All published articles of this journal are available on ScienceDirect.

Spiritual Health and Job Satisfaction are Inversely related to Nurse Burnout
Abstract
Background:
Recently, the topics of spiritual health and job satisfaction, and burnout of nurses have received the attention of health system researchers. This study aimed at determining the state of spiritual health and job satisfaction and its relationship with job burnout in nurses affiliated with Shahroud University of Medical Sciences.
Materials and Methods:
This cross-sectional study selected 130 nurses working in affiliated hospitals of the university by proportional random sampling in 2022. Also, the study used spiritual health, job satisfaction, and job burnout questionnaires. After data collection, they were analyzed with Chi-square tests and the structural equation method (SEM).
Results:
Most of the studied individuals (n= 90, 69.2%) were female nurses. Most of the nurses (80.8%), which were 105 individuals, had moderate spiritual health and 83 (63.8%) had moderate job satisfaction. According to the results, 30 nurses (23.1%) had high emotional exhaustion (EE). Also, 121 individuals (93.1%) had low and moderate personal inadequacy. Meanwhile, 29 individuals (22.3%) had high depersonalization (DP). The level of spiritual health, job satisfaction, and job burnout of nurses was average. There was an inverse relationship between spiritual health and job burnout, as well as job satisfaction and job burnout.
Conclusion:
The levels of spiritual health, job satisfaction, and job burnout were average in nurses working in the studied hospitals. Therefore, by conducting activities in the field of promoting spiritual health and creating motivation, and reducing the factors that reduce job satisfaction among nurses, the university can help to increase their level of satisfaction, improve the quality of services, and reduce job burnout.
1. INTRODUCTION
Job burnout is a phenomenon that is characterized by chronic stress, depersonalization (DP), emotional exhaustion (EE), and reduced work productivity, and this phenomenon may vary from low to high levels [1]. Job burnout is a physical-psychological syndrome that leads to fatigue as well as negative behavior and attitude of a person toward himself, his job, clients, and lack of job satisfaction [2, 3]. This syndrome is common in jobs where most of the time is spent supporting others [4]. This syndrome is introduced as one of the inevitable consequences of occupational stress, and it is observed with complications such as low morale, decreased sense of adequacy and commitment to work and productivity and increased absenteeism and tardiness of employees, conflict, and change of job. Also, it indicates health problems and low levels of job satisfaction among employees [5-7].
Job burnout is more common in healthcare professionals than in other job categories. Nursing is considered a stressful position that requires technical skills and judgment. The health status of nurses and their satisfaction is related to higher patient satisfaction and lower hospital costs. Job Burnout can have negative effects on nurses, patients and healthcare providers and indirectly effects on public health of the population [4, 5, 8].
According to studies, nurses experience burnout more than other occupations [9-11], and its global prevalence among nurses is reported to be 15-60% [12]. The prevalence of burnout among nurses in developed countries ranges from 49 to 57%, while in sub-Saharan African countries, this has been reported between 40 and 80% [13-17].
Various factors such as type of job, role conflict and confusion, excessive work pressure, type of management, lack of social and spiritual support, organizational changes and intense competition, working hours, inappropriate working conditions, the feeling of organizational inefficiency, the feeling of lack of success, lack of opportunity for promotion and the rigid rules and regulations in the organization and job dissatisfaction and low spiritual health are effective in creating and spreading job burnout [4, 5, 18-21]. Job satisfaction as one of the organizational concepts is effective on the performance of employees and their quality of services and healthcare and job burnout [17].
Job satisfaction is a positive or pleasant emotional state that is the result of job evaluation or individual experience [22] and comes from fulfilling the expectations and needs of employees at the workplace [23] and provides the possibility of achieving or facilitating the achievement of important job values [22]. Job satisfaction of health system employees refers to their inner feeling and attitude toward their job and other work-related elements, such as the work environment, which shows their mental satisfaction with the job [24]. Nurses are the majority of the healthcare workforce in hospitals, and their job satisfaction is an important issue in hospital management. Accordingly, job dissatisfaction among nurses not only increases the wastage of financial resources and the costs of personnel management but also affects the quality of nursing care, which can also lead to risks for patients [24-26]. By committing to their job with a positive attitude, nurses with high job satisfaction can increase the productivity of the organization [27]. Meanwhile, a decrease in their job satisfaction can lead to a decrease in the quality of patient care and appear in the form of job burnout, anxiety, and depression [28, 29].
The topics of spirituality and spiritual health and the job satisfaction of nurses have gained attention in recent decades [30]. The World Health Organization emphasizes the fourth dimension in the definition of health, i.e., the spiritual dimension, along with the three physical, mental, and social dimensions [31, 32]. Generally, spiritual health consists of having a sense of acceptance, positive feelings towards others, morality, and a sense of positive interrelationship with superior power, a sense of positive interrelationship with others and oneself that is achieved through a dynamic and coordinated cognitive, emotional, active, and personal consequence process [32-35]. Spiritual health includes two dimensions: religious health and existential health. Religious health reflects the relationship with God or infinite power, and existential health includes the relationship of a person with oneself, others, and the environment, which can be considered as the ability to integrate various dimensions of existence and have different choices that affect the satisfaction of a person with life and work [32, 36, 37]. Those with stronger spiritual health have more social support. In addition, they have the ability to adapt to spiritual stress and can cope with emerging problems and crises. Meanwhile, the loss of spiritual health may cause depression, feeling alone, and losing the meaning of life [21], which affects life satisfaction and job satisfaction as well as the quality of health care of a person [38].
Considering the issue's importance, this study aimed at determining the state of spiritual health and job satisfaction and its relationship with job burnout in nurses affiliated with Shahroud University of Medical Sciences.
2. MATERIALS AND METHODS
This cross-sectional study was conducted from April to June 2022 at Shahroud University of medical sciences hospitals. Based on the prevalence of moderate and high burnout (35%) in previous studies [4] and type I error of 0.05, power of 80%, and estimation error of 13%, the sample size of this study was estimated to be 106 individuals. According to the number of nurses working in each hospital (300 in Imam Hussein Hospital and 150 in Bahar Hospital), 90 nurses in Imam Hussein Hospital and 50 nurses in Bahar Hospital (a total of 140 nurses) were studied through proportional random sampling. Of the 130 nurses who completed the questionnaires (response rate of 0.93). Working in university-affiliated hospitals and being willing to participate in the study were the inclusion criteria. Also, the exclusion criteria were the out-of-service nurses as well as those who were on maternity, unpaid or illness leaves for more than one month.
2.1. Data Collection Tools
This study included 3 questionnaires on spiritual health [39], Minnesota job satisfaction [40-42], and Maslach burnout inventory [7]. These questionnaires have a number of demographic questions regarding age, gender, work shift, work experience, level of education, marital status, number of children, spouse's occupation, spouse's education level, level of satisfaction with income, and interest in the job, place of residence, and name of the hospital ward.
The 20-question spiritual health questionnaire includes 10 questions to measure religious health and 10 others to measure the existential health of a person [39]. The score of spiritual health is the sum of these two subgroups, the range of which is from 20 to 120. The answers to these questions are classified on a 6-point Likert scale from completely disagree to completely agree. In questions 3, 4, 7, 8, 10, 11, 14, 15, 17, 19, and 20, the choice of completely disagree is scored by 1, and in questions 1, 2, 5, 6, 9, 12, 13, 16, and 18, the same choice is scored by 6. Finally, the spiritual health of the individuals was divided into three categories: low (20-40), medium (41-99), and high (100-120) [43]. The validity of the Persian version of this questionnaire has been reported as 0.82 [44] and 0.92 [32] in studies in Iran.
2.2. Minnesota Job Satisfaction Questionnaire
This questionnaire aims at investigating job satisfaction in 6 dimensions with 19 questions. These dimensions include payment system (questions 1, 2, and 3), type of job (questions 4, 5, 6, and 7), growth opportunities (questions 8, 9, and 10), organizational relationships (questions 11 and 12), leader behavior (questions 13, 14, 15, and 16), and physical conditions (questions 17, 18, and 19). Each question is scored using a Likert scale (completely disagree 1; disagree 2; have no opinion 3; agree 4; and completely agree 5). If the total scores are between 19 and 38, the level of job satisfaction is weak and if the scores of the questionnaire are between 38 and 57, the level of job satisfaction is at an average level. Also, scores above 57 correspond to very good job satisfaction. The validity of the Persian version of this questionnaire has been reported as 0.82 and 0.86 in studies in Iran [40-42, 44].
2.3. Maslach Burnout Inventory (MBI)
This questionnaire is the most common tool for measuring job burnout [7]. The MBI, which is known as a gold standard measurement tool for measuring the level of job burnout, was created by Maslach and Jackson in 1981 and is a test to measure the level of emotional distress caused by the work environment [20]. The Persian version of the job burnout questionnaire includes 25 questions in four areas. Questions 1 to 9 measure the level of emotional exhaustion, 10 to 17 the level of personal functioning, 18 to 22 the level of depersonalization, and 23 to 25 the level of conflict. The answers are classified based on the spectrum of never (score 0), several times a year (score 1), monthly (score 2), several times a month (score 3), every week (score 4), several times a week (score 5) and every day (score 6). The reliability of the Iranian version of the MBI has been investigated in various studies in Iran with Cronbach's alpha coefficient, and its value has been reported as 82 to 90% [4, 45, 46].
The questionnaires were delivered by trained interviewers to nurses during their shifts and were completed in a self-administered form. All questionnaire was checked by interviewers, and if data were missed, it was returned to the participant and completed with more explanation.
2.4. Ethical Considerations
This study has been reviewed and approved by the Ethics Council of Shahroud University of Medical Sciences under the Code of Ethics IR.SHMU.REC.1400.227. The questionnaires were completed anonymously and voluntarily by nurses.
After data collection, the comparison between the groups was examined by ANOVA and Chi-square tests through Stata software. The structural equation method (SEM) was used to investigate the relationships between hidden variables of job burnout, job satisfaction, and spiritual health.
3. RESULTS
Most of the participants in this study, that is, 90 (69.2%) individuals, were female nurses. Also, 106 (81.5%) participants had a bachelor's degree, which was the highest number. The rest of them which was 24 (18.5%), had a postgraduate degree. Married participants were the most frequent, with 82 in numbers (63.1%). Meanwhile, 66 (50.8%) of the participants were working in the morning or evening shift, and the remaining, that is, 64 (49.2%), were working in rotating shifts. In response to the question “How satisfied are you with your income?” 22 (6.9%), 64 (49.2%), and 44 (33.8%) were satisfied, relatively satisfied, and dissatisfied with their income, respectively. In response to the question “How much are you interested in your job?”, 97 (74.6%) participants had expressed great interest in their job.
According to the findings, 105 (80.8%) nurses had moderate spiritual health, and 25 (19.2%) had high spiritual health. Classification of job satisfaction scores showed that 7 (5.4%), 83 (63.8%), and 40 (30.8%) nurses had low, medium, and high satisfaction, respectively. In terms of job burnout dimensions, the results showed that 59 (45.4%), 41 (31.5%), and 30 (23.1%) nurses had low, moderate, and high emotional exhaustion, respectively. In terms of personal Accomp-lishment, 121 (93.1%) nurses had low and moderate personal Accomplishment, and 9 (6.9%) had high personal Accomplishment. In the dimension of depersonalization, 78 (60%), 23 (17.7%), and 29 (22.3%) nurses had low, moderate, and high depersonalization, respectively.
The findings of Table 1 showed a significant relationship between spiritual health and spouse's education (P=0.03), satisfaction with income (P=0.01), and interest in a nursing career (P=0.04). However, there was no significant relationship between spiritual health and gender, marital status, education, spouse's occupation, work shift, and having a job other than nursing (P≥0.05).
The findings of Table 2 showed a significant relationship between job satisfaction and gender (P=0.02), education (P=0.05), satisfaction with income (P<0.001), and interest in the nursing career (P=0.001). But there was no significant relationship between job satisfaction and marital status, spouse's education, spouse's occupation, shift, or having a job other than nursing (P≥0.05).
The findings of Table 3 showed a significant relationship between emotional exhaustion and marital status (P=0.007) and interest in a nursing career (P<0.001). But there was no significant relationship between emotional exhaustion and gender, education, spouse’s job, work shift, having a job other than nursing, and satisfaction with income. Also, there was a significant relationship between personal failure and a spouse's education (P=0.001) and depersonalization and income satisfaction (P=0.012).
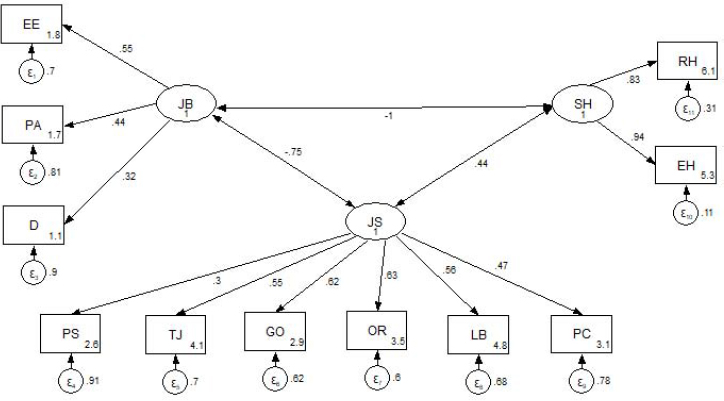
The SEM was used to study the relationship between spiritual health, job satisfaction, and job burnout. The results are presented in Fig. (1). The standardized coefficients of relationships between the hidden variables of burnout and job satisfaction and spiritual health showed a significant and inverse relationship between spiritual health and job burnout. That is, an increase of one score in spiritual health led to a decrease of one score in burnout. Furthermore, there was an inverse relationship between job satisfaction and burnout. Namely, by increasing one job satisfaction score, the job burnout score decreases by 0.75. Also, there was a positive relationship between spiritual health and job satisfaction. Accordingly, by increasing one score in spiritual health, the standardized score of job satisfaction increased by 0.44.
Pearson’s correlation coefficients between spiritual health dimensions and job burnout showed a negative correlation between religious (r=-0.55) and existential health (r=-0.63).
| Variables | Spiritual Health N (%) | - | - | |
| Moderate & Low 105 (80.8) | High 25 (19.2) | X2 | P.V | |
| Gender | - | - | - | - |
| Male | 33 (82.5) | 7 (17.5) | 0.111 | 0.81 |
| Female | 72 (80) | 18 (20) | ||
| Marital Status | - | - | - | - |
| Single | 41 (85.4) | 7 (14.6) | 1.058 | 0.36 |
| Married | 64 (78) | 18 (22) | ||
| Education | - | - | - | - |
| Bachelor | 86 (81.1) | 20 (18.9) | 0.049 | 0.78 |
| Postgraduate | 1979.2 () | 5 (20.8) | ||
| Spouse's Education | - | - | - | - |
| Diploma and less | 15 (100) | 0 (0) | - | - |
| college | 49 (73.1) | 18 (26.9) | 5.16 | 0.03 |
| Spouse's occupation | - | - | - | - |
| Housewife | 9 (90) | 1 (10) | 0.938 | 0.61 |
| Employee | 31 (75.6) | 10 (24.4) | ||
| Other | 24 (77.4) | 7 (22.6) | ||
| Work Shift | - | - | - | - |
| Fixed | 52 (78.8) | 14 (21.2) | 0.339 | 0.66 |
| Rotational | 53 (82.8) | 11 (17.2) | ||
| Having a Job other than Nursing | - | - | - | - |
| Yes | 10 (83.3) | 2 (16.7) | 0.056 | 1.00 |
| No | 95 (80.5) | 23 (19.5) | ||
| Income Satisfaction | - | - | - | - |
| Satisfied | 14 (63.6) | 8 (36.4) | 8.81 | 0.01 |
| Relatively satisfied | 50 (78.1) | 14 (21.9) | ||
| Dissatisfied | 41 (93.2) | 3 (6.8) | ||
| Interest in a Nursing Career | - | - | - | - |
| Low And Moderate | 31 (93.9) | 2 (6.1) | 4.94 | 0.04 |
| High | 74 (76.3) | 23 (23,7) | ||
| Variables | Job Satisfaction, N (%) | - | - | ||
| Poor 7 (5.4) | Moderate 83 (63.8) | High 40 (30.8) | X2 | P.V | |
| Gender | - | - | - | - | - |
| Male | 0(0) | 22(55.0) | 18(45.0) | 7.62 | 0.02 |
| Female | 7(7.8) | 61(67.8) | 22(24.4) | ||
| Marital Status | - | - | - | - | - |
| Single | 1(2.1) | 30(62.5) | 17(35.4) | 2.10 | 0.35 |
| Married | 6(7.3) | 53(64.6) | 23(28) | ||
| Education | - | - | - | - | - |
| Bachelor | 7(6.6) | 71(67) | 28(26.4) | 6.01 | 0.050 |
| Post Graduate | 0(0) | 12(50) | 12(50) | ||
| Spouse’s Education | - | - | - | - | - |
| Diploma and Less | 2(13.3) | 12(80) | 1(6.7) | 4.57 | 0.10 |
| College | 4(6) | 41(61.2) | 22(32.8) | ||
| Spouse’s Occupation | - | - | - | - | - |
| Employee | 0(0) | 70(70) | 3(30) | 5.51 | 0.24 |
| Housewife | 2(4.9) | 24(58.5) | 15(36.6) | ||
| Other | 4(12.9) | () | 5(16.1) | ||
| Work Shift | - | - | - | - | - |
| Fixed | 3(4.5) | 40(60.6) | 23(34.8) | 1.12 | 0.57 |
| Rotational | 4(6.3) | 43(67.2) | 17(26.6) | ||
| Having a Job other than Nursing | - | - | - | - | - |
| Yes | 0(0) | 8(66.7) | 4(33.3) | 0.757 | 0.69 |
| No | 7(5.9) | 75(63.6) | 36(30.5) | ||
| Income Satisfaction | - | - | - | - | - |
| Satisfied | 0(0) | 7(31.8) | 15(68.2) | 21.40 | >0.001 |
| Relatively Satisfied | 3(4.7) | 42(65.6) | 19(29.7) | ||
| Dissatisfied | 4(9.1) | 34(77.3) | 6(13.6) | ||
| Interest in a Nursing Career | - | - | - | - | - |
| Low and Moderate | 4(12.1) | 27(81.8) | 2(6.1) | 14.74 | 0.001 |
| High | 3(3.1) | 56(57.7) | 38(39.2) | ||
| Variable | Emotional Exhaustion, N (%) | |||||||
| Emotional Exhaustion N (%) | Personal Accomplishment N (%) | Depersonalization N (%) | ||||||
| Low | Moderate | High | Low & Moderate | High | Low | Moderate | High | |
| Gender | - | - | - | - | - | - | - | - |
| Male | 24 (60) | 9 (22.5) | 7 (17.5) | 37 (92.5) | 3 (7.5) | 24 (60) | 7 (17.5) | 9 (22.5) |
| Female | 35 (38.9) | 32 (35.6) | 23 (25.6) | 84 (93.3) | 6 (6.7) | 54 (60) | 16 (17.8) | 20 (22.2) |
| X2 | 4.99 | 0.30 | 0.002 | |||||
| P | 0.08 | 1.00 | 0.99 | |||||
| Education | - | - | - | - | - | - | - | - |
| Bachelor | 47 (44.3) | 31 (29.2) | 28 (26.4) | 98 (92.5) | 8 (7.5) | 64 (60.4) | 20 (18.9) | 22 (20.8) |
| Postgraduate | 12 (50) | 10 (41.7) | 2 (8.3) | 23 (95.8) | 1 (4.2) | 14 (58.3) | 3 (12.5) | 7 (29.2) |
| X2 | 3.87 | 0.35 | 1.08 | |||||
| P | 0.14 | 1.00 | 0.58 | |||||
| Marital Status | - | - | - | - | - | - | - | - |
| Single | 28 (58.3) | 12 (25) | 8 (16.7) | 45 (93.8) | 3 (6.3) | 32 (66.7) | 9 (18.8) | 7 (14.6) |
| Married | 31 (37.8) | 29 (35.4) | 22 (26.8) | 76 (92.7) | 6 (7.3) | 46 (56.1) | 14 (17.1) | 22 (26.8) |
| X2 | 5.20 | 0.054 | 2.65 | |||||
| P | 0.007 | 1.00 | 0.27 | |||||
| Work Shift | - | - | - | - | - | - | - | - |
| Fixed | 34 (51.5) | 19 (28.8) | 13 (19.7) | 59 (89.4) | 7 (10.6) | 40 (60.6) | 13 (19.7) | 13 (19.7) |
| Rotational | 25 (39.1) | 22 (34.4) | 17 (26.6) | 62 (96.9) | 2 (3.1) | 38 (59.4) | 10 (15.6) | 16 (25) |
| X2 | 2.09 | 2.82 | 0.72 | |||||
| P | 0.35 | 0.09 | 0.70 | |||||
| Spouse’s Occupation | - | - | - | - | - | - | - | - |
| Housewife | 5 (50) | 5 (50) | 0 (0) | 8 (80) | 2 (20) | 6 (60) | 3 (30) | 1 (10) |
| Employee | 16 (39) | 14 (34.1) | 11 (26.9) | 40 (97.6) | 1 (2.4) | 21 (51.2) | 7 (17.1) | 13 (31.7) |
| Other | 10 (32.3) | 10 (32.3) | 11 (35.4) | 28 (90.3) | 3 (9.7) | 19 (61.3) | 4 (12.9) | 8 (25.8) |
| X2 | 4.92 | 4.07 | 3.07 | |||||
| P | 0.30 | 0.13 | 0.54 | |||||
| Spouse’s Education | - | - | - | - | - | - | - | - |
| Diploma and less | 3 (20) | 7 (46.7) | 5 (33.3) | 10 (66.7) | 5 (33.3) | 9 (60) | 3 (20) | 3 (20) |
| College | 28 (41.8) | 22 (32.8) | 17 (25.4) | 66 (98.5) | 1 (1.5) | 37 (55.2) | 11 (16.4) | 19 (28.4) |
| X2 | 2.49 | 18.32 | 0.46 | |||||
| P | 0.29 | 0.001 | 0.79 | |||||
| Income Satisfaction | - | - | - | - | - | - | - | - |
| Satisfied | 13 (59.1) | 8 (36.4) | 1 (4.5) | 20 (90.9) | 2 (9.1) | 14 (63.6) | 2 (9.1) | 6 (27.3) |
| Relatively Satisfied | 30 (46.9) | 20 (31.3) | 14 (21.9) | 59 (92.2) | 5 (7.8) | 38 (59.4) | 7 (10.9) | 19 (29.7) |
| Dissatisfied | 16 (36.4) | 13 (29.5) | 15 (34.1) | 42 (95.5) | 2 (4.5) | 38 (59.4) | 7 (10.9) | 19 (29.7) |
| X2 | 7.58 | 0.63 | 12.84 | |||||
| P | 0.11 | 0.73 | 0.012 | |||||
| Interest in Nursing Career | - | - | - | - | - | - | - | - |
| Low | 2 (6.1) | 16 (48.5) | 15 (45.5) | 30 (90.9) | 3 (9.1) | 14 (42.4) | 8 (24.2) | 11 (33.3) |
| High | 57 (58.8) | 25 (25.8) | 15 (15.5) | 91 (93.8) | 6 (6.2) | 64 (66) | 15 (15.5) | 18 (18.5) |
| X2 | 28.69 | 0.32 | 5.76 | |||||
| P | 0.000 | 0.69 | 0.056 | |||||
| Having a Job Other than Nursing | - | - | - | - | - | - | - | - |
| Yes | 7 (58.3) | 3 (25) | 2 (16.7) | 12 (100) | 0 (0) | 6 (50) | 4 (33.3) | 2 (16.7) |
| No | 52 (44.1) | 38 (32.2) | 28 (23.7) | 109 (92.4) | 9 (7.6) | 72 (61) | 29 (16.1) | 27 (22.9) |
| X2 | 0.903 | 0.98 | 2.24 | |||||
| P | 0.64 | 1.00 | 0.33 | |||||
4. DISCUSSION
In response to the question, how satisfied are you with your income? 22 (6.9%), 64 (49.2%), and 44 (33.8%) nurses were satisfied, relatively satisfied, and dissatisfied with their income, respectively. The results of a study in Ahvaz hospitals, Iran showed that 3.8% of nurses were satisfied with their income, 62.5% were relatively satisfied, and 33.8% were dissatisfied with their income status, which is the same percentage of dissatisfaction in this study [40]. It seems that income is one of the most important reasons to choose a job that, in many cases, it can even cause other factors to be ignored. The inadequacy of wages makes it necessary for some employees to try to do a second job, and these side jobs reduce their strength and energy to a great extent. This has negative effects on the quality of work productivity and performance of governmental and private organizations in the form of various social damages.
In response to the question, how much are you interested in your job? Ninety-seven nurses (74.6%) expressed great interest in their job. The results of a study in Iran showed that 63.8% were interested in the nursing profession, which is close to the results of this study [40]. It seems that being interested in a job not only leads to the progress of an individual in different fields but can also have a significant impact on the progress and success of an organization and society. Job satisfaction scores showed that 83 (63.8%) and 40 (30.8%) nurses had moderate and high job satisfaction, respectively. The result of a study in Ahvaz Medical Sciences hospitals showed that 55% of nurses had moderate job satisfaction and 45% had high job satisfaction, which is different from the results of this study [40]. A study in the USA showed that 98.6% of nurses had moderate and high satisfaction, which is more than the results of this study [47].
The job satisfaction score of nurses in this study was moderate. The results of this study are consistent with the results of other studies in Iran and the world [24, 40, 48]. According to the results of a study in Croatia, the participants had high job satisfaction scores, which is not consistent with the results of this study [29]. Job satisfaction would vary depending on social and environmental conditions such as the position of the nursing profession in society, hospital facilities and equipment, salary, allowances, income, and even nurses' attitudes. Job satisfaction can have a positive effect on nurses' performance.
There was a significant relationship between job satisfaction and gender, education, satisfaction with income, and interest in a nursing career. The results of a study in Croatia showed a significant relationship between job satisfaction and gender, which is consistent with the results of this study [29]. Social identity of females and their roles in the community as motherhood and wife can interact with their occupation and can lead to decreasing job satisfaction levels. In a study in Iran, a significant relationship has been reported between job satisfaction and interest in nursing, which is consistent with the results of this study [40]. The results of a study in China showed a relationship between the level of education and job satisfaction, which is consistent with the results of this study [24]. The relationship between job satisfaction and education can be caused by the relationship between job status and education. That is, those with higher education enjoy better job positions. The results of a study in Iran showed that there is no significant relationship between job satisfaction and income satisfaction, which is not consistent with the results of this study [40]. The relationship between gender and job satisfaction is a very interesting and noteworthy result. Because the majority of nurses in hospitals are female, and therefore serious measures should be taken to increase their job satisfaction in the workplace.
There was no significant relationship between job satisfaction and marital status, education, spouse’s job, work shift, and having a job other than nursing. The results of studies in China and Croatia showed that there is a relationship between marital status and job satisfaction, which is not consistent with the results of this study [24, 29]. In another study at Shahroud University of Medical Sciences in 2008, no significant relationship was observed between job satisfaction and marital status, and education, which is consistent with the results of this study [48]. The difference in the results of the domestic and foreign studies should be considered as a result of the difference in cultures, the different positions of the profession in different societies, and the difference in the used questionnaires.
The findings showed that 105 (80.8%) of the nurses had moderate spiritual health, and 25 (19.2%) had high spiritual health. In another study in Iran, 45% of participants had moderate spiritual health, and 55% had high spiritual health, which is different from the results of this study [21]. There was a significant relationship between spiritual health and the spouse's education, satisfaction with income, and interest in the nursing career. However, there was no significant relationship between spiritual health and gender, marital status, education, spouse's job, work shift, and having a job other than nursing. The results of studies in Iran and South Korea showed a significant relationship between spiritual health and age, marital status, and education, which is not consistent with the results of this study [21, 49], but there was no significant relationship between spiritual health and gender, which is consistent with the results of this study [21]. In another study in Qom, Iran hospitals, no significant relationship was observed between spiritual health and gender, marital status, and education of nurses, which is consistent with the results of this study [50]. Perhaps one of the reasons for the differences can be the difference in research samples and environments.
In terms of emotional exhaustion, the results indicated that 45.4%, 31.5%, and 23.1% of nurses had low, moderate, and high emotional exhaustion, respectively. The results of another study on health service providers showed that 64.2%, 18.4%, and 17.3% of participants have low, moderate, and high emotional exhaustion, respectively, which is different from the results of this study [4]. In a study in 2020 in Iran, 34.1%, 31.7%, and 34.2% of the participants had low, moderate, and high emotional exhaustion, respectively [51]. In a study in China, 22.09% of participants had emotional exhaustion [52], which indicated moderate emotional exhaustion in nurses. Also, 93.1% had low and moderate personal inadequacy, and 6.9% had high personal inadequacy. The results of another study on health service providers showed that 50.4%, 15.7%, and 39.9% of participants had low, moderate, and high personal inadequacy, respectively [4].
In a study in 2020 in Iran, 24.9%, 19%, and 56.1% had low, moderate, and high personal inadequacy, respectively [51]. In a study in China, 10.7% of participants had personal inadequacy [52]. Meanwhile, 60%, 17.7%, and 22.3% of nurses had low, moderate, and high levels of depersonalization, respectively. The results of another study on health service providers showed that 81.2%, 10%, and 8.8% had low, moderate, and high levels of depersonalization, which is different from the results of this study [4]. In a study in 2020 in Iran, 9.4%, 41.9%, and 48.7% had low, moderate, and high levels of depersonalization [51]. Also, in a study in China, 23.58% of participants had depersonalization, which is somewhat close to the results of this study [52]. The difference in the results of the domestic and foreign studies should be considered as a result of the different cultures and the different positions of the profession in various societies.
Due to emotional exhaustion and moderate depersonalization, and low level of personal inadequacy, job burnout in nurses was moderate. The results of studies in Croatia and South Korea showed high job burnout in participants, which is not consistent with the results of this study [29, 49] .Perhaps one of the reasons is the mismatch between the results of the type of hospitals and conducting the study on nurses working in certain departments of the hospital.
There was a significant relationship between emotional exhaustion and marital status, and interest in nursing. In a study in Iran in 2020, a significant relationship was reported between emotional exhaustion and marital status, which is consistent with the results of this study [51]. But there was no significant relationship between emotional exhaustion with gender, education, spouse's education, spouse's occupation, work shift, having a job other than nursing, and satisfaction with income. The results of studies in Iran and England showed a significant relationship between emotional exhaustion and gender, which is not consistent with the results of this study [51, 53]. However, no significant relationship was reported between emotional exhaustion and education, which is consistent with the results of this study [53].
There was a significant relationship between individual lack of personal accomplishment and spouse's education, yet, there was no significant relationship with gender, education, spouse's job, work shift, having a job other than nursing, and satisfaction with income. The result of a study in England showed a significant relationship between lack of personal accomplishment and gender, which is not consistent with the results of this study [53]. However, no significant relationship was observed between a lack of personal accomplishment and education, which is consistent with the results of this study [53]. In a study in 2020 in Iran, a significant relationship was reported between lack of personal accomplishment with gender and marital status, which is not consistent with the results of this study [51].
There was a significant relationship between depersonalization and income satisfaction. But there was no significant relationship between depersonalization and gender, education, spouse's education, spouse's occupation, work shift, having another job other than nursing, and satisfaction with income. The result of a study in England showed no significant relationship between depersonalization and gender and education, which is consistent with the results of this study [53]. In a 2020 study in Iran, a significant relationship was reported between depersonalization and gender and marital status, which is not consistent with the results of this study [51].
The SEM showed a significant and inverse relationship between spiritual health and job burnout which is consistent with the results of studies conducted in Iran and South Korea [21, 50]. Considering the fact that having peace in dealing with occupational tensions is necessary for the effective actions and interventions of the nursing staff and because spiritual health can create conditions for enduring the hardships of the work environment as well as making work enjoyable, it seems that using religious and existential educations in work environments can increase spiritual health, reduce job burnout, and increase productivity. Our results showed from these two dimensions of spiritual health; existential health is more correlated with job burnout (negative correlation). Existential health reflects the relationship of a person with oneself, others, and the environment, which can be considered as the ability to integrate various dimensions of existence and affects the satisfaction of a person with life and work.
The SEM concerned with the relationship between job satisfaction and burnout showed an inverse relationship between them which is consistent with the results of this study [29, 52, 54, 55]. Increasing the responsibility, motivation, and productivity of the staff of any organization depends on the problem of job satisfaction. The job satisfaction of nurses can reduce their desire to leave the service and job burnout.
LIMITATIONS OF STUDY
Due to the cross-sectional nature of the study, the causal relationship between job satisfaction and spiritual health with job burnout could be subject to a reverse causality error. Generalizing the results of the study to the entire nursing community is limited due to the number and limitation of the study to two hospitals. Good study design and appropriate sample size, and the use of standard questionnaires were the strengths of this study.
CONCLUSION
Considering the high prevalence of depersonalization in nurses and the average level of spiritual health, job satisfaction, and job burnout in nurses working in the studied hospitals, the activities and interventions related to promoting spiritual health, creating motivation, and increasing job satisfaction and income satisfaction can lead to reducing burnout and increasing service levels.
AUTHORS' CONTRIBUTION
AR.Z performed the data gathering and analysis, interpreted the ensuing results, and drafted the manuscript. M.A. and A.Kh conceived the idea, supervised the study, contributed to the conception, and revised the manuscript. All the authors read and approved the final draft.
LIST OF ABBREVIATIONS
| ANOVA | = Analysis of Variance |
| MBI | = Management Buy-in |
| SEM | = Structural Equation Method |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethical review board of Shahroud University of Medical Sciences with the code IR.SHMU.REC.1400.227.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
COREQ guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available on request due to privacy/ethical restrictions.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The researchers are grateful to all nurses who participated in this study. In addition, we would like to thank the Deputy of Research at Shahroud University of Medical Sciences.

