All published articles of this journal are available on ScienceDirect.

Senior Nursing Pain Management Applications in Accordance with Bandura's Social Cognitive Theory: A Cross-sectional Study
Abstract
Introduction:
There has been a substantial improvement in the tools and methods for managing pain, but there is still a deficiency in the practices of pain management. Thus, the current study provides an overview of Jordanian pain management practices in relation to Bandura's Social Cognitive Theory.
Aims:
This study aims to examine nurses' Attitudes, Subjective Norms, and Pain Management Practices. Also, it aims to evaluate the impact of Attitudes and Subjective Norms on Pain Management Practices.
Objective:
The objective of this study is to determine the relationship between attitudes, subjective norms, and pain management practices associated with senior Jordanian nurses determine the level of attitudes, subjective norms, and pain management practices among senior Jordanian nurses.
Methods:
Using simple random sampling, nurses were selected. A total of 300 questionnaires were sent, but only 67 returned and were analyzed. A descriptive analysis of study variables was performed using the Statistical Package for the Social Sciences (SPSS), and a correlation analysis was conducted using Smart PLS.
Results:
As a result of the findings, all the hypothesized relationships have been found to be true, particularly the hypothesis that attitude and subjective norms have a direct influence on pain management practices.
Conclusion:
Bandura's social cognitive theory appears useful in predicting nurses' pain management practices, according to the present study. A conclusion can be drawn that the independent variables (Attitude and Subjective Norms) explained 55% of the variation in the dependent variable (pain management practices) in this study. It is, therefore, essential that future researchers consider other personal and environmental factors, including workload, knowledge, experience, and the availability of policies and guidelines.
1. INTRODUCTION
Globally, the pain management system is deficient in both developed countries and developing nations. There are approximately 10% of people worldwide who suffer from uncontrolled pain [1]. There are two types of pains according to the time onset: the first one is an acute pain characterized by high response to analgesics and treatment [2-4] and its endurance of it is less than three months. The second one is chronic pain characterized by low response to analgesic treatment and it leads to the feeling of pain for three months or more [5]. Both types of pain are developed as a result of surgeries, illnesses, injuries, or therapeutic treatments [6], which affect psychological and physiological well-being [7]. This necessitates the use of effective pain management techniques.
In general, pain management practices encompass a wide range of procedures that a healthcare provider should render in order to effectively manage the pain of the patient [8, 9]. Patients are assessed for pain, appropriate interventions are implemented, and the patient is re-evaluated once the pain is controlled. Both doctors and nurses are responsible for managing pain, but nurses play an especially crucial role [10]. Consequently, nurses have been the focus of most studies related to pain management.
In Jordanian hospitals, nurses were found to provide inadequate pain management to relieve in his study patients’ pain [11, 12]. According to Daibes, the nurses neglected to assess the patients’ pain especially between 11 pm and early morning. Also, the female nurses, in particular, avoided assessing patients of a different gender. They also only administered the prescribed analgesic without taking any immediate action, such as using non-pharmacological intervention. In summary, the pain management deficiency in Jordan occurs in all phases of the pain management process.
Uncontrolled pain is a leading cause of individuals visiting hospitals, despite the improvement in the quality of healthcare in the healthcare sector [13]. Studies have shown that 27% of hospitalized children experience moderate or severe pain [14], and 36% of adults report the same [15].
There has been a great deal of study examining the relationship between the factors affecting nurses' pain management (i.e. attitudes, knowledge, subjective norms) and their use of pain management techniques (assessing, intervening, and reassessing) [16-26]. Prior studies did not examine how these factors relate to the senior group, which is the group predominantly responsible for evaluating and controlling patients' pain in hospitals. In previous studies, different theoretical frameworks, including the Theory of Planned Behavior (TPB), the Theory of Reasoned Action (TRA), and the KAP model, were used to analyze the determinants of pain management. It is unfortunate that these theories are ineffective in assessing factors affecting pain management. Studies conducted in the past have demonstrated that the TRA and TPB are appropriate tools for assessing optional behaviors [27, 28], although treating pain is an essential function and a patient's right [29, 30]. On the other hand, the KAP model places sole emphasis on personal factors, even though many studies have demonstrated that pain management is influenced both by personal and environmental factors such as family members, friends, work policies and guidelines [31, 32]. As a result, Bandura's social cognitive theory will prove to be useful for assessing pain management factors. According to this model, the actual behavior (such as pain management) depends on both individual and environmental factors (like attitudes, knowledge & subjective norms) [33].
Bandura's theory has been used in many fields to assess various behaviors. Among them are assessing the learning of speech skills [34], investigating the effects of sports simulation on motor skills [35] and identifying the psychological factors that influence household adoption of water-efficient practices [36]. Furthermore, it has been used in the study of health behavior, such as assessing how organizational factors influence advance care planning [37] and exploring the factors affecting medication administration errors among registered nurses [38]. Bandura's social cognitive theory is the foundation for this research. This study aims to determine the effect of the exogenous variables (i.e. attitudes, subjective norms & knowledge) on the endogenous variable (i.e. pain management practices) for the senior Jordanian nurses. Also, it will assess the moderating effect of knowledge on the relationships between attitudes, subjective norms and pain management practices. Finally, it will assess the level of the study variables (i.e. High, Moderate or Low).
2. MATERIALS AND METHODS
The present study utilized Krejcie and Morgan's table to determine the convenient sample size [39]. The total number of registered nurses who are working in Jordanian public hospitals is 11163 [40]. Based on this table, the appropriate sample size is 375 registered nurses. Out of 375 senior nurses, only 67 completed the questionnaire and returned it. Taking information from published studies and adapting it to meet the needs of the responding population, a cross-sectional structured, validated questionnaire is developed. For assessing the main study variable, 71 study questions were scored on a Likert scale of 1-7. As a whole, 4 categories were assigned to these questions (Attitude, Subjective Norms, Knowledge & Pain Management Practices). There were 22 questions designed to investigate nurses' attitudes toward managing pain. Furthermore, 4 questions are included to assess subjective norms in the study survey and 9 questions to assess the nurses’ knowledge regarding pain management. Moreover, 36 questions are included to assess the nurse's approach to managing the pain of the patient. As a final element of the survey, the nurses were asked six demographic questions related to their gender, age, education, experience, and training and experience pertaining to pain. In the survey, senior nurses were selected by random sampling from 13 public hospitals of the Hashemite Kingdom of Jordan for participation. Senior nurses are defined in the study as those who have graduated from a nursing program, have met the requirements of the Jordan Nurses Association, and have more than ten years of experience in the field.
In this study, the dependent variable (i.e. Pain management practices) is defined as a comprehensive process that should be provided by nurses to control the patients’ pain. On the other hand, the independent variables include the attitude towards pain management which is defined as the intrinsic negative or positive feeling to control patients’ pain. Also, the independent variables of the current study include subjective norms towards pain management which are defined as the nurses’ perception of the favorableness of important others (i.e. family members or friends) towards controlling the patients’ pain. The last independent variable (Knowledge) is defined as awareness of technologies to help patients achieve optimal pain relief.
A statistical analysis of the descriptive data was conducted using SPSS (version 20). A final step involved the analysis of the data with Structural Equation Modeling (SEM), employing Partial Least Square (SmartPLS version 3.0), which provides the capacity to estimate models with several constructs, structural model relationships, and multiple indicators for each construct [41] and this model can be used with a small sample size as recommended by [42].
3. RESULTS
3.1. Respondent Demographics
The majority of surveyed nurses (52 nurses) were female (78%). It is recorded that the average age of nurses was 37. Survey results indicate that the majority of respondents (39 nurses) have experience ranging from 11 to 15 years (58%). There were 59 respondents (88%) with bachelor's degrees, while eight (12%) held master's degrees. Data indicated that the majority of nurses (51 nurses) had never participated in a pain management training program (76%). More than half of the nurses (57 nurses) indicated that they had suffered from severe pain at some point in their lives (85%).
Table 1 below provides a summary of the demographic characteristics of the respondents.
3.2. Latent Construct Descriptive Analysis
Descriptive analysis of the variables in the model was conducted using means and standard deviations. In the present study, all variables were measured based on the Likert scale 1-7, with 7 denoting strong agreement and 1 denoting strong disagreement. Three categories of the Seven-Point Scale have been defined to facilitate analysis of the present study: low, moderate, and high. In general, low scores are considered to be less than 2 (7/7 + lowest value 1); high scores are considered to be more than 6 (highest value 7 - 7/7); while moderate scores are found between low and high [43, 44].
The overall mean value for the study variables can be found in Table 2. It ranges between 4.338 and 5.1505. The mean and standard deviation for Pain Management Practices were 5.1505 and 1.22373, respectively. As a result, it appears that respondents are practicing pain management at a moderate level. Also, the table indicates that nurses' attitudes towards pain management are, on average 4.5848, with a standard deviation of .99658, suggesting moderate attitudes regarding pain management. Further, the results indicate that subjective norms are perceived as moderate (Mean = 4.7687, Standard deviation = 1.21645). Moreover, the nurses have a moderate level of knowledge regarding pain management (Mean =4.338, Standard deviation = 1.032).
| - | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 15 | 22% |
| Female | 52 | 78% |
| Education | ||
| Bachelor degree | 59 | 88% |
| Master degree | 8 | 12% |
| Experience | ||
| From 11-15 years | 39 | 58% |
| From 16-20 years | 28 | 42% |
| Training | ||
| Yes | 16 | 24% |
| No | 51 | 76% |
| Sever Pain Experience | ||
| Yes | 57 | 85% |
| No | 10 | 15% |
| Age | Mean | Std. Deviation |
| 37.41818 | 6.448344 | |
| Study Variables | Number of Items | Mean | Standard Deviation |
|---|---|---|---|
| Pain Management Practices | 36 | 5.1505 | 1.22373 |
| Attitude | 22 | 4.5848 | .99658 |
| Subjective Norms | 4 | 4.7687 | 1.21645 |
| Knowledge | 9 | 4.338 | 1.032 |
| Construct | Cronbach’s Alpha | Composite Reliability | AVE |
|---|---|---|---|
| Attitudes | 0.873 | 0.901 | 0.566 |
| Subjective Norms | 0.803 | 0.870 | 0.627 |
| Knowledge | 0.871 | 0.897 | 0.524 |
| Pain Management | 0.983 | 0.984 | 0.638 |
3.3. PLS-SEM Path Model Evaluation
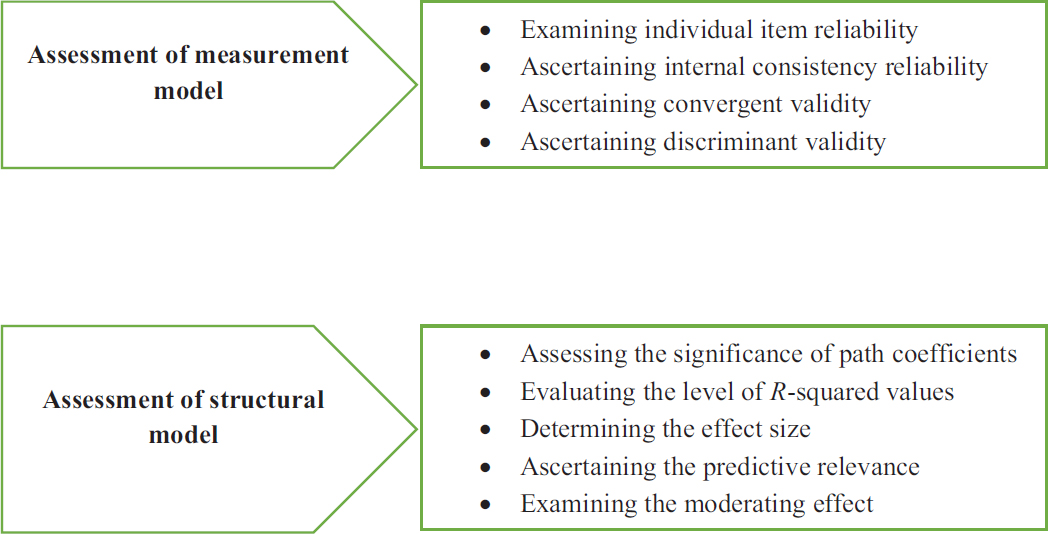
As part of this study, PLS-SEM path evaluation and reporting were undertaken in two steps. A two-step assessment process was adopted that included (1) measurement model evaluation and (2) an evaluation of a structural model, as mentioned in Fig. (1) [45-47].
3.4. Measurement Model Assessment
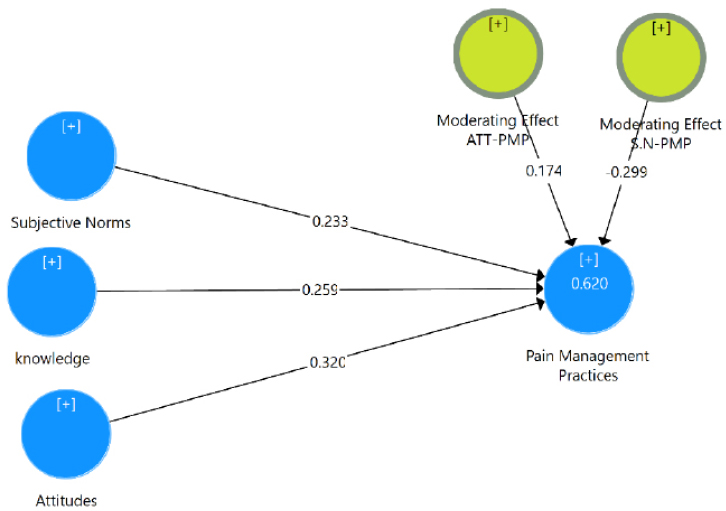
When assessing a measurement model, individual items must be evaluated for reliability, internal consistency reliability, convergent validity, and discriminant validity [45-47]. Based on each construct's outer loadings, each item's reliability was assessed [45, 46, 48]. Afterwards, all items with an outer loading of less than 0.40 or more than 0.7 were removed [49]. In order to achieve the accepted level of composite reliability (.70 or more), the internal consistency reliability is assessed via the composite reliability evaluation, followed by the deletion of some items with the lowest outer loadings [50, 51]. In a study [52], the next test was the convergence validity test, which measured each latent construct's average variation extracted (AVE). A minimum AVE of .50 is required for every latent construct [53]. A discriminant validity estimate was obtained by comparing the square roots of the average variance extracted with the correlations among latent constructs. As a rule of thumb, the AVE should have a square root greater than the correlation between latent constructs [52]. Table 3 and Fig. (2) show the results of the evaluation of the measurement model.
3.5. Analyzing the Structural Model
In order to evaluate a structural model, it is important to examine the significance of the path coefficients, the R-squared value, the size of the effect, and the relevance of the model to prediction [47].
3.6. The Significant of Path Coefficient
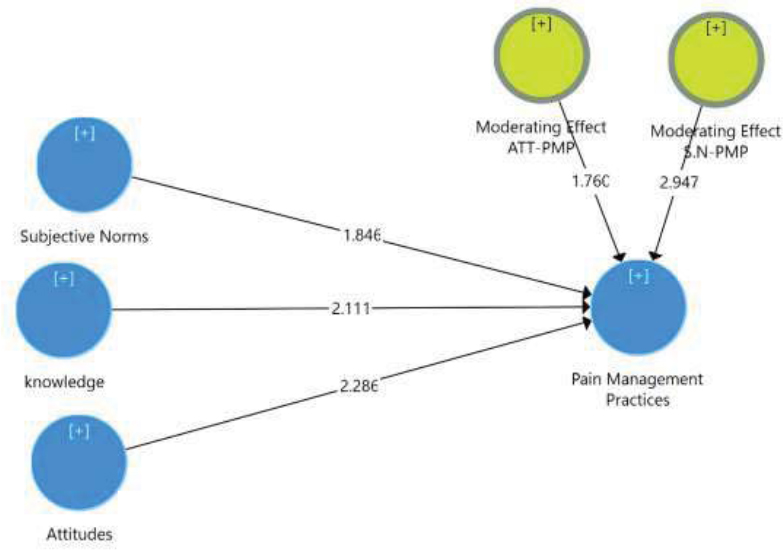
In the present study, 5000 bootstrapping samples were used for the evaluation of path coefficients [49]. Table 4 and Fig. (3) show an analysis of path coefficients for the structural model.
Table 4.
| Hypotheses | Relation | Beta | SD | T-Value | P-Value | Findings |
|---|---|---|---|---|---|---|
| H1 | Attitude & Pain management practices | 0.320 | 0.140 | 2.286 | 0.011 | Supported** |
| H2 | Subjective Norms & Pain management practices | 0.233 | 0.126 | 1.846 | 0.032 | Supported** |
| H3 | Knowledge & Pain management practices | 0.259 | 0.123 | 2.111 | 0.017 | Supported** |
| H4 | Moderating Effect of Knowledge on Attitude & Pain management practices | 0.174 | 0.099 | 1760 | 0.039 | Supported** |
| H5 | Moderating Effect of Knowledge on Subjective Norms & Pain management practices | -0.299 | 0.102 | 2.947 | 0.002 | Supported*** |
| Independent Variable | F-squared | Effect |
|---|---|---|
| Attitude | 0.169 | Moderate |
| Subjective Norms | 0.086 | Weak |
| Knowledge | 0.031 | Weak |
| Endogenous Latent Variables | SSO | SSE | 1-SSE/SSO (cv-red Q2) |
|---|---|---|---|
| Pain Management practices | 2412.000 | 1488.600 | 0.383 |
A positive correlation would exist between senior nurses' attitudes toward pain management and their pain management practices, according to Hypothesis 1. Results of the study (Table 4 and Fig. 3) indicated that these variables were significantly related to each other (β = 0.320, t = 2.286, p< 0.05), in agreement with Hypothesis 1. The study also found that Subjective Norms were significantly correlated with Pain Management Practices (β = 0.233, t = 1.846, p < 0.05), supporting Hypothesis 2. Hypothesis 3 predicted a significant and positive relationship between knowledge and pain management practices. The result showed that the relationship was significant (β = 0.259, t = 2.111, p < 0.05), and, therefore, the hypothesis was supported.
3.7. Testing of Moderating Effect
This study did not only assess the direct relations but also the moderating effect of knowledge on the relationships between attitudes, subjective norms, and pain management practices. Hypothesis 4 posited that knowledge moderates the relationship between attitudes and pain management practices. The results of this study provided support for the hypothesis (β = 0.174, t = 1760, p < 0.05), indicating that the relationship between attitude towards pain management and pain management practices was stronger when knowledge was higher. Finally, Hypothesis 5 predicted that knowledge highly moderates the relationship between subjective norms and pain management practices. The study result showed support for the hypothesis (β = -0.299, t = 2.947, p < 0.01). This implies that the relationship between subjective norms and pain management practices was weaker when the knowledge of the nurses higher.
3.8. Evaluating the Level of R-squared (R2) Value
Statisticians use R-squared to calculate the amount of variation in a dependent variable that can be explained by at least one predictor variable [54, 55]. In PLS-SEM, R2 values for the dependent variables of 0.26, 0.13, and 0.02 can be categorized as substantial, moderate, and weak, respectively [56]. In this study, the R2 value was 0.62, which is considered substantial. In this regard, the independent variables (attitude, knowledge and subjective norms) accounted for 62% of the dependent variables (Pain management practices).
3.9. Assessment of Effect Size (f2)
Effect size can be estimated by using changes in R-squared to estimate how an exogenous latent variable affects an endogenous latent variable [53]. f 2 values of 0.02, 0.15 and 0.35 as having weak, moderate, and strong effects, respectively [56]. In Table 5, the independent variables of the structural model are listed with regard to their effect sizes. In the current study, the f2 was “Moderate” for Attitude variable and “Weak” for the remaining exogenous latent variables (i.e. Subjective Norms & Knowledge).
3.10. Assessment of Predictive Relevance (Q2)
Predictive relevance is often used to determine the goodness-of-fit for partial least squares structural equation models [48]. To test predictive relevance, blindfolding is suggested. “The blindfolding method is only used for endogenous latent variables with reflective measurement models used for operationalization” [57]. Cross Validated redundancy values were calculated using a blindfolding procedure (cv-red value). Models with CV-Red values greater than 0 are predictively relevant, whereas models with CV-Red values less than 0 are not [58]. According to Table 6, blindfolding results for the current study were above zero (Table 6), indicating that the model has predictive relevance [47, 53].
4. DISCUSSION
Bandura's social cognitive theory suggests there are two factors that affect every practice: individual characteristics (such as attitudes) and environmental characteristics (such as subjective norms) [33]. This study defines a person's attitude towards pain management as their general preference for or disfavor of pain management [9]. In addition, Subjective Norms (SNs) are perceptions of social pressure to behave in a given way [59].
An analysis of the current study variables revealed moderate levels of pain management practices (mean = 5.1505, standard deviation = 1.22373), in accordance with previous studies [8, 9]. The study also revealed a moderate level of Subjective norms, consistent with previous research [9, 20]. Similarly, the descriptive analysis revealed moderate attitudes toward pain management, which was consistent with previous studies [8, 9, 20]. Finally, the analysis result showed a moderate level of knowledge regarding pain management, in line with earlier studies [8, 9].
The attitude of Jordanian nurses toward pain management and the practices of their pain management were highly significant and positively related (p < .05). This finding is similar to that found in previous Jordanian studies [9, 18, 60] as well as in other countries [20, 61]. A positive relationship was also found between subjective norms and pain management practices (p < .05). According to previous studies, this result is also consistent [20, 62]. The study results showed significant positive relationship between knowledge of nurses regarding pain management practices and their actual practices to control the patients’ pain, in line with earlier Jordanian studies [9, 18, 60].
This study makes a significant contribution to the literature by assessing the moderating effect of knowledge to fill the literature gap in the pain management field. The study results showed that knowledge played a key moderating role in the relationship between attitudes, subjective norms and pain management practices. That is, the relationship between attitudes towards pain management and pain management practices is stronger for nurses who have a high level of knowledge as opposed to nurses who have low pain management knowledge. On the other hand, the relationship between subjective norms and pain management techniques is weaker for nurses with high levels of knowledge than it is for nurses with low levels of knowledge.
Moreover, the study analysis also demonstrated the level of R-squared value (R2), the level of Effect Size (f2) and the predictive relevance (Q2). R-squared value (R2) was 0.62, indicating that at least 62% variation in the dependent variable could be accounted for by the independent variables (attitude, subjective norms & knowledge). On the other hand, the level of Effect Size (f2) describes how an exogenous latent variable affects an endogenous latent variable by changes in the R-squared [53]. The Attitude variable had a moderate effect size in this study (f2 = 0.169) and it was weak for Subjective Norms (f2= 0.086). This means Subjective Norms only explained 8.6% of pain management practices variance, while knowledge explained only 3.1% of it. Q2 is an indicator of the predictive capability of the model. In this study, the Q2 was assessed using cv-red value and the result showed 0.383. The cv-red value of >0 indicates that the model has a predictive value [58].
CONCLUSION AND RECOMMENDATION
Senior nurses should have a high level of pain management knowledge as they attend many pain training sessions in healthcare settings. Unfortunately, the study result showed a moderate level of knowledge among senior nurses. Future studies should focus on finding the determinants of knowledge deficiency for them.
This study assessed the determinants of pain management practices by focusing on individual factors (i.e knowledge, and subjective Norms). One of the previous Jordanian studies found that controlling pain is not only affected by individual factors but also by organizational factors [27]. So, future studies should emphasize on the organizational factors that can affect the pain management level (i.e. policies, guidelines & overload).
Bandura's social cognitive theory appears useful in predicting nurses' pain management practices, according to the present study. A conclusion can be drawn that the independent variables (Attitude Subjective Norms & knowledge) explained 62% of the variation in the dependent variable (pain management practices) in this study. It is, therefore, essential that future researchers consider other personal and environmental factors, including workload, experience, and the availability of policies and guidelines.
Additionally, the current cross-sectional study showed that Attitudes, Subjective Norms, Knowledge and Pain Management Practices were moderately prevalent. Using a longitudinal research design, future research should assess the effect of providing interventional programs (e.g. Workshops, Training sessions, E-learning) to improve these variables. Also, the present study focused only on one group of population which was senior nurses. Future studies should focus on both groups (senior & junior) to determine whether significant differences exist for some predefined measures between these groups.
Finally, the current study found that knowledge plays a significant moderator role in pain management practices. So, healthcare organizations should enhance their nurses’ knowledge level by providing extra workshops and training sessions in pain management field. Also, universities should review and redesign the existing curriculums to include general knowledge and skills related to assessing, managing and reassessing patients’ pain. Additionally, researchers can utilize this moderator in other nurses’ practices (i.e. infection control & health education) or with other healthcare population (i.e. physicians, paramedics).
LIST OF ABBREVIATIONS
| PLS-SEM | = Partial least squares structural equation modeling |
| SEM | = Structural Equation Modeling |
| TRA | = Temporary Reserved Area. |
| KAP | = Knowledge, Attitudes, and Practices |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The current study has been approved by the Ethical Committee of UUM, Malaysia; approval no. UUM/OYAGSB/ K-14.
HUMAN AND ANIMAL RIGHTS
No animals were used that are the basis of this study. All human procedures were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study are available within the article.
STANDARDS OF REPORTING
COREQ guidelines were followed.
FUNDING
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This study would not have been possible without the participation of all the participants.

