All published articles of this journal are available on ScienceDirect.

Characteristic Features of Dietary Patterns and Physical Activity among Medical Students
Authors Info & Affiliations
Abstract
Introduction
This paper deals with the investigation of controlled risk factors associated with body weight disorders of young people with overweight and obesity. Authors are convinced that the formation of a conscious attitude to health in youth and early diagnosis of any abnormalities through the dynamic monitoring of adolescents and young people with excess body weight could help in the solution to this problem.
Methods
Statistical and sociological methods were used during the investigation. 80 students from a medical university participated in this research. In the survey, Google Forms online application were used. The authors followed all the principles of bioethics and medical deontology in conformity with the requirements of the Helsinki Declaration. The questionnaire contained points about the diet, food habits and preferences, socio-economic status of the respondent’s family, the level of their physical activity, knowledge about a healthy lifestyle, and relationships in the group.
Results
The primary processing of the obtained data was carried out using the methods of descriptive and analytical statistics with the provision of results in the form of relative indicators (Р, %) with an error (m, p). The specificity of the eating behavior of youth was connected with the absence of a food regime, the multiplicity of meals, and the low level of eating culture (lack of a permanent place to eat or eating in front of a computer or TV). Moreover, such habits, like eating before going to bed, eating under stress, or frequently visiting fast food restaurants, were typical for this group of population. A large number of young people were found to be prone to use advertised products.
Conclusion
Young people’s awareness of healthy nutrition has been found to be insufficient, and the level of physical activity in the studied group as unsatisfactory. Significant features of physical activity associated with maladaptive eating behavior have been observed to be a lack of physical activity on weekdays, absence of morning gymnastics, failure to comply with the norms of rational nutrition in the family, or low level of information about healthy nutrition.
1. INTRODUCTION
The significant spread and constant growth of non-infectious diseases in the world have the features of an epidemic. The World Health Organization (WHO) emphasizes that the basis of the development of non-communicable diseases, including ones associated with body weight disorders, is a leading role played by behavioral, i.e., controlled risk factors, and the preventive focus of medical care is still imperfect, especially among young people in matters of formation of conscious attitude to health or early diagnosis of any abnormalities [1].
According to the WHO, obesity and excess body weight in today’s conditions are one of the important problems healthcare systems in the world are faced with. Although obesity is an undeniable physical handicap, it also has a number of potential complications, such as an increased risk of cardiovascular disease, lipid metabolism abnormalities, diabetes, sleep apnea, and depression.
The formation of comorbid pathology has also become a problem for health. Thus, it is determined that among children with excess body weight, 19% of children have two risk factors for the development of cardiovascular diseases, and among those with obesity, already 39% of children have two or more cardiovascular risk factors [2].
The problem of obesity and excess body weight is faced by the Ukrainian population as well, as evidenced by the data of official statistical reporting [3] and the results of the world’s scientific research [4-6]. Eating disorders and a low level of physical activity are usually the factors contributing to body weight disorders. Therefore, timely identification of maladaptive eating behavior in combination with physical activity may provide an opportunity for the introduction of timely corrective measures.
The purpose of the work was to determine the peculiarities of eating behavior and physical activity of modern youth in order to introduce programs for preventing body weight disorders.
2. MATERIALS AND METHODS
2.1. Study Design
The cross-sectional survey research was carried out from December 2022 to March 2023 among medical students.
2.2. Setting
The survey was conducted among students of a higher medical school in a large industrial city (Kharkiv National Medical University, Kharkiv, Ukraine).
2.3. Study Population and Sampling Strategies
Based on generally accepted methods [7, 8], it was determined that the acceptable number of samples should be 10% or more of the general population. Our study was conducted among students with 3–5 years of study, the total number of which was 526 people. 80 correctly filled questionnaires were included in the analysis, accounting for 25 questionnaires from 3rd-year students, 27 questionnaires from 4th-year students, and 28 questionnaires from 5th-year students, respectively.
2.4. Measurement
The questionnaire for data collection was developed by specialists in the department taking into account the issues being the focus of interest. The questionnaire was presented as a Google form. The results and explanations are presented below. The questions of the questionnaire, the research algorithm, and compliance with the rules for the preservation of personal data were considered at the meeting of the Commission on Ethics and Bioethics of the Kharkiv National Medical University (approval no. 1) dated January 12, 2021. After obtaining consent to participate in the study, students had access to the questionnaire. The questionnaire was anonymous, and all results were calculated in a general form.
2.4.1. Outcome Variables
The questionnaire contained 60 questions about diet, food habits and preferences, physical activity, and knowledge about a healthy lifestyle. The answer options had the following gradation: yes, sometimes, no. The questions related to the definition of time intervals had a gradation: up to three hours, more than three hours. Questions related to knowledge or possession of information had a gradation of answers: yes, possess, partially possess information, do not possess/do not know. The survey was conducted anonymously, eliminating any questions of analysis bias.
2.4.2. Explanatory Variables
The questionnaire was logically divided into subsections. The first subsection included general characteristics (gender, age, course of study). The second subsection was focused on the physical activity that the respondents had (performing morning physical exercises, classes in sports sections, independent sports activities, frequency of using stairs to climb the floor or moving on foot, mobile activity, or physical work on weekdays or weekends). Answers to the questions included a gradation of “yes, sometimes, never”.
The third section was devoted to issues related to diet, food preferences, and peculiarities of eating behavior. The wording of the questions also included answers according to the gradation of “yes, sometimes, no”. Part of the questions had open-answer options.
The fourth section dealt with the preventive component, knowledge about adherence to health-oriented behavior, healthy nutrition, physical activity, and support for maintaining a healthy lifestyle. The gradation of answers to this group of questions was “yes, I have it”, “I partially have the information”, and “I do not have it/do not know”.
The questionnaire was reviewed by reviewers and pilot-tested with the participation of 30 students of the same age group. The average time for answering questions was 35 minutes.
2.5. Data Collection
The study was conducted every week from December 2022 to March 2023, during students’ attendance at practical online classes at the Department of Public Health and Health Care Management of the Kharkiv National Medical University. Before conducting the questionnaire, the purpose of the study was explained to the students, and voluntary consent to conduct the study was obtained. It was also clarified that the data will be processed in a general form, and the confidentiality of personal data will be respected. After that, students got access to the online questionnaire. The analysis included questionnaires that contained answers to all the questions posed.
2.6. Statistical Analyses
For data analysis, the answers were exported from the Google form in the form of an MS Excel file with subsequent preparation of its analysis in the STATA program (License of Kharkiv National Medical University).
The primary processing of the obtained data was carried out using the methods of descriptive and analytical statistics with the provision of results in the form of relative indicators (Р,%) with an error (m, p).
The research was intended to determine the characteristics of physical activity depending on food habits/preferences that are unfavorable for health. To compare the data in the selected groups, the methods of Student's coefficient and φ-test were used. To ensure statistical significance, the test was applied at a threshold value of 0.05.
3. RESULTS
The results of the research have been presented in two parts: in the first, the data on descriptive and analytical statistics are presented, and in the second, the characteristics of physical activity depending on food habits/preferences, which are not favorable for health, are described.
3.1. General Characteristics of Respondents
As part of the research, attention was paid to the issues of determining the characteristic features of the eating behavior of modern youth and their physical activity in the context of their consideration as possible factors in the formation of body weight disorders. Also, an analysis of literary sources was carried out regarding physiological, social, or other factors that influence the formation of food preferences or maladaptive eating behavior and related health disorders.
The issue of determining lifestyle features, other social determinants, and physiological features involved in the development of body weight disorders is highlighted in many scientific sources. Thus, it is determined that excessive consumption of caloric food can undermine the processes of self-regulation due to the impact on brain function and behavioral control. These changes may cause persistent maladaptive eating behaviors that underlie adult obesity and related metabolic syndromes [9].
Some studies have pointed to a person’s inability to maintain stable behaviours around palatable foods (high in sugar and fat) as one of the reasons for medical care inefficacy. These scientific publications highlight the link between binge eating behavior and neurotransmitter activity in certain brain regions involved in emotional behavior and reward circuitry. It is determined that dopaminergic activity is involved in the formation of executive skills that play an important role in social adaptation and behavioral control. The conclusions drawn in the publication remind us of the need to be aware of environmental and behavioral factors to better define the cognitive and emotional profile, which will contribute to improving the treatment of obesity in children [6].
Other researches suggest that measures of emotional eating and routine restraint are associated with activity in brain regions involved in urges and self-control. Even in the literature, the term emotional nutrition is used [10].
Therefore, in the conducted research, the questionnaire included various questions about diet, food preferences, and behavioral characteristics.
Thus, based on the respondents’ answers, only 29.0% of them were established to have a traditional diet of “breakfast, lunch, dinner”. The vast majority of students did not have a clear diet; the answers were as follows: “I always eat when I’m hungry” (28.8%) or “I often skip breakfast, eat at lunchtime and in the evening” (35.0%, Fig. 1).
Given the prevalence of “emotional eating”, the question “Do you eat tasty food when you are stressed or in a bad mood?” was included in the questionnaire. 35.0% of students gave an affirmative answer to this question. Only 25.0% of the responses of not using sweets during stress were found.
An important factor in the development of body weight disorders is a violation of the diet. The question that characterized the eating regimen concerned the frequency of eating immediately before going to bed. It was found that a fairly significant proportion (37.5%) of students had food right before going to bed, while 62.5% of respondents denied the existence of this habit.


An interesting question was regarding the usual place of eating. Thus, 51.2% of respondents indicated the “kitchen table/table in the dining room” as a usual place, while for 48.8% of students, the dining room was not a usual place for eating; 20.0% reported that they like to eat in front of the TV or by computer, and 28.8% did not state any specific place for eating at all (Fig. 2).
The obtained data can be evaluated as negative because some scientific results show that a longer time spent on social networks is indirectly related to an uncontrollable desire to eat due to increased impulsivity [11]. The risk of overeating increases when people experience moments of temporary inattention and loss of cognitive control while eating. Such overeating is defined as the consumption of a large amount of food within a limited period of time, with the accompanying feeling of loss of control [4].
During the survey, attention was paid to such peculiarities of nutrition as frequent visits to fast food establishments and preferences for products that are widely advertised. For example, fast food establishments, which mainly offer unhealthy food, usually rich in sugar and fat, were visited by the majority of medical students (57.5%), characterizing a lack of responsibility for one’s own health and the inability to become an example for patients on issues of eating behavior.
Enough scientific research has been dedicated to the issues of food advertising and the influence of social networks. Thus, it has been indicated that young people are increasingly exposed to social media and their image/video-based activities. They use these platforms to share advice in various areas, such as food and nutrition, recipe ideas, nutrition opinions, or specific diets. With the development of digital technologies, the prevalence of eating disorders among young people has been emphasized to grow [11-13].
Recently, Wilksch et al. [14] showed increased daily time spent on Instagram of adolescent girls to be associated with significant eating disorders. Similar violations were also determined among boys [15]. Also, there is growing evidence that social media and food advertising companies are using social media to spread their advertising.
According to the data of our research, the majority of respondents spent more than three hours a day watching TV and on the computer (78.8%).
The results of our survey regarding the use of products widely advertised on television or social networks were as follows: 8.8% of respondents preferred advertised products, 43.8% reported that they sometimes use products from advertising, and 47.5% of respondents reported not using the advertised products at all (Fig. 3).
In addition to a conscious, responsible attitude to food preferences, it is assumed that future doctors should also have the same attitude to physical activity. Besides that, they must take into account what WHO defines the fundamental mechanism of obesity and overweight as “energy imbalance between consumed and expended calories” [6, 16].
Therefore, a number of questions in our questionnaire were devoted to questions related to physical activity. According to the answers, only 13.8% of students reported performing morning physical exercises (gymnastics), the vast majority of respondents (47.5%) “did sometimes”, and 38.8% did not exercise in the morning at all (Fig. 4).


Only 32.5% of students practiced sports, while 51.2% indicated that they were physically active on weekdays (biking, moving, doing housework, etc.). 65.0% of medical students indicated that they often walk, and a significant number of students (67.5%) reported often climbing the stairs to the floors.
It is known that any habits, including eating behavior and physical activity, are formed in the family, reflecting either positive or negative experiences. Thus, 21.2% of students identified their parents’ weight as “above normal”.
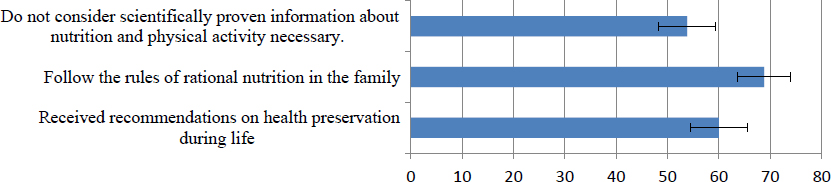
It is unfortunate to admit, but the statement of the WHO regarding the weakness of the preventive component of medical care in most of the world is valid. On the basis of the conducted questionnaire, it was determined that only 60.0% of students were given written or oral recommendations regarding proper nutrition and adequate physical activity during their lifetime. 62.5% had information about rational, healthy nutrition, and a little more, i.e., 68.8% of students believed that they followed the rules of healthy eating in the family; however, at the same time, a significant proportion (53.8%) of the respondents did not consider scientifically proven information about nutrition and physical activity to be necessary (Fig. 5).
3.2. Сharacteristics of Physical Activity Depending on Eating Habits/preferences not Favorable for Health
The conducted research also determined the peculiarities regarding physical activity among respondents in the presence of some maladaptive eating habits/preferences.
So, the questionnaire included a question about how often food was consumed immediately before going to bed. When determining the characteristics of physical activity, it was found that among those who ate food immediately before going to bed, the number of those who did not do morning gymnastics was twice higher in comparison to physically active students (56.7 ± 9.2% vs. 28.0 ± 6.4%, p ˂ 0.05; Table 1).
| Answer Options | Take Food Immediately Before Going to Bed | Do Not Take Food Immediately Before Going to Bed | General Result | ||
|---|---|---|---|---|---|
| - | n | Р, % ± m,p | n | Р, % ± m,p | |
| Yes, I do | 1 | 33,33 ±3,33 | 10 | 20 ± 5,71 | 11 |
| Sometimes I do | 12 | 40 ± 9,09 | 26 | 52 ± 7,13 | 38 |
| No, I do not do it | 17 | 56,7 ± 9,2 * | 14 | 28 ± 6,41 * | 31 |
| General result | 30 | 100,0 | 50 | 100 | 80 |
| Аnswer Options | I Visit Fast-food Establishments | I do not Visit Fast-food Establishments | General Result | ||
|---|---|---|---|---|---|
| n | Р, % ± m,p | n | Р, % ± m,p | ||
| Yes, I do | 38 | 82,6 ± 5,65 * | 21 | 61,8 ± 8,45 * | 59 |
| Sometimes I do | 3 | 6,5 ± 3,68 | 4 | 11,8 ± 5,6 | 7 |
| No, I do not do it | 5 | 10,9 ± 4,63 | 9 | 26,5 ± 7,67 | 14 |
| General result | 46 | 100 | 34 | 100 | 80 |
In the group of respondents who consumed delicious food “under stress”, only 39.3 ± 9.3% had physical activity on a weekday (cycling, physical games, physical housework) against 75.0 ± 9.9% of those who “did not eat” delicious food in stressful situations (p ˂ 0.05).
Among those who used products advertised on television, all (100.0%) respondents identified that they often climb stairs (versus 63.2 ± 7.9% not using products from advertising). They reported more often attending physical education classes in high schools (100% versus 63.2 ± 7.9% of those who did not use products from advertising).
Among students who visited fast-food establishments (pizzerias, etc.), there were significantly more students who attended physical education classes in higher school, i.e., 82.6 ± 5.6% versus 61.8 ± 8.4% (р ˂ 0.05) of those who did not have the habit of frequently visiting fast food establishments (Table 2).
In this group, the percentage of respondents whose parents’ weight was characterized as “normal, ordinary” was higher, i.e., 84.6 ± 5.3% versus 67.6 ± 8.1% of whom not attending institutions of this type (р ˂0.05), where a smaller number of parents with body weight “above normal” (13.0 ± 5.0% versus 32.4 ± 8.1%, p ˂ 0.01) was found. Among this same group of participants, the number of people with partial information about rational (healthy) nutrition was smaller (26.1 ± 6.5% versus 47.1 ± 8.6%, p ˂ 0.05).
Among students who defined their diet as “I often skip breakfast, eat at lunchtime and in the evening”, there were fewer who followed the rules of rational nutrition compared to respondents who had a traditional diet (breakfast, lunch, and dinner), i.e., 60.7 ± 9.4% against 89.7 ± 5.7%; p ˂ 0.01 (Table 3).
Respondents who did not have a strict diet in terms of time and frequency did not exercise in the morning more often (49.1 ± 6.8% vs. 21.4 ± 11.0%, p ˂ 0.01) than those who had regular meals, three times a day (Table 4).
Respondents of the group with a less strict diet more often reported doing physical exertion on weekdays than those with a regular diet in terms of frequency and time, respectively (56.4 ± 6.7% vs. 28.6 ± 11.4%; p ˂ 0.01, Table 5). A lower specific weight was found for those who followed the rules of rational/healthy nutrition in their families than those who did not (58.2 ± 6.7% versus 92.9 ± 7.1%, p ˂ 0.001).
| Аnswer Options | I Always Eat When Hungry | I Have Breakfast, Lunch, and Dinner | I Often Skip Breakfast, and Eat Lunch and Dinner | General Result | |||
|---|---|---|---|---|---|---|---|
| n | Р, % ± m,p | n | Р, % ± m,p | n | Р, % ± m,p | ||
| Yes, I do | 12 | 52,17 ± 10,64 | 26 | 89,65± 5,75 * | 17 | 60,71 ± 9,39 * | 55 |
| No, I do not do it | 11 | 47,82 ± 10,64 | 3 | 10,34 ± 5,7 | 11 | 39,28 ± 9,39 | 25 |
| General result | 23 | 100 | 29 | 100 | 28 | 100 | 80 |
| Аnswer Options | There is no Strictly Defined Regime (Absence of a Specific Time and Frequency of Eating) |
Eating At the Same Time Up to 3 Times a Day |
Eating At the Same Time More Often than Three Times a Day |
General Result | |||
|---|---|---|---|---|---|---|---|
| n | Р, % ± m,p | n | Р, % ± m,p | n | Р, % ± m,p | - | |
| Yes, I do | 6 | 10,90 ± 4,24 | 3 | 21,42 ± 11,38 | 2 | 18,18 ± 12,19 | 11 |
| Sometimes I do | 22 | 40 ± 6,66 | 8 | 57,14 ± 13,72 | 8 | 72,72 ± 14,08 | 38 |
| No, I do not do it | 27 | 49,09 ± 6,80 * | 3 | 21,42 ± 11,38 * | 1 | 9,09 ± 9,09 | 31 |
| General result | 55 | 100 | 14 | 100 | 11 | 100 | 80 |
| Аnswer Options | There is no Defined Regime (Absence of a Specific Time and Frequency of Eating) | Eating At the Same Time Up to 3 Times a Day | Eating At the Same Time More Often Than Three Times a Day | General Result | |||
|---|---|---|---|---|---|---|---|
| n | Р, % ± m,p | n | Р, % ± m,p | n | Р, % ± m,p | - | |
| Yes, I do | 31 | 56,36 ± 6,74* | 4 | 28,57 ± 12,52* | 6 | 54,54 ± 15,74 | 41 |
| Sometimes I do | 15 | 27,27 ± 6,06 | 8 | 57,14 ± 13,72 | 4 | 36,36 ± 15,21 | 27 |
| No, I do not do it | 9 | 16,36 ± 5,03 | 2 | 14,28 ± 9,70 | 1 | 9,09 ± 9,09 | 12 |
| General result | 55 | 100 | 14 | 100 | 11 | 100 | 80 |
Among the respondents who often ate in front of the TV or did not have a usual place for eating, fewer of them exercised on weekdays (25.6±7.1% vs. 4.9±3.4%, p˂0.05).
Thus, the significant features associated with maladaptive eating behavior have been found to be an absence of physical activity on weekdays, not performing morning gymnastics, and not observing the norms of rational nutrition in the family or having information about healthy nutrition.
4. DISCUSSION
There is a need to analyze the eating behavior of modern youth as a possible factor involved in body weight disorders, leading to the development of associated diseases. The peculiarities of the eating behavior of modern youth, found in this study, are as follows: non-compliance with the regime and having a multiplicity of meals, and having a reduced culture of eating (lack of a permanent place to eat, eating in front of a computer/TV). Moreover, such habits, like eating before going to bed, eating under stress, or frequently visiting fast food establishments, have been found to be widespread. A significant number of young people have been found to be prone to using advertised products. Also, young people’s awareness of healthy nutrition has also been found to be insufficient, with the level of physical activity among interviewed persons as unsatisfactory.
CONCLUSION
Eating behavior is one of the predictors of body weight disorders. In order to detect violations of the eating regime or food culture, it is advisable to conduct screening questionnaires on these issues both among adult students and school-age children, in order to be able to correct negative eating habits as early as possible. In order to increase the level of food consumption culture, it is necessary to introduce information/educational campaigns with the involvement of teachers, doctors, and mass media, and the use of printed information products. The knowledge of the expediency of a rational and calorically balanced diet, as well as the harm of fast food, should be a part of the informational activities of doctors and nutritionists. A significant number of respondents had a background of psycho-emotional stress (for example, exams), eating unhealthy food, and eating in stressful situations. Therefore, it can be stated that the mental health of young people is subject to control, especially against the background of recent events in Ukraine, which can be done by organizing and facilitating access of young people to “help lines” or psychological support groups. Ensuring accessibility to recreation or places for sports, by including them in the institutions of higher education, may contribute to an increased level of physical activity among young people.
It is advisable to conduct similar studies among students of other educational institutions or schools to determine the main trends regarding the level of physical activity and nutritional characteristics in order to develop and introduce educational programs for the formation of a responsible attitude to health at the regional or state level.
AUTHORS’ CONTRIBUTION
OVA, PTV, NVH, MNM, and PKH wrote sections of the manuscript. All authors have contributed to the manuscript revision and reading, and approved the submitted version.
ABBREVIATION
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The questions of the questionnaire, the research algorithm, and compliance with the rules for the preservation of personal data were considered at the meeting of the Commission on Ethics and Bioethics of the Kharkiv National Medical University (approval no. 1), dated January 12, 2021.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.

