with interpreters (on standby) as needed. All study settings were intended to strengthen the contextual transferability of study results to this unique community.
| Research Team Member | Credential | Training in Trauma-informed Qualitative Methods | Gender Identity | Cultural/ Linguistic Background | Relationship to WAWAC | Relationships with Participants and Positionality |
|---|---|---|---|---|---|---|
| First author and Principal Investigator (RY) | MD, MPH. | Yes | Female | West African background. Fluent speaker of English, Hausa, Pidgin, and Basic Arabic | Served on WAWAC board from 2024-20245. Not on the WAWAC board during study procedures | No relationship with participants. RY identifies as an immigrant woman from West Africa and culturally Muslim recognizes and validates the participants' experience of DV due to growing up witnessing DV, several years’ experience working with DV survivors in the local immigrant community, public speaking about DV, and teaching classes on Violence prevention at the University of Washington. This has allowed her to recognize cultural nuances during interviews and in carrying out study procedures. Some participants also recognized her as a trusted person to open up to during the interview. |
| Co-author and Research Assistant (PJ) | MD, MPH. | Yes | Female | West African background. Fluent speaker of English, Twi | No relationship with WAWAC | No relationship with participants. |
| Co-author and Research Assistant (AT) | BSc Public Health-Global Health | Yes | Female | European American background. Fluent speaker of English and French | No relationship with WAWAC | No relationship with participants. |
| Co-author (DM) | BVM, MSc, PhD | Yes | Male | East African background. Fluent speaker of English, Korean, and Luganda | No relationship with WAWAC | No relationship with participants. DM is a witness to DV growing up in a large East African family living together in a patriarchal multigenerational home. |
| Co-author (OJ) | High School, Non-Baccalaureate education | No | Male | West African background. Fluent speaker of English, Wolof, and Mandinka | Works at WAWAC | Works closely with the key informant and co-runs the DV program. OJ is a witness to DV growing up in a large West African patriarchal multigenerational home. OJ provided support with connecting the academic team with program staff and potential participants for recruitment, funding of one research assistant, and providing feedback on culturally sensitive matters, including during manuscript development. |
2.3. Study Population
2.3.1. Eligibility and Recruitment
We employed a purposive sampling technique to recruit immigrant African women survivors of DV who have received services through WAWAC. Women were recruited via WAWAC’s WhatsApp messaging using e-fliers advertised at all WAWAC program websites and physical locations (Appendix A). It was not possible to track how many individuals actually viewed the materials, but we estimate that up to 500 people were potentially reached through all the channels. Survivors who felt ready and able to share their experiences self-identified and contacted WAWAC, who in turn contacted the study team using the information provided, who then proceeded with screening for eligibility, informed consent, and applying other study procedures. The recruitment process is outlined in Fig. (1) below.
We determined eligibility for the study according to our inclusion criteria and excluded those who did not meet them.
2.3.1.1. Inclusion Criteria
We included people who self-identified as adult African immigrant women 18 years or older, married, in long-term intimate or cohabiting relationships of any duration, living in Snohomish, King, or Pierce County. Must be receiving or have received services from WAWAC.
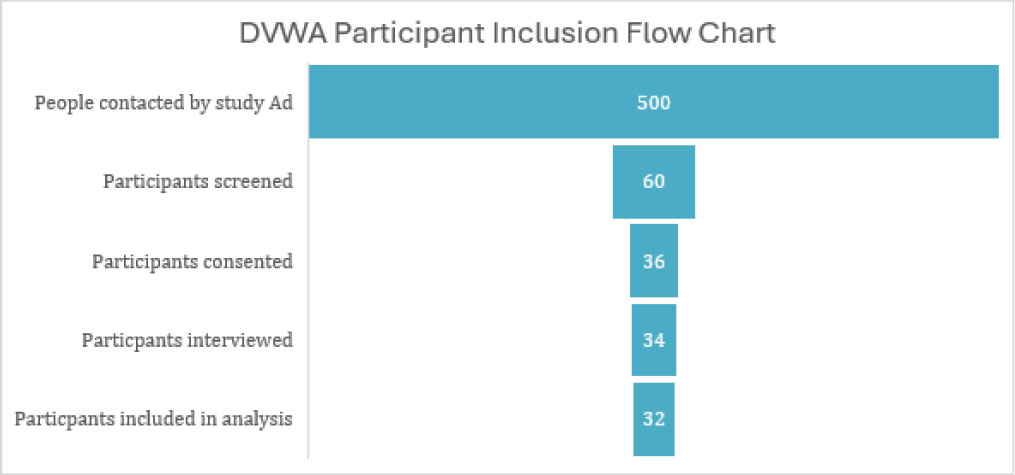
Study participant recruitment flow chart.
2.3.1.2. Exclusion Criteria
We excluded those who did not meet our inclusion criteria, i.e., those who did not identify as African immigrant women who had never been in a cohabiting DV relationship, such as marriage or ever living together, and those who never lived in areas served by WAWAC (i.e. lived outside of Snohomish, King, or Pierce counties of WA states). People who were unable to provide verbal consent in the languages included (English, French, Wolof, Hausa, Fulfulde, Mandinka) were also excluded.
Following the advertisement, we were contacted by about 60 women, and we determined that 34 of them were potentially eligible for in-depth interviews (IDI). During the IDIs, researchers interviewed 34 women, of whom 31 experienced violence from long-term heterosexual relationships with male partners, while 2 women experienced violence from other women in same-sex relationships, and one was a key informant.
As our study is on DV in this predominantly culturally conservative community, we excluded the data collected from the 2 participants who were in same-sex relationships to prevent an outlier effect on the results. Cases involving same-sex relationships were outside the scope of this project due to the study’s focus on heterosexual IPV dynamics within the majority conservative West African immigrant community. Only 2 out of the 33 participants were in same sex female only sexual relationships, and that largely did not reflect this community. Study finding is expected to be transferable to other similarly conservative demographic African immigrant communities, but may likelynot be transferable to the LGBTQ+ survivor communities, where risk factors may be different.
2.4. Data Collection
We used in-depth interviews to gather all our data from the study participants. We used purposive sampling techniques to recruit only participants who fit our inclusion criteria and who had accessed any of WAWAC’s services or programs. WAWAC acted as collaborative study partners to aid us in recruiting participants and achieving our study objectives.
2.4.1. Qualitative Data Collection
Researchers conducted in-depth interviews (IDIs) of 45-60 minutes each with 30 women survivors of DV and one key informant involved in the Grandma Association Counselling Program. IDIs were conducted in a private location of choice of the individual participants, including remotely over Zoom. We verbally obtained and then documented informed consent for the study in English (Appendix B) or French (Appendix C) based on the preference of each of the study participants. Participants who were not proficient in English were accommodated with an interpreter offered during both the informed consent process and the IDI process. All IDIs were audio-recorded on a non-Internet-connected portable recording device (Klitten 64GB professional voice recorder), immediately transcribed, de-identified, and translated into English. About 3 participants did not consent to be recorded, and for those, only interview notes were obtained. The original recordings with identifiable audio were then permanently deleted and destroyed to maintain confidentiality. All transcripts were stripped of identifiers, and master ID keys were stored separately from the data. This workflow ensured both linguistic fidelity and participant confidentiality. Questions to all interviewees were similar using a structured interview guide (Appendix D) to gather key information on (1) knowledge of DV -types, aggravators and pacifiers, (2) experience with surviving DV, (3) barriers and motivators to exiting DV, (4) experience navigating community resources to prevent or exit DV especially from WAWAC.
In addition to DV survivors, we also conducted one IDI with a key informant from WAWAC to enrich the data, to get a sense of how programs and services were tailored towards DV prevention programs and what the perceived challenges for WAWAC are for program success. The key informant was a member of WAWAC’s Grandma Association, which provided traditional marriage counseling services at WAWAC for immigrant couples and contributed towards the culturally relevant model of services provided at WAWAC.
Each participant completed one in-depth, semi-structured interview lasting approximately 45-60 minutes. With participant permission, interviews were audio-recorded; if a participant declined recording, the interviewer took detailed hand-written field notes. The research team followed a trauma-informed interviewing protocol throughout the study that prioritized human-centered approaches, humility, and empathy. The questionnaire was designed with rapport building first and asking heavier questions last. During interviews, researchers carefully took time to respectfully explain and obtain informed consent, establishing rapport, emphasizing safety and confidentiality, and being explicitly flexible about taking breaks and emotional support throughout interviewing. All audio recordings and notes were de-identified by removing names and other identifying details and assigning a participant number (e.g., w1, w2, w3, etc.) before transcription. During data collection, the research team huddled each day before starting to anticipate and prepare for emotionally taxing conversations; and after interviewing, researchers would debrief and check in for mental well-being and other healing exercises, as well as discuss lessons learned from the survivors. These wellness and preparatory checks for both researchers and participants prevented and mitigated triggers and re-traumatization, additionally it provided space for more authentic relationships during and after the study.
Interpreter services were available throughout the study as needed for clarity, but we found that all participants spoke English and, in fact declined use of interpreters, which may have diluted some of the data despite all our interpreters were seasoned for sensitive community-based research.
2.4.2. Qualitative Data Analysis
After concluding the in-depth interviews, we collated all the transcripts. Researchers used reflexive thematic analysis following Braun & Clarke’s six-phase approach to qualitatively analyze data from 30 IDIs of women survivors of DV and 2 key informants. A codebook was manually developed in English inductively from the transcribed de-identified data. Field notes were also used to capture non-verbal expressions and cues of the women participants and to provide context to their speech during the interview. A total of 3 researchers participated in data collection and analysis of the data, including code development.
Researchers independently manually coded an initial set of transcripts, met to discuss interpretations, and refined the codebook through consensus. Because reflexive thematic analysis emphasizes depth rather than quantification, intercoder agreement metrics were not used intentionally. A meeting with the Community partner at WAWAC was conducted to discuss findings and collaboratively correct any errors, misconceptions, or misinterpretations in the analysis.
Researchers identified 3 core themes and several sub-themes running through narratives consistent with (1) general perceptions of domestic, gender-based, and intimate partner violence, (2) with reasons for staying (3) or leaving an abusive long-term relationship by the women.
3. STUDY LIMITATIONS AND MITIGATIONS
3.1. Language Barrier
WAWAC serves diverse African and colonial language speakers (English, French, Mandinka, Wolof, Hausa, Fulfulde, Pidgin). We mitigated these by providing options to communicate research materials in the language of choice of the participants, both verbally and in print.
3.2. Recall Bias
People might not recall in full detail experiences of violence, especially very traumatic events, for which forgetting was a coping mechanism. Researchers mitigated this bias by allowing interviewees sufficient time to think about their answers before answering.
3.3. Social Desirability Bias & Underreporting
DV is a very stigmatized subject in the West African immigrant community, associated with a lot of shame about being a victim of DV. It is possible that the actual severity of violence experienced was underreported, watered down, or hidden. Participants were given the option to opt-out of audio-recording, to ensure confidentiality and maintain anonymity.
3.4. Economic Ethical Threat
Participants of the study each received $20 grocery gift cards from WAWAC to compensate for their time after being interviewed by the research team. To mitigate, participants were not aware that they would be receiving the gift card until a week after all data collection was completed. It is worth noting that, $20 is regarded a fair compensation for an hour according to the Seattle area standard minimum wage of $20.76 per hour.
3.5. Rigor and Trustworthiness of Data
All the women included in the study came directly from a pool that was reached out to through the advertisement by WAWAC DV program personnel. Phone numbers and other contact information included in the Ad only listed WAWAC official phone numbers (see Appendix A), making the participant pool strictly from WAWAC program recipients. Only one key informant was included in the study, and data from the key informant largely confirmed participants’ results and sentiments on DV risk, causality, and experience in this unique mostly religiously conservative community. As mentioned earlier in the paper, study results were presented to community members in December 2024 with many of the participants in attendance, appreciating how their stories, strengths, and resiliency were respectfully portrayed.
4. ETHICAL CONSIDERATIONS
The authors confirm this research was conducted on humans by the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931). The study was approved by the University of Washington Institutional Review Board (IRB ID# STUDY00018293) on July 11th, 2023. A verbal informed consent document was provided and/or documented in English and French. Strict confidentiality of participants was maintained throughout by collecting data in private settings, deidentifying data during analysis, and ensuring the anonymity of the participants. Participants were repeatedly reminded of their rights, risks, and benefits of participating in the study and about their right to withdraw from the study at any time without consequences from WAWAC for social services benefits they were obtaining from WAWAC.
5. RESULTS
5.1. Demographic Characteristics of Study Participants
The study participants were 31 women in total (N=31); 30 were survivors of DV, while one was a key informant. The mean and modal age of the male abusers were identified as 29 and 30 years, respectively. The mean age was 25 years, and the modal age of the participants was 26 years. The duration of an abusive relationship reported ranged from 3 to 36 months. The overall mean duration of abuse was 32 months. See Table 2 below for a tabular representation of the overall key socio-demographic characteristics of the participants included in the study.
5.2. Findings
5.2.1. Nature of the Abuse
Almost all the participants reported being physically abused (n=29, ~94%). Verbal abuse was common (n=24,77%), followed by a common factor of emotional abuse (n=14, ~45%). Sexual abuse (n=6, ~19%) and financial abuse (n=3, ~10%) were the least reported types of abuse.
5.2.2. History of Abuse
During their relationship prior to marriage or cohabiting the same living space, only 5 women (~16%) reported male partner abuse; of which, 3 reported verbal abuse, one reported physical abuse, and one reported emotional abuse.
| Key Demographic Characteristics of Participants | Value Range |
|---|---|
| Age range of Female Survivors | Age range of 21–48 years, Mean Age of 25 years, Modal Age of 26 years |
| Age of Male Abusers | Mean Age of 29 years, Modal age of 30 years |
| Marital status | Married, separated, divorced |
| Country/region of origin | The Gambia, Senegal, Sierra Leone, Liberia, Cameroon, Nigeria |
| Years living in the U. S | 1–15 years |
| Duration of Abuse before exiting | Duration range is <1 year to 8 years. Mean duration is 2. 7 years |
| Language used in the interview | English |
| Interpreter use | An interpreter was used to develop an informed consent form in French. Interpreter offered to participants for consenting and interview in the language of their choice (French, Wolof, Hausa, Fulfulde, Mandinka), but all participants declined and maintained conversations in English. |
| Employment/household roles | Employed (self-employment or corporate) -Unemployed. |
As for prior history of abuse in a woman’s family, prior to the relationship, most women (n= 29, ~94%) reported witnessing or experiencing physical or verbal abuse in their home by a male family member, with several women (n=20, ~65%) insisting that verbal abuse from fathers towards wives and children was a normal common occurrence. A sentiment echoed by our one key informant (w33) who said, “Well, it’s normal for men to verbally abuse us, they are tired and come home wanting to rest. If you bother them, they will curse you out. That’s normal and acceptable.”
5.2.3. Reasons for Remaining in the DV Relationship and Home
Love of the male partner, family, or children was the commonest reason to stay in abusive relationships, and 8 women (26%) explicitly mentioned love, while 5 women (~16%) mentioned belief that the abuser will change or having faith in the abuser as a reason to remain in DV relationships. Considering both as sentiments of affection, we can say that love and affection are the most common reasons for women to stay in DV relationships or situations (40%). One survivor (w20) said, “I was attached to him because I felt this manly love for him …I loved him so much”.
More than 10% of participants cited concerns about their children growing up without a second parent or father as a reason why they did not leave an abusive situation. One woman (w21) said, “So, it’s because of my children. I just couldn’t leave because I did not want my children to grow up without a father.”
Avoiding contact with the police and other legal channels was another strong motivator for remaining in violent, abusive relationships. About 18% of participants cited avoiding police encounters and going to court, either because they fear adverse outcomes from police such as jail time for their spouse or reflecting negatively on their immigration paperwork. One woman (w5) reported, “He has this sick mom, so I didn’t want to involve the police because it might trigger something (sic: healthwise for the mom)”.
Researchers also learned that there is widespread social stigma associated with disclosing being in an abusive relationship in the West African community culture, or of being divorced or unmarried, mentioned explicitly by 5 women (16%). One survivor said (w4), “I couldn't tell my friend that I was being abused, …. then to me, it was something to be ashamed of that your man is actually hitting you”. Our key informant (w33) said, “Well it’s not nice to be divorced. I think they (survivors) stay for the kids so they won’t have broken homes and so they too can be respected in the community. If you are a grown woman in your twenties and no husband, then you have no value- people will think you are wayward.”
5.2.4. Strategies for Survival / Resilience and Reasons to Exit DV Relationships
Researchers discovered that situations that led to independence and empowerment of the women account for most of the reasons why women leave DV situations. Those reasons include family and friend support (50%), Self-determination via economic empowerment (~8%), concern for personal safety (10.5%) and education about DV (~5%).
Almost half of all participants (n=16) strongly reported being able to exit the abusive relationship because of the strong family or friend support they received. They were more likely to exit a relationship if they perceived that there was someone close to them that is supportive. One woman (w20) who previously gave store affection as a reason to stay said,“… talking to some friends who encouraged and told me I am better, and I don’t deserve what I was experiencing in my relationship”.
Leaving because of children’s safety, born and unborn, was reported by about 20% of women (n=8) who exited abusive homes. One survivor (w32) who was able to exit the abusive relationship after 7 years of living in a violent marriage and a near-death experience which left her in a coma said, “Leave the relationship, it’s hard, but for the sake of your life and children just leave”.
6. DISCUSSION
6.1. Risk Factors for DV Among Immigrant Communities
It has been established that migrants and refugees are at an increased risk of experiencing DV because they are isolated from supportive families, face unstable employment, have economic dependence on their partner, have an uncertain immigration status, struggle with a language barrier, and are more likely to report a lack of access to support services [25, 27]. We found that all our study participants had reported one or more of these well-known risk factors to accompany their experience of DV.
In a 2009 analysis of the relationship between immigration and experience of DV, interviews with 137 immigrant women in the United States revealed how the stress of relocation to the US introduced their partners to new interests, such as alcohol, drugs, gambling, and infidelity, which were soon followed by new abusive behaviors by their partners [31, 32]. We unfortunately heard similar narratives from the women in this study who reported that relocation to the U.S. was associated with a rise in the level of violence in about 50% (n=16) of cases, with another 22% (n=7) stating that violence from their partner began after relocation to the US.
Several studies over time and space have consistently reported the role of patriarchy and gender roles in risking by several studies of predictors of IPV and DV over time and place. Several studies have postulated how the increased economic opportunities in the U.S. for immigrant women threatened widely accepted patriarchal traditional gender hierarchy and norms in their community, with some men responding with violence when those long-held beliefs are challenged [31-34]. It is important to note that traditional gender roles that inform behavior remain dominant in this culturally conservative West African community, with many of our study participants reporting that their personal economic success in the USA, which challenged traditional gender roles were not welcomed by their envious male spouses, who in turn sometimes responded with violence and/or abuse.
Another important intersection we found that worsened DV was an unfavorable or vulnerable immigrant status, such as the DV victim being undocumented or dependent on a male spouse to obtain a permanent residence permit (green card). About 42% of the women we spoke to (n=13) reported spouses using threats of deportation as a tool of financial, sexual, and emotional abuse, similar to some studies that reported threats of calling Immigration and Customs Office (ICE) officials and reporting their spouse’s irregular immigration status [31]. A meta-analysis of 30 IPV studies in Canada also identified the use of immigration as a threat to women by their spouses [24]. However, we uncovered a unique situation in this study, not supported by the literature review, whereby the male perpetrator of violence is protected from immigration enforcement by the DV survivors because the women feared community stigma of marital separation (n= 5), or did not want their children to be without a father (n= 8).
Another study of Korean immigrant women experiencing IPV in the US attributes childhood victimization and patriarchy as a risk factor for experiencing, staying, and or accepting IPV [17]. A 2023 study found strong links between the occurrence of IPV and patriarchy in the homes and lives of DV survivors on asylum applications in the United States [20]. Both patriarchy and weaponizing precarious immigration situations of women have been blamed to increase risk of DV by the women in our study. Other risk factors like toxic masculinity, antisocial personality disorders, low level of education, substance use, and traditional gender roles/ patriarchy that give men perceived control or rights, including sexual liberties over their female spouses and partners, have been well studied as factors increasing the risk of perpetrating DV/IPV against women and girls [29, 35-37]
6.2. Impacts of Violence Against Women, DV, IPV, and GBV
Globally, women exposed to IPV have a 42% increased risk of death and serious physical and sexual injury from the encounter, while about 38% of all murdered women died at the hands of their intimate partner [1, 3]. Victims of IPV/GBV are 2 times more likely to experience depression, anxiety, sleep and eating difficulties, psychiatric and other substance use disorders; 1.5 times more likely to acquire a sexually transmitted infection, and 16% more likely to have poor birthing outcomes, including preterm deliveries and low birth weight babies [26, 28]
Women suffering IPV are more likely to suffer isolation, lost wages, and poverty than their non-abused counterparts, while children living in violent homes are more likely to suffer behavioral and emotional problems, are at increased risk of experiencing and perpetrating violence later in life, and more likely to die or suffer childhood illnesses as their mothers have limited access or ability to care for themselves [3, 17, 23]
6.3. Strategies for Survival / Resilience
In a 2017 qualitative study of survival strategies used by low-income black women who experience intimate partner violence, religion was uncovered as an internal strategy to surviving DV [38]. Some of our study participants (n=5, 16%) shared that their faith, belief in God, their religion, or reaching out in church helped them endure or overcome the violence experienced at the hands of their abusers.
Another internal strategy was independence and self-reliance. Many of the women (n= 8, ~26%) identified strategies to gain financial independence, such as getting a job or working a degree. Women attributed obtaining independence to empowering them to leave the abusive relationship, while others reported physically fighting back using defensive violence to either save their lives or to reduce the violence inflicted on them by their abusers.
A common external strategy used by most women (n=21, ~68%) was leaning into social support networks, such as relying on close family or friends or community elders to plead with their husband or man about ending the abuse. However, they also reported that this strategy was usually unsuccessful. This finding is similar to other regional DV studies in North America on immigrant groups [29, 36, 37].
Another documented external strategy was utilizing community resources, including hospitals, shelters, DV organizations, or other non-punitive/legal organizations in the community. In our study, few women (n=4, ~13%) reported the use of DV services shelters to exit the abusive relationship, even though they expressed favor of emergency shelter and housing as a culturally appropriate long-term solution to ending DV. This finding was similar to a 2017 US study on low-income black women experiencing DV [38].
Well-known barriers to access and utilization of social services by abused immigrant women include language/ communication barriers, involvement of legal systems, and complex immigration issues [23]. As some of our study participants (n= 6,~19%) have explicitly alluded to aversion to legal channels like involving the police to resolve DV, the successes of such strategies that involve criminalization will likely continue to be perceived as not culturally suited or appropriate in tackling DV; like an earlier Canadian study among immigrant communities [24]. In fact, in our studies, most women (n=22, 71%) preferred to do nothing rather than reach out to community resources for DV intervention for fear of stigma or the possibility of negative outcomes because of involvement of police or immigration officials when resolving DV matters.
A scoping review of 15 articles addressing the topic of DV among Asian and Latinx immigrant communities suggests building unique interventions unique to the immigrant groups, which would better prioritize survivors and enable survivors to engage in social services, rather than going the path that criminalizes perpetrators, which induces fear of social isolation [38]. Such an example of a culturally responsive program to ending DV, known as SASA! was developed and implemented in Uganda. SASA! uses aspects of the UN/WHO RESPECT framework for preventing violence against women and tenets to address power imbalances of traditional gender roles. SASA! also utilizes community mobilization, interactive and reflective activities (rather than the path of criminalization) to unpack different dimensions of power and other key themes (gender, violence, activism, and collective responsibility) to help create community-level collective change in violent behaviors. SASA! The program has been shown to make communities safer for women by decreasing women’s risk of experiencing physical violence from their male partners by 52% [39-41].
CONCLUSION
This study highlights the importance of emotional family values as reasons why women both stay and leave abusive relationships. We discovered a cohesive community and population averse to police presence and legal channels for resolving DV, so much so that those channels are paradoxically a reason women stay in harmful situations. Policymakers and community organizations like WAWAC should leverage family values in finding lasting, culturally acceptable solutions that center on family values in interrupting and preventing DV.
We recommend policymakers lessen barriers to the immigration rights of women by continuing legislation like the Violence Against Women Act that protects the rights of minority immigrant women surviving violence from US spouses in the immigration process.
We recommend community organizations working to prevent DV against women to use approaches and strategies that include all community members, especially male perpetrators of violence, when preventing future violence is especially a priority. A successful program they can adopt is SASA!, a successful community mobilization program in Uganda that uses approaches that address power imbalances of gender inequality to prevent violence against women in communities. SASA! worked by challenging community members to interrogate and critically analyze their use of power in their interpersonal relationships. When SASA! Was tested in a randomized controlled trial, SASA! was shown to change beliefs of women's rights and prevent physical and sexual violence against women in communities. It was implemented versus control communities that did not implement SASA! Programs in their communities [39].
We further recommend that policymakers work with community organizations and leaders such as WAWAC, places of worship, and families to adopt evidence-based successful strategies in ending all violence against women, including DV. The World Health Organization and the United Nations’ RESPECT for Women framework for preventing violence against women, can be adapted to prevent DV and VAW in immigrant communities, especially where current modalities are unsuccessful. The RESPECT women framework champions strategies that transform attitudes, beliefs, and norms around DV and VAW by employing strategies that reduce poverty, improve access to social services, strengthen relationship skills, empower women, and expand safe and enabling spaces for survivors of violence. Furthermore, the RESPECT women framework empowers families and communities to abolish harmful cultural practices and norms. We found that WAWAC was already delivering vital social services recommended by the RESPECT women framework through its DV prevention program that centered on the needs of the family. WAWAC programs aimed to lessen DV stressors and empower communities with adult literacy classes, afterschool kids’ program, Sutura housing program, bi-weekly family food distribution, and other community and work navigation resources that eased common DV stressors/aggravators like poverty, housing instability, and lack of education. Furthermore, WAWAC had engaged with several policymakers, local and state, to partner on solutions for long-term DV prevention, like WAWAC Futuristic Housing Project for the community and expansion of educational programs, including WAWAC’s Grandma Association marriage counselling
AUTHOR’S CONTRIBUTIONS
The authors confirm contribution to the paper as follows: R.Y., P.J., O.J.; Study conception and design; R.Y., P.J, A.T.: Data collection; R.Y., P.J., A.T., O.J.: Analysis and interpretation of results; R.Y., P.J, A.T, O.J, D.M.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| IPV | = Intimate Partner Violence |
| DV | = Domestic Violence |
| VAW | = Violence against Women |
| WAWAC | = Washington West Africa Center |
| R.E.S.P.E.C.T | = Relationship skills strengthened, Empowerment of women ensured, Services ensured, Poverty reduced, Environments made safe, Child and adolescent abuse prevented, and Transformed attitudes, beliefs, and norms. |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the University of Washington Institutional Review Board (IRB ID# STUDY00018293) on July 11th, 2023. Researchers were given exclusive consent to approach and conduct the study collaboratively and transparently with WAWAC, which recruited study participants from its already-running DV prevention programs.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
We obtained informed consent from each participant included in our study. The informed consent procedures respected each participant’s consent for aspects of their interview they wanted shared by publishing.
Portions of the study results from this community-based participatory research have been presented at a community gathering with the study participants on December 4th, 2023. Study results have been shared with WAWAC and their program participants at a community function to discuss the results on December 4, 2023, at WAWAC offices, Lynnwood, WA, USA.
AVAILABILITY OF DATA AND MATERIALS
All data set associated with the article is stored in the Science Data Bank and accessible for viewing at https://doi.org/10.57760/sciencedb.28351 and can be shared upon reasonable request to the corresponding author.
FUNDING
The study employed 2 part-time research assistants to assist with study procedures, who were jointly funded by the principal investigator Dr. RY, and WAWAC. Study participants were provided with $20 grocery gift cards each, which were funded by WAWAC after all in-depth interviews were completed. Participants were not aware they were receiving gift cards to compensate for their time.
AKNOWLEDGEMENTS
All Survivors of DV everywhere
Women participants of the research study
Grandma Association- Marriage Counselors
WAWAC leadership, volunteers & & DV program team
WAWAC donors: All others who tirelessly support WAWAC efforts
Appendix B
Principal Investigator: Rabi Yunusa
Hello, I am an assistant professor at the University of Washington, Seattle, in the School of Public health (Department of Health systems and population health). I am planning to conduct a research study, which I invite you to take part in.This form has important information about the reason for doing this study, what we will ask you to do if you decide to be in this study, and the way we would like to use information about you if you choose to be in the study.
Why are you doing this study?
You are being asked to participate in a research study about Domestic Violence (DV) among the West African Immigrant Community of Washington State.
The purpose of the study is to find out how domestic violence affects the west african immigrant community for which you are part of, how women and families are coping with domestic violence and how to improve available community services to tackle domestic violence against women in the community. Overall, we anticipate that this study will uncover things to help the community become healthier and safer.
What will I do if I choose to be in this study?
You will be asked to tell me in your own words about your experience with domestic violence and your knowledge of the resources available in the community to support you.
I am interested in knowing when the assault started and how long it lasted. I am also interested in hearing about how you coped during the abuse and how domestic violence has affected children in your relationship with the abuser. I will be asking you of events that you think immediately lead to violence against you by your husband or intimate partner.
Study time: Study participation will take approximately one hour from start to finish and involves only one interview today.
Study location: In this study, interviews will be conducted either remotely through phone calls or in a private room at WAWAC Lynnwood site office to ensure confidentiality .Our entire conversation will be audio recorded to make sure that I remember accurately all the information you provide. You will be provided with water, soft drinks and tissues in the room should you require it.
What are the possible risks or discomforts?
I understand that your participation today will involve you talking about some personal matters which will cause some short term emotional upset. I do not expect the experience during this interview to cause ort involve any physical or emotional risk to you beyond that of everyday life. If you feel emotional or upset when answering some of the questions, stop me at any time to take a break or terminate the interview. You are free to not answer or to skip to the next question any question you are not comfortable answering.
What are the possible benefits for me or others?
This study is designed to learn more about the resources available for victims of domestic violence from the West African Immigrant Community of Washington State. As a recipient of services at WAWAC, the results of this study may lead to improvement of domestic violence services at WAWAC. If you plan to or are already receiving those services, you are likely to have direct benefit from being in this research study within a few months following the analysis of the study results.Taking part in this research study may therefore benefit you personally in the long term, or may benefit others in similar situations seeking DV services from WAWAC in future.
How will you protect the information you collect about me, and how will that information be shared?
Results of this study may be used in publications and presentations. Your study data will be handled as confidentially as possible. If results of this study are published or presented, individual names and other personally identifiable information will not be used.
To minimize the risks to confidentiality, we will keep these tapes in a safe and secure location where they will only be accessible and used by myself (the principal researcher). All the audio recording will be erased as soon as I commit the information to paper (transcribe) which will be within 24 hours/ one day. Any personal information that could identify you will be removed or changed before the data we collect are shared in any way, including with other researchers, or in publications and presentations.
Financial Information
Participation in this study will involve no cost to you. You will not be paid for participating in this study.
What are my rights as a research participant?
Participation in this study is voluntary. If at any time and for any reason, you would prefer not to participate in this study, please feel free not to. If at any time you would like to stop participating, please tell me. We can take a break, stop and continue at a later time today or stop altogether. You may withdraw from this study at any time, and you will not be penalized in any way for deciding to stop participation. If you decide to withdraw from this study, the researchers will ask you if the information already collected from you can be used.
Who can I contact if I have questions or concerns about this research study?
If you have questions, you are free to ask them now. If you have questions later, you may contact the researchers at Rabi Yunusa, +1(206)566-9597 and rabiy@uw.edu.
If you have any questions about your rights as a participant in this research, you can contact the following office at the University of Washington:
University of Washington Institutional Review Board
4333 Brooklyn Ave NE
Box 359470
Seattle, WA 98195-9470
Phone: +1 (206) 543-0098
Email: hsdinfo@uw.edu
Consent to Quote from Interview
I may wish to quote from this interview either in the presentations or articles resulting from this work. A pseudonym will be used in order to protect your identity.
Do you agree to allow me to quote your remarks in any presentations or articles about this research study?
Record Subject’s response: Yes No
Appendix C
Bonjour, je suis professeur assistant à l'Université de Washington, Seattle, à l'École de santé publique (Département des systèmes de santé et des populations, et santé mondiale). Je prévois de mener une étude de recherche à laquelle je vous invite à participer. Ce formulaire contient des informations importantes sur la raison de faire cette étude, ce que nous vous demanderons de faire si vous décidez de participer à cette étude et la manière dont nous aimerions utiliser les informations vous concernant si vous choisissez d’y participer.
Pourquoi faites-vous cette étude ?
On vous demande de participer à une étude de recherche sur la violence domestique (DV) au sein de la communauté des immigrants ouest-africains de l'État de Washington.
Le but de l'étude est de découvrir comment la violence domestique affecte la communauté d'immigrants ouest-africains dont vous faites partie, comment les femmes et les familles font face à la violence domestique et comment améliorer les services communautaires disponibles pour lutter contre la violence domestique à l'égard des femmes dans la communauté. Dans l'ensemble, nous prévoyons que cette étude révélera des choses pour aider la communauté à devenir plus saine et plus sûre.
Que vais-je faire si je choisis de participer à cette étude ?
On vous demandera de me parler dans vos propres mots de votre expérience de la violence conjugale et de votre connaissance des ressources disponibles dans la communauté pour vous soutenir.
J'aimerais savoir quand l'agression a commencé et combien de temps elle a duré. J'aimerais également savoir comment vous vous êtes débrouillé pendant les abus et comment la violence domestique a affecté les enfants dans votre relation avec l'agresseur. Je vous poserai des questions sur les événements qui, selon vous, conduisent immédiatement à la violence contre vous par votre mari ou votre partenaire intime.
Durée de l'étude: la participation à l'étude va prendre environ une heure du début à la fin et sera en seul séance
Lieu de l'étude: dans cette étude, les entretiens seront menés soit à distance par téléphone, soit dans une salle privée au bureau du site WAWAC Lynnwood pour garantir la confidentialité. Toute notre conversation sera enregistrée en audio pour m'assurer que je me souviens avec précision de toutes les informations que vous fournissez. De l'eau, des boissons non alcoolisées et des mouchoirs vous seront fournis dans la salle si vous en avez besoin.
Quels sont les risques ou inconforts possibles ?
Je comprends que votre participation aujourd'hui implique que vous parliez de certaines questions personnelles qui causeront un bouleversement émotionnel à court terme. Je ne m'attends pas à ce que l'expérience de cet entretien vous cause ou implique un risque physique ou émotionnel au-delà de la vie quotidienne. Si vous vous sentez émotif ou contrarié lorsque vous répondez à certaines des questions, arrêtez-moi à tout moment pour faire une pause ou mettre fin à l'entretien. Vous êtes libre de ne pas répondre ou de passer à la question suivante si vous ne vous sentez pas à l'aise de répondre.
Quels sont les avantages possibles pour moi ou pour les autres ?
Cette étude est conçue pour en savoir plus sur les ressources disponibles pour les victimes de violence domestique de la Communauté des immigrants ouest-africains de l'État de Washington. En tant que bénéficiaire de services à WAWAC, les résultats de cette étude peuvent conduire à l'amélioration des services de violence domestique à WAWAC. Si vous prévoyez ou recevez déjà ces services, vous bénéficierez probablement directement de votre participation à cette étude de recherche dans les quelques mois suivant l'analyse des résultats de l'étude. Participer à cette étude de recherche peut donc vous être personnellement bénéfique à long terme. ou peut-être bénéficier à d'autres dans des situations similaires cherchant des services DV de WAWAC à l'avenir.
Comment allez-vous protéger les informations que vous collectez à mon sujet et comment ces informations seront-elles partagées ?
Les résultats de cette étude peuvent être utilisés dans des publications et des présentations. Les données de votre étude seront traitées de manière aussi confidentielle que possible. Si les résultats de cette étude sont publiés ou présentés, les noms individuels et autres informations personnellement identifiables ne seront pas utilisés.
Afin de minimiser les risques de confidentialité, nous conserverons ces bandes dans un endroit sûr et sécurisé où elles ne seront accessibles et utilisées que par moi-même (le chercheur principal). Tous les enregistrements audio seront effacés dès que je commenterai les informations sur papier (transcris) ce qui se fera dans les 24 heures/un jour. Toute information personnelle qui pourrait vous identifier sera supprimée ou modifiée avant que les données que nous collectons ne soient partagées de quelque manière que ce soit, y compris avec d'autres chercheurs, ou dans des publications et des présentations.
L'information financière
La participation à cette étude ne vous coûtera rien. Vous ne serez pas rémunéré pour participer à cette étude.
Quels sont mes droits en tant que participant à la recherche ?
La participation à cette étude est volontaire. Si à tout moment et pour quelque raison que ce soit, vous préférez ne pas y participer, n'hésitez pas à nous le dire.Nous pouvons faire une pause, arrêter et continuer plus tard dans la journée ou nous arrêter complètement. Vous pouvez vous retirer de cette étude à tout moment et vous ne serez en aucun cas pénalisé pour avoir décidé d'arrêter de participer. Si vous décidez de vous retirer de cette étude, les chercheurs vous demanderont si les informations déjà recueillies auprès de vous peuvent être utilisées.
Qui puis-je contacter si j'ai des questions ou des préoccupations concernant cette étude de recherche ?
Si vous avez des questions, vous êtes libre de les poser maintenant. Si vous avez des questions plus tard, vous pouvez contacter les chercheurs de Rabi Yunusa, +1(206)566-9597 et rabiy@uw.edu.
Si vous avez des questions sur vos droits en tant que participant à cette recherche, vous pouvez contacter le bureau suivant de l'Université de Washington: Comité d'examen institutionnel de l'Université de Washington
4333 Brooklyn Ave NE
Box 359470
Seattle, WA 98195-9470
Téléphone: +1 (206) 543-0098
Courriel: hsdinfo@uw.edu
Rubrique Consentement
Vous souhaitez participer ?
Enregistrer la réponse du sujet: Oui Non
Consentement à la citation d'une entrevue
Je souhaiterai peut-être citer cet entretien soit dans les présentations, soit dans les articles résultant de ce travail. Un pseudonyme sera utilisé afin de protéger votre identité.
Acceptez-vous de me permettre de citer vos remarques dans des présentations ou des articles sur cette étude de recherche ?
Enregistrer la réponse du sujet: Oui Non
Consentement à l'enregistrement audio de l'entrevue
Acceptez-vous de me permettre d'enregistrer cet entretien en audio ?
Enregistrer la réponse du sujet: Oui Non
__________________________________________________
Nom de la personne obtenant le consentement
__________________________________________________
Date
Appendix D
1. Greetings. What is your age today? How old were you when you got married or started living with your intimate partner/ husband? [How was courtship like- how long did you know each other prior to marriage? Were you related to each other? How old was your abuser at the time of marriage or living together?]
2. What do you understand about domestic violence and abuse against women?
3. Can you tell me about a time you felt or experienced domestic violence in your relationship with your husband or intimate partner? Tell me when the abuse started in relation to the time you became a couple.
4. How has it been trying to stop the abuse? What have you done in the past to stop or interrupt it?
5. What is your support structure like- family, friends, community? Did you ever seek help outside your home? How did that look like?
6. Do you have children? How has the experience of domestic violence affected them? [Any legal process for custody, etc, who has the kids?]
7. Did having children affect the way you coped with domestic violence? Did it make you want to leave/ stop the abuse or not? how?
8. What programs are you aware of at WAWAC for domestic violence? Which ones have you tried in the past? Any suggestions on how to improve those programs?

