All published articles of this journal are available on ScienceDirect.

The Effect of Additional Childcare Roles on COVID-19 Symptom Knowledge Among Youth in South Africa
Abstract
Background:
As of March 2020, young people performed additional household responsibilities due to COVID-19 in South Africa. In particular, youth assisted with childcare since schools were closed. However, little is known of the impact of changing roles and additional responsibilities on young people’s ability to keep abreast of important information regarding the spread of the virus.
Objective:
The aim of the study was to determine the relationship between additional childcare responsibilities and complete awareness of the knowledge of symptoms of COVID-19 among young people in South Africa.
Methods:
Using data from the South African National Income Dynamics CRAM Survey (wave 1), 710 (72.08%) young individuals (18-24 years old) who listed symptoms of COVID-19 were analysed. The study controlled for covariates as additional childcare responsibilities, demographic and socioeconomic characteristics of the respondents. Cross-tabulations and a binary logistic regression model were used to determine the relationship between covariates and the outcome of the knowledge of symptoms.
Results:
None of the respondents reported 100% knowledge of the symptoms of COVID-19 while 57.5% reported having additional childcare responsibilities. Among youth with additional childcare, 90.71% knew regarding approximately half (50%) of the symptoms. Finally, not having additional childcare roles increased the odds of knowing at least three symptoms of the coronavirus (OR= 2.36; CI: 1.227387 - 2.543323).
Conclusion:
Youth, especially those spending increasing time caring for children, need more access to information regarding the virus. This information is key to protecting themselves and the children in their care.
1. INTRODUCTION
In early 2020, the COVID-19 had spread to nearly every country in the world. The global pandemic has resulted in more than three million deaths and over 167 million infected cases worldwide [1]. The virus is transmitted among people in close contact with each other and via droplets containing the virus that are inhaled or come directly into contact with the eyes, nose, or mouth [2], making it very difficult to prevent transmission between individuals. However, the World Health Organisation (WHO), working with other research groups, soon identified and recommended key preventive measures to contain the virus, including social distancing, washing hands regularly using soap, and wearing a face mask [3]. In addition, when patients with COVID-19 started presenting with the disease, a list of more common symptoms was made public, which included fever, dry cough and tiredness, among other less common symptoms [3]. Governments across the world have made concerted efforts to ensure that both the preventative measures and symptoms were communicated widely to curb the spread of infection.
In South Africa, mass media campaigns were introduced to inform the public of the possible symptoms and to increase testing for the virus [4]. These campaigns, along with the work by healthcare officials, resulted in the country being able to moderately manage infection and mortality rates [4]. However, the virus has placed significant strain on the healthcare system, with hospitals reportedly running out of personal protective equipment (PPE), beds and oxygen for infected patients [5]. This shows the many difficulties the healthcare sector in South Africa is faced with, but it also suggests that mass communication messages and regulation regarding prevention and symptom monitoring have not been completely successful. South Africa is not alone in the struggle to communicate COVID-19 symptom knowledge; a study in Iran showed low levels of the knowledge of the disease, and an early study of healthcare workers in March 2021 found 61% to have poor knowledge of transmission of the disease.
In addition to the challenges associated with the healthcare system in South Africa, COVID-19 regulations, especially the ‘lockdown’ which prohibited the movement of individuals for non-essential purposes, disrupted the daily lives of everyone in the country [6, 7]. The ‘hard lockdown’, levels 5 and 4, under which the strictest protocols were observed, including the prohibited sale of alcohol and cigarettes, the closure of retail centres and shopping malls, and the suspension of contact teaching in schools, lasted from March to May 2020 [8]. During this time, unemployment, intimate partner violence as well as mental and emotional stress increased [9]. In fact, one study has shown that adults who lost employment due to the lockdown in South Africa had higher rates of depression than those who were employed [9]. Further, with schools being closed, many parents and caregivers struggled with the demands of working from home or unemployment while providing childcare [10]. However, parents and caregivers alone, including grandparents, were not affected by school closures. Young people also performed roles of additional childcare for younger siblings and relatives [11]. Research has shown that lower-income families and those with special needs were the most affected [11]. These young people also had education and employment disrupted by the virus with subsequent lockdown and additional roles within households; this must have potentially affected their ability to learn and adhere to safety protocols.
The purpose of this study was, thus, (1) to estimate the levels of knowledge of COVID-19 symptoms among young people in South Africa, and (2) to determine the relationship between additional childcare roles during the lockdown and the knowledge of the disease symptoms.
2. MATERIALS AND METHODS
2.1. Data
This study made use of data from the National Income Dynamics Study - Coronavirus Rapid Mobile Survey 2020 (NIDS- CRAM). The survey explores the social and economic consequences of the global coronavirus pandemic in South Africa. NIDS-CRAM is part of a broader study called the Coronavirus Rapid Mobile Survey (CRAM). The data for this study comes from the first wave of data collection spanning from May to June 2020 [12]. The data have been made freely available for research purposes at https://www.datafirst.uct. ac.za/dataportal/index.php/catalog/817.
2.2. Sample Size
The study included 985 (n) young individuals 18-24 years old. Of these, 710 (72.08%) responded to questions regarding the knowledge of COVID-19 symptoms.
2.3. Study Variables
This study involved the assessment of the ‘knowledge of COVID-19 symptoms’. The survey asked respondents to list up to eight symptoms of COVID-19. The list of symptoms was not predetermined and enumerators filled in the responses given by participants. Using the WHO’s information website [3], Table 1 shows the symptoms that were used in this study to measure the knowledge of the youth respondents regarding the Covid-19 symptoms. These responses have been ranked in the order of the most commonly-known symptom to the least-known. The percentage per known symptom has been generated.
In the analysis of this study, we enumerated these symptoms known by the respondents as a percentage variable.
The key independent variable in this study was ‘additional childcare’. Survey respondents were asked “in April, did you personally spend more time than usual looking after the kids?”. This question was asked due to schools being closed and youth having to spend more time than usual taking care of siblings and other children in the household. This variable involved binary (yes/no) responses.
Control variables used for the study included the age group (18-24 years old), sex (male and female), race (African, White, Coloured, Indian/Asian), the highest level of education, type of dwelling (house/flat, traditional house like mud hut or informal house like a shack or other), number of resident household members (with the mean number being six members), employment status measured by the survey question “any paid activity/ job to return to at the end of April”1 living in a household receiving any government grant (yes/no) and COVID-19 behavioural change (yes/no).
| Symptoms | Rank | Frequency | Percentage |
|---|---|---|---|
| Cough | 1 | 350 | 62.50 |
| Fever* | 2 | 301 | 53.75 |
| Sore throat | 3 | 141 | 25.18 |
| Difficulty breathing | 4 | 134 | 23.93 |
| Headache | 5 | 62 | 11.07 |
| Dry cough* | 6 | 59 | 10.54 |
| Tiredness* | 7 | 57 | 10.18 |
| Loss of taste or smell | 8 | 18 | 3.21 |
| Total | 560 | 100.00 |
2.4. Analysis Plan
Descriptive statistics was used to show the distribution of participants’ characteristics according to the knowledge of COVID-19 symptoms. Cross tabulations of the percentages of identified COVID-19 symptoms (none or 0%; 1-50% and 51%- 87.5%) with the characteristics of the respondents show the accuracy of knowledge among youth. A binary logistic regression model, with the outcome modified into the knowledge of 0-3 symptoms (0) and 4-8 symptoms (1), was used to identify the likelihood of knowledge by respondents’ characteristics.
3. RESULTS
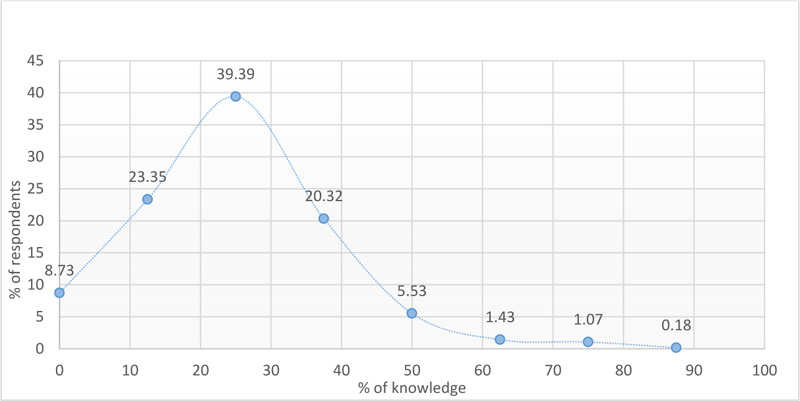
Fig. (1) shows that 39.39% of the young people had only 25% knowledge of symptoms, that is knowing approximately 2 symptoms. Less than 1% (0.18%) of the young people were able to mention upto 87.25% of the symptoms. None of the young people had complete knowledge of the eight symptoms of coronavirus, while 8.73% of the young people did not know regarding any of the symptoms.
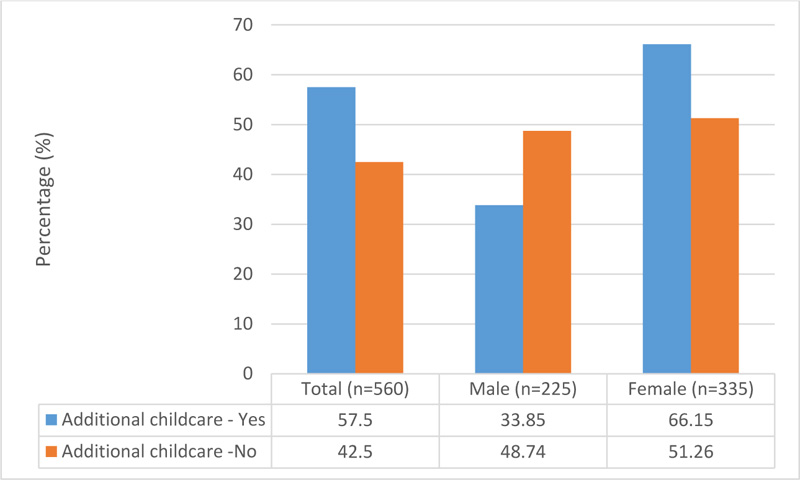
Fig. (2) shows that 57.5% of young people performed extra duties of childcare during the lockdown while 42.5% did not engage in any additional childcare activities. Females (66.15%) were more reported with additional childcare roles compared to males (33.85%).
The distribution of the knowledge of respondents regarding coronavirus symptoms with respect to their characteristics is shown in Table 2. Overall, only 2.39% of young people were found to know over 50% of the symptoms. The majority of young people (89.15%) were aware of less than half (1%-50%) of the symptoms of COVID-19. Just over 4% of young people without additional childcare roles knew more than 50% of the symptoms of the virus, compared to 1.55% those with additional childcare responsibilities. In addition, females (2.43%), whites (12.45%), those living in traditional houses (3.45%), and those having secondary education (2.45%) and living in a household while not receiving a government grant (2.39%) had knowledge of more than half of the symptoms.
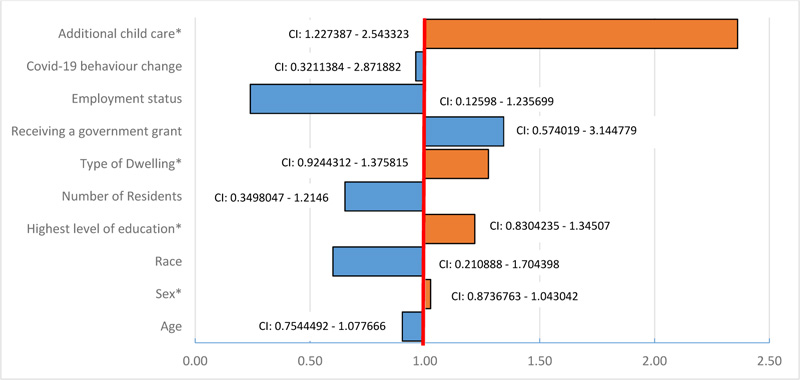
Fig. (3) displays the result of the logistic regression model showing the odds of young people’s knowledge of COVID-19 symptoms with respect to their demographic and socioeconomic characteristics. Among the selected characteristics, additional childcare roles, sex, level of education and type of residential house were the significant factors that affected the awareness of the virus’ symptoms. Further, the result shows that not having additional childcare roles increases the odds of knowing more than three symptoms of coronavirus (OR= 2.36; CI: 1.227387 - 2.543323). Females are likely to know more than three symptoms of the virus (OR=1.03, CI: 0.8736763 - 1.043042) compared to their male (OR = 1.00 or even odds) counterparts. In addition, having at least primary education (OR=1.22; CI: 0.8304235 - 1.34507) and not living in a flat (OR=1.26; CI: 0.9244312 - 1.375815) increases the likelihood of knowing more than three symptoms of COVID-19.
Table 2.
| Respondent Characteristics | None | 1%-50% | 51%-87.5% | Total | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | |
| Total | 60 | 8.45 | 633 | 89.15 | 17 | 2.39 | 710 |
| Age* | |||||||
| 18 | 3 | 14.29 | 18 | 85.71 | 0 | 0.00 | 21 |
| 19 | 14 | 12.17 | 97 | 84.35 | 4 | 3.48 | 115 |
| 20 | 6 | 5.22 | 106 | 92.17 | 3 | 2.61 | 115 |
| 21 | 12 | 9.68 | 110 | 88.71 | 2 | 1.61 | 124 |
| 22 | 8 | 6.67 | 109 | 90.83 | 3 | 2.50 | 120 |
| 23 | 13 | 11.71 | 93 | 83.78 | 5 | 4.50 | 111 |
| 24 | 4 | 3.85 | 100 | 96.15 | 0 | 0.00 | 104 |
| Sex* | |||||||
| Male | 34 | 11.45 | 256 | 86.20 | 7 | 2.36 | 297 |
| Female | 26 | 6.31 | 376 | 91.26 | 10 | 2.43 | 412 |
| Race* | |||||||
| African | 57 | 8.64 | 550 | 83.33 | 53 | 8.03 | 660 |
| White | 0 | 37.50 | 7 | 87.50 | 1 | 12.50 | 8 |
| Coloured | 3 | 0.00 | 32 | 88.89 | 1 | 2.78 | 36 |
| Asian/Indian | 0 | 0.00 | 6 | 100.00 | 0 | 0.00 | 6 |
| Highest level of education obtained* | |||||||
| None | 0 | 0.00 | 2 | 100.00 | 0 | 0.00 | 2 |
| Primary | 3 | 25.00 | 9 | 75.00 | 0 | 0.00 | 12 |
| Secondary | 57 | 8.23 | 619 | 89.32 | 17 | 2.45 | 693 |
| Tertiary | 0 | 0.00 | 3 | 100.00 | 0 | 0.00 | 3 |
| Type of dwelling* | |||||||
| House/flat | 43 | 7.60 | 509 | 89.93 | 14 | 2.47 | 566 |
| Traditional house, like a mud hut | 13 | 14.94 | 71 | 81.61 | 3 | 3.45 | 87 |
| Informal house, like a shack | 4 | 7.41 | 50 | 92.59 | 0 | 0.00 | 54 |
| Other | 0 | 0.00 | 3 | 100.00 | 0 | 0.00 | 3 |
| Number of residents in dwelling* | |||||||
| 0-5 | 24 | 6.76 | 322 | 90.70 | 9 | 2.54 | 355 |
| 6 and more | 36 | 10.14 | 311 | 87.61 | 8 | 2.25 | 355 |
| Receiving a government grant?* | |||||||
| Yes | 5 | 4.07 | 115 | 93.50 | 3 | 2.44 | 123 |
| No | 55 | 9.37 | 518 | 88.25 | 14 | 2.39 | 587 |
| Employment status* | |||||||
| Employed | 2 | 5.26 | 35 | 92.11 | 1 | 2.63 | 38 |
| Unemployed | 58 | 8.63 | 598 | 88.99 | 16 | 2.38 | 672 |
| COVID-19 behavioural change* | |||||||
| Yes | 51 | 7.85 | 583 | 89.69 | 16 | 2.46 | 650 |
| No | 9 | 15.00 | 50 | 83.33 | 1 | 1.67 | 60 |
| Additional childcare* | |||||||
| Yes | 25 | 7.74 | 293 | 90.71 | 5 | 1.55 | 323 |
| No | 24 | 10.08 | 204 | 85.71 | 10 | 4.20 | 238 |
| No children in household | 11 | 7.38 | 136 | 91.28 | 2 | 1.34 | 149 |
4. DISCUSSION
The aim of this study was to investigate the relationship between additional childcare roles inthe COVID-19 lockdown and knowledge of the symptoms of the virus among young people in South Africa. It is likely that the virus will remain with populations for years to come, resulting in fluctuating periods and intensities of lockdowns, whereby children will be confined to their homes due to closing of schools and day-care centres for varying periods of time. For this reason, there is a need to reliably and continuously address the social and economic consequences of such lifestyle changes as a result of the pandemic. This study, which has identified a relationship between additional childcare roles and the reduced knowledge of the symptoms of the virus, adds to a growing number of studies aimed at addressing the various impacts of COVID-19 on the lives of young people.
The results of this study indicate that youth without additional childcare responsibilities during the lockdown in South Africa are more likely to have the knowledge of more than three symptoms of COVID-19. This finding is similar to a study done in India, where it was found that caregiver knowledge of symptoms of the virus was lower than non-caregivers; however, the study in India did not focus on young people exclusively [14]. In general, caregivers have suffered higher levels of fatigue, anxiety and stress in the pandemic [15]. This mental and emotional stress could understandably affect their ability to focus on and learn the symptoms of the virus. This result is particularly concerning since most (more than 50%) of the youth in the study had additional childcare responsibilities.
In South Africa, 19.2% of the population involves children under the age of nine [16]. Youth, who are 18-24 years old, predominantly reside in households with at least one parent (26.7%), grandparent (17.52%), or are parents to young children (5.46%) themselves [17]. Results of this study show that more than half of the youth in the survey spent more time than usual caring for children in the household. This was undoubtedly a result of schools being closed during the lockdown. But this also suggests that the added responsibilities and time spent caring for children compromised young people’s abilities to gain knowledge of the most common symptoms of the virus, among other factors. In addition, these concerns were highlighted in a study on youth (15-25 years old) who presented concerns regarding food security and having children in the household to feed while being unemployed, as well as having feelings of bleakness, uncertainty and nervousness over future education and employment prospects in the country during the pandemic [18]. In the current study, the majority of young people had a secondary education but most were unemployed. It is, therefore, possible that youth caring for children during the lockdown may also have been struggling to find employment due to the economic environment and the added household responsibilities.
No young respondent in the study had 100% knowledge of the symptoms of COVID-19. This is concerning as none of the respondents listed all eight common symptoms. The results instead show that most respondents had knowledge of only a quarter (25%) of the symptoms. These numbers are low compared to a study done on young people in Kenya that showed over 90% of youth to have knowledge of all the most common symptoms of the virus [19]. In South Africa, the low knowledge of symptoms among young people is not completely unexpected, as a recent study of the population done online showed that only 83% of participants could correctly identify the main symptoms of the virus [20]. This may be due to misinformation and ‘myths’ spread socially about the disease and through various forms of media [21, 22], and the general public’s mistrust in the national government [23]. The consequences of the spread of misinformation and mistrust are not only incomplete knowledge of the symptoms of the virus but also inaccurate knowledge. The latter was found in an analysis of Twitter feeds in South Africa, where messages about conspiracies and the role of ‘5g’ were found to be trending throughout the country [24]. Without complete and accurate information about the symptoms of the disease, efforts to protect against and prevent the spread of the virus are severely challenging.
There are several strengths of this study. First, the data are recent and capture the most contemporary challenges of the South African population during the early stages of the pandemic. This is useful as the results highlight the most recent experiences and the knowledge of the population during the country’s COVID-19 lockdown. Second, the study has found an association between additional childcare responsibilities and reduced knowledge of COVID-19 symptoms. This proves that country is undergoing substantial social change due to the pandemic. Policymakers and social development program initiators need to be aware of this in order to adjust and create policies accordingly in the future. Third, while the sample of the study is small, it is still nationally representative and includes a diverse number of young people across the country.
There are a few limitations to this study. First, this study does not investigate whether the increased or decreased knowledge of COVID-19 symptoms translates into behavioural changes. However, levels of stress and depression have been reported among children and youth due to the pandemic [15], leading to behavioural changes in this difficult time. That is, knowing regarding the symptoms is not sufficient; there needs to be consistent testing of change in behaviour when symptoms occur among the population. Second, the data are cross-sectional; therefore, it cannot be determined if the additional childcare roles are the cause of the decreased probability of symptom knowledge among the youth in the country. Third, the study does not measure the amount of additional time young people are spending on childcare in the pandemic. This study would improve our knowledge regarding the extent to which additional childcare disrupts lifestyle, learning, education and employment for young people. Finally, the data for the NIDS CRAM Wave 5 were collected telephonically, which might have been subjected to connection issues and non-responsiveness of participants, both in answering the calls and being busy or distracted during the interview. Also, not everyone in the sampled household was interviewed; thus, the analysis for this study is restricted to individual-level interpretation. A complete household survey would have provided more information about the collective knowledge and represented the shared experiences of the households.
CONCLUSION
The COVID-19 pandemic has altered the roles of youth, with many taking on additional childcare responsibilities. This has resulted in an increased probability of young people having limited knowledge of the symptoms of the virus. Knowledge of the symptoms of the virus will prove to be beneficial for youth and the children in their care as it will enable young people to teach children the symptoms, thereby ensuring their prevention from the virus and disseminating care throughout households and communities.
A few recommendations can be made following this study. First, there should be more and better channels of knowledge dissemination to youth in South Africa. Efforts to increase the propagation of accurate information through media and social media are needed. Second, there is a need to investigate how young individuals are spending their time during the Covid-19 pandemic. With this information, youth who are spending more hours or days caring for children can be assisted with gaining symptom information, as well as other social and economic activities. Finally, a study which interrogates sources of information of youth would be beneficial for understanding the origins of inaccurate and incomplete information.
NOTES
In South Africa, the ‘hard lockdown’ in April suspended all non-essential services and employment activities. Approximately 46,4% of the population indicated temporary closure or paused trading activity during this time 13. Statistics SA, Business impact survey of the COVID-19 pandemic in South Africa, in Report-00-08-01, S.S. Africa, Editor. 2020, Statistics South Africa: Pretoria, South Africa.
ETHICAL STATEMENT
The study uses fully anonymised secondary data from the South African National Income Dynamics CRAM Survey, which is free to download online at https://cramsurvey.org/
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this article are available within the article.
FUNDING
This study was funded by the DST-NRF Centre of Excellence in Human Development.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors are thankful to the DST-NRF Centre of Excellence in Human Development for their support.

