All published articles of this journal are available on ScienceDirect.

The use of Experience-based Co-design with Patients and Health Care Professionals in Development of an Intervention for Integrated HIV and NCDs Care in Health Care Settings: A Systematic Review
Authors Info & Affiliations
Abstract
Introduction
The rising burden of comorbidities of HIV and NCDs, such as hypertension and diabetes mellitus, particularly in resource-limited settings, is the cause of high mortality rates. To curb the mortality rates and improve health outcomes of people living with HIV and NCDs, involvement of patients and the health care professionals in patient-centred care interventions aimed at improving the health outcomes is key. The objective was to systematically review and synthesise the evidence on the use of Experience-Based Co-Design (EBCD) with patients and healthcare professionals in the development of interventions to integrate HIV and NCD care within healthcare settings.
Methods
A systematic review was conducted using five electronic databases (Scopus, Proquest, PubMed, Web of Science, and Ebscohost) covering data from January 2014 to December 2024. Among 591 identified records, 10 studies met the eligibility criteria. The review followed PRISMA guidelines and was registered on Covidence (26 February 2025).
Results
None of the reviewed studies fully implemented EBCD; partial patient engagement features were observed. Most interventions were expert-driven and disease-specific, developed through integration of research findings rather than co-design, due to resource constraints, limited funding, and lack of researcher skills in EBCD.
Discussion
This highlights a gap in participatory approaches for integrated HIV-NCD care. The absence of EBCD in intervention development highlights the need for frameworks that actively engage patients and healthcare professionals in designing integrated, patient-centred care models.
Conclusions
Strengthening participatory approaches could enhance health outcomes and reduce mortality among individuals living with multimorbidity in resource-constrained settings.
1. INTRODUCTION
The rising burden of both HIV and NCDs in Low- and Middle-Income Countries (LMICs) represents a pressing global challenge. In 2023, approximately 38 million people were living with HIV, while NCDs were responsible for over 74% of global deaths, with 85% of these occurring in LMICs [1,2]. In Sub-Saharan Africa, the convergence of the co-occurrence of HIV, Hypertension, and Diabetes Mellitus is driving increased morbidity, premature mortality, and health systems strains [3].
Despite efforts to develop integrated care models, a critical gap persists where interventions are rarely informed by the lived experiences of patients living with comorbidities. Experience-Based Co-Design is a participatory methodology that offers a structured and flexible approach to actively involve patients and healthcare professionals in identifying service gaps and designing improvements [3]. ECBD is grounded in principles of equity, partnership, and narrative inquiry and has benefitted its users with improved communication, trust, and service delivery [4]. However, its application in integrated HIV-NCD care remains limited, largely due to resource constraints, lack of training, and institutional support [5]. While there has been substantial investment made in integrated models such as the Patient-Centred Medical Home, Chronic Care Model, and WHO’s Integrated People-Centred Health Services [6,7], most were designed without active patient involvement [8,9]. The lack of interventions developed through co-design methodologies may impact the effectiveness and sustainability, particularly in primary health care settings, which are culturally diverse and resource-constrained [10-12].
In LMICs, including South Africa, where the first point of care is the primary health care and health systems struggle with fragmented services, EBCD can offer an opportunity to reframe integrated care as a collaborative human-centred process [13-15]. This review aims to synthesize existing evidence on the application of EBCD in the development of integrated HIV and NCD interventions, identifying gaps and opportunities for future research.
The research questions were formulated using the PICOT framework, as outlined below:
- Population (P): Adults (18 years and older) living with HIV and at least one NCD (hypertension and/or diabetes mellitus)
- Intervention (I): Integrated care interventions developed using Experience-Based Co-Design (EBCD)
- Comparison (C): Interventions developed without co-design or participatory methods
- Outcome (O): Improved health outcomes, service user satisfaction, patient engagement, and care delivery
- Time (T): Studies published between January 2014 and December 2024
The review questions are:
- What integrated healthcare interventions have been developed using EBCD to improve outcomes for individuals living with co-morbid HIV and NCDs between January 2014 and December 2024?
- To what extent do existing integrated healthcare interventions reflect patient-centred design principles between January 2014 and December 2024?
2. MATERIALS AND METHODS
This systematic review was conducted using Covidence software, with the review project created on 26 February 2025. The review adhered to PRISMA 2020 guidelines to ensure methodological transparency and reporting accuracy. A systematic review was most suitable for this study as it allowed for a comprehensive and transparent synthesis of existing evidence on the use of EBCD in developing integrated care interventions for people living with HIV and NCDs.
2.1. Search Strategy
Searches were performed using five electronic databases supported by the University of Pretoria library, namely Scopus, Proquest, PubMed, Web of Science, and Ebscohost, covering data from January 2014 to December 2024. Key terms included “Patient engagement,” “Experience-Based Co-Design,” HIV, NCDs, and primary healthcare. Boolean operators (AND, OR) were applied to refine searches. The full search strategy is provided in Appendix 1.
2.2. Eligibility Criteria
Eligibility criteria were guided by PICO and SPIDER frameworks, which allowed the reviewers to capture both quantitative and qualitative studies relevant to EBCD [16,17]. A summary of inclusion and exclusion criteria is presented in Table 1.
2.3. Study Selection
A total of 591 records were identified, after removing 32 duplicates, 559 titles and abstracts were screened, and 539 records were excluded. Leaving 20 full-text articles for assessment, among them 10 studies met the inclusion criteria. Six reviewers participated in the screening of articles, whilst disagreements were resolved through consensus-building tools provided in Covidence.
2.4. Data Extraction
A total of 10 studies were included in the data extraction phase. The studies were selected based on whether they developed a formal or informal intervention, employed EBCD or a Participatory Action Research methodology, or combined both approaches. The included studies reflected key elements of patient engagement, such as co-designed or co-developed interventions, or service integration guided by expert or stakeholder input. The first and sixth reviewers (N.S. and N.V.) independently assessed all eligible studies to ensure methodological consistency and alignment with the inclusion criteria, with a focus on identifying interventions that demonstrated co-design principles in both development and implementation.
| Eligibility Criteria | Include | Exclude |
|---|---|---|
| Population | • Studies involving adults (≥18 years) living with HIV and/or those with non-communicable diseases (e.g., diabetes, hypertension). • Studies involving healthcare professionals working with patients with HIV and/or NCDs in primary health care settings. • Studies that specifically target the needs and experiences of populations with HIV/NCDs |
• Studies involving pediatric populations (<18 years) exclusively. • Studies focusing solely on patients with either HIV or NCDs but not both (i.e., not addressing integrated care). • Studies that do not involve healthcare professionals as part of the co-design process. |
| Intervention/Exposure | • Studies that focused on the design, implementation, or evaluation of interventions developed using EBCD. • Interventions that aim to integrate care for HIV and NCDs within primary health care settings. • Studies that address how EBCD was used to inform the development, adaptation, or evaluation of the intervention. |
• Interventions developed without the use of EBCD or similar participatory approaches. • Studies focusing solely on medical or pharmacological interventions without an emphasis on care integration or co-design processes. • Interventions focused only on secondary or tertiary care settings, such as hospitals or specialized care centers. |
| Comparator /Context | • Studies have been conducted in primary health care settings, including community clinics, general practices, and other outpatient settings. • Studies from any geographic location, provided they address primary care integration for HIV and NCDs. |
• Studies conducted exclusively in high-resource, specialized care settings without a primary care focus. • Interventions that do not address integrated care in primary health care contexts (e.g., those focused only on hospital-based or inpatient care). |
| Outcomes | • Studies that report outcomes related to patient or provider experiences, feasibility, acceptability, and/or effectiveness of the intervention. • Studies reporting on the process and impact of co-design on service delivery, patient engagement, or health outcomes. |
• Studies that do not report on experiences or outcomes related to the co-design process (e.g., focus only on clinical outcomes like viral suppression without patient or provider perspectives). • Articles that do not evaluate or describe the impact of EBCD on the integration of HIV and NCDs care. |
| Study characteristics | • Studies that employed Experience-Based Co-Design (EBCD) methods involving patients and/or healthcare professionals. • Qualitative, quantitative, or mixed-method studies. • Studies that included Participatory Action Research (PAR) or other participatory design methods specifically involving EBCD. |
• Studies that do not employ EBCD methods or any other participatory co-design approach. • Editorials, opinion pieces, letters, conference abstracts, or commentaries without primary data. • Studies that do not include any form of stakeholder engagement in the development of interventions. |
| Other | • Peer-reviewed articles, including original research, reviews, and case studies. • Published in English. • Articles published within the last 10–15 years to ensure relevance to current practice and methodologies. |
• Articles published in languages other than English • Review papers • Grey literature, such as unpublished reports, dissertations, and policy briefs, unless they provide substantial data on EBCD in a peer-reviewed format. • Articles published more than 15 years ago, if they do not provide significant relevance to current practices in co-design or integrated care models. |
2.5. Quality Assessment
The quality of the included studies was assessed using the CASP checklist for systematic reviews, which is a widely recognised tool for evaluating the methodological rigour and trustworthiness of qualitative, quantitative, and mixed-methods research [18,19]. Each study was independently appraised by the second and fourth (S.J. and L.A.) to determine the clarity of the research aims, appropriateness of the study design, recruitment strategies, data collection and analysis methods, and the overall value and transferability of the findings. Discrepancies in quality ratings were resolved through discussion and consensus, with oversight provided by a third reviewer (L) to ensure objectivity and consistency.
2.6. Review Selection
The selection process for this systematic review adhered to the PRISMA 2020 guidelines and was managed using EndNote and Covidence software. A total of 591 records were initially identified through database searches. After removing 32 duplicates, 559 titles and abstracts were screened by all five reviewers based on predefined eligibility criteria. Of these, 539 records were excluded for failing to meet the inclusion criteria outlined in Table 1. The remaining 20 full-text articles were retrieved and assessed for eligibility. Following full-text screening, 10 studies met the inclusion criteria and were retained for data extraction and synthesis. Throughout the process, disagreements were resolved through consensus, with oversight and periodic quality checks provided by two additional reviewers (N.S and S.H). The entire selection process was documented in Covidence and is summarised in the PRISMA flow diagram depicted in Fig. (1).
2.7. Ethical Consideration
This systematic review did not require formal ethical clearance, as it involved the analysis of previously published studies and did not include direct engagement with human participants. However, the review forms part of the postdoctoral research conducted by the first reviewer Dr NMM, which received ethical approval from the University of Pretoria Faculty of Health Sciences Research Ethics Committee. The study was granted clearance under the ethics reference number 589/2025.
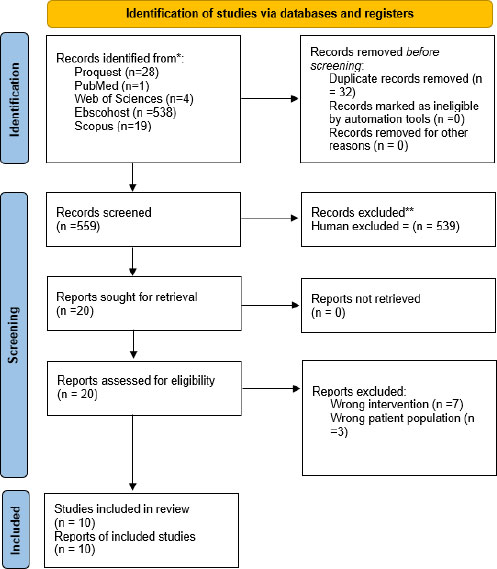
PRISMA flow diagram of the study selection.
3. RESULTS
The review included an initial search that identified 591 records, and Covidence identified 32 duplicates. A total of 559 articles were included in the abstract and title screening stage. After relevance screening, 539 records were excluded. Subsequently, 20 records qualified for full-text review, and 10 studies were excluded because they fell outside the study criteria for various reasons, including incorrect outcomes, interventions, study designs, populations, and studies published earlier than January 2014 or later than December 2024. Ten published studies were included in the data extraction, as they met the inclusion criteria for the analysis.
3.1. Study Characteristics
Most studies employed qualitative methods (interviews, focus groups, thematic analysis) [20-29], with two observational studies [21,22], one randomised controlled trial, and one [28] tool development study. Studies were conducted in LMICs (South Africa, Malawi, Mali, Namibia) and high-income countries (France, USA, Australia, Taiwan). Target populations included people living with HIV, people living with multimorbidity, healthcare workers, and community stakeholders. Several studies combined participatory features, such as patient feedback or consultative involvement; however, none fully implemented EBCD, although several reflected partial elements of patient engagement. Table 2 summarises the study's characteristics.
Three descriptive themes emerged: (1) Fragmented intervention development, with most studies addressing HIV or NCDs separately [20-29]; (2) Absence of full EBCD application, though partial engagement features were noted [20-23,25]; (3) Expert-driven designs with limited community-led input [20,21,24,25].
| Author(s) & Year | Study Title | Country | Aim | Study Design | Population | Key Findings | EBCD & Intervention Status |
|---|---|---|---|---|---|---|---|
| [20] | Patients' experiences of self-management and strategies for dealing with chronic conditions in rural Malawi | Malawi | To explore self-management practices and challenges in chronic care | Qualitative | Patients with chronic conditions | Barriers: poverty, limited disease knowledge, weak support systems | EBCD: No; Intervention: No |
| [21] | A rehabilitation model as a key to comprehensive care in the era of HIV as a chronic disease in South Africa | South Africa | To evaluate a rehabilitation model for HIV care | Qualitative | PLHIV, healthcare providers | Barriers: transport, finances; community-based rehab as enabler | EBCD: Yes; Intervention: Yes |
| [22] | Patients' perspective on how to improve the care of people with chronic conditions in France | France | To collect patient input on care improvement using citizen science | Qualitative | Adults with chronic conditions | Emphasis on communication, coordination, and reducing admin | EBCD: No; Intervention: No |
| [23] | Chronic patient as an intermittent partner for policy-makers in Mali | Mali | To explore patient participation in policy-making | Qualitative | Patients with HIV and diabetes, policy actors | Stronger support structures for HIV than for diabetes | EBCD: Yes; Intervention: No |
| [24] | GREAT study: A pragmatic randomized controlled trial of activation in PLHIV | USA | To assess the effectiveness of the activation intervention | Randomized Control Trial | PLHIV | Improved retention and adherence | EBCD: No; Intervention: Yes |
| [25] | Healthcare empowerment and HIV viral control... | USA | To explore the effect of empowerment on viral control | Qualitative | PLHIV | Empowerment improves adherence and viral suppression | EBCD: No; Intervention: Yes |
| [26] | Integration of NCDs, HIV/AIDS & mental health care through empowerment evaluation | South Africa | To explore service integration using empowerment evaluation | Mixed Methods | Chronically ill patients | Service integration improved outcomes | EBCD: Yes; Intervention: Yes |
| [27] | Strengthening Namibia’s health system through palliative care integration | Namibia | To integrate palliative care into the health system | Qualitative | Patients with chronic illness and providers | Improved end-of-life care despite resource issues | EBCD: No; Intervention: Yes |
| [28] | My Wellbeing Journal: A tool to improve care for older adults with multimorbidity | Australia | To develop a communication and goal-setting tool | Qualitative | Older adults with multimorbidity | Tool-enhanced provider-patient communication | EBCD: Yes; Intervention: Yes |
| [29] | Patient engagement and self-management across the care continuum | Taiwan | To explore patient engagement/self-management strategies | Mixed Methods | Chronic care patients | Self-management improved engagement & outcomes | EBCD: No; Intervention: No |
4.DISCUSSION
Recent evidence suggests that while patient involvement is increasing, structured co-design involving both patients and healthcare workers remains limited, especially in low- and middle-income settings [27]. This absence is noteworthy because the core of EBCD is not merely patient consultation but collaborative service development based on lived experiences. In a book chapter, three authors argued that there is evidence of patient engagement in the design or implementation phases; however, it occurred in silos, focusing either on HIV or NCDs independently. This segmented approach reflects the findings from the studies reviewed in the paper. Others emphasise that most integration efforts have been additive rather than transformative [29].
4.1. Summary of Key Findings
This systematic review found no evidence of integrated healthcare interventions for HIV and NCDs that fully utilised the EBCD methodology. While some studies incorporated elements of patient engagement, none demonstrated the bidirectional co-design processes central to EBCD. Most interventions were expert-driven and disease-specific, reflecting fragmented interventions directed to multimorbidity care [ 20-29]
4.2. Fragmented and Siloed Intervention Development
A prominent observation across the studies was the fragmented nature of interventions, where most targeted either HIV or NCDs separately, with no evidence of integrated service delivery models. For instance, Chetty and Hanass-Hancock (2016) [21] developed a rehabilitation model focusing on HIV care in South Africa, but there was no linkage with other chronic conditions. Similarly, Wilson et al. (2018) [25] and Carroll et al. (2019) [24] focused on patient empowerment within HIV services, yet their interventions did not integrate care for patients living with multiple conditions. This siloed approach contradicts global recommendations for integrated, person-centred care and reflects ongoing structural limitations in healthcare delivery systems.
4.3. Absence of Full EBCD Application
Although none of the reviewed studies explicitly adopted the full EBCD methodology, several reflected its principles, particularly in patient engagement. For example, Tran et al. (2019) [22] employed a citizen science approach to gather patient feedback on chronic care improvement in France, which aligns with EBCD’s emphasis on user experience. Lawless et al. (2024) [28] developed a communication and goal-setting tool for older adults using feedback loops between patients and clinicians. However, these initiatives lacked the bi-directional co-design processes between patients and staff that define authentic EBCD practices.
4.4. Expert-driven Designs with Limited Community-led Input
The majority of interventions were developed through expert consultation, often involving programme managers, clinicians, or researchers, but without meaningful co-creation with patients and healthcare providers. Studies such as those by Martini et al. [23] and Van Deventer [26] highlighted the role of institutional actors in shaping interventions, with minimal evidence of collaborative design with end-users. Even where patient involvement was evident, as in Angwenyi et al. [20], it was typically consultative rather than generative, limiting the intervention's sustainability and contextual relevance.
4.5. Comparison with Existing Evidence
Our findings align with global literature indicating that integrated care models often lack meaningful co-design, particularly in LMICs. WHO frameworks advocate for person-centred care, yet operationalisation remains limited [7,11,30,31]. Previous reviews confirm that integration efforts are frequently additive rather than transformative, focusing on service access rather than redesigning care delivery models [4, 32, 33]. Many African countries have introduced NCD services into HIV clinics without fundamentally restructuring care delivery [34,35]. This segmented approach aligns with our findings and underscores the need for participatory design methods, such as EBCD [36,37].
4.6. Implications for Integrated HIV and NCD Care
The absence of a full EBCD application suggests that current interventions may fail to capture patient experiences, cultural contexts, and practical challenges. Without participatory design, integrated care risks poor uptake, limited sustainability, and suboptimal health outcomes [38]. Embedding EBCD could improve patient ownership, enhance provider-patient trust, and increase the relevance of interventions, ultimately leading to improved health outcomes in resource-limited settings [4,11,39]
4.7. Methodological and Contextual Barriers
Several interrelated factors explain the lack of full EBCD implementation in integrated HIV and NCD care interventions:
4.8. Resource and Funding Constraints
In LMICs, limited financial resources and competing health priorities often restrict the adoption of participatory methodologies such as EBCD. Health systems in these settings prioritize essential service delivery and disease-specific programs, leaving little room for investment in co-design processes that require time, training, and facilitation [30,33]
4.9. Institutional Barriers
Existing health systems in LMICs are characterized by vertical programming and fragmented service delivery models. These structural challenges hinder the integration of HIV and NCD care and create operational silos that make collaborative design difficult [11,13,26]. Institutional cultures often prioritize top-down decision-making, where interventions are designed by policymakers and program managers without meaningful engagement of patients and frontline providers. This lack of organizational readiness for participatory approaches perpetuates the gap between policy aspirations and practical implementation.
4.10. Limited Researcher Capacity and Training
EBCD requires specialized skills in qualitative research, facilitation, and stakeholder engagement. Many researchers and health professionals in LMICs lack formal training in participatory methods, which limits their ability to implement EBCD effectively [4,10]. Additionally, academic and funding structures often emphasize traditional research designs and quantitative outcomes, discouraging investment in co-design methodologies that prioritize experiential knowledge [28, 29].
These barriers collectively highlight the need for capacity-building initiatives, institutional reforms, and dedicated funding to support participatory approaches [1,8]. Embedding EBCD within health system strengthening strategies could enhance the contextual relevance, acceptability, and sustainability of integrated HIV and NCD interventions [ 9,28]. Policy frameworks should mandate stakeholder engagement as a core component of intervention design, and research agendas must prioritize training and resources for participatory methodologies [12, 27, 29].
4.11. Recommendations for Future Research
The findings suggest that future research should adopt EBCD as a guiding principle for intervention design to enhance the success of integrated care interventions. Interventions developed through EBCD can improve patient engagement and promote better healthcare outcomes, particularly in PHC settings. Public health practitioners and researchers must prioritize integrated interventions informed by participatory approaches to tackle the dual burden of HIV and NCDs and improve health outcomes in under-resourced environments. This review demonstrates that despite the increasing need for integrated HIV and NCD interventions, full implementation of Experience-Based Co-Design remains rare. Future studies should embed EBCD principles across all stages of intervention development to ensure contextual relevance, sustainability, and patient ownership.
4.12. Public Health Implications
The findings of this review have important public health implications, particularly in resource-limited settings where primary healthcare is the first point of contact for individuals with comorbid HIV and NCDs. One significant observation from the review is the fragmentation of interventions targeting these conditions, with most studies developing solo interventions for either HIV or NCDs. There is a clear need for integrated healthcare interventions that simultaneously address both conditions. This is consistent with current global health frameworks, which emphasize the importance of integrated, patient-centred care in improving outcomes [ 30]. The lack of a full EBCD methodology in the reviewed studies limits the ability to develop comprehensive, sustainable interventions. Research shows that EBCD, which involves collaboration between patients and healthcare workers, ensures more context-sensitive and accepted interventions [30].
4.13. Strengths
This systematic review demonstrates several strengths in its methodology, study characteristics, findings, and public health implications. The choice of methodology, utilizing both the PICOT and SPIDER frameworks, provided a robust structure for addressing the review questions. These frameworks allowed for a comprehensive exploration of both qualitative and quantitative studies, ensuring a thorough examination of integrated healthcare interventions for individuals with comorbid HIV and NCDs. The diverse range of studies included qualitative, quantitative, mixed-methods, and randomized controlled trials, adding depth to the findings and highlighting not only the types of interventions developed but also the patient engagement approaches used across different settings. This methodological rigor ensured that the review captured the most relevant and recent evidence from 2014 to 2024.
The findings identify the lack of fully integrated interventions and the absence of a true EBCD approach, a gap that was explored in the discussion. The discussion effectively connected the study findings to the broader literature, emphasizing the importance of adopting participatory design principles in future interventions. Finally, the public health implications highlight the need for integrated care interventions that address both HIV and NCDs simultaneously, with a particular emphasis on patient-centred design. The review advocates for the implementation of EBCD to improve healthcare outcomes, particularly in primary healthcare settings in resource-limited environments. Lastly, the review’s methodological rigor, comprehensive study selection, and thought-provoking discussion make a significant contribution to the understanding of integrated care interventions.
5. LIMITATIONS
This systematic review has several limitations that should be considered when interpreting the findings. One significant limitation is the lack of studies that have used the EBCD approach in the development of integrated care interventions for individuals with comorbid HIV and NCDs. Although the review aimed to identify studies using EBCD, few of the included studies exclusively employed this approach, and only a few reflected elements of health care providers and patient engagement. This limitation may indicate a gap in the literature, suggesting that the EBCD approach has not yet been widely adopted in the context of integrated care for HIV and NCDs. Additionally, the review focused on studies published in English, which may have excluded valuable research published in other languages. Studies from non-English-speaking countries could have offered diverse perspectives and interventions that might have enhanced the review’s findings. Another limitation is the inclusion of studies from a relatively short time frame (2014–2024). While this ensured that the review was up to date, it may have excluded older studies that could have contributed valuable insights.
Furthermore, the exclusion of grey literature and unpublished studies may have resulted in publication bias, as studies with negative or inconclusive results are less likely to be published. This bias could skew the findings toward interventions perceived as successful. In addition, the inclusion of diverse study designs, including qualitative, quantitative, mixed-methods, and randomized controlled trials, while enriching the review, introduces heterogeneity in methodologies, outcomes, and contexts. This variability limits direct comparability and may affect the synthesis of findings. Recognizing these factors is essential for interpreting the results cautiously and underscores the need for future systematic reviews to incorporate strategies for minimizing bias and addressing heterogeneity.
These limitations highlight the need for further research that explores the use of EBCD in integrated care interventions, including studies from diverse linguistic and cultural contexts, broader time frames, and grey literature sources.
CONCLUSION
This systematic review highlights several strengths in its study characteristics, findings, and public health implications, specifically in relation to integrated healthcare interventions for people living with HIV and NCDs. While interventions exist, they are often fragmented, targeting either HIV or NCDs independently, and none have fully implemented the EBCD methodology. Limited patient engagement and reliance on expert-driven designs highlight the need for a paradigm shift toward participatory approaches.
To improve care integration and sustainability, future interventions must adopt EBCD as a guiding principle, ensuring collaborative design between patients and healthcare providers. Embedding EBCD into integrated HIV–NCD care models can enhance contextual relevance, patient ownership, and health outcomes, particularly in resource-limited primary healthcare settings. This review strongly advocates for policy frameworks and research agendas that prioritize EBCD-driven strategies as essential for addressing the dual burden of HIV and NCDs and achieving person-centred, equitable care.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows N.S.M.M, S.J.N, L.A..S, L.M, S.H.M. and N.V.S.: Study conception and design; N.S..M.M, L.M. and L.A.S.: Data collection; N.S.M.M., S.J.N. and S.H.M.: Analysis and interpretation of results; N.S.M.M, N.V.S.: Draft manuscript; N.S.M.M, S.J.N., L.M., L.A.S., S.H.M. and N.V.S.: Reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| HIV | = Human Immunodeficiency Virus |
| NCDs | = Non-Communicable Diseases |
| EBCD | = Experience-Based Co-Design |
| LMICs | = Low- and Middle-Income Countries |
| WHO | = World Health Organization |
| PICOT | = Population, Intervention, Comparison, Outcome, Time |
| PICO | = Population, Intervention, Comparison, Outcome |
| SPIDER | = Sample, Phenomenon of Interest, Design, Evaluation, Research type |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PHC | = Primary Health Care |
| PLHIV | = People Living with HIV |
| PAR | = Participatory Action Research |
| CASP | = Critical Appraisal Skills Programme |
| USA | = United States of America |
| HIV/AIDS | = Human Immunodeficiency Virus / Acquired Immunodeficiency Syndrome |
| RCT | = Randomised Controlled trial |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
We are indebted to the University of Pretoria Faculty of Health Sciences, School of Health Care Sciences, Department of Nursing Sciences, for providing this opportunity to conduct research, Prof RSM. Dr. N.S. is grateful for the contributions and insights of Dr. SJN, Prof LM, Prof NV, Prof LAS, and Dr. SHM. This article is partially based on Dr. N.S.’s research development project entitled ‘Co-designing a patient-centred integrated care intervention to enhance multimorbidity management in primary health care settings: an experience-based co-design study in Limpopo province, South Africa’. The project is ongoing at the time of publication.

