All published articles of this journal are available on ScienceDirect.

Patients’ Experiences Regarding the Nursing Care of Dual Diagnosis: A Qualitative Study
Abstract
Background/Introduction
Studies have shown that the needs of patients with dual diagnosis are complex, and that professional nurses providing effective nursing care to them require specialized knowledge, skills, and attitudes. However, research on the experiences of patients diagnosed with dual diagnosis regarding nursing care is limited, and their experiences are unknown in Ghana. The purpose of this study was to explore and describe the experiences of patients diagnosed with dual diagnosis regarding the nursing care they receive in psychiatric hospitals in Ghana.
Methods
An exploratory-descriptive qualitative research design was used to conduct this study. Sixteen participants with dual diagnoses were recruited for the study. A purposive sampling technique was used to select potential participants. Individual, semi-structured interviews were used to collect data from the patients. The researcher and co-coder independently used thematic analysis to analyse the data.
Results
Three main themes emerged, namely (1) patients’ experiences of nursing care rendered at psychiatric units, (2) challenges experienced by patients diagnosed with dual diagnosis, and (3) recommendations for improving care of patients diagnosed with dual diagnosis.
Discussion
The findings stress the dual reality of psychiatric nursing care for patients with dual diagnosis, marked by both positive experiences of holistic, supportive interventions and negative experiences shaped by stigma, structural barriers, and lack of collaboration. The study highlights the urgent need for systemic reforms, including capacity building for staff, infrastructural improvements, patient-centred practices, and integration of recovery-oriented models. By addressing these gaps, psychiatric nursing care could shift closer to a model that fully respects the dignity, autonomy, and holistic needs of individuals with dual diagnosis, thereby enhancing both clinical outcomes and patient satisfaction.
Conclusion
Patients with dual diagnosis experience both supportive, holistic nursing care and systemic challenges in psychiatric hospitals in Ghana. Positive therapeutic engagement fosters recovery, yet negative attitudes, limited involvement, and poor infrastructure hinder recovery. Integrating clinical competence, empathy, patient autonomy, and adequate environments is vital for achieving sustainable, patient-centred rehabilitation outcomes.
1. INTRODUCTION
Dual diagnosis or co-occurring disorders are commonly accepted terms used within the mental health profession to refer to patients suffering from mental disorders and substance use disorders [1-3]. This condition can occur simultaneously or sequentially, making the relationship complex [4]. Persons with this diagnosis face numerous challenges, such as increased risk of nonadherence and suicidal thoughts [5] and other health conditions. The problematic use of alcohol and other substances in tandem with the mental disorder is also correlated to poor outcomes [6], including relapse, more psychiatric symptoms, high risk of suicide [5], readmissions, and dropouts [7].
Clinical services for this population are offered in an inpatient setting with high rates because they are ongoing and varied, including crisis interventions, psychotherapy, family therapy, and detoxification [8, 9]. Nursing care is one of the many complex demands of this group, which calls for specialised knowledge and clinical skills [10-12]. Professional assistance, standardised training, and additional education for nurses are necessary to meet the set of competences required to deliver successful nursing care [13, 14]. Proposed therapy paradigms include integrated and non-integrated treatment, with the integrated paradigm claiming to be better than the other.
A systematic review showed that integrated treatment yielded significantly greater reductions in psychiatric symptomatology, particularly PTSD symptoms, compared to non-integrated treatment. Non-integrated and integrated treatment elicited comparable results between-group improvement in substance use symptomatology. Meanwhile, integrated and non-integrated treatments elicited similar retention rates. However, non-integrated treatment was specifically observed to significantly improve completion rates compared to integrated treatment [8]. There are resources available in guiding the patient care, but these resources provide generic direction for clinicians, and none are specifically designed for nurses providing hospital-based care [2, 9, 10].
A literature search identified two studies that explored nursing care from the perspective of inpatients with dual diagnosis. The first, a qualitative descriptive study (n = 12), reported that patients perceived nursing care as encompassing the fulfilment of physical needs such as nutrition, hygiene, and mobility; the promotion of psychosocial well-being through structured activities, recreational opportunities, facilitation of family visits, and provision of information and support to families. This study also focuses on addressing substance use by enforcing hospital rules, prohibiting drugs and alcohol, and dispensing prescribed medications. In tandem, the study recommends delivering humane and humanising care, characterised by dual diagnosis patients being treated with dignity and having their feelings acknowledged [12].
The second study, using a phenomenological– hermeneutical approach (n = 5), highlights the importance of caring conversations. Participants described reciprocity that fostered safety and trust, as well as honesty, respect, and a sense of connection with nurses. This second study recommends recognition of suffering, whereby patients were offered compassionate presence, attentive listening, and shared humanity. Such care culminated in the restoration of self-esteem through respecting dual diagnosis patients as human beings rather than reducing them to their substance use, which in turn promoted dignity and recovery [13].
Together, these studies underscore the critical role nurses play in shaping the quality and outcomes of care for patients with dual diagnosis. However, as both were conducted in developed countries, their findings may not be directly generalisable to the context of developing countries such as Ghana.
The above information shows that nursing care for patients with dual diagnosis is limited, and the experiences of patients regarding the nursing care in Ghana are yet to be systematically explored. Responding to the question, “What are the experiences of patients regarding the nursing care received in Ghana?”, this empirical study fills this gap. Therefore, the aim is to explore and describe the experiences of patients with dual diagnosis regarding the nursing care they receive in Ghana’s psychiatric hospitals.
2. METHODOLOGY
2.1. Study Design
An exploratory-descriptive qualitative research design [14] was employed to explore and describe the experiences of patients diagnosed with dual diagnosis concerning the nursing care they receive in psychiatric hospitals in Ghana. This approach was informed by the epistemological assumption that patients themselves are experts in their care needs and can provide valuable insight into the quality and nature of nursing care [15]. Braun and Clarke's thematic analysis approach was used to analyse data [16, 17].
2.2. Setting
This study was carried out in Ghana’s three major public psychiatric hospitals, referred to as Hospitals A, B, and C. All three are tertiary-level facilities that also function as teaching hospitals, offering mental health training opportunities for medical, nursing, and allied health students. The patient population in these hospitals ranges between 140 and 220. The medical, nursing, and allied health staff deliver care to individuals with diverse mental health conditions from across Ghana and neighbouring countries. Each hospital has a rehabilitation unit that provides specialised treatment for alcohol and substance use disorders; however, none of the facilities have a dedicated unit specifically for patients with dual diagnosis.
2.3. Sample and Recruitment Process
Data collection commenced following ethical approval from the North-West University Health Research Ethics Committee [HREC](NWU-00038-24-A1), the Ghana Health Service (GHS-ERC 005/07/24), and the ethics committees of the participating hospitals. Participants were eligible for inclusion if they met the following criteria: had a documented history of both mental illness and substance use; were on admission in the three psychiatric hospitals; were able to communicate in English or Asante Twi (local language); were 18 years of age or older; provided voluntary consent through signing a consent form; were in their full faculty at the time of recruitment; were either approaching discharge or discharged but awaiting final departure; and had been recommended by a psychiatrist or clinical psychologist or nurse manager.
Recruitment was conducted over a three-month period, from October 2025 to January 2025. During this time, the researcher maintained regular contact with hospital clinical coordinators and nurse managers, who played a central role in identifying eligible patients. Nurse managers assisted by suggesting inpatient units with potential participants with dual diagnosis. To support the recruitment process, the researcher prepared written summaries of the study for patients and distributed informational pamphlets to those selected. Patients who expressed interest in receiving more information were referred to the researcher for individual meetings held within the hospital wards.
At these meetings, the researcher introduced himself as a doctoral candidate in Health Sciences with a specialization in Nursing Science at the Mafikeng Campus of the North-West University and provided detailed explanations of the study's purpose, process, and expectations. A purposive sampling technique was employed, accounting for demographic considerations over time to maximise diversity across gender, age, years of admission, ward/unit, and other relevant factors. A total of 16 patients agreed to be contacted by the researcher after individual meetings on separate days and times. Ultimately, 16 were enrolled in the study. The following research questions were asked to elicit data from the participants:
- What are your experiences regarding how you are currently receiving care from the nurses?
- What are the challenges you are experiencing as a patient diagnosed with dual diagnosis?
- What can be done to improve how you are currently receiving care from the nurses?
- What can be included in the guidelines regarding how the nurses should care for you?
2.4. Data Collection
Data were collected through face-to-face individual interviews supplemented with field notes from patients who voluntarily participated in the study. Interviews were conducted in English and Twi (the local language in Ghana), depending on participants’ language preference, to ensure clarity and depth of expression. All interviews took place in designated rooms within the hospital wards that were convenient and ensured privacy for participants. Each interview lasted a minimum of 30 minutes. Data collection continued until data saturation was achieved, confirmed by two additional interviews, resulting in a total of 16 interview sessions. A 17th participant was not interviewed because, after agreeing to participate, he changed his mind and demanded a huge sum of money before granting the interview. Field notes were maintained throughout the data collection process to capture contextual observations, non-verbal cues, and the researcher’s reflective insights. The data collection methods were congruent with the study aim and were designed to elicit participants’ needs, perspectives, and lived experiences of nursing care for dual diagnosis.
2.5. Researcher Positionality
The researcher acknowledges that his professional background, academic training, and personal perspectives may have influenced various stages of the research process, including study design, data collection, analysis, and interpretation. As a registered mental health nurse and doctoral candidate in Nursing Science, the researcher occupied both insider and outsider positions. The insider position was informed by prior clinical experience within mental health settings and sustained engagement with patients experiencing psychiatric and substance use disorders. This background provided contextual sensitivity to the clinical environment, professional culture, and complexities of mental health care delivery in Ghana, thereby facilitating rapport and open communication with participants. However, the researcher recognised that this familiarity could also introduce assumptions or preconceptions. To mitigate potential bias, the researcher deliberately adopted an outsider stance by maintaining a critical and reflective orientation throughout the study. Conscious efforts were made to bracket prior knowledge and allow participants’ narratives to emerge authentically. The researcher was also attentive to how his professional status and academic role might influence participants’ responses and took steps to minimise power imbalances during interviews.
2.6. Reflexivity
Reflexivity was an ongoing and integral component of the research process [18]. The primary researcher (FN) continuously examined how his professional identity as a registered mental health nurse, academic role as a lecturer, and experience in qualitative research might shape interactions with participants and the interpretation of data. Recognising the dual role of clinician and researcher, deliberate efforts were made to balance empathic engagement with analytical distance. Reflective journaling was used consistently to document assumptions, emotional responses, and methodological decisions. Regular reflective discussions with supervisors further supported critical examination of how positionality influenced data collection and meaning-making. This reflexive practice created space for participants’ voices to be foregrounded and reduced the imposition of researcher-driven interpretations.
2.7. Trustworthiness
Multiple strategies were employed to ensure the trustworthiness of the study, addressing credibility, dependability, confirmability, transferability, and reflexivity [19]. Credibility and auditability were enhanced through prolonged engagement in the study settings, which facilitated rapport building and elicited rich, detailed accounts from participants. Comprehensive records were maintained, including audio recordings, verbatim transcripts, field notes, and coding documentation. Field notes were recorded immediately after interviews and cross-checked against audio recordings to ensure accuracy. Peer debriefing with academic supervisors and colleagues provided opportunities for critical reflection and validation of emerging interpretations. Dependability was ensured through a systematic, transparent, and well-documented research process [20]. A detailed audit trail was maintained, capturing each stage of the study from data collection to analysis and interpretation. Interview guides, reflexive journals, and field notes were retained to allow external scrutiny of methodological decisions. Consistent use of guiding interview questions supported methodological coherence across participants. To enhance confirmability, the researcher actively minimised personal bias by maintaining neutrality during interviews and analysis [21]. Reflexive journaling supported continuous self-monitoring of assumptions and interpretive decisions, while peer review of emerging themes ensured that findings were grounded in participants’ accounts rather than researcher predispositions. Transferability and authenticity were addressed through the provision of rich, thick descriptions of the study context, participant characteristics, and healthcare settings [19, 21]. Detailed contextual reporting enables readers to assess the applicability of the findings to similar settings and populations.
2.8. Data Analysis
Data were analysed using Braun and Clarke’s six-phase thematic analysis, which provides a systematic and flexible approach for identifying, analysing, and reporting patterns within qualitative data [16, 17]. This method was considered appropriate for exploring and interpreting patients’ lived experiences of nursing care for dual diagnosis within psychiatric settings. The first phase involved familiarisation with the data. All interviews were transcribed verbatim to ensure accuracy and preserve the depth of participants’ accounts. The researcher and an independent co-coder read and re-read the transcripts independently and at different times to gain an in-depth understanding of the content, context, and nuances of patients’ experiences [16]. During this phase, initial notes and observations were made to capture early impressions, significant statements, and recurring ideas related to nursing interactions, care practices, and perceived support. Next, initial codes were generated systematically across the dataset. Segments of data that reflected meaningful aspects of patients’ experiences, such as communication with nurses, emotional support, stigma, involvement in care, and responsiveness to needs, were identified and labelled. Coding was largely inductive, allowing codes to emerge directly from participants’ narratives [17]. The next phase involved searching for themes, during which related codes were collated into broader patterns of meaning. Codes capturing similar experiences were grouped together to form potential themes that reflected shared perceptions of nursing care among patients with dual diagnosis. These preliminary themes represented key dimensions of patients’ experiences, including perceived quality of care, relational dynamics, and barriers to effective support. In the fourth phase, themes were reviewed and refined to ensure coherence and distinctiveness. This involved checking that the themes accurately represented the coded data and the dataset as a whole. Some themes were merged, others were refined into subthemes, and those lacking sufficient supporting data were discarded. This iterative process was conducted collaboratively between the researcher and the independent co-coder to enhance analytic rigour and credibility. The researcher's supervisors were available to resolve any discrepancies in coding; however, no issues of consensus arose. The fifth phase focused on defining and naming themes. Each theme was clearly articulated to capture its essence and relevance to patients’ experiences of nursing care for dual diagnosis. Theme names were carefully chosen to reflect participants’ voices while maintaining analytical clarity and alignment with the study objectives. A thematic map shown in Fig. (1) was developed to illustrate the hierarchical relationship between the central phenomenon, overarching themes, and sub-themes, demonstrating the progression from raw data to analytically meaningful categories.
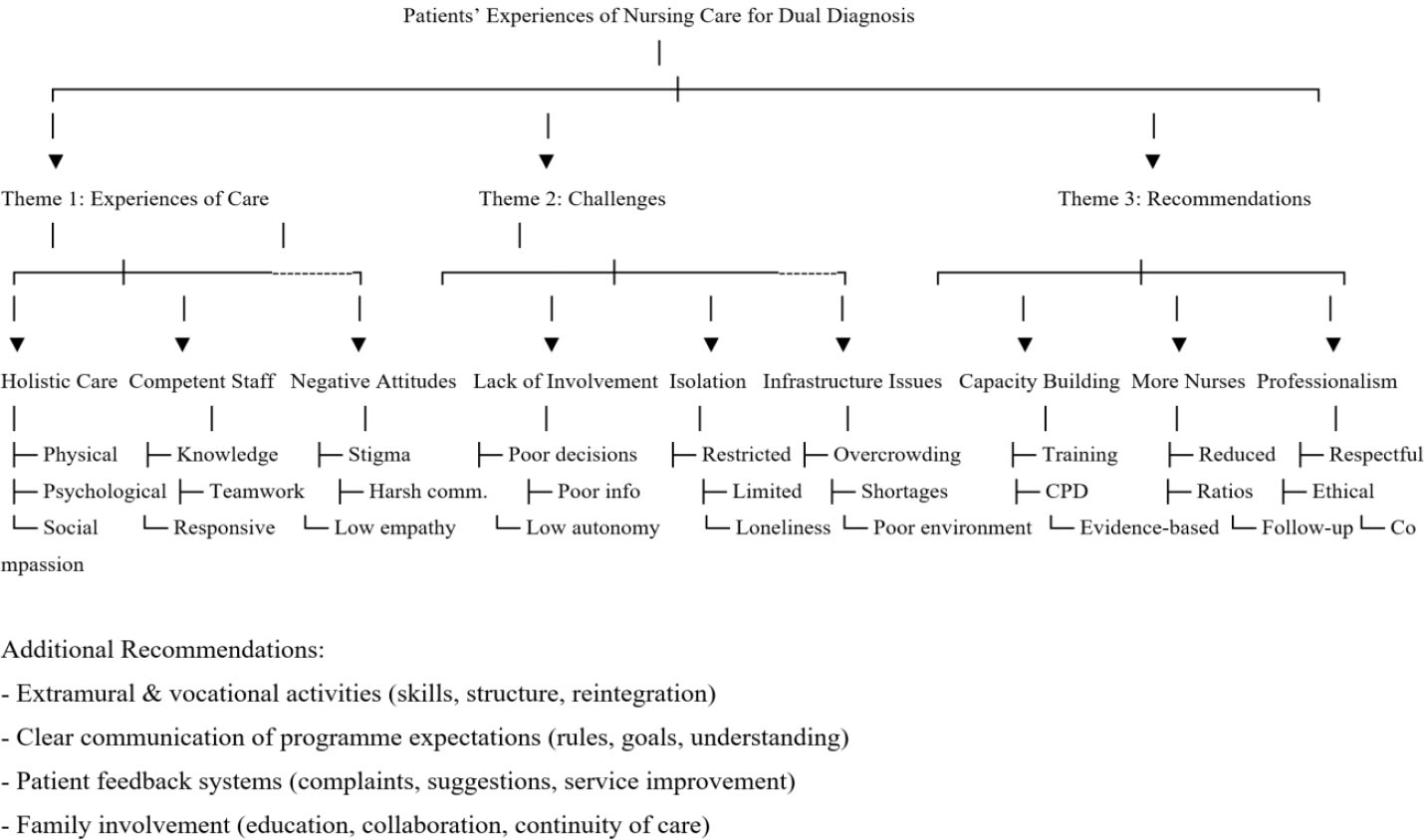
Thematic map.
The final phase involved producing the report, where the themes were woven into a coherent analytic narrative. Direct quotations and vignettes from participants were used to illustrate key findings, enhance transparency, and give voice to patients’ lived experiences. The final themes were reviewed against the research objectives to ensure consistency and analytic depth. This rigorous and transparent process strengthened the trustworthiness of the findings and ensured that the analysis was firmly grounded in the data [16, 17].
2.9. Ethical Considerations and Consent to Participate
The study was approved by the North-West University Scientific Review Committee and the Health Research Ethics Committee [HREC] (NWU-00038-24-A1), as well as by the Ghana Health Service Ethics Review Committee, which provided the country-specific ethical approval (GHS-ERC 005/07/24). We followed the Helsinki declaration during the research process. Written informed consent was obtained from the nurses who participated in the study. To protect participants’ privacy, all information was gathered and kept in a secure, anonymised database. Participation was entirely voluntary, with assurances of both confidentiality and anonymity. The data were safely stored, and access was restricted solely to authorised personnel.
3. RESULT
3.1. Participant Demographics
A total of 16 participants took part in the study, comprising 14 males and 2 females. Participants’ ages ranged from 18 years to above 40 years. One participant was aged 18–25 years, two were aged 26–30 years, three were aged 31–35 years, five were aged 36–40 years, and five were aged above 40 years. Regarding employment status, 10 participants were employed, while 6 were unemployed at the time of the study. In terms of educational background, 4 participants had completed primary education, 4 had secondary education, 3 had obtained a Diploma, 3 held a Bachelor’s degree, and 2 had attained a Master’s degree. Regarding substance use, alcohol (n=8) and cannabis (n=9) were the most commonly reported substances. Other substances used included cocaine (n=4), heroin (n=2), pethidine (n=1), opioids (n=1), and tramadol (n=1). Participants were also diagnosed with a range of psychiatric conditions. These included recurrent depressive disorder (n=1), mental and behavioural disorder (n=4), psychotic disorder (n=1), bipolar disorder (n=1), mania without psychotic disorder (n=1), schizophrenia (n=1), psychotic disorder and schizophrenia (n=1), depression (n=1), delusional disorder (n=1), severe depression with suicidal intent (n=1), and psychotic disorder with bipolar disorder (n=1). Table 1 displays the psychiatric disorders of the participants.
| No. | Identifier | Gender | Age (years) | Education | Employment Status | Length of Stay (days) | Diagnosis | Hospital |
|---|---|---|---|---|---|---|---|---|
| 1 | 0001P1 | Male | Above 40 | Primary | Employed | 31-60 | ii. Alcohol use disorder ii. recurrent depressive disorder | Hospital A |
| 2 | 0001P2 | Female | Above 40 | Primary | Unemployed | More than 90 | i. Mental and behavioural disorder due to the use of cannabinoids): Harmful use ii. Recurrent depressive disorder |
Hospital A |
| 3 | 0001P3 | Male | Above 40 | Secondary | Unemployed | More than 90 | Mental and Behavioural disorder due to the use of alcohol | Hospital A |
| 4 | 0001P4 | Male | 26-30 | Secondary | Unemployed | 14-30 | Mental and Behavioural disorder due to multiple drug use (alcohol, cannabis, opioids) | Hospital A |
| 5 | 0001P5 | Male | 3I-36 | Diploma | Employed | 14-30 | Cannabis abuse with psychotic disorder unspecified | Hospital A |
| 6 | 0001P6 | Male | 18-25 | Secondary | Employed | 14-30 | Mental and behavioural disorders due to multiple substance use (cannabis, tramadol, cigarettes) | Hospital A |
| 7 | 0002P1 | Male | 36-40 | Master’s | Employed | More than 90 | I. Substance use disorder (alcohol) ii. Bipolar affective disorder |
Hospital B |
| 8 | 0002P2 | Male | 36-40 | Diploma | Unemployed | 61-90 | I. Cannabis Abuse Uncomplicated. ii. Mania without psychotic symptoms |
Hospital B |
| 9 | 0002P3 | Male | 36-40 | Master’s | Unemployed | More than 90 | I. Cannabis induced psychotic disorder. ii. Bipolar disorder |
Hospital B |
| 10 | 0002P4 | Male | 36-40 | Primary | Unemployed | More than 90 | I. Multiple substance dependence (cannabis, cocaine &heroin). ii. Depression |
Hospital B |
| 11 | 0002P5 | Male | Above 40 | Diploma | Employed | More than 90 | i. Alcohol dependence ii. Alcohol induced delusions |
Hospital B |
| 12 | 0002P6 | Female | 31-36 | Bachelor’s degree | Employed | More than 90 | i. Severe depression with suicide intent ii. Pethidine abuse |
Hospital B |
| 13 | 0002P7 | Male | Above 40 | Secondary | Employed | 60-90 | Schizophrenia with co-morbid substance use (alcohol, cannabis, cocaine, heroin, tobacco) | Hospital B |
| 14 | 0003P1 | Male | 31-36 | Bachelor’s degree | Employed | 31-60 | Mental and behavioural disorder due to multiple substance use (cannabis and cocaine) | Hospital C |
| 15 | 0003P2 | Male | 26-30 | Bachelor’s degree | Employed | 14-30 | Schizophrenia and multiple substance use (alcohol, cannabis, and cocaine) | Hospital C |
| 16 | 0003P3 | Male | 36-40 | Primary | Employed | 61-90 | Substance (alcohol) induced psychotic disorder and schizophrenia | Hospital C |
3.2. Findings
Three main themes and fourteen sub-themes emerged from the findings of the study, namely (1) patients’ experiences of nursing care rendered at the psychiatric units, (2) challenges experienced by patients diagnosed with dual diagnosis, and (3) recommendations for improving care for patients diagnosed with dual diagnosis. Table 2 presents the main themes and sub-themes. These themes and sub-themes are supported by literature in the following section.
| Theme | Sub-themes |
|---|---|
| Theme 1: Patients’ experiences of nursing care rendered at the psychiatric units | • Care is holistic in nature • Care is rendered by competent nurses and supportive staff • Patients experience negative attitudes from some staff members |
| Theme 2: Challenges experienced by patients diagnosed with dual diagnosis | • Lack of patient involvement in care • Isolation from family • Poor infrastructure and inadequate resources • Poor food quality |
| Theme 3: Recommendations for improving care for patients diagnosed with dual diagnosis | • Continuous capacity building and upskilling of nurses on the management of dual diagnosis • Employing more nurses for continuity of care • Enhanced professionalism among nurses • Provision for extramural activities and vocational training • Improved communication of programme expectations • Provision for patient complaints and suggestions on the programme • Family involvement in rehabilitation programmes |
3.2.1. Theme 1: Patients’ Experiences of Nursing Care Rendered at the Psychiatric Units
Participants gave their account of nursing care rendered as holistic in nature, rendered by competent and supportive staff. However, some participants recounted experiencing negative attitudes from some staff members.
3.2.1.1. Care is Holistic in Nature
Participants recounted that the care they experience is holistic in nature:
“Okay, so, finely is average. So, the average person would say, they give me my medications when they have to. They make sure things are done the way they are supposed to be done for me. They make sure my primary needs are attended to. They make sure... They help with addressing any other issues I have. So, being finely taken care of is more or less being done to my expectation” (Hospital B, participant 4).
This view was endorsed by Participant 1 at Hospital C:
“Yeah, they actually take care of our well-being, they make sure that we maintain hygiene, that we are well-kept, we are well-fed, and I think the hospitality to us is okay. Where we sleep, where we take our showers, where we ease ourselves, I think it's satisfactory” (Hospital C, participant 1)
Participant 3 at Hospital A was more expressive and grateful:
“Very, really, very wonderful. I am grateful for taking good care of me, getting up early, making sure I have to do what I'm supposed to do, getting my medicine, yes, taking care of my morning exercise, and going through the morning therapies, we call it group therapy, N.A., which is Narcotic Anonymous, yeah, N.A., then other things” (Hospital A, participant 3).
3.2.1.2. Competent Nurses and Supportive Staff Render Care
Other participants recounted the care they received from competent nurses:
“They help us build our self-esteem. And they basically teach us strategies and coping mechanisms to actually sustain our recovery. Because I am an addict, and I'm here for rehab. I'm here to learn stuff about addiction and learn how to stay fit. So that's basically the teaching that goes on here” (Hospital C, participant 1).
Participant 6 at Hospital B was profusely thankful:
“So with the emotional and psychological part, the counsellors are there too for you to see them. So even if you have nights, people, night counsellors. So whenever you are not emotionally fit, there's whom to see. That's your primary counsellor. And he or she is responsible for you at any given time. If the primary counsellor is not around, there are other counsellors you can see” (Hospital B, participant 6).
This same perception colours the views and perceptions of Participant 1 at Hospital A:
“So they have time, they will have enough time for you to explain everything. They will tell you don't hide anything, like I'm sitting here, I have to explain everything, that answer that you are asking, I have to, the person that you are asking, I have to answer it, right? I don't want to, I don't want to lie, I have to say the truth” (Hospital A, participant 1).
3.2.1.3. Experience of Negative Attitudes from some Staff Members
Two participants narrated the negative attitudes experienced from some of the nurses:
“The negative is that they still do have that, you know, my way or the highway sort of attitude towards patients, just less so than what I found in assessments. As one example, I mean, yeah, well, I'll give you two” (Hospital B, participant 3).
A more nuanced critique came through in Participant 5 at Hospital B:
“That is, it is the patient who knows how he feels when it comes to sickness. So sometimes the nurses that are here, excuse me to say, they don't normally see us when we complain of a sickness, they don't take it serious because of our addiction. And when he comes, the sort of like annoyance that he has brought from home is on him. So he wants to do it to us. But don't forget that we are patients who are seeking for recovery” (Hospital B, participant 5).
3.2.2. Theme 2: Challenges Experienced by Patients Diagnosed with Dual Diagnosis
Some participants mentioned being left out of their care, isolation from family, poor food quality, poor infrastructure, and inadequate resources.
3.2.2.1. Lack of Patient Involvement in Care
Two participants lamented the lack of involvement in their care:
“But all the same, I have a diagnosis, and it just seems to follow me everywhere. I've never had the chance to meet a professional ready to say, okay, I'm ready to review you from scratch. Ready to explain to you, okay, you see how you're behaving, or you see how you were behaving” (Hospital B, participant 3).
This sentiment is evident in the vignette below:
“That are to help us get rid of maladaptive behaviours that we had formed back in addiction. So, …And you are being told to do it. And you have to do it. That's how it is. It's more or less. You are being coerced. Like, do this now at this time. Do this now at this time. And at times, you know how human beings are. We want to have things go out. We just want to do things our own way. Let me say, recovering addicts, we like to do things our own way sometimes” (Hospital B, participant 4).
3.2.2.2. Isolation from Family
Other participants spoke about being isolated from their family in this vignette below:
“You know, I believe that, uh, as human beings, you must have compassion, uh, compassion where, um, um, um, yesterday I was, I couldn't go to session because I was emotionally imbalanced. I couldn't, I couldn't sit because I, I, I didn't see why I should be kept here for eight months, you know, where I finished the programme and just my family to come and say that, um, blah, blah, blah, I should be kept here for another three months because they said I'm owing somebody” (Hospital B, participant 1).
“For now, sometimes you may also want to visit your people, they will not allow you to go out. That is another challenge. That is the only challenge we face here as a patient” (Hospital C, participant 4).
3.2.2.3. Poor Food Quality
Participants from hospitals A and B spoke about food quality as:
“The food comes with the beans, right? It comes just raw beans with gari, no plantain. At times, even if they don't bring the plantain, they won't explain to you that the rice is not well-cooked. Sometimes very hard. It's just once, once or twice that it's cooked well. But it's still very, very horrible. The, the, the, the stew is okay, but the, the soup, the groundnut soup is not, is not good. And the, the, the fish itself is normal, which sometimes is bent, you know? So these are some of the challenges we face” (Hospital B, participant 1).
“Okay. The food, we don't get satisfied when it comes to the food. There's not many. And also, some of the food. I don't eat cabbage. But they mostly bring cabbage to you. And when we don't have anything to replace the cabbage, that means you have to eat the rice. We're all like that. So, that's a challenge we also face sometimes” (Hospital A, participant 5).
“Sometimes the food doesn't come in good quality. So these are the challenges” (Hospital B, participant 6).
3.2.2.4. Poor Infrastructure and Inadequate Resources
Participants in hospital B were unhappy about resources and infrastructure:
“Another challenge we have is uh, our bathroom or toilet facility. Currently, we are almost about 22 residents here, and we only have two toilets that are good. So it means that even if the males are 20, it means that 15 or 10 will share one toilet. And just imagine sometimes we catch infections here as a doctor, you know? Mm-Hmm, <affirmative>. So we currently have three, but two is effectively working. So 20 residents use one toilet” (Hospital B, participant).
“I think, for being in the prospectus, instead of certain things, maybe they can just add one plastic chair. So that when I come in, I know I'm coming with a plastic chair. I know I'll be there. Because people come in with back pain and other things. Sometimes you have to sit on a chair and be holding the chair and be sitting, because the women swing the chair. Sometimes people have to be rushing to go for sessions because some of the chairs are not good, others are good in coordination. So people want to rush and get the good ones in coordination. When you get the broken one, it's up to you whether you fall or you don't fall” (Hospital B, participant 6).
3.2.3. Theme 3: Recommendations for Improving Care for Patients Diagnosed with Dual Diagnosis
Participants provided suggestions for improving nursing care, such as continuous capacity building and upskilling of nurses on the management of dual diagnosis, employing more nurses for continuity of care, enhanced professionalism by nurses, provision of recreational activities and vocational training, improved communication of programme expectations, allowing space for patient complaints and suggestions on the programme, and family involvement in rehabilitation programmes.
3.2.3.1. Continuous Capacity Building and Upskilling of Nurses on the Management of Dual Diagnosis
Participants in Hospitals A, B, and C were unanimous regarding capacity building as:
“So, if they are educated better, and if they are given the skills better, they equip with the knowledge, if they are better equipped in their own area of expertise, it makes us that we are in their care, we feel better off too” (Hospital C, participant 1).
“So I think seminars and courses should be organised for the nurses and counsellors so that they will improve upon their way of handling people. Because when you look at the structure, there are other institutions, there are other competitive districts out there” (Hospital B, participant 5).
“So what I would prefer is, you people have to, I mean, improve them more, so that the knowledge, you understand, the knowledge will go higher, so that, I mean, we all can, what, recover them, go to our various places” (Hospital A, participant 1).
3.2.3.2. Employing more Nurses for Continuity of Care
Other participants advanced the argument for more nurses in this vignette:
“But I think we can have more nurses over here to cater for our needs generally. At times, there are few hands on deck. So, you just have to wait” (Hospital B, participant 4).
“What can be done is if the nurses that are here are not enough, they are really not enough, if there will be more nurses. Even though the clients are not many, if there are more nurses, I think it will be good” (Hospital B, participant 2).
3.2.3.3. Enhanced Professionalism by Nurses
A participant in Hospital ‘A’ did not mince her words on professionalism by nurses as:
“So I think they should improve on their confidentiality level and their professionalism level, and also compassion, which is part of the hospital’s core values. So these three cardinal areas, professionalism, uh, confidentiality, and compassion must be part of the programme” (Hospital A, participant 1).
“So I think they should improve on their confidentiality level and their professionalism level, and also compassion, which is part of the hospital’s core values. So these three cardinal areas, professionalism, uh, confidentiality and compassion must be part of the programme” (Hospital A, participant 5).
“Talking to the person. Talking to the person. In a polite manner. Okay. Such that the person is going to admit it and be, like, in order to change from his bad behaviour into doing good behaviours” (Hospital A, participant 6).
3.2.3.4. Provision for Recreational Activities and Vocational Training
Other participants spoke about recreational and vocational activities as:
“Which sometimes, I don't like always being at one place. So, I feel like sometimes, during the weekend, we should take you for a walk. Or a morning exercise at least, for a walk” (Hospital B, participant 5).
“If they can also get us a place that we can also have, let's say, you can have any craft work or anything like schooling. It will be like a vocational school for us. Right” (Hospital C, participant 4).
3.2.3.5. Improved Communication of Programme Expectations
All the participants from hospitals A, B, and C wanted improved communication in this vignette:
“So, you teaching me, you that I am in your care, you should have a better understanding of what it is you're telling me to adhere to or to go through or to learn. So, yeah, so proper diffusion of information and then proper education” (Hospital C, participant 1).
“Stop shouting. They should use reason instead of like voice volume. Use reasoning and then? Not voice volume to get their way. Right” (Hospital B, participant 3).
“If there can be a notice board for the patients, where we can also go and read information about ourselves. How the process is going on” (Hospital A, participant 5).
3.2.3.6. Provision of Space for Patient Complaints and Suggestions on the Programme
Some participants from Hospital B made suggestions for consideration as:
“An opportunity to review, like a periodic review of like the facility, done by both residents and nurses. So, you know, if it looks like, I don't know, we have a chair situation right now, a chair that's getting broken, we're running out of chairs for residents. There should be some sort of yearly review where we can mention these problems and have them fixed” (Hospital B, participant 3).
“So maybe the way they are caring for you is something that you would have wished that they add to how they are caring for you. And they are not adding. So that is what you can talk about it now, so that it will be captured” (Hospital B, participant 2).
3.2.3.7. Family Involvement in Rehabilitation Programmes
Other participants talked about family involvement in the programme:
“We are about 25, 30. So if they can make it like weekends after washing or after church service, they can make it like you have some sort of 15 minutes that you can make a call to your families for them to know how you are doing. Because they will also be sort of thinking about how you are feeling” (Hospital B, participant 5).
“Also, the orientation should be done for them so that they also take their time. Orientation should be done for... I mean, I don't know” (Hospital B, participant 4).
4. DISCUSSION
The findings of this study highlight that patients with dual diagnosis encounter a complex blend of nursing care within psychiatric units, which they perceived as both supportive and, at times, challenging. On the positive side, participants reported that nursing care was holistic, competent, and supportive, consistent with broader literature advocating for person-centred mental health services. Holistic care in this context extended beyond symptom management to include attention to physical health needs, medication administration, personal hygiene, nutrition, and psychosocial well-being. This multidimensional approach reflects the principles of Orem’s Self-Care Deficit Nursing Theory, which emphasises the nurse’s critical role in identifying and addressing gaps in patients’ self-care abilities, thereby supporting recovery through both basic and therapeutic interventions [22]. When nurses integrated counselling, coping skills education, and emotional availability into routine care, participants perceived these efforts as significant enablers of recovery. These practices resonate strongly with recovery-oriented frameworks, which emphasise empowerment, hope, and the therapeutic value of collaborative nurse-patient relationships [23, 24].
However, the study also identified significant negative experiences that undermined patients’ trust and sense of support within psychiatric care. Participants described some staff attitudes as dismissive, authoritarian, or lacking empathy. Such negativity created barriers to therapeutic engagement. Such accounts mirror findings in prior research showing that stigma and negative stereotyping of individuals with co-occurring mental illness and substance use disorders persist within healthcare systems [25]. These perceptions were particularly concerning in cases where patients felt their physical health concerns were disregarded, often due to their addiction history. This reflects the phenomenon of diagnostic overshadowing [26, 27], whereby a patient’s mental illness or substance use status leads clinicians and nurses to misinterpret, minimise, or overlook physical symptoms. The implications are profound, as untreated physical health issues not only compromise overall well-being but may also exacerbate psychiatric symptoms and hinder recovery progress.
Beyond interpersonal interactions, structural and systemic challenges were also evident. Participants cited lack of involvement in their own care planning, social isolation from family, substandard food quality, and infrastructural deficiencies such as broken furniture and insufficient sanitary facilities. The absence of shared decision-making contradicts the core principles of recovery-oriented care, which emphasise patient autonomy, collaboration, and active participation in treatment planning [23, 24]. Similarly, limited family engagement was perceived as an additional barrier. Given that family systems provide crucial social support and act as protective factors against relapse, their exclusion may weaken patients’ recovery outcomes. These systemic shortcomings highlight how institutional environments and organisational practices can inadvertently perpetuate disempowerment, isolation, and dissatisfaction among patients with dual diagnosis.
In response to these challenges, participants suggested practical and constructive recommendations. They emphasised the importance of continuous professional development for nurses in managing dual diagnosis, particularly in fostering empathy, communication, and evidence-based care strategies. Training could also mitigate stigma by reshaping attitudes and increasing staff competence in integrated care approaches. Calls for increased staffing and continuity of care reflect ongoing concerns about nurse-patient ratios in mental health facilities, where workforce shortages can compromise quality of care and patient safety. Similarly, participants highlighted the need for improved professionalism and transparency in communicating programme expectations, which could enhance trust and therapeutic alliance.
Participants also advocated for expanding the scope of psychiatric care to include recreational and vocational opportunities. Such activities address the occupational and social dimensions of recovery, providing patients with skills, purpose, and a sense of belonging - all central to the Recovery Model’s emphasis on meaningful engagement in life roles [23, 24]. Introducing structured mechanisms for patient feedback was another key suggestion, reflecting a desire for systemic openness and responsiveness. By allowing space for patient voices, services could better align with the principles of collaborative care frameworks, where service user input is not only valued but actively shapes policies and practices. Finally, greater family involvement in treatment was understood to be vital for strengthening social support networks, reducing isolation, and fostering continuity of care post-discharge.
Taken together, these findings stress the dual reality of psychiatric nursing care for patients with dual diagnosis, marked by both positive experiences of holistic, supportive interventions and negative experiences shaped by stigma, structural barriers, and lack of collaboration. The study highlights the urgent need for systemic reforms, including capacity building for staff, infrastructural improvements, patient-centred practices, and integration of recovery-oriented models. By addressing these gaps, psychiatric nursing care could shift closer to a model that fully respects the dignity, autonomy, and holistic needs of individuals with dual diagnosis, thereby enhancing both clinical outcomes and patient satisfaction.
5. LIMITATIONS
This study recruited participants primarily from rehabilitation units and wards known to provide care for individuals with substance use and mental health conditions. As a result, patients in other wards who had not yet been diagnosed with dual diagnosis may have been excluded, potentially limiting the breadth of perspectives captured. Secondly, requiring recommendations from a psychiatrist, psychologist, or nurse manager creates a gatekeeper effect that likely excludes patients with conflicted relationships with staff or those perceived as “difficult.” In addition, study rigour could have been strengthened through member checking, such as returning transcripts to participants for verification and clarification, to enhance the credibility of the findings. While the results provide valuable insights into the nursing care of patients with dual diagnosis, the experiences described are specific to individuals receiving care within psychiatric hospitals in Ghana. Consequently, the findings may not be fully transferable to patients with dual diagnosis in other cultural or healthcare contexts.
6. IMPLICATIONS FOR NURSING PRACTICE
The findings have several implications for nursing practice in psychiatric and rehabilitation settings: Adoption of recovery-oriented care principles: nurses must shift from a purely directive approach to one that fosters autonomy, mutual respect, and collaborative goal-setting. Stigma reduction in clinical encounters: training should target implicit biases toward patients with substance use histories, ensuring equitable response to all health complaints, and integration of holistic assessment. Nursing assessments should consistently address physical, psychological, social, and spiritual needs, ensuring no dimension of care is overlooked. Enhanced communication skills: nurses should employ therapeutic communication techniques to de-escalate conflict, encourage openness, and build trust. Advocacy for resources: nurses have a role in advocating for improved staffing, infrastructure, and patient amenities, recognising their impact on health outcomes. Family-centred care: incorporating family education and involvement in the rehabilitation process can strengthen community reintegration post-discharge. Evidence-based interventions: nurses should implement interventions grounded in current best practice guidelines for managing dual diagnosis disorders.
By integrating these implications into routine practice, nurses could enhance therapeutic relationships, improve patient satisfaction, and ultimately contribute to better rehabilitation outcomes for individuals with dual diagnosis.
CONCLUSION
The experiences of patients with dual diagnosis in psychiatric care settings demonstrate a complex interplay between positive therapeutic engagement and ongoing systemic gaps. While holistic, competent, and supportive nursing care fosters a sense of safety and progress in recovery, instances of negative staff attitudes, inadequate involvement in care, and infrastructural deficiencies compromise overall patient satisfaction and potentially impede recovery outcomes. The findings underscore the necessity for a balanced approach that integrates clinical competence with empathy, patient autonomy, and environmental adequacy. Addressing both the interpersonal and systemic dimensions of care is essential to achieving sustained, patient-centred rehabilitation for individuals with dual diagnosis.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: F.N.: A PhD candidate, conceptualised the study from the title and methodology, conducted the interviews, and drafted the manuscript; L.A.S. and M.M.M.: PhD supervisors, recast the title and methodology and reviewed the manuscript for a PhD study.
LIST OF ABBREVIATIONS
| HREC | = Health Research Ethics Committee |
| NWU | = North-West University |
| GHS-ERC | = Ghana Health Service Ethics Review Committee |
| PTSD | = Post-traumatic Stress disorder |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the North-West University Scientific Review Committee and the Health Research Ethics Committee, South Africa [HREC] (NWU-00038-24-A1), as well as by the Ghana Health Service Ethics Review Committee, which provided the country-specific ethical approval (GHS-ERC 005/07/24).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the nurses who participated in the study. To protect participants’ privacy, all information was gathered and kept in a secure, anonymised database. Participation was entirely voluntary, with assurances of both confidentiality and anonymity. The data were safely stored, and access was restricted solely to authorised personnel.
AVAILABILITY OF DATA AND MATERIALS
All information is included in the manuscript; however, this can be made available on reasonable request through the corresponding author [F.N].
ACKNOWLEDGEMENTS
The researchers thank the North-West University Health Research Ethics Committee [HREC] (NWU-00038-24-A1), the Ghana Health Service Ethics Review Committee (GHS-ERC 005/07/24), and the selected hospitals in Ghana for approving the study. We are equally grateful to the patients who participated in the study.

