All published articles of this journal are available on ScienceDirect.

Regional and Temporal Trends in the Prevalence of Musculoskeletal Disorders in the Iranian Elderly Population: Results from the Global Burden of Disease Study from 1990 to 2019
Abstract
Objectives
This study aimed to estimate temporal and regional trends in musculoskeletal disorders (MSDs) prevalence among the Iranian elderly population.
Methods
An ecological analysis of the Global Burden of Disease (GBD) dataset was conducted to examine the prevalence of MSDs among individuals aged 60–89 years. Joinpoint regression identified temporal changes, and ArcGIS mapped provincial prevalence in 2019.
Results
The trend analysis from 1990 to 2019 demonstrated the six-year period in which the highest annual percent change for prevalence of MSDs was reported in males (1990 to 1996: 0.392; [95% UI:0.376, 0.413]), females (1996-1999:1.512; [95% UI:1.423, 1.597]), and both sexes (1996-1999: 0.814; [95% UI: 0.755, 0.858]) of the whole population. Also, the regional analysis showed that the highest average annual percent change for prevalence of MSDs was in males (0.322; [95% UI: 0.301, 0.343]), in females (0.333; [95% UI: 0.320, 0.346]), and both sexes (0.341; [95% UI: 0.331, 0.352]) in Kohgiluyeh and Boyer-Ahmad Province. Finally, the highest prevalence of MSDs in 2019 was found in males (46377 to 51228 per 100,000), females (54342 to 62845 per 100,000), and both sexes (50410 to 54966 per 100,000) in Ardabil, Alborz, Tehran, and South Khorasan Provinces, respectively.
Discussion
The observed rise in the prevalence of MSDs reflects Iran’s population aging and potential lifestyle factors. Significant geographic disparities highlight the need for region-specific public health strategies.
Conclusion
This study reveals an upward trend in MSDs among Iran’s elderly. These findings necessitate evidence-based aging policies and targeted interventions for high-burden regions to address systemic health challenges.
1. INTRODUCTION
Reports demonstrated that more than 1.5 billion people were affected by musculoskeletal disorders (MSDs) worldwide in 2019 [1]. The most common MSDs include rheumatoid arthritis (RA), osteoarthritis (OA), low-back pain (LBP), neck pain (NP), and gout [2]. A sixth category of other MSDs is a wide range of diverse conditions affecting bones, joints, muscles, and connective tissues [3]. MSDs are usually associated with limitation of mobility and are known as the most common cause of chronic pain. Besides, population growth and aging contribute to the rising number of individuals living with MSDs [2]. The absolute burden of vertebral fractures has increased globally owing to population aging [4].
According to estimates in 2017, these disorders ranked 5th and 7th among all diseases worldwide and in the Eastern Mediterranean (EMRO) region. Also, the highest prevalence of LBP, Other MSDs, and NP has been obtained worldwide in the EMRO region. The highest risk of MSDs is related to females over the age of 30 in the EMRO region [5]. In general, studies in some provinces of Iran and across different occupational groups show a high prevalence of these disorders [6, 7]. Nevertheless, the overall prevalence of these disorders and trends is unavailable in Iran.
As life expectancy increases, the elderly population is growing, particularly in developing countries. MSDs are common in the elderly and are one of the causes of physical disability in these people [8]. Musculoskeletal disorders (MSDs) are a major cause of activity limitations, reduced functional capacity, and, consequently, a lower quality of life. They also impose substantial healthcare costs due to increased use of medical services and medications, as well as early retirement [9]. In developing countries such as Iran, there is a lack of accurate information on the prevalence rate and other epidemiological measures of MSDs in the elderly population.
The high prevalence of MSDs is a significant issue, along with the aging of the population. In developing countries, where healthcare systems and societies are not yet adequately prepared to address this growing need, awareness of its prevalence and accurate identification of the issue seem essential. Awareness of the prevalence and trend of these disorders will lead to the development of appropriate health policies and a program to promote health, especially in the elderly. As a result, this study aims to estimate trends in the prevalence of MSDs in the Iranian elderly population (60 to 89 years old) from 1990 to 2019.
2. METHODS
2.1. Study Area
Iran is part of the EMRO (Eastern Mediterranean Regional Office of the World Health Organization) and is geographically located in Western Asia. It is divided into 31 provinces. The population is about 84,000,000, and 50.5% are males and 49.5% are females [10].
2.2. Data Source and Processing
The data for this study were obtained from the Global Burden of Disease (GBD) dataset (2019), which is publicly accessible to researchers and provides annual estimates of measures such as prevalence across different sexes and age groups. The GBD study involves more than 10,000 collaborators from over 150 countries, along with 21 nations with subnational estimates. Data sources include vital registration systems, verbal autopsies, clinical informatics, household surveys, disease registries, censuses, and health service contacts. Iran is one of the countries with subnational estimates at the first administrative level. For this analysis, inclusion criteria encompassed individuals aged 60–89 years with valid and complete provincial and temporal data on MSDs in Iran between 1990 and 2019, while records outside this age range or lacking essential information were excluded [11, 12].
2.3. Trend Analysis
Joinpoint regression was used to identify changes in the prevalence trends of these disorders over time. All analyses were conducted using Joinpoint software, developed by the US National Cancer Institute for trend analysis. In this approach, the annual prevalence rates and their corresponding standard errors (SE) were used as inputs to the model. Annual percent changes (APC) were estimated along with their 95% confidence intervals (CI) for each identified segment of the trend. In addition, the average annual percent change (AAPC) was calculated for each province across different geographic regions.
Points at which statistically significant changes in trend occur are defined as joinpoints, dividing the time series into distinct segments. Trend variations between these joinpoints were assessed, and statistical significance was evaluated using the Monte Carlo permutation method [12].
3. RESULTS
In general, the APC for the prevalence of MSDs in Iran had an increasing trend during 1990–2019, except for the 2011–2014 period, when the prevalence had a small decreasing trend (Fig. 1). According to the joinpoint regression model, the trends in the APC for the prevalence of MSDs in Iran are displayed in Table 1. In males, the highest APC was observed during 1990–1996 (0.392 95% UI: 0.376, 0.413), and the lowest APC was seen during 2005–2011 (0.059 95% UI: 0.043, 0.076). In females, from 1996 to 1999, the highest APC for prevalence (1.512 95% UI: 1.423, 1.597) and the lowest APC (0.056 95% UI: -0.003, 0.104) were found during the 2005–2011 period. In both sexes, the highest APC was related to the 1996–1999 period (0.814 95% UI: 0.755, 0.858), and the lowest APC was related to the 2014–2019 period (0.091 95% UI: 0.063, 0.119).
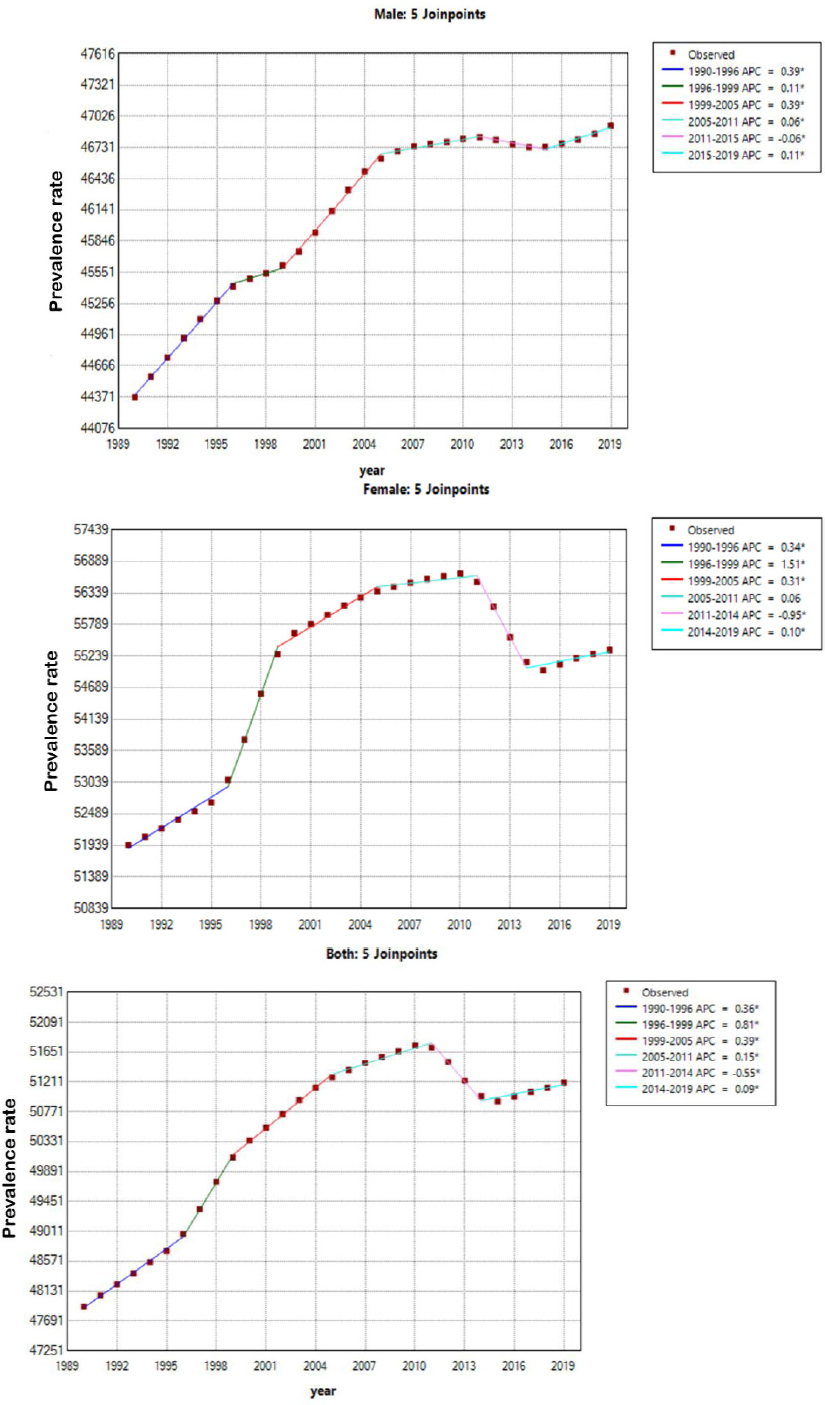
The annual percent change for prevalence of musculoskeletal disorders in Iran during the 1990–2019 period.
| Segment (Year Rzange) | Annual Percent Change (95% UI) | ||
|---|---|---|---|
| Male | Female | Both Sexes | |
| 1990-1996 | 0.392 (0.376, 0.413) | 0.341 (0.292, 0.393) | 0.360 (0.332, 0.386) |
| 1996-1999 | 0.106 (0.078, 0.163) | 1.512 (1.423, 1.597) | 0.814 (0.755, 0.858) |
| 1999-2005 | 0.390 (0.376, 0.407) | 0.312 (0.263, 0.374) | 0.391 (0.361, 0.418) |
| 2005-2011 | 0.059 (0.043, 0.076) | 0.056 (-0.003, 0.104) | 0.149 (0.123, 0.176) |
| 2011-2014 | -0.064 (-0.110, -0.031) | -0.953 (-1.030, -0.870) | -0.550 (-0.591, -0.510) |
| 2014-2019 | 0.110 (0.080, 0.164) | 0.101 (0.045, 0.155) | 0.091 (0.063, 0.119) |
The AAPC for the prevalence of MSDs in Iranian provinces during the 1990–2019 period is shown in Table 2. In males, Kohgiluyeh and Boyer-Ahmad Province established the highest AAPC (0.322 95% UI: 0.301, 0.343), while Tehran Province showed the lowest AAPC (0.067 95% UI: 0.063, 0.071). In females, Kohgiluyeh and Boyer-Ahmad (0.333 95% UI: 0.320, 0.346), and Qom (0.311 95% UI: 0.302, 0.321) provinces had the highest AAPC, and Tehran province had the lowest AAPC (0.078 95% UI: 0.076, 0.081). In both sexes, the highest AAPC was observed in Kohgiluyeh and Boyer-Ahmad (0.341 95% UI: 0.331, 0.352) and Lorestan (0.330 95% UI: 0.324, 0.336) provinces, and the lowest AAPC was observed in Tehran (0.076 95% UI: 0.068, 0.085) and Alborz (0.147 95% UI: 0.143, 0.152) provinces.
| Provinces | Average Annual Percent Change (95% UI) | ||
|---|---|---|---|
| Male | Female | Both Sexes | |
| Alborz | 0.115 (0.112, 0.119) | 0.158 (0.149, 0.166) | 0.147 (0.143, 0.152) |
| Ardebil | 0.244 (0.238, 0.249) | 0.270 (0.261, 0.281) | 0.304 (0.298, 0.309) |
| Bushehr | 0.186 (0.174, 0.199) | 0.231 (0.222, 0.241) | 0.229 (0.224, 0.235) |
| Chahar Mahal and Bakhtiari | 0.223 (0.217, 0.230) | 0.238 (0.230, 0.247) | 0.272 (0.265, 0.279) |
| East Azerbaijan | 0.102 (0.093, 0.110) | 0.220 (0.210, 0.230) | 0.191 (0.185, 0.197) |
| Fars | 0.267 (0.263, 0.272) | 0.289 (0.277, 0.301) | 0.298 (0.291, 0.305) |
| Gilan | 0.193 (0.190, 0.197) | 0.244 (0.232, 0.258) | 0.233 (0.225, 0.241) |
| Golestan | 0.102 (0.099, 0.106) | 0.175 (0.164, 0.186) | 0.170 (0.164, 0.176) |
| Hamadan | 0.241 (0.238, 0.245) | 0.287 (0.277, 0.297) | 0.294 (0.289, 0.300) |
| Hormozgan | 0.181 (0.153, 0.209) | 0.216 (0.203, 0.230) | 0.237 (0.230, 0.245) |
| Ilam | 0.193 (0.168, 0.219) | 0.212 (0.201, 0.223) | 0.257 (0.208, 0.306) |
| Isfahan | 0.129 (0.126, 0.132) | 0.182 (0.173, 0.191) | 0.161 (0.156, 0.165) |
| Kerman | 0.106 (0.101, 0.112) | 0.183 (0.169, 0.199) | 0.169 (0.159, 0.179) |
| Kermanshah | 0.141 (0.137, 0.145) | 0.178 (0.167, 0.189) | 0.205 (0.199, 0.211) |
| Khorasan-e-Razavi | 0.146 (0.143, 0.149) | 0.190 (0.182, 0.199) | 0.200 (0.195, 0.204) |
| Khuzestan | 0.233 (0.228, 0.237) | 0.300 (0.291, 0.310) | 0.283 (0.277, 0.288) |
| Kohgiluyeh and Boyer-Ahmad | 0.322 (0.301, 0.343) | 0.333 (0.320, 0.346) | 0.341 (0.331, 0.352) |
| Kurdistan | 0.157 (0.153, 0.163) | 0.231 (0.220, 0.243) | 0.235 (0.228, 0.241) |
| Lorestan | 0.276 (0.271, 0.283) | 0.291 (0.280, 0.303) | 0.330 (0.324, 0.336) |
| Markazi | 0.263 (0.260, 0.267) | 0.296 (0.287, 0.305) | 0.307 (0.301, 0.313) |
| Mazandaran | 0.241 (0.237, 0.244) | 0.192 (0.186, 0.199) | 0.248 (0.244, 0.253) |
| North Khorasan | 0.183 (0.180, 0.186) | 0.211 (0.200, 0.223) | 0.231 (0.225, 0.237) |
| Qazvin | 0.229 (0.224, 0.233) | 0.272 (0.264, 0.281) | 0.281 (0.275, 0.286) |
| Qom | 0.256 (0.252, 0.260) | 0.311 (0.302, 0.321) | 0.287 (0.282, 0.293) |
| Semnan | 0.261 (0.257, 0.264) | 0.288 (0.278, 0.298) | 0.291 (0.285, 0.297) |
| Sistan and Baluchistan | 0.133 (0.130, 0.137) | 0.183 (0.173, 0.193) | 0.202 (0.195, 0.209) |
| South Khorasan | 0.173 (0.169, 0.178) | 0.213 (0.202, 0.223) | 0.225 (0.220, 0.231) |
| Tehran | 0.067 (0.063, 0.071) | 0.078 (0.076, 0.081) | 0.076 (0.068, 0.085) |
| West Azerbaijan | 0.190 (0.186, 0.195) | 0.240 (0.230, 0.250) | 0.255 (0.249, 0.261) |
| Yazd | 0.268 (0.265, 0.271) | 0.304 (0.294, 0.316) | 0.286 (0.278, 0.294) |
| Zanjan | 0.240 (0.236, 0.244) | 0.291 (0.277, 0.306) | 0.308 (0.301, 0.315) |
| IRAN | 0.191 (0.188, 0.195) | 0.220 (0.211, 0.230) | 0.229 (0.224, 0.234) |
Based on the results of the geographical distribution, the prevalence of MSDs in 2019 is shown in Fig. (2). In males, the highest prevalence of MSDs in 2019 (46377 to 51228 per 100000) was in the provinces of Alborz, Tehran, Ardabil, North Khorasan, South Khorasan, Ilam, and Kermanshah and the lowest prevalence of MSDs (44230 to 45485 per 100000) was in the provinces of Sistan and Baluchistan, Kerman, Khuzestan, Qom, Kurdistan, Zanjan, Gilan and East Azerbaijan. In females, the highest prevalence of MSDs in 2019 (54342 to 62845 per 100000) was observed in Ardabil, Mazandaran, Alborz, Tehran, Isfahan, Yazd, and South Khorasan. The lowest prevalence of MSDs (52870 to 53843 per 100000) was in the provinces of East Azerbaijan, Zanjan, Gilan, Qom, Chaharmahal, Bakhtiari, Kohgiluyeh and Boyer Ahmad, Kerman, and Sistan and Baluchestan. Regarding both sexes, the highest prevalence of MSDs in 2019 (50410 to 54966 per 100000) was in the provinces of Ardabil, Mazandaran, Alborz, Tehran, North Khorasan, Razavi Khorasan, and South Khorasan, while the lowest prevalence of MSDs (48585 to 49733 per 100000) was in the provinces of East Azarbaijan, Gilan, Kurdistan, Qom, Chaharmahal and Bakhtiari, Kohgiluyeh and Boyer Ahmad, Kerman, and Sistan and Baluchistan.
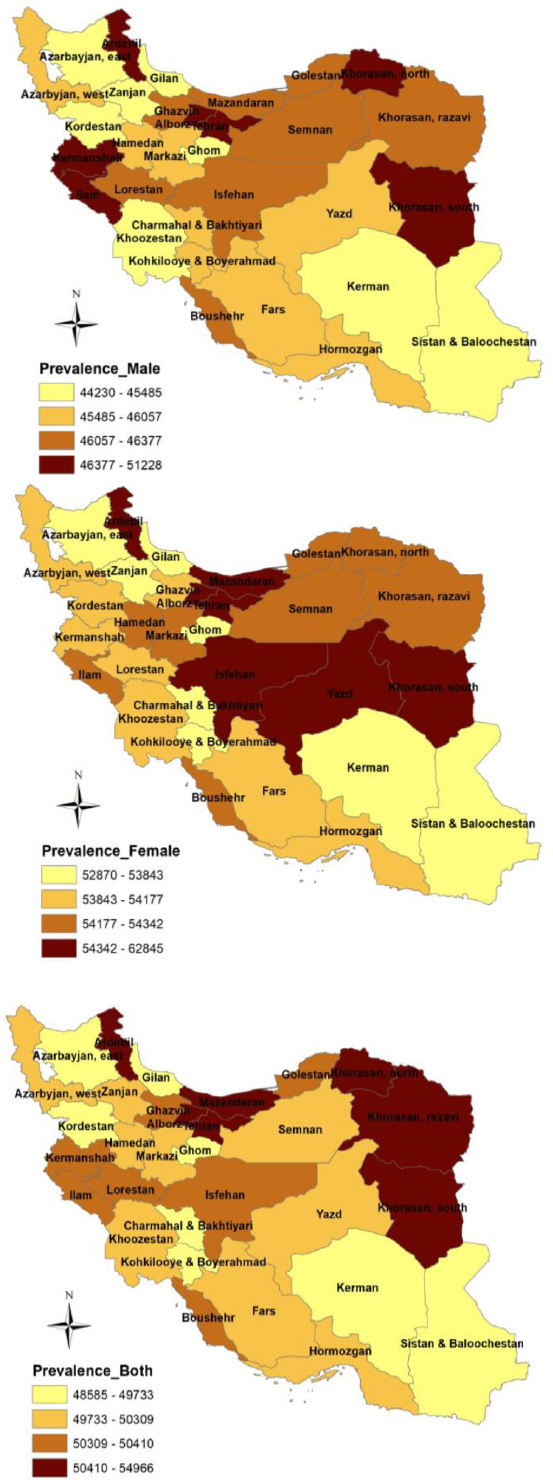
The geographic distribution for prevalence of musculoskeletal disorders by sex in Iran, 2019 (per 100,000 population).
4. DISCUSSION
To the best of our knowledge, this study provides the most recent and comprehensive estimates of regional and temporal trends for the prevalence of MSDs among the Iranian elderly population (aged 60 to 89 years), disaggregated by sex and province, from 1990 to 2019. Our results showed that, in general, the APC for the prevalence of MSDs in Iran increased from 1990 to 2019, except during 2011–2014. In males, the highest APC occurs from 1990 to 1996; in females and both sexes, it occurs from 1996 to 1999. The lowest APCs in females and males are observed during the 2005-2011 period and in both sexes from 2014 to 2019. For males, females, and both sexes, the highest AAPC for MSD prevalence is in Kohgiluyeh and Boyer Ahmad Province, and the lowest is in Tehran Province.
Few studies have investigated temporal trends in MSD prevalence; therefore, results cannot be directly compared. A study across the Middle East and North Africa region showed an increase in the age-standardized prevalence rate from 1990 to 2019 [13]. Also, a study in Mexico revealed a significant increase in the prevalence of MSDs from 1990 to 2019 [14]. A study in China showed that the AAPC for the prevalence between 1990 and 2017 for RA, OA, NP, and gout had an increasing trend and a decreasing trend for LBP [15]. Likewise, a study in Latin America and the Caribbean reported the growing trend in the AAPC for the prevalence of other MSK (other than RA, OA, gout, LBP, and NP) from 1990 to 2019 [16]. The results of another study investigating the AAPC for the prevalence trend of knee osteoarthritis in Finland showed an upward trend from 1996 to 2015 [17].
There are several possible explanations for the increasing prevalence trend in our study. Obesity and insufficient physical activity are the individual risk factors for MSDs [18]. With the progression of urbanization in Iran, there has been a significant increase in the prevalence of obesity and overweight among the elderly [19], alongside rising levels of insufficient physical activity and sedentary behavior [20]. Another contributing factor may be the increase in life expectancy and population aging, driven by a decline in premature mortality in Iran [21]. However, the cause of these increases may be improved healthcare coverage, leading to better recording and reporting of MSDs.
Our results revealed that, for males, females, and both sexes, Ardabil, Alborz, Tehran, and South Khorasan provinces have the highest prevalence, and East Azerbaijan, Kerman, Sistan and Baluchistan, Qom, and Gilan have the lowest prevalence of MSDs in 2019. There are limited studies on the prevalence of MSDs in the elderly in different provinces of Iran. A study in northwest Iran on people aged 35 to 70 years reported a very high prevalence of MSDs in 2014 [22]. Another study in the rural areas of northwestern Iran showed a very high prevalence of rheumatic complaints in rural areas of Iran [23]. A study in the southeast of Iran on people aged 15 and older revealed a high prevalence of MSDs, with knee osteoarthritis [5].
Stress, anxiety, and psychological factors are risk factors leading to MSDs, and the high prevalence of these factors in the elderly in Ardabil, Tehran, and South Khorasan provinces can be one of the reasons for the high prevalence of MSDs [24-27]. Ergonomic risk factors constitute a major portion of the risk factors [18]. Additionally, the level of employment is higher in cities, and in provinces with a higher level of urbanization, a higher prevalence of MSDs is expected. Tehran and Alborz are among the provinces with the highest level of urbanization. Also, Sistan and Baluchistan, and Kerman are among the provinces with the lowest level of urbanization, which can partly explain the MSDs prevalence rate in these provinces [28].
Considering the growth of the elderly population in developing countries like Iran, it is important to consider the outcomes of a high prevalence of MSDs and effective health policy. These disorders can result in diagnostic and treatment costs for both individuals and society, the reduction of workforce productivity, and absenteeism. It is recommended to conduct extensive research on the elderly and to devise national health programs that increase awareness and promote healthy lifestyles, prevention, and rehabilitation care within Iranian society. Future trend studies can be enhanced by applying Bayesian meta-regression and Das Gupta decomposition methods, in line with GBD approaches [29].
5. STRENGTHS AND LIMITATIONS
To the best of our knowledge, this is the first study to examine temporal trends in the prevalence of musculoskeletal disorders (MSDs) among the elderly population in Iran, stratified by sex and province. Given the increasing life expectancy and rapid population aging in Iran, these findings provide important insights for identifying strengths and gaps within the national healthcare system.
The analysis was based on data from the Global Burden of Disease (GBD) database, which covers large and relatively representative populations. However, several limitations should be acknowledged. First, this study is purely descriptive and focuses on temporal trends without incorporating potential explanatory variables or predictors. Therefore, it does not identify underlying determinants of observed changes, limiting interpretation to descriptive epidemiology. Second, causal relationships were not assessed; thus, observed associations should not be interpreted as causal, and any related factors may represent consequences rather than drivers of MSD trends.
Third, potential bias may arise from heterogeneity in data sources and methodologies used in the GBD database, including measurement error, underreporting, and the absence of primary data in some settings. The quality and completeness of GBD inputs vary across countries and regions depending on data availability and research investment [12]. In Iran, limitations in systematic registry systems may further affect the accuracy of national and subnational estimates.
In addition, the relatively small population aged 90 years and older, along with limited data availability for this age group, may have led to underestimation of MSD prevalence among the oldest-old. Finally, the observed decrease in the annual percent change (APC) between 2011 and 2014 is not supported by clear epidemiological evidence and may reflect methodological updates within the GBD modeling process; therefore, this finding should be interpreted with caution.
CONCLUSION
The findings of this study indicate an increasing trend in the prevalence of musculoskeletal disorders among the Iranian elderly population from 1990 to 2019. This pattern is likely influenced by population aging, as well as lifestyle, occupational, and environmental factors. In 2019, Ardabil, Alborz, Tehran, and South Khorasan provinces showed the highest prevalence rates, highlighting important geographic disparities that require targeted public health interventions.
These results underscore the need for policymakers and public health authorities to develop evidence-based strategies focused on the prevention, early detection, and effective management of MSDs among older adults. In this context, the implementation of community-based rehabilitation programs may play a key role in improving functional status and enhancing the quality of life of the elderly population in Iran.
AUTHORS' CONTRIBUTIONS
All authors participated in this study; M.T.S.: is the principal investigator and the main author, who supervised the study; M.T.S., F.S.S., and V.B.: Analyzed the data and wrote the final draft of the manuscript; V.B., M.T.S., and F.S.S.: revised and approved the manuscript before submission. The authors read and approved the final manuscript.
LIST OF ABBREVIATIONS
| AAPC | = Average annual percent change |
| APC | = Annual Percent Change |
| EMRO | = Eastern Mediterranean |
| GBD | = Global Burden of Disease |
| LBP | = Low-Back Pain |
| MSDs | = Musculoskeletal Disorders |
| NP | = Neck Pain |
| OA | = Osteoarthritis |
| RA | = Rheumatoid Arthritis |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Research Ethics Committee of Shahid Sadoughi University of Medical Sciences, Iran, with the Ethical ID IR.SSU.SPH.REC. 1403.070.
CONSENT FOR PUBLICATION
Not applicable. This study was conducted with aggregated data (without personal information).
AVAILABILITY OF DATA AND MATERIALS
The datasets are freely available in the Global Burden of Disease Study (GBD) repository, [https://vizhub. healthdata.org/gbd-results/].
ACKNOWLEDGEMENTS
I would like to thank the Institute for Health Metrics and Evaluation (IHME) for available the data for research.

