All published articles of this journal are available on ScienceDirect.

Depression and Quality of Life among Women Hospitalized during COVID-19 Pandemic
Authors Info & Affiliations
Abstract
Introduction:
The outbreak of the new coronavirus (COVID-19) can lead to the development of several mental disorders. Women are an important part of any society, and psychological factors can affect their quality of life. The present study aimed to investigate the depression level among hospitalized women and its relationship with their quality of life during the COVID-19 pandemic in 2021.
Methods:
This descriptive-analytical study was conducted on 465 women admitted to public educational hospitals affiliated with the Minister of Health, Iran. The data collection tools were the Goldberg Depression Scale and the World Health Organization Quality of Life-BREF (WHOQOL-BREF) Questionnaire. Descriptive and inferential statistical methods were used to analyze the data by applying SPSS software version 23.
Results:
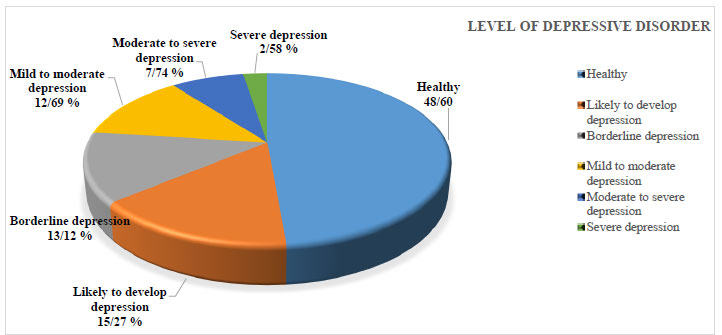
According to the results, 48.60% of the women were mentally healthy. While 15.27% of them were more likely to develop depression, 13.12% of the others were borderline depressed. At the same time, 12.69% of the women who participated in the study suffered from a mild to moderate level of depression, 7.74% of women had moderate to severe depression, and 2.58% of the rest tolerated severe depression. Other results show that the mean score of quality of life (QOL) of the women was 58.49±11.51 (out of 120). Moreover, a significant and inverse correlation between depression and QOL was observed among the studied women (r=-0.564, P<0.001). Statistically significant relationships between depression and the variables of age (P=0.007), place of residence (P=0.04), marital status (P=0.006), level of education (P<0.001), and income level (P=0.03) were also observed. Moreover, there was also a statistically significant relationship between women's QOL and their marital status (P=0.02).
Conclusion:
According to the results, providing social support and establishing effective communication based on mutual interaction among hospitalized women and healthcare workers can be recommended to decrease their level of depressive disorder and enhance their QOL.
1. INTRODUCTION
COVID-19 is an acute respiratory disease that is much more complex than previous coronavirus diseases. The reason behind this complexity is that COVID-19 is highly transmittable, and quite difficult to control and treat [1].
Coronaviruses are a large family of viruses that cause various illnesses, from the common cold to acute and severe respiratory syndromes [2]. In Iran, the first case of the disease was reported in Qom on February 19, 2020. From that point on, the virus spread rapidly to other parts of the country [3]. The COVID-19 pandemic still remains a serious and concerning threat to people's physical and mental health [4]. Recent studies have confirmed the high prevalence of mental disorders such as stress, anxiety, and depression in different communities following the COVID-19 crisis [5-7]. Mental illnesses resulting from the spread of this virus ranged from depression, mild anxiety, and stress to schizophrenia and complete insanity. Depression is the most common mental illness worldwide, with about 10% of people experiencing at least one period of depression yearly [8].
Depression is one of the most common mental disorders in human society that covers a wide range of emotional and mental states, from sadness and low self-esteem to emotional and physical disability. This disorder may be developed as a reaction to external events such as the death of loved ones, divorce, violence, and so on [9]. However, one may also develop depression for no apparent reason. In addition to hereditary and genetic aspects, depression is often associated with social and psychological factors caused by social events [10]. All of us are vulnerable to this disease, regardless of race, class, or social status [11]. A meta-analysis reported a 7-time increase in the prevalence of depression during COVID-19 [5]. Various studies identified factors affecting depression during the COVID-19 pandemic, such as age, gender, occupation, marital status, socio-economic level, level of education, exposure to stressors, history of chronic physical and mental illness, interaction with the media, and following news [5, 12-14].
Quality of life (QOL) is another psychological aspect of people's lives [15] that covers a wide range of one's life. This concept is highly influenced by one's physical and mental health, personal beliefs, and social relationships [16]. Research has shown that due to the contagious nature of COVID-19, its unknown mode of transmission, and people's fear of being affected by the virus, people's quality of life has been negatively affected by this virus [17-19]. In addition, mental disorders such as depression, another possible consequence of COVID-19, have reportedly been much effective in lowering patients' quality of life [20].
As a significant part of all societies, women play a significant role in societies and in their family's mental health [21]. Moreover, depression is one of the most common mental disorders in women in different societies. Overall, research has shown that approximately 1 in 8 women experiences depression at some point in their lives [22]. In most studies, it was stated that at the time of the COVID-19 pandemic, women were more prone to depression than men [6, 13, 14, 23].
The results of some studies conducted in Iran have shown different levels of depression and quality of life among women. Foroutani, in their research in Larestan, showed that 41.2% of the studied women had some degree of depression [ 24 ]. Hadavi et al. reported the prevalence of depression among women referring to health centers in Rafsanjan as 18% mild, 19.1% moderate, and 4.3% severe [ 25 ]. Further, Pazande et al., in their study on the prevalence of depression in women referring to teaching hospitals in Tehran city, showed that 45.7% of women were depressed [ 26 ]. According to Mirzaei et al., a study of the quality of life of women in Tabriz showed a 56 out of 100 rating for the quality of life of women [ 27 ].
Restated, women play a key role regarding families' security and the formation of moral and emotional ties in a family. They are also responsible for educating the next generation. Furthermore, as half of the population, women play an important and undeniable role in society's development and progress [22]. Depression causes undesirable consequences for women, such as fear and insecurity in life, inability to do normal things in life, physical health problems, etc. Furthermore, the COVID-19 crisis doubles the need to study the matter of depression among women. Accordingly, the present study aimed to examine the level of depressive disorder and its relationship with the quality of life of women admitted to public hospitals. The Results of the study can shed light on health policymakers to be cognizant of the condition for better preparedness for similar outbreaks or the likelihood of disasters.
2. METHODS
2.1. Design and Setting
The present descriptive-analytical cross-sectional study was conducted in 2021. The study population consisted of women admitted to nine large public hospitals.
2.2. Participants
The sample size was estimated to be at least 465 with a 95% confidence level. The distribution of these 465 women among the hospitals was proportional to the size of the population of each of the studied hospitals. First, the number of women admitted to each of the studied hospitals was determined, and then, the sample size was selected in proportion to this number. Then, the selected women were asked to participate in the study. Moreover, in each hospital, several women were selected and assessed using the simple random sampling technique. The inclusion criteria in this study were conscious consent, the ability to speak, and the minimum level of literacy to read and write. Based on the study entry criteria, 465 women were invited, all of whom participated in the study and cooperated with the researchers.
2.3. Instruments
A three-part questionnaire was used to collect the data. The first part of the questionnaire included women's demographic information, including age, place of residence, marital status, education level, and income level. The second part included the main items related to the Goldberg Depression Scale (1990). This part of the questionnaire contained 18 questions scored on a Likert scale (0-5 for not at all, very low, low, medium, high, and very high respectively). Based on this scale, the average scores of 0-9, 10-17, 18-21, 22-35, 36-53, and 54 and up mean “healthy”, “likely to develop depression”, “borderline depression”, “mild to moderate depression,” “moderate to severe depression, and “severe depression”, respectively. The Cronbach's alpha coefficient was calculated for a sample of 40 questionnaires to assess the reliability of the said questionnaire. Based on the calculated coefficients, the Goldberg Depression Scale met the reliability acceptance range (0.82). The validity of this questionnaire was initially confirmed by six members of the faculty of Psychology and Medical Sociology.
The third part of the survey was the World Health Organization Quality of Life-BREF (WHOQOL-BREF) Questionnaire. This scale included 24 questions in four areas of physical health, psychological health, social relationships, and living environment. The answers to these 24 questions were graded based on a 5-part Likert scale (scores of 1 to 5). Different categories were used to determine the surveyed women's quality of life, including favorable (average 89-120), moderate (57-88), and unfavorable (24-56). The validity and reliability of this scale have already been confirmed in previous studies [28, 29].
2.4. Procedures and Statistical Analysis
Regarding the research procedures, two of the researchers (ERD and ZK) referred to the concerned hospitals on different weekdays in morning, evening, and night shifts and distributed questionnaires and collected the required information. First, necessary explanations were given to the participants about the research objectives. Then, they were reassured of the confidentiality of the information they presented to the researchers. Questionnaires were then distributed among the patients. Questionnaires were completed by the patients; however, some patients asked the research team (ERD and SD) to help them fill out the survey.
Afterward, the collected data were analyzed using descriptive and inferential statistical methods via SPSS [23]. Kolmogorov-Smirnov test was used to confirm the normality of the data distribution, and according to p=0.556, the test was not significant. We performed Pearson’s correlation to test the relationship between the main research variables (depression and quality of life) and women’s age. T-test has been used to investigate the mean difference between depression and quality of life based on women’s place of residence. The ANOVA test has been applied to analyze if there are any differences between the main research variables and participants' profiles such as marital status, education, and income level variables.
For research ethics, the questionnaires have been delivered anonymously. The ethical committee of Shiraz University of Medical Sciences with the ID of IR confirmed this study.SUMS.REC.1398.744.
3. RESULTS
As Table 1 shows, most of the studied women were in the age group of 20-35 years (39.14%), lived in urban areas (58.71%), were married (81.09%), had a high school diploma or higher education (68.60%), and had an income level of ten to twenty million Rials as a national currency (52.90%).
Table 2 manifests the frequency of the level of depressive disorder in samples. The results showed that women in the age group over 50, living in rural areas, and divorced women suffered from severe depression, with frequency percentages of 1.81%, 2.08%, and 7.69%, respectively. Moreover, 5.88% and 8.70% of women with primary education level and an income of twenty-one to thirty million Rials per month suffered from severe depression, respectively (Table 2). Fig. (1) emphasizes on the different levels of depression among the participants. According to the figure, about more than half of the participants (51.40%) showed some degree of depression that should be mentioned.
| Variable | Category | Frequency | Percentage |
|
Age (years) |
<20 | 59 | 12.69 |
| 20-35 | 182 | 39.14 | |
| 36-50 | 169 | 36.34 | |
| >50 | 55 | 11.83 | |
| Total | ----- | 465 | 100 |
| Place of Residence | Rural areas | 192 | 41.29 |
| Urban areas | 273 | 58.71 | |
| Total | ----- | 465 | 100 |
| Marital Status | Single | 53 | 11.39 |
| Married | 377 | 81.09 | |
| Divorced | 26 | 5.59 | |
| Widowed | 9 | 1.93 | |
| Total | ---- | 465 | 100 |
| Education Level | Illiterate | 23 | 4.95 |
| Primary school | 51 | 10.97 | |
| Middle school | 72 | 15.48 | |
| High school diploma | 319 | 68.60 | |
| Total | ----- | 465 | 100 |
| Income Level (per month) | No income | 167 | 35.92 |
| 10-20 million Rials | 246 | 52.90 | |
| 21-30 million Rials | 46 | 9.89 | |
| 30+ million Rials | 6 | 1.29 | |
| Total | ----- | 465 | 100 |
| Variable | Category | Frequency of Depression Level | Frequency | |||||
| Healthy | Likely to Develop Depression | Borderline Depression | Mild to Moderate Depression | Moderate to Severe Depression | Severe Depression | |||
| Age (year) | <20 20-35 36-50 >50 |
32 (54.23) * 89 (48.90) 76 (44.97) 11 (20) |
7 (11.86) 39 (21.43) 43 (25.45) 12 (21.83) |
8 (13.57) 18 (9.89) 19 (11.24) 16 (29.1) |
9 (15.26) 22 (12.09) 22 (13.02) 8 (14.45) |
3 (5.08) 14 (7.69) 8 (4.73) 7 (12.72) |
0 (0) 0 (0) 1 (0.59) 1 (1.81) |
59 182 169 55 |
| Place of Residence | Rural areas Urban areas |
56 (29.17) 117 (42.86) |
39 (20.31) 41 (15.02) |
34 (17.71) 36 (13.18) |
48 (25) 59 (21.61) |
11 (5.73) 17 (6.23) |
4 (2.08) 3 (1.1) |
192 273 |
| Marital Status | Single Married Divorced Widowed |
26 (49.06) 224 (59.24) 12 (46.15) 4 (44.45) |
7 (13.20) 51 (13.53) 3 (11.54) 2 (22.22) |
6 (11.32) 42 (11.14) 3 (11.55) 1 (11.11) |
5 (9.43) 31 (8.22) 2 (7.69) 0 (0) |
5 (9.43) 17 (4.51) 4 (15.38) 1 (11.11) |
4 (7.56) 12 (3.18) 2 (7.69) 1 (11.11) |
53 377 26 9 |
| Education Level | Illiterate Primary school Middle school High school diploma |
9 (39.13) 12 (23.53) 18 (25) 133 (41.69) |
10 (43.48) 21 (41.18) 21 (29.16) 118 (36.99) |
0 (0) 4 (7.48) 16 (22.23) 24 (7.52) |
1 (4.35) 5 (9.81) 6 (8.33) 19 (5.96) |
2 (8.69) 6 (11.76) 9 (12.5) 16 (5.02) |
1 (4.35) 3 (5.88) 2 (2.78) 9 (2.82) |
23 51 72 319 |
| Income Level (per month) | No income 10-20 million Rials 21-30 million Rials 30+ million Rials |
48 (28.74) 71 (28.86) 12 (26.09) 3 (50) |
36 (21.56) 43 (17.48) 11 (23.91) 2 (33.34) |
26 (15.57) 51 (20.73) 4 (8.69) 1 (16.66) |
25 (14.97) 46 (18.70) 9 (19.56) 0 (0) |
21 (12.57) 26 (10.57) 6 (13.05) 0 (0) |
11 (6.59) 9 (3.66) 4 (8.70) 0 (0) |
167 246 46 6 |
As we can see in Tables 3 and 4, the mean quality of life score was 58.49±11.51 (out of 120), indicating an average quality of life. According to the results, 85.59% of the women had an average quality of life. Moreover, the quality of life of women over the age of 50, rural residents, divorced women, women with primary level education, and women with no income were undesirable compared to other groups with frequencies of 25.45%, 16.67%, 76.92%, 35.29%, and 17.36%, respectively.
Table 3.
| Variable | Category | Frequency of Quality of Life | Frequency | ||
| Desirable | Average | Undesirable | |||
|
Age (year) |
<20 20-35 36-50 >50 |
7 (11.87) * 6 (3.30) 5 (2.96) 3 (5.45) |
43 (72.88) 166 (91.21) 151 (89.35) 38 (69.10) |
9 (15.25) 10 (5.49) 13 (7.69) 14 (25.45) |
59 182 169 55 |
| Place of residence | Rural areas Urban areas |
9 (4.69) 12 (4.39) |
151 (78.64) 247 (90.48) |
32 (16.67) 14 (5.13) |
192 273 |
| Marital status | Single Married Divorced Widowed |
6 (11.33) 12 (3.18) 2 (7.69) 1 (11.11) |
30 (56.60) 361 (95.76) 4 (15.39) 3 (33.33) |
17 (32.07) 4 (1.06) 20 (76.92) 5 (5.56) |
53 377 26 9 |
| Education level | Illiterate Primary school Middle school High school diploma |
1 (4.35) 2 (3.92) 5 (6.94) 13 (4.07) |
14 (60.87) 31 (60.79) 56 (77.78) 293 (91.86) |
8 (34.78) 18 (35.29) 11 (15.28) 13 (4.07) |
23 51 72 319 |
| Income level (per month) | No income 10-20 million Rials 21-30 million Rials 30+ million Rials |
3 (1.80) 15 (6.10) 2 (4.35) 1 (16.67) |
135 (80.84) 217 (88.21) 37 (80.43) 4 (66.66) |
29 (17.36) 14 (5.69) 7 (15.22) 1 (16.67) |
167 246 46 6 |
| Variable | Dimension | Rank | Frequency | % | Mean±Standard Deviation |
| Quality of life | Physical Health | Desirable | 24 | 5.16 | 58.31±11.09 |
| Average | 364 | 78.28 | |||
| Undesirable | 77 | 16.56 | |||
| Psychological Health | Desirable | 11 | 2.37 | 55.46±9.27 | |
| Average | 412 | 88.60 | |||
| Undesirable | 42 | 9.03 | |||
| Social Relationships | Desirable | 29 | 6.24 | 59.11±12.41 | |
| Average | 404 | 86.88 | |||
| Undesirable | 32 | 6.88 | |||
| Living Environment | Desirable | 18 | 3.87 | 61.09±13.22 | |
| Average | 411 | 88.39 | |||
| Undesirable | 36 | 7.74 | |||
| Total Quality of Life | - | Desirable | 21 | 4.52 | 58.49±11.51 |
| Average | 398 | 85.59 | |||
| Undesirable | 46 | 9.89 |
According to Table 5, among the four dimensions of quality of life, the lowest score was associated with the psychological health dimension and the highest score was associated with the dimension of the living environment. The results showed a statistically significant and inverse relationship between depression and the quality of life of the studied women (r= -0.564, P<0.001). Among the dimensions of quality of life, the dimension of “Psychological Health” had the highest correlation (r= -0.644, P<0.001) with depression.
| Total Quality of Life r (p) | Dimensions of Quality of Life | - | |||
| Living Environment r (P) | Social Relationships r (P) | Psychological Health r (P) |
Physical Health r (P) |
- | |
|
-0.564 (<0.001) |
-0.446 (0.003) |
-0.506 (0.002) |
-0.644 (<0.001) |
-0.628 (<0.001) |
Depression r (P) |
Table 6.
| - | Demographic Variables | ||||
| Main Research Variables | Age | Place of Residence | Marital Status | Education Level | Income Level |
| Depression | r=0.42 P=0.007 |
t=1.54 P=0.04 |
F=2.86 P=0.006 |
F=3.19 P<0.001 |
F=2.08 P=0.03 |
| Quality of Life | r= -0.18 P=0.11 |
t=1.14 P=0.07 |
F=2.16 P=0.02 |
F=1.78 P=0.06 |
F=1.63 P=0.08 |
As for the demographic profile of the sample, (Table 6) revealed that there was a statistically significant relationship between women's depression level and the variables of age (P=0.007), place of residence (P=0.04), marital status (P=0.006), level of education (P<0.001), and level of income (P=0.03). This indicated that the level of depressive disorder was higher in women aged 35-50 years. The findings also suggested that the level of depression was higher in women living in rural areas than urban residents, single women compared to married women, illiterate women compared to women in other educational groups, and women without income than women in other income groups. Besides, married women had a significantly higher quality of life (P=0.02) than single women (Table 6).
4. DISCUSSION
As one of the most common mental disorders, depression covers a wide range of emotional and mental states. The present study aimed to investigate the level of depressive disorder and its relationship with the quality of life of women hospitalized in public hospitals affiliated with Shiraz University of Medical Sciences during the COVID-19 pandemic in 2021. Research findings showed that as far as the level of depressive disorder was concerned, 51.4% of the surveyed women were in the spectrum of “likely to develop depression” to “severe depression”. The results of a systematic review study show that depressive symptoms ranged from mild to extremely severe in 32.7% of Iranian pregnant women during the COVID-19 pandemic [30]. In a study conducted during the COVID-19 pandemic in Cyprus, 72% of the participants were female, and 48% and 9.2% of these female subjects reported mild depressive symptoms and moderate to severe depressive symptoms, respectively [31].
Other studies have indicated different rates of depression, among them Zareipour et al. have reported a prevalence of 42.4% for depression among the studied sample in Iran [32]. Moreover, the findings of another study in Iran by Zareipour et al. suggested that the rate of depressive disorder in women was 31.7% [33]. According to the findings of the study by Alizade et al., the prevalence of severe depression in women in Isfahan was 5.57% [34]. In another study by Rees et al., in the USA, the prevalence of severe depression in women was reported to be 7.4% [35]. In the research by Mangoli et al., the prevalence of depression was 43.3% [36]. This rate can be diverse according to the physical condition of the women. For instance, Ahmadzadeh conducted a study in Isfahan, Iran, and showed that the rate of depression was 7-13% higher in pregnant women than in other females [37].
A prevalence of more than 50% was observed in the reviewed women, ranging from “prone to develop depression” to “severe depression”. The reason for this prevalence among hospitalized women could be that the illness could be an underlying cause of mental problems such as depressive disorder. On the other hand, the prevalence of COVID-19 and the fear, stress, and anxiety of being infected by the virus could be other causes of depressive disorder among the women admitted to the studied hospitals. According to the results of a systematic review study, chronic physical and mental illnesses have been among the risk factors for depression during the COVID-19 pandemic [12]. In another review by Salari et al., it was concluded that there was a significant relationship between a history of chronic physical illness and mental disorders such as depression during the COVID-19 pandemic [23].
Research findings were indicative of a significant relationship between depression and age, place of residence, marital status, education level, and income level of the participants. According to the research results, women living in rural areas suffered from a higher level of depression than women living in cities. In this regard, factors that must be considered were the poor economic situation of some rural households caused by frequent droughts and devastating floods. These issues have always led to the destruction of farms in some Iranian villages, which aggravated mental disorders such as depression along with suffering from other diseases. The present study's findings conveyed that single women suffered from higher levels of depression than married women. In this regard, some studies' findings showed a significant relationship between depression and marital status [38, 39]. The results of most studies indicated that married people were in a better state as far as depression was concerned [40, 41]. In addition, in the study by Rajabizadeh, it was concluded that the score of depression was higher in divorced women than in other groups [42]. However, in some studies, there was no connection between depression and marital status [43, 25]. Receiving emotional support from the spouse and children and having a life purpose in this group might have been a key factor in the lower rate of depression in married women.
In this study, illiterate women suffered from higher levels of depression compared to women in other educational groups. In the studies by Sajadi et al. and Zareipour et al., there were statistically significant relationships between education level and depression variables, meaning that women with a lower education level experienced higher levels of depression [33, 44]. According to Fallahzadeh et al., women with doctoral degrees and higher education suffered from lower levels of depression than other women [45]. One possible reason for this finding could be that the majority of illiterate women also belonged to the low-income or middle-income classes and were more likely to be diagnosed with depression. However, higher levels of awareness and knowledge played a crucial and undeniable role in protecting educated women against depressive disorder. On the other hand, education seems to give a better understanding of the problems of these people. Thus, they experienced depression less than uneducated people. Although the results of a systematic review study showed that during the COVID-19 pandemic, people with higher levels of education were more likely to report anxiety, depression, and stress [23], which contradicted the results of the present study. According to a study conducted in China during the COVID-19 pandemic, mental disorders were more prevalent among people with higher education, which was probably due to this group's high self-awareness of their health [46].
In the present study, the highest frequency of depression was observed in women with low economic status (no income) compared to other income groups. This finding was consistent with the results of other studies that considered economic status an important factor as far as diagnosis of depression was concerned [47, 48]. Various studies have shown that poor economic conditions have been a major risk factor for depression during the COVID-19 pandemic [5-7]. In a study conducted during the COVID-19 pandemic in Cyprus, 48% of the study participants reported financial distress [27]. Due to the need for people to keep social distance and quarantine during the COVID-19 pandemic and their impact on the business of people with lower economic status, low-income people have become much more prone to depression.
Based on the research findings, the quality of life of the examined women was average, which was in line with the findings of Abedzadeh et al. [49] and the study of Aloumanis et al. [50]. A study by Oleksik et al. [51] and a study conducted in Ecuador [52] showed that more than half of the studied women had a high-quality life. By comparing women leading low quality of life in this study and other studies, it could be inferred that the people in the present study had a lower score in psychological and physical dimensions than the people in other studies. In a study conducted in Cyprus, due to the COVID-19 pandemic, increasing financial worries significantly changed the quality of life of 66.7% of participants, almost half of whom (mostly women) also reported some degree of depression [31].
Among the four dimensions of quality of life, the lowest score was associated with the psychological health dimension. This finding indicated that a significant number of women were suffering from undesirable levels of stress, anxiety, and depression before completing the questionnaires. They were relatively dissatisfied with themselves, with life, and with their personal relationships.
Moreover, in this study, the highest score was associated with the dimension of the living environment. This finding indicated that most of the investigated women were in a relatively desirable condition regarding a healthy living environment, access to health services, travel status, the possibility of recreational activities, and satisfaction with their living conditions. Abaszadeh et al. [53] concluded that the lowest score was related to the dimension of limitation caused by physical problems, and the highest score was associated with the mental health dimension. This finding contradicted the results of the present study. Research findings in examining the relationship between demographic variables and different dimensions of quality of life showed that only marital status had a significant relationship with women's quality of life. This could be because receiving psychological support from one's spouse and family and the presence of a spouse during the illness was emotionally essential and prevented patients from isolation and depression. Bjørnnes et al. reported a significant correlation between marriage and health-related quality of life [54].
The findings also showed a statistically significant and inverse relationship between depression and the quality of life of the studied women. Hospitalization during the spread of the coronavirus could actually be stressful and lead to increased depression in hospitalized patients. In a study by Daneshfar et al., it was concluded that during the COVID-19 pandemic in Iran, a significant relationship was observed between the dimensions of quality of life and anxiety and depression in the studied women. Their findings also suggested that the anxiety caused by COVID-19 had a direct effect on the quality of life of Iranian women [55]. A study conducted in China [20] and other studies [56, 57] concluded that the quality of life score of women with depressive symptoms was significantly lower than women without depressive symptoms. This could be due to the fact that these women suffered from mental and psychological problems in addition to physical problems. Therefore, they also experienced a lower quality of life. Fear of being hospitalized, inability to visit patients, and lack of social support from relatives, quarantine, increased social distance for a long while and losing physical contact with family, friends, and relatives, changes in social norms, problems with virtual education for children have probably led to the development of depression and a lower quality of life in the studied women.
In sum, more than half of the surveyed women showed certain levels of depressive disorder, ranging from “likely to develop depression” to “severe depression.” Therefore, making plans for addressing this issue seems to be rather crucial. Other suggestions would be establishing centers at the hospitals and creating a happy and friendly atmosphere, improving the level of women's awareness about ways to reduce depression, and sending psychologists to the hospital in cases of urgent matters and emergencies. It is also recommended that the hospital staff provide social support and effective and communication to reduce women's level of depressive disorder. Furthermore, according to the present study's findings, the participants' quality of life was average and inversely related to depression which needs severe attention and applied interventions by health policymakers.
5. LIMITATIONS
One of the limitations of the present study was the cross-sectional nature of this study, which restricted the generalization of the results. Therefore, it is suggested to conduct longitudinal studies to eliminate this limitation and enhance the comparability and generalizability of the results. Furthermore, this research was a self-reported survey that may cause social desirability bias in regard to answers to the questions. Other studies with a mixed approach of observation and survey might be very helpful.
6. CONCLUSION
The findings of this study could provide useful information to nurses, managers, and health policymakers for better planning and preparedness to overcome the mental effects of future disasters and probable outbreaks. This information could be used to identify women at risk, and to prevent the development of various diseases, including depression, in hospitalized women. The information could also be used along with regular screening programs to emphasize regular exercise and proper nutrition, which could improve women's quality of life.
AUTHORS' CONTRIBUTIONS
ARY and ZK have designed the study and collected the data. ARY and ERD have contributed to the data analysis and initial drafting of the article. ARY and ZK have finalized the quantitative analysis and GM has finalized the manuscript. All authors have read and approved the manuscript.
ABBREVIATION
| QOL | = Quality of life |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Shiraz University of Medical Sciences ethics committee with the approval number of IR.SUMS.REC.1398.744.
HUMAN AND ANIMAL RIGHTS
No animals were used for the studies that are the basis of this research. All human procedures followed were in accordance with the guidelines of the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
Informed consent was obtained from all subjects and/or their legal guardian(s).
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analyzed during the current study are available from the corresponding author [G.M] upon reasonable request.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
FUNDING
There was no funding.
ACKNOWLEDGEMENTS
The present study has been derived from a research project approved by the Vice-Chancellor for Research of Shiraz University of Medical Sciences with the code 20067. Researchers hereby wish to thank the Vice Chancellor for Research of the University, who provided the researchers with the necessary material and spiritual assistance. The researchers also would like to express their gratitude to the participants.

