All published articles of this journal are available on ScienceDirect.

Development of an Information System to Support Occupational Therapy Services from Hospital to Community
Authors Info & Affiliations
Abstract
Background:
Information systems for occupational therapy (OT) services need to adapt effectively for improving performance by taking advantage of digital technology.
Objective:
This research aimed to develop an information system for supporting occupational therapy services in the community.
Methods:
This study used a mixed methods research design divided into two phases. Phase I: system requirements were gathered from nine occupational therapists who represented each of the nine provinces in northern Thailand. Focus groups and in-depth interviews were used in detail to explore the system requirements for occupational therapy services in the community. This information system applied a responsive web design. Phase II: usability testing, involved thirty occupational therapists in a northern network, who were selected to evaluate an information system by using a questionnaire.
Results:
Results showed that participants requested two components: 1) Occupational Therapist data, and 2) a referral system. The information system could be used by occupational therapists in a northern Thai OT network to insert their own information actively for providing a referral system. The overall usability assessment was at a high level (mean ± SD = 4.27 ± 0.07).
Conclusion:
This study concluded that an OT digital network system may offer a strategy to support OT services from hospital to community in a complex system of healthcare.
1. INTRODUCTION
Changes in Thai government policy have transferred various public health functions to local governments [1]. Thus, health service delivery has been organized as a multi-level system of working together in a holistic network. Primary healthcare in Thai communities has a complex infrastructure [2]. Its performance in hospitals promoting sub-district healthcare in Thailand still needs to improve a comprehensive healthcare service with easy accessibility [3, 4]. Primary care provides the opportunity to increase the potential of the profession [5], which is very challenging in the context of community mobility [6]. Occupational Therapy (OT) practitioners are care managers, who play an important role in community hospitals in Thailand [7]. They evaluate the ability of patients on their return to community life, which may require technology, facilities, and environmental modification as well as the follow-up, home visits, and coordination with primary healthcare services [8, 9]. The transition service for clients is a part of the OT process in providing programs focused on independent living skills [10, 11]. Home visits by occupational therapists focus on the ability of clients to manage daily activities directly in their home environment at the family and community level [12, 13]. Furthermore, occupational therapists also provide assistive technology (AT) to help clients achieve more independence or comfort when performing daily activities [14, 15].
Technology and innovation are growing rapidly in healthcare, and the challenge is whether they can help physicians to work better than ever before [16-18]. The Ministry of Public Health (MoPH) of Thailand [19] has driven the digital health system to encourage the healthcare sector by using the eHealth Strategy as a framework. Health information technology refers to the use of various electronic methods for managing information when providing public healthcare services [20]. For instance, the World Health Organization [21] focuses on the health information that is used for decision-making at various levels of the healthcare system. Information at different levels (provincial, district, sub-district, and community) can provide better coordination and a cross-sectorial approach to primary healthcare in community-based OT services. Thus, a coordinated OT intervention plan can create a unique service throughout the transition from hospital to community and help clients to increase independence in daily life activities, which are necessary for community integration. Health Informatics for the OT Community-based Service was developed for children from birth to 6 years of age [7]. However, this health information program was developed for use by occupational therapists who work with such children in local communities. It is essential for the system to transfer information and bring data on health to all services in order to reach maximum benefit and better cooperation that covers the whole picture. Therefore, this study aimed to provide data on the specifications of system requirements for a web-based design and usability testing in developing a web information system that networks OT in Thailand for clients who are returning to the community, with the goal of living successfully.
2. MATERIALS AND METHODS
This study focused on covering northern Thailand with public health zone 1, which covers its upper and lower regions with three types of facilities (provincial, district, sub-district, and community), containing a good combination of types. The study was divided into 2 phases by using a mixed-method research methodology. Ethics approval was obtained by the Faculty of Associated Medical Sciences, Chiang Mai University.
Phase I: system requirement for a proposed information system was investigated with focus groups and in-depth interviews. Focus group sessions were designed by reviewing related literature [22]. A sensibly sized system requirement group (N=9) was formed to capture different perspectives to cover health zone 1. Nine participants, who were heads of OT services from each of the nine provinces in northern Thailand, were selected purposively. The purposeful recruiting criteria included being an occupational therapist and residing in northern Thailand for at least the past 5 years, and being able to participate in ongoing research throughout the project. All of the participants were asked for their informed consent, and they signed the consent form. Two focus group sessions were held at the Faculty of Associated Medical Sciences, Chiang Mai University, on June 28 and December 13 (8:30 a.m. to 11:30 a.m. and 1:00 p.m. to 4:00 p.m., 2018, respectively). A semi-structured guideline, which included various questions on OT discharge planning, was used by the focus group for clients transferred from the hospital to the community. This achieved more successful transition and information required for OT services at the hospital and community during transitional periods. The main question on the information given in this system included a discussion on “what information occupational therapists need to communicate with each other in order to link the OT service between hospital and community”. The researcher, who had more than 5 years experience in conducting focus groups and in-depth interviews, was a moderator in the focus group session and conductor of individual in-depth interviews with questions probing for more information on interesting issues. The focus group sessions and in-depth interviews were recorded by a voice recording device, once permission had been obtained from the participants, and the contents were transcribed verbatim. A thematic analysis was then conducted [23]. Themes were then reviewed to check those that could be compatible with both the coded extracts and the whole dataset from the focus group in order to generate a thematic map. Validity of contents was established by using various methods; member checking (e.g., directly asking questions to the participants during and after focus group sessions and summarizing at the end of them). The thoughts of the focus group members about the content and function of the web-based program design were expected outcomes. The researcher drafted the paper-based content from the thematic analysis. The system programming of the web-based program was produced by software engineers. The second focus group aimed to test and edit its performance among nine participants, researchers, and software engineers.
Phase II: usability testing was conducted in order to obtain feedback on identified issues on the design from users in the northern OT network, which was conducted on January 25, 2019, at the Faculty of Associated Medical Sciences, Chiang Mai University. Thirty occupational therapists were selected by purposive sampling as participants to evaluate the information system and perform the testing. A trial session was demonstrated for 45 minutes, with its effectiveness assessed by a questionnaire. The researcher explained the features and functions of system programming and then demonstrated how to input the data from a one-case scenario and export it from the program. The questionnaire from Panyo [7] was used in the usability testing, based on subjective and comprehensive views of the system’s users. All of the items in the questionnaire were rated as 1 to 5 on the Likert scale (1-Not satisfactory, 2-Satisfactory, 3-Good, 4-Very good, 5-Excellent). The scoring of each item was interpreted into five levels [7]. Moreover, a discussion on how to use this OT network was provided to improve the service with more coherence from hospital to community and connect the network for 30 minutes.
3. RESULTS
3.1. Phase I: System Requirement
The participants comprised nine occupational therapists, whose type of facility was at the provincial level. The demographics of the OT participants are shown in Table 1. The results revealed that females were the majority of participants. OT work experience was between 8 and 24 years. The category of position was in the range of levels from low to high such as practitioner level (K1), professional level (K2), and senior professional Level (K3).
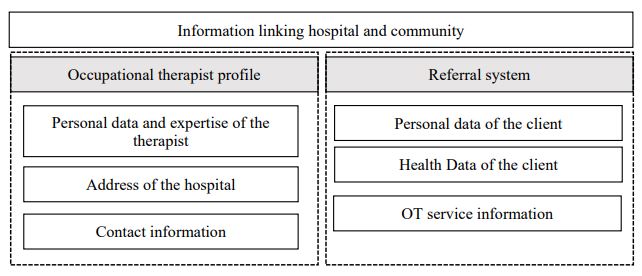
The features and functions of system programming were developed from the perspectives of the participants. There were two domains: occupational therapist profile and referral system. The details of each domain emerged from qualitative findings and illustrative examples of the participants as follows:
Occupational therapist profile: “OT profile in the information system is very important for successful transition. It should be included in personal data with expertise of the therapist.”
Referral system. “I have been provided OT service for discharge planning and sharing the OT goal, and a plan at the hospital can ensure a smooth transition for clients.”
A report was produced by synthesizing all of the themes identified in the content of system requirements, as shown in Fig. (1).
The referral system was designed for use among hospitals in this network, and OT users could bring client data into the system independently. Users had to choose the hospital in which they worked under the right granted by the administrator. Data privacy and a security process were protected by a password. Occupational therapists could click on the information required and add details of advice that might range from a specific prescription to general suggestions under aspects of the OT domain, including entry referring to OT at other levels (the primary–secondary care level) for discharge planning.
| Participants | Age, year | Experience in OT, years | Gender | Category of Position | Expertise |
|---|---|---|---|---|---|
| 1 | 44.67 | 23 | Female | Professional level (K2) | Pediatrics, Neurological rehabilitation, Hand & Splints |
| 2 | 33.25 | 11 | Female | Professional level (K2) | Pediatrics, Neurological rehabilitation, Hand & Splints |
| 3 | 40.75 | 19 | Male | Professional level (K2) | Pediatrics, Neurological rehabilitation, Hand & Splints, Community |
| 4 | 44.25 | 22 | Female | Professional level (K2) | Pediatrics, Neurological rehabilitation, Community |
| 5 | 29.50 | 8 | Female | Senior professional Level (K3) | Pediatrics, Neurological rehabilitation, Hand & Splints |
| 6 | 43.25 | 21 | Male | Practitioner level (K1) | Neurological rehabilitation, Hand & Splints |
| 7 | 40.42 | 18 | Female | Professional level (K2) | Pediatrics, Neurological rehabilitation, Hand & Splints |
| 8 | 46.42 | 24 | Female | Professional level (K2) | Pediatrics, Neurological rehabilitation, Hand & Splints |
| 9 | 40.42 | 16 | Female | Practitioner level (K1) | Pediatrics, Neurological rehabilitation, Hand & Splints |
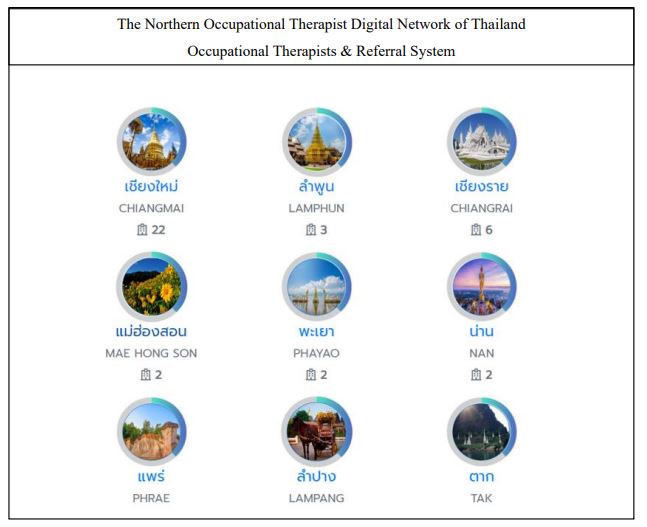
The Northern Occupational Therapist Digital (NOTD) network was designed as a web application that can be installed on a server for use with the system via the Internet. The development period totalled six months from June to November 2019. The main page (http://portal.localhealth.in. th/) shows that the network in the northern region comprises nine provinces (Fig. 2).
The head of the OT network (administrator) in each province provided information from occupational therapists who were responsible within the scope of general hospitals. In Thailand, general hospitals come under the jurisdiction of the Ministry of Public Health. The information system comprises lists of hospitals and occupational therapists. The information loop of the NOTD network links all data to the cloud system, as shown in Fig. (3). The following codes (P1, P2, ….and P9) are determined as a province code, for example, P1 represents Chiang Mai province, whereas sub-codes (P1.1,…P1.22) are determined as sub-level under Chiang Mai province. Users were classified into two groups: normal users and administrators.
The head of OT in a public hospital is an administrator at the tertiary care – level (Admin P1, Admin P2, … Admin P9), whereas normal users, who were OT practitioners, were at the provincial, district, sub-district, and community level (P1.1, P2.1…, P9.1). The occupational therapists were presented by separating the provincial networks that comprise the name of an administrator, from the lists of provincial hospital networks and occupational therapists.
All of the users (administrators as well as normal users) utilized the same form to log in, but normal users were not allowed to access admin pages. The login page allowed the user to access the system by entering their username and password. Occupational therapist profiles were provided in two parts: status of the user (administrator or normal user), and hospital and OT profile (name, expertise, position, and contact). The page of occupational therapist profiles opened into a new window when clicking on the provincial hospital network icon.

3.2. Phase II. Usability test of the Northern Occupational Therapist Digital Network of Thailand
This survey gave an insight into the use of the NOTD network by the user. The results indicated that overall satisfaction with use was at a good level (
After usability testing, the participants were asked their opinion of the effectiveness and usefulness of the NOTD network. They reported that this web-based program was a collaborative tool, which supported the provision of OT intervention for clients during transition periods.
4. DISCUSSION
The NOTD network of Thailand was developed in two parts of an information system: an occupational therapist profile in northern Thailand and a referral system for clients. This information system can support OT services among the complex healthcare services. However, system requirement was provided by representatives of each hospital in northern Thailand. The function of the system was developed from a personal perspective and experience. Thus, this system was tailored to a specific group.
The healthcare system in Thailand is based on primary healthcare and substantial delivery of services through the district health network at the provincial level. Development of the NOTD network of Thailand has provided great benefit to the OT network of the northern region, thus allowing a smoother process of relating clients at different levels of OT service to the Thai health system. The performance of primary healthcare in promoting sub-district hospitals in northern Thailand needs to improve in accessibility, comprehensiveness, and continuity [3]. Information and communication technology (ICT) has led to new advantages and challenges that provide and support a better quality of healthcare. Encryption for data protection is used for the OT network in order to protect privacy and security. Only authorized users with the proper corresponding keys can log in and access network information. Data encryption is one of the most effective security techniques that makes innovations possible [24]. The web application makes for easier access to communication with OT within the network, as well as OT profiles and referral data. The Thai health system has been reformed internationally for the sustainable development of quality services that contribute to health equity by functioning close-to-client primary healthcare [25]. It emphasizes developing a strong collaborative health network and providing service at the provincial level through districts and the community. According to a previous study [7], the development of health informatics cares for children in communities with an OT service provides many opportunities to make decisions on faster and easier intervention.
Technology has brought efficiency in providing access to and delivery of services in the local context. Thus, the development of this OT network can fill the gap in organizing comprehensive OT services. Hamm et al. [26], designed “guide to measure-OT”, which is a mobile 3D measurement guidance application that improves the falls-risk assessment process in the home environment. Moreover, this OT information system focuses on providing assistive technology (AT) services in the context of each client. AT is an important element of OT intervention, and it supports individuals, improves their performance, and increases their participation in activities [27]. AT has an impact on the performance of everyday activities. A management system of providing AT is the key to success in achieving the common goal of receiving AT and giving it directly to people for success in the community and district health system [28]. Thus, developing an information system can link the OT service to work from the provincial to the community level.
Usability testing of the NOTD network of Thailand showed that the system was easy to use, due to its simple and custom-made design. One of the most important aspects of the design was making the product usable for everyone [29, 30]. Occupational therapists form a group of users, who are unique and familiar with the technology. Therefore, they can access the database more easily. Panyo et al. [7] (2018) found that usability in the Health Informatics for Caring for Children in Occupational Therapy Service Communities was at a high level. In addition, observation proved that the system has more positive usability achievement across the OT network, which helped bridge the gap between the design and the user of the product. Despite an overall favourable opinion of the usability of this system, most of the users expected it to have more functionality by adding notifications to OT members in the network when other users put in new data, even though this function is not required for usability testing. This was a limitation of the design in meeting the needs of the users during usability testing. This finding relates to Lersilp et al. [31], who stated that users need more functions in the design during usability testing. Thus, this study on usability can provide new ideas and requirements that are challenging for researchers in improving this innovative product.
The limitations of this study revealed that the NOTD network was developed in the Thai health system context. However, further study might prove that the OT network can link information of OT discharge planning for more successful transitions from the hospital to the community. Moreover, using the system in the OT service is needed for evaluating usage and continuous improvement.
CONCLUSION
The NOTD network was developed in this study and comprised two parts, including the occupational therapist, and client and referral system. This digital network was developed to link the OT service from the provincial to the community level with the Thai health system. It was useful for building communication among occupational therapists in order to strengthen the service. This network system was divided into two kinds of users: administrators and normal users. Usability testing was found to be at a good level. Development of the OT network is a crucial step in ensuring that the users have the ability to access, understand and use this web application when delivering it via the internet. This OT network could be used as a model for other countries or localities. Most importantly, it will streamline the existing disorganized referral process in order to strengthen it by bridging the access gap between the hospital and community levels.
LIST OF ABBREVIATION
| OT | = Occupational Therapy |
AUTHORS CONTRIBUTIONS
Supawadee Putthinoi designed the research, analyzed the data, and developed the manuscript.
Suchitporn Lersilp designed the research and analyzed the data.
Napalai Chaimaha collected and analyzed the data.
Rujirek Chaiwongsab reviewed the literature and approved the manuscript.
Peerasak Lerttrakarnnon provided advice on the research design.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval for this project was obtained from the Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University (AMSEC-62EX-056).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans were used in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Potential participants were asked for informed consent.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available by the first author [S.P] upon request.
FUNDING
This study was funded by the Faculty of Associated Medical Sciences, Chiang Mai University Research Grant under grant no. 448.
CONFLICT OF INTERESTS
The authors report no conflicts of interest, and they agreed with the current content of the manuscript.
ACKNOWLEDGEMENTS
Declared none.

