All published articles of this journal are available on ScienceDirect.

Perception and Knowledge of Adults Toward the Newly Evoked Variant Omicron: A Web-based National Survey from Jordan
Abstract
Background:
Omicron B.1.1.529 possesses the highest number of mutations among all SARSCoV-2 variants. The Omicron variant spread quickly and became globally dominant; the currently available COVID-19 vaccines provided less immunity to the Omicron variant.
Objectives:
This study aimed to explore Jordanians' knowledge and perceptions about the omicron variant and the role of vaccines in protection.
Methodology:
The questionnaire was created using Google Forms and was distributed online via different social media platforms. Participants were recruited through a convenient sampling method and snowball distribution of the questionnaire. Inclusion criteria: being an adult and living in the Hashemite Kingdom of Jordan
Results:
A total of 708 participants responded and filled out the questionnaire with an average age of 39.87 ± 11.09. Less than half of the participants were infected with the coronavirus. Most of the participants were infected only once (238, 78.8%) and mostly with the original strain of the coronavirus. Almost all the participants were vaccinated (661, 93.4%); the majority received two doses (504, 76.3%), followed by three doses (142, 21.5%), and only fifteen participants (2.4%) received one dose of vaccine. Pfizer-BioNTech was the most frequently used type of vaccine. In the multivariate analysis, predictors of a higher knowledge score were education levels (only in postgraduate degree compared to high school or lower education), monthly income higher than 400, presence of comorbidities, and vaccination.
Conclusion:
As the Omicron variant spreads rapidly, educational programs and interventions are needed to improve public knowledge and perceptions, especially for those with low educational levels and monthly income.
1. INTRODUCTION
The latest identified Covid-19 variant was Omicron B.1.1.529, which possesses the highest number of mutations among all SARSCoV-2 variants, with almost 60 mutations in the form of substitutions/deletions/insertions. This new variant is deadlier than the Delta variant, which showed only eight spike protein mutations [1]. Mutations reside in the receptor-binding domain (RBD) of spike glycoprotein, which explains the increased transmissibility and altered efficacy of vaccines [2]. Some reports show that it was first spread in western Europe before It was first reported in South Africa [3]. Omicron, most probably, has evolved early from other SARS-CoV-2 variants [4].
Recent research findings suggest that available vaccines provided less immunity to the omicron variant than other variants [5]. This indicates that vaccines might not be effective against the Omicron variant. One recent study showed that three doses of mRNA vaccines provided better protection against the Omicron variant than two doses [6]. Scientific evidence also revealed that vaccinated individuals have a lower risk of severe disease from omicron infection. Consequently, combining vaccination and public health measures remains the most effective strategy [7].
The efficacy of different types of vaccines is diverse. Vaccines based on the mutant spike have higher neutralizing antibodies against mutant viruses [8]. This result suggests that developing vaccines based on the Omicron variant's mutated spike or the other variants containing one or more Omicron mutations effectively prevents Omicron infection. Moreover, the Omicron variant possesses a high reinfection capacity and may affect previously infected COVID-19 patients [1]. Since This variant can resist current antibodies and has an easier spread than previous variants, the public must become aware of the importance of maintaining present public health preventive measures such as wearing masks, maintaining physical distance, and washing hands. In addition, early diagnosis and quarantine are essential for minimizing virus transmission. This study aimed to explore the knowledge and perceptions of Jordanians about the omicron variant and the role of vaccines in protection. The research question was, ‘Does the Jordanian public have enough knowledge and correct perceptions about the newly evoked Omicron variant?’
2. METHODOLOGY
This web-based cross-sectional study was conducted in Jordan through the distribution of a self-administered questionnaire. Ethical approval was obtained from the institutional review board at Al-Ahliyya Amman University before commencing the study.
The questionnaire was created using Google Forms and was distributed online via different social media platforms, mainly WhatsApp. Participants were recruited through a convenient sampling method and snowball distribution of the questionnaire (considered a limitation of this study). Participants were invited to voluntarily and anonymously complete and then submit their responses. A cover letter was attached to the questionnaire describing the study's aims and importance, guaranteeing the collected data's confidentiality and anonymity. The questionnaire opened only if they chose to participate in the study, and completing it was considered consent to participation. Methods in this research comply with international and national standards for the Declaration of Helsinki, so this study was approved by the Institutional Review Board (IRB) of Al-Ahliyya Amman University (AAU), Research Ethics Committee, with a reference number (IRB: AAU/4/4/2021-2022).
Inclusion criteria: being an adult (18 years or older) and living in the Hashemite Kingdom of Jordan
2.1. Sample Size Calculation
The sample size was calculated using the Raosoft® online sample calculator [9].
50% response distribution was chosen to provide the largest sample size. Based on the Jordanian Department of Statistics, the estimated population of Jordan in 2020 was around 10,200,000 [10]. A margin of error of 5% was selected, and a confidence level of 95%. The sample size was 664, but a larger sample was targeted for better representation. The Google form was available for completion from the 20th of January till 2022. A week before the 24th of February, the number of submissions was almost constant and sufficient; hence the questionnaire was closed.
2.2. Development of the Questionnaire
The questionnaire was developed and written after a thorough literature review. The self-developed questionnaire was constructed based on the study's aims and the information that must be collected from the participants to achieve them. The questionnaire included three sections; demographics and social data, covid 19 infection and vaccination, and information related to the perceptions and knowledge concerning the Omicron variant. It included different types of questions: close-ended, open-ended, and Likert scales. The questionnaire was constructed in English, translated to Arabic, and then back-translated to English to achieve the same meaning. The Arabic version was presented to the participants.
Two external examiners reviewed the questionnaire for scientific competency and relevance, and a language expert checked the clarity and linguistic characteristics of the questions. A pilot study that included 20 individuals known to the researchers from different demographic characteristics was conducted to check the appropriateness of the questions, easy flow, and lack of ambiguity. Based on their remarks and comments, corrections and modifications of the questionnaire were performed accordingly. Responses from the pilot study were not included in the analysis.
2.3. Statistical Analysis
Data were analyzed using IBM SPSS statistics (version 25) software. Descriptive analysis included frequency and percentage for categorical variables and mean ± standard deviation for continuous data. The scores from the knowledge-related questions were summed into a total score, and possible predictors of knowledge were assessed using univariate and multivariate linear regression. P values below 0.05 were considered significant.
3. RESULTS
A total of 708 participants responded and filled out the questionnaire from the 20th of January till the 24th of February 2022, with an average age of 39.87 ± 11.09. Less than half of the participants were infected with the Coronavirus (302, 42.7%), (Table 1).
Table 1.
| - | Frequency (%) |
|---|---|
| Gender | - |
| Male | 252 (35.6%) |
| Work status | - |
| Unemployed | 296 (41.8%) |
| Employed in the health sectors | 104 (14.7%) |
| Employed in non-health sectors | 308 (43.5%) |
| Education | - |
| High school or lower | 89 (12.6%) |
| Community college | 69 (9.7%) |
| University degree | 330 (46.6%) |
| Postgraduate degree | 220 (31.1%) |
| Smoking status | - |
| No | 514 (72.6%) |
| The geographic location of the residence | - |
| North of Jordan | 142 (20.1%) |
| Middle of Jordan | 492 (69.5%) |
| South of Jordan | 74 (10.5%) |
| Place of residence | - |
| Urban | 599 (84.6%) |
| Rural | 109 (15.4%) |
| Monthly income (Jordanian Dinars- JOD) | - |
| Less than 400 | 211 (29.8%) |
| 400-800 | 225 (31.8%) |
| More than 800 | 272 (38.4%) |
| Health condition | - |
| Weak | 10 (1.4%) |
| Moderate | 186 (26.3%) |
| Excellent | 512 (72.3%) |
| Presence of co-morbidities | - |
| No | 557 (78.7%) |
| Number of infections with coronavirus (number of infected participants = 302) | - |
| One time | 238 (78.8%) |
| Two times | 62 (20.5%) |
| Three times | 1 (0.3%) |
| Five times | 1 (0.3%) |
| The severity of symptoms associated with coronavirus infection (number of infected participants = 302) | - |
| No symptoms | 19 |
| Mild symptoms and did not need hospitalization | 78 |
| Moderate symptoms and did not need hospitalization | 179 |
| Severe symptoms and needed hospitalization | 26 |
| Number of vaccine doses (number of vaccinated participants = 661) | - |
| One dose | 15 (2.35) |
| Two doses | 504 (76.3%) |
| Three doses | 142 (21.5%) |
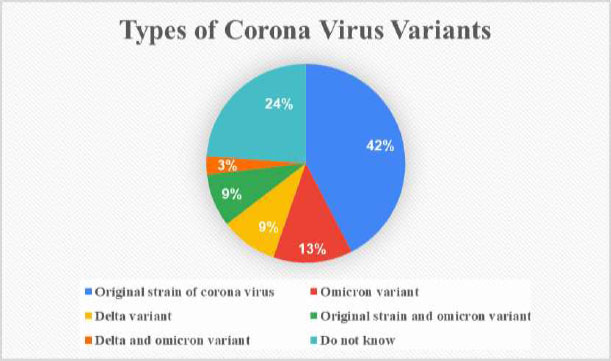
Most of the participants were infected only once (238, 78.8%) and mostly with the original strain of the coronavirus. Among the 302 participants infected with the coronavirus, the original strain was the most common cause (Fig. 1).
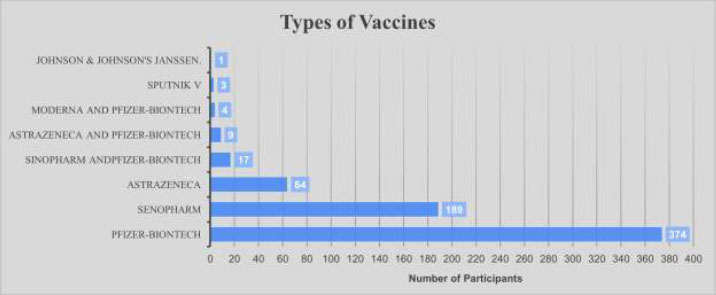
Almost all the participants were vaccinated (661/708, 93.4%); the majority received two doses (504/661, 76.3%), followed by three doses (142, 21.5%), and only fifteen participants (2.4%) received one dose of vaccine. Pfizer-BioNTech was the most frequently used type of vaccine (Fig. 2).
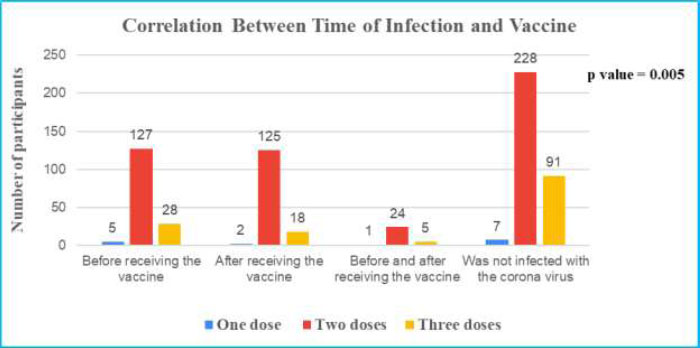
Despite receiving the vaccine, 285/661 (43.1%) participants were infected with the coronavirus, and 17/47 (36.2%) non-vaccinated participants were infected, p-value = 0.352. Of the 661 who received the vaccine, 326 participants (49.3%) were not infected with the coronavirus before/after receiving the vaccine, 160 participants (24.2%) were infected with the coronavirus before receiving the vaccine, 145 participants (21.9%) were infected with the coronavirus after receiving the vaccine, 30 participants (4.5%) were infected with the coronavirus before and after receiving the vaccine.
A cross-tabulation between the time of infection and COVID-19 vaccine doses reveals a p-value of 0.005 (Fig. 3).
Attitudes of participants towards the Omicron variant and restrictive measures for protection against the Omicron variant were assessed. Results are shown in Table 2.
| - | Frequency (%) |
|---|---|
| More health measures (masks and hand washing) are important to reduce infection with the Omicron variant | - |
| Agree | 330 (46.6%) |
| Neutral | 147 (20.8%) |
| Do not agree | 231 (32.6%) |
| Booster doses of the vaccine must be encouraged to reduce the rate of infection with the Omicron variant | - |
| Agree | 280 (39.5%) |
| Neutral | 203 (28.7%) |
| Do not agree | 225 (31.8%) |
| A participant who was not vaccinated, will the emergence of the omicron variant encourage you to take the vaccine (N=47) | - |
| Agree | 15 (31.9%) |
| Neutral | 20 (42.6%) |
| Do not agree | 12 (25.5%) |
| The emergence of the Omicron variant makes you worried and stressed | - |
| Agree | 238 (33.6%) |
| Neutral | 197 (27.8%) |
| Do not agree | 273 (38.6%) |
| Normal life can be restored after | - |
| After 6 months | 295 (41.7%) |
| After a year | 95 (13.4%) |
| After more than a year | 165 (23.3%) |
| Never | 153 (21.6%) |
Knowledge of different aspects of the Omicron variant was evaluated using 8 statements in Table 3. Correct answers were assigned one mark, and wrong answers or “do not know” were given zero. A total of complete, correct knowledge would have a score of 8.
The average total knowledge score was 4.19 ± 2.06 (out of 8); individual scores for each statement are shown in Table 3.
Concerning the time when normal life can be restored, most participants (295, 41.7%) believed that this is possible after 6 months, a lower percentage believed that more than a year is needed (165, 23.3%), 95 (13.4%) participants thought that within a year we could go back to normal life, and some believed that we would never go back to our previous way of life (153, 21.6%).
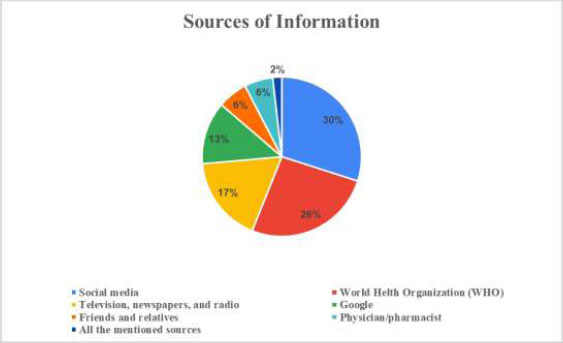
Jordanians received their information mainly from social media, WHO reports, television, newspapers, radio, and google (Fig. 4).
In the multivariate analysis, predictors of a higher knowledge score were education level (only in postgraduate degree compared to high school or lower education), monthly income higher than 400, presence of comorbidities, and being vaccinated (Table 4).
| - | Frequency (%) | Average Score |
|---|---|---|
| Infection with the omicron variant is confirmed by | - | 0.62/1 |
| PCR * | 442 (62.4%) | - |
| Blood sample | 30 (4.2%) | - |
| Symptoms | 115 (16.2%) | - |
| I do not know | 121 (17.1%) | - |
| Protection against the omicron virus is accomplished after | - | 0.20/1 |
| After three doses of vaccines * | 143 (20.2%) | - |
| After two doses of vaccines | 66 (9.3%) | - |
| After one dose of the vaccine | 6 (0.8%) | - |
| Regardless of doses, the vaccine does not provide protection | 323 (45.6%) | - |
| I do not know | 121 (17.1%) | - |
| The Omicron variant spreads more easily than other corona variants | - | 0.80/1 |
| Yes * | 567 (80.1%) | - |
| No | 21 (3.0%) | - |
| I do not know | 120 (16.9%) | - |
| Vaccination reduces the severity of omicron variant infection | - | 0.64/1 |
| Yes * | 452 (63.8%) | - |
| No | 90 (12.7%) | - |
| I do not know | 166 (23.4%) | - |
| Vaccines provide less protection against the Omicron variant than other variants | - | 0.31/1 |
| Yes * | 222 (31.4%) | - |
| No | 149 (21.0%) | - |
| I do not know | 337 (47.6%) | - |
| Previous infection does not protect against omicron variants | - | 0.51/1 |
| Yes * | 364 (51.4%) | - |
| No | 90 (12.7%) | - |
| I do not know | 254 (35.9%) | - |
| The Omicron variant is less dangerous than other corona variants | - | 0.65/1 |
| Yes * | 458 (64.7%) | - |
| No | 78 (11.0%) | - |
| I do not know | 172 (24.3%) | - |
| Symptoms of infection with the Omicron variant are different than those of other Corona variants | - | 0.46/1 |
| Yes * | 323 (45.6%) | - |
| No | 170 (24.0%) | - |
| I do not know | 215 (30.4%) | - |
| Total knowledge score | - | 4.19/8 |
| Variable | Univariate Linear Regression | Multivariate Linear Regression | ||||
|---|---|---|---|---|---|---|
| - | B | 95% CI | P value | B | 95% CI | P value |
| Age | 0.020 | 0.007- 0.033 | 0.003 | 0.004 | -0.010 - 0.018 | 0.607 |
| Gender | - | - | - | - | - | - |
| Male # | - | - | - | - | - | - |
| Female | 0.194 | -0.123 - 0.511 | 0.230 | 0.325 | -0.008 - 0.658 | 0.056 |
| Smoking status | - | - | - | - | - | - |
| No # | - | - | - | - | - | - |
| Yes | -0.469 | -0.808 - 0.130 | 0.007 | -0.294 | -0.647 - 0.058 | 0.102 |
| Education | - | - | - | - | - | - |
| High school or lower # | - | - | - | - | - | - |
| Community college | 0.220 | -0.408 - 0.848 | 0.492 | -0.044 | 0-.666 - 0.579 | 0.891 |
| University degree | 0.936 | 0.468 - 1.403 | <0.001 | 0.394 | -0.114 - 0.902 | 0.128 |
| Postgraduate degree | 1.546 | 1.054 - 2.038 | <0.001 | 0.875 | 0.320 - 1.430 | 0.002 |
| Place of residence | - | - | - | - | - | - |
| Urban # | - | - | - | - | - | - |
| Rural | -0.438 | -0.858 - 0.018 | 0.041 | -0.027 | -0.442 - 0.387 | 0.898 |
| Monthly income (Jordanian Dinars- JOD) | - | - | - | - | - | - |
| Less than 400 # | - | - | - | - | - | - |
| 400-800 | 0.994 | 0.617 - 1.371 | <0.001 | 0.618 | 0.218 - 1.018 | 0.003 |
| More than 800 | 1.095 | 0.734 - 1.456 | <0.001 | .614 | .183 - 1.045 | 0.005 |
| Health condition | - | - | - | - | - | - |
| Weak # | - | - | - | - | - | - |
| Moderate | 1.117 | -0.183 - 2.417 | 0.092 | 0.696 | -0.553 - 1.946 | 0.274 |
| Good | 1.663 | 0.385 - 2.942 | 0.011 | 1.162 | -0.091 - 2.415 | 0.069 |
| Presence of co-morbidities | - | - | - | - | - | - |
| No # | - | - | - | - | - | - |
| Yes | 0.289 | -0.081 - 0.660 | 0.126 | 0.591 | 0.185 - 0.997 | 0.004 |
| Infected with coronavirus | - | - | - | - | - | - |
| No # | - | - | - | - | - | - |
| Yes | -0.042 | -0.349 - 0.265 | 0.788 | -0.156 | -0.449 - 0.137 | 0.296 |
| Received the vaccine | - | - | - | - | - | - |
| No # | - | - | - | - | - | - |
| Yes | 1.236 | 0.632 - 1.839 | < 0.001 | 0.999 | 0.396 - 1.603 | 0.001 |
4. DISCUSSION
It's known that the emergence of new COVID-19 variants has raised general concerns [11]; so far, 5 variants for COVID-19 have been announced by WHO, Alpha, Beta, Gamma, Delta, and the newly evoked Omicron [12]. The Omicron variant is the most mutated COVID-19 variant, with around 50 mutations in its genome and 39 mutations in its spike region (S) [13]. Studies evaluating the knowledge of the Jordanian public on Omicron are scarce and still an unexplored subject. Findings from this study have shown that Jordan is a youth country since the mean age in this study is less than forty, which is supported by literature according to UNICEF that 63% of the Jordanian population is under 30 years old [14]. Less than half of the participants were infected with Coronavirus, mostly with the original strain (only 13% of participants were infected with the Omicron Variant) despite almost all the respondents being vaccinated, mostly with two doses frequently with Pfizer-BioNTech. In the literature, the initial breakthrough infections with the Omicron variant in South Africa were reported in persons vaccinated with the Pfizer vaccine [15]. A large percentage of respondents (45.6%) believed that the available COVID-19 vaccines don’t protect against the Omicron variant, but they were convinced that vaccines reduced the severity of Omicron variant infection. BioNTech has speculated results about the effectiveness of their vaccines against the Omicron variant in less than two weeks [16]. Center for Disease Control and Prevention (CDC) [17] and World Health Organization (WHO) [12] have recommended that the booster dose or the third dose protects against the Omicron variant. In addition, findings from Accorsi et al>. revealed that three doses of the COVID-19 mRNA vaccine, compared with being vaccinated with 2 doses, were associated with protection against both the Omicron and Delta variants [18]. Moreover, another recent study indicated that COVID-19 vaccination protects against severe COVID-19 infection caused by SARS-CoV-2 variants, including Omicron [19]. Most participants thought that the Omicron variant was less dangerous than other corona variants and symptoms of infection with the Omicron variant were different than those of other Corona variants. Khandia et al>. discovered that the Omicron variant had a shorter incubation period, and the clinical symptoms were similar to or milder than the previous variants [20]. The initially infected persons with the Omicron variant in South Africa were young university students reporting mild symptoms of fatigue [21]. Thereafter, WHO officially mentioned that Omicron cases are mild [12]. Mohsin & Mahmud stated in their review that the Omicron variant might be less severe than other COVID-19 variants. However, its rapid spread and immune evasiveness represent a great risk to the global health systems [22]. Recent data published from South Africa revealed that the Omicron variant has an increased reinfection risk if compared with Beta and Delta [23, 24]. In this study, when participants were asked if they were worried and stressed due to the Omicron variant, only 38.6% disagreed with this statement, which reflected the real concerns regarding the Omicron variant among Jordanians. This attitude is supported in the literature, as a recent study conducted in Saudi Arabia after the emergence of the Omicron variant has shown a high-stress level and increasing worry among healthcare providers [25]. The overall knowledge score was low, which indicates that the Jordanian public is unaware of the Omicron variant-related information, despite its recent speedy spread [26]. As a result, it is crucial to increase public awareness of omicron severity [27]. Concerning the time needed to restore normal life, most respondents believed this might be possible within 6 months. Predictors for the high knowledge score were education level (only in postgraduate degree compared to high school or lower education), monthly income higher than 400, presence of comorbidities, and being vaccinated. Most participants were infected before receiving the vaccine; the infection correlated with two doses of vaccines, more than three or one dose. This finding supports the need for the booster dose. Surprisingly, the most common information source among the Jordan public was social media. This suggests the need to educate the public on spreading false and misleading information unsupported by scientific evidence. The results revealed in this study will help guide public health policies and government efforts toward better awareness campaigns to address gaps in knowledge and correct misconceptions.
CONCLUSION
This web-based cross-sectional study was conducted in Jordan through the distribution of a self-administered questionnaire. This study aimed to explore the knowledge and perceptions of Jordanians about the Omicron variant and the role of vaccines in protection. Findings from this study demonstrated that the overall knowledge score for Jordanians was low, which indicates that the Jordanian public is unaware of Omicron variant-related information, despite its recent speedy spread. Consequently, educational programs and interventions are needed to improve the knowledge and perceptions of the public, especially those with low educational levels and monthly income.
LIST OF ABBREVIATIONS
| RBD | = Receptor-Binding Domain |
| IRB | = Institutional Review Board |
| AAU | = Al-Ahliyya Amman University |
| CDC | = Center for Disease Control |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Institutional Review Board (IRB) of Al-Ahliyya Amman University (AAU), Research Ethics Committee, with a reference number (IRB: AAU/4/4/2021-2022).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All authors confirm that all authors have read and approved the manuscript. All named authors have approved the order of authors listed in the manuscript.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIAL
The data that support the findings of this study are available from the corresponding author, [M.A], on special request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge all the Staff of Yarmouk University and Al-Ahliyya Amman University for helping the authors in distributing this questionnaire all over the targeted areas.

