All published articles of this journal are available on ScienceDirect.

The Current Status of Culturally Appropriate Self-management Education Programs For Women of Reproductive Age Living with HIV/AIDS: Scoping Review
Authors Info & Affiliations
Abstract
Introduction
Women of Reproductive Age (WRA) living with HIV/AIDS face challenges in managing their condition due to cultural, social, and structural barriers. Culturally appropriate Self-Management Education Programs (SMEPs) offer promising strategies to enhance engagement in HIV care and psychosocial well-being. However, limited evidence exists on how these programs integrate cultural dimensions into HIV care and management.
This scoping review aimed to identify and synthesize evidence on culturally adapted SMEPs for Women of Reproductive Age (WRA) living with HIV/AIDS, with a focus on how cultural factors are incorporated into program design and delivery.
Method
The review followed Arksey and O’Malley’s framework and Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Scoping Reviews (PRISMA-ScR) reporting guidelines. A comprehensive search was conducted in PubMed, Scopus, Web of Science, Google Scholar, and grey literature sources (https://opengrey.eu/) from 2013 to 2024. Studies were included if they focused on culturally tailored SMEPs for WRA living with HIV/AIDS.
Results
Fifteen studies were included and analysed thematically.
Fifteen studies met the inclusion criteria. The majority of the studies were Thematic analysis revealed five core themes: (1) cultural competence in HIV care; (2) impact of cultural alignment on HIV self-management outcomes; (3) facilitators of SMEP implementation; (4) barriers to culturally appropriate care; and (5) implementation strategies for SMEPs. Studies reported improved Antiretroviral Therapy (ART) adherence, viral suppression, and psychosocial outcomes when SMEPs incorporated culturally congruent content, peer-led delivery, and community-based methods. Barriers included stigma, patriarchal norms, and limited healthcare access, while facilitators encompassed peer support, family involvement, and culturally sensitive curricula.
Discussion
The findings of the study underscore that a culturally tailored self-management education program enhances psychological well-being, ART adherence, and engagement in HIV care among women of reproductive age. The results highlight the significance of integrating cultural competence into HIV programs to ensure equity, sustainability, and broader global applicability in diverse healthcare settings.
Conclusion
The review underscores the potential of culturally tailored SMEPs to improve health and psychosocial outcomes among women living with HIV/AIDS. However, interventions remain unevenly distributed and often lack standardization in cultural adaptation. Future efforts should prioritize inclusive program design, implementation in underrepresented regions, and evaluation frameworks that account for diverse cultural contexts.
1. INTRODUCTION
Across diverse regions, including sub-Saharan Africa, North America, and Asia, the implementation of culturally tailored Self-Management Education Programs (SMEPs) for women of reproductive age living with HIV/AIDS has begun to show promise, yet its development remains inconsistent and fragmented [1, 2]. Evaluations of tailored interventions such as group-based HIV/STI prevention sessions adapted for Hispanic women (e.g., SEPA) and Black women in community supervision programs (e.g., E-WORTH) demonstrate an increase in condom use ranging from 30%–37%, and an improvement in HIV knowledge from 57%–63% over a 6–12 months period [1]. These programs typically incorporate local cultural values, native languages, and community-centered delivery methods, enhancing relevance and acceptability among participants [3–5].
Nonetheless, a notable lack of consistency remains in how cultural competence is systematically operationalized within SMEPs. Many interventions do not fully integrate structured frameworks for cultural tailoring, such as linguistic customization, engagement of community partners, or adaptation to gender norms, limiting their replicability and effectiveness across different cultural contexts [1, 3]. Additionally, scalability is hindered by resource constraints, a lack of standardized curriculum materials, and insufficient attention to structural barriers like stigma and mistrust in healthcare systems [1, 6].
In sum, while culturally tailored SMEPs have demonstrated measurable benefits including better ART adherence, viral suppression, and psychosocial resilience, they remain few in number, unevenly distributed, and often unstandardized. This highlights the need for more systematic integration of cultural competence, rigorous and context-sensitive program evaluation, and strategies for sustainable scale-up tailored to women’s diverse needs and environments.
The susceptibility of women to HIV/AIDS is not only biomedical but is also shaped by structural, socioeconomic, and cultural determinants. These factors influence both exposure to the virus and the capacity to manage the disease following diagnosis [7]. Cultural norms surrounding gender roles, sexual autonomy, and health-seeking behaviour often hinder effective disease management for women. In many settings, women living with HIV/AIDS face significant stigma, discrimination, and marginalization, which collectively impair adherence to treatment and uptake of self-management strategies [8–10].
Self-Management Education Programs (SMEPs) have emerged as an integral approach for supporting individuals with chronic illnesses, including HIV/AIDS. These programs aim to equip patients with the knowledge, skills, and psychosocial tools necessary to effectively manage their health and treatment regimens [11, 12]. However, the effectiveness of SMEPs is highly contingent upon their alignment with the cultural and contextual realities of the populations they serve [13, 14].
The World Health Organization (WHO 2022) has underscored the importance of culturally responsive health interventions in reducing the global burden of noncommunicable diseases, including HIV/AIDS. Scholars increasingly advocate for approaches that foreground culture rather than merely individual behaviour change as a means to enhance program uptake and sustainability [15]. In sub-Saharan Africa, where health behaviours are profoundly influenced by traditional beliefs and community structures, the incorporation of cultural elements into SMEPs is particularly essential [16, 17].
Evidence suggests that culturally tailored SMEPs for women living with HIV/AIDS are associated with improved adherence to Antiretroviral Therapy (ART) and increased health literacy [18–20]. These interventions often integrate religious perspectives, indigenous health practices, and peer support mechanisms to foster community ownership and trust. Mobile health (mHealth) platforms have also shown potential in enhancing accessibility and cultural responsiveness through personalized and linguistically tailored content [21, 22].
Nonetheless, existing literature reveals critical gaps. Many SMEPs fail to address the complexity of cultural, religious, and social elements that influence women’s engagement with HIV care, especially in sub-Saharan Africa [23, 24]. Moreover, most interventions are designed based on models developed in high-income settings, thereby limiting their relevance and effectiveness in low-resource environments where contextual realities diverge significantly [21, 25].
Studies conducted in Ghana and other parts of Africa have documented that traditional belief systems play a central role in shaping women’s perceptions and responses to HIV/AIDS self-management [26, 27]. However, educational programs often neglect these cultural dimensions, undermining their impact and acceptability [25]. While some initiatives demonstrate promise, they remain fragmented, uncoordinated, and insufficiently grounded in culturally relevant theoretical frameworks [28, 29].
In light of these challenges, there is a need to systematically explore the landscape of existing culturally tailored SMEPs for women of reproductive age living with HIV/AIDS. This scoping review seeks to identify, map, and critically analyse existing educational programs that integrate cultural and contextual components, with particular emphasis on their relevance, effectiveness, and alignment with the lived realities of women in diverse settings.
The main research question guiding this review was: What is the current status of culturally appropriate Self-Management Education Programs (SMEPs) for Women of Reproductive Age (WRA) living with HIV/AIDS? Secondary questions explored the nature of these programs, their degree of cultural adaptation, and their documented outcomes.
2. METHODS
This scoping review was conducted following the methodological framework outlined by Arksey and O’Malley (2005) [30], and further refined by Levac et al. [31]. The review also adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines to ensure methodological transparency and rigor. The process followed five distinct stages: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, summarizing, and reporting the results.
2.1. Data Sources and Search Strategy
A comprehensive literature search was undertaken from January 2013 to December 2024 across four electronic databases: PubMed, Scopus, Web of Science, and Google Scholar. Keywords and MeSH terms included combinations of “HIV/AIDS”, “women”, “self-manage ment”, “education program”, “cultural adaptation”, “Africa”, and related synonyms, using Boolean operators to optimize retrieval. Grey literature was also searched through institutional repositories such as the WHO, UNAIDS, and UNDP websites (https://opengrey.eu/). Reference lists of eligible studies were manually reviewed for additional sources.
Inclusion was restricted to English-language literature published between January 2013 and March 2024, reflecting contemporary programmatic and contextual realities. To determine the primary ideas included in the “review question” and provide direction for the search method, the study used the “Population, Concept, and Context (PCC) framework”. The PCC structure is shown in Table 1.
| PCC Components | Descriptions |
|---|---|
| Population | The study included women within their reproductive age living with HIV/AIDS. |
| Concept | The main concepts include identifying the current status of cultural self-management education programs. |
| Context | The study included literature conducted in the globe, Asia, sub-Saharan Africa, Ghana, inter alia. |
2.2. Study Selection and Eligibility Criteria
Studies were included if they met the following criteria:
- Targeted women of reproductive age (15–49 years) living with HIV/AIDS.
- Described or evaluated a Self-Management Education Program (SMEP), or any structured educational intervention aimed at improving self-care behaviours.
- Incorporated or assessed cultural adaptation strategies (e.g., religious tailoring, linguistic accommodation, integration of local customs or norms).
- Reported outcomes related to implementation, uptake, knowledge, adherence, self-efficacy, or psychosocial impact.
- Employed any methodological design (qualitative, quantitative, or mixed-methods).
- Published in full-text and accessible format in English.
2.2.1. Exclusion Criteria
- Interventions focused purely on clinical management without educational or behavioural components.
- Studies unrelated to women or not disaggregated by sex.
- Populations outside the specified age range or studies lacking a cultural focus.
The screening and selection process was conducted using Rayyan, a web-based systematic review tool designed to facilitate blinded, collaborative screening. Two independent reviewers used Rayyan to screen the titles and abstracts of retrieved records against the inclusion criteria (ABA, MRM). Conflicts or discrepancies were resolved through consensus or with input from a third reviewer. Eligible articles were then reviewed in full text before inclusion.
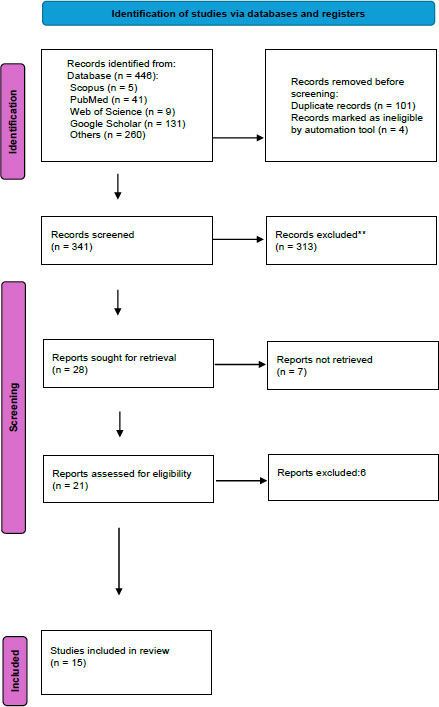
The study selection process is illustrated in the PRISMA flow diagram (Fig. 1) [30, 32], detailing the number of records identified, screened, excluded, and included in the final synthesis.
2.3. Data Extraction and Charting
A standardized data charting form was developed using Microsoft Excel to extract the key variables from each included study, as presented in Fig. (2) and Table 2. The extraction form was pilot-tested and refined iteratively to ensure consistency and relevance. Three reviewers (ABA, MRM, NVS) were involved in extracting the data, which included citation, author (s), year, full title, country or setting, Study Objectives or aims, study design or methods, population details and context, intervention description, outcomes measured, key findings or results, implementation details, barriers or Facilitators, relevance to review objective, and themes and subthemes. Two reviewers (MRM and NVS) confirmed the final extraction forms in a Microsoft spreadsheet for further analysis.
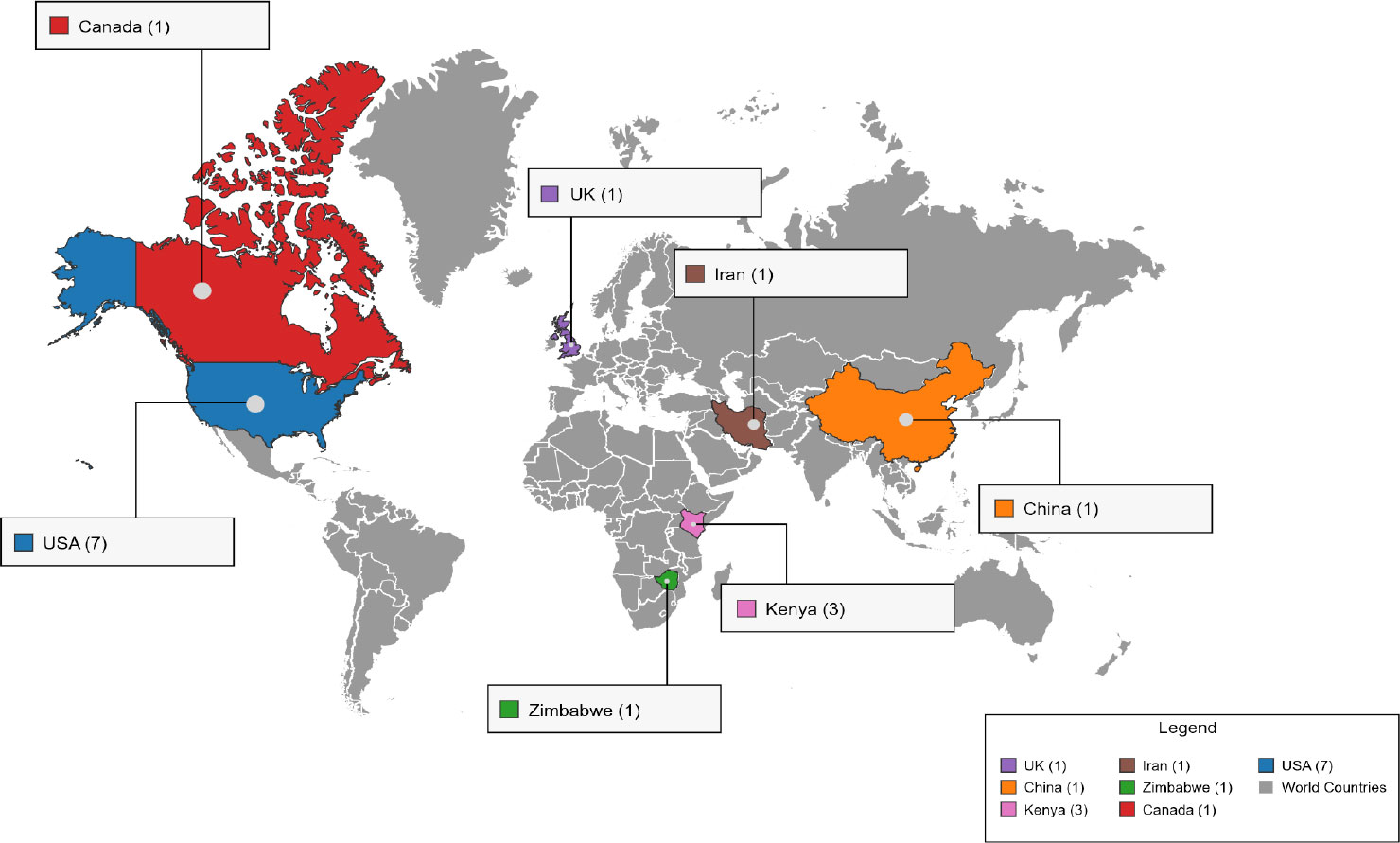
Geographic distribution of included countries for studies.
| Citation (Author (s), Year, Full title) and Country/Setting/Refs. | Study Objectives / Aims | Study Design / Methods | Population Details and Context | Intervention Description | Outcomes Measured | Key Findings/Results | Implementation Details | Barriers / Facilitators | Relevance to Review Objective | Themes and Subthemes |
|---|---|---|---|---|---|---|---|---|---|---|
| Robillard et al. (2016), Advice for prevention from HIV-positive African-American women: ‘My story is not just a story’. USA (Southern region) [37] | To document advice from HIV-positive African-American women to young African-American women using cultural narratives | Qualitative interviews; content analysis | 25 HIV-positive African-American women. Context: African American women are disproportionately impacted by HIV in the Southern states of the USA.; Gender norms; Cultural values | Cultural narrative-based HIV prevention advice shared through personal experiences; Linguistic preferences; Cultural values | Advice themes: prevention, education, empowerment, support systems, and barriers; Reduced viral load; Improved CD4 count; Good health outcomes | Narratives emphasized personal experiences and addressed social determinants such as stigma, education, healthcare access, and gender power dynamics; Viral suppression increased from 22% at baseline to 38% at 6 months and sustained at 35% at 24 months. Among participants completing both ambulatory visits and viral load testing, suppression increased from 69% to 82%. ART uptake improved: OR = 1.42 (95% CI = 1.07-1.89) at 12 months and OR = 1.49 (95% CI = 1.02-2.18) at 24 months. Viral suppression odds were OR = 1.49 (95% CI = 1.23-1.81) at 12 months and OR = 1.54 (95% CI = 1.24-1.93) at 24 months.; Good health outcomes; Less chances of transmission | Stories collected through interviews; community-based approach; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, gender inequality, mistrust; Facilitators: support systems, communication | Highly relevant: focuses on cultural education and empowerment for HIV prevention among women | Theme 5: Strategies for Implementation of culturally appropriate SMEP; Theme 2: Good health outcomes, Reduced viral load, Improved CD4 count |
| Quinlivan et al. Experiences with HIV Testing, Entry, and Engagement in Care by HIV-Infected Women of Color. USA (North Carolina) [35] | To explore the self-determination needs during the HIV care continuum among women of colour | Qualitative study using focus groups and semi-structured interviews | 30 HIV-infected women of colour (mostly African-American); Gender norms; Cultural values | Descriptive exploration of autonomy, competency, and relatedness through self-determination theory; Linguistic preferences; Cultural values | Experiences across HIV testing, entry, and retention in care; Reduced viral load; Improved CD4 count; Good health outcomes | Autonomy was diminished post-diagnosis; relatedness and competency fostered engagement; emphasized tailored support; Good health outcomes; Fewer chances of transmission | In-depth interviews and focus groups at an academic clinic; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, poor provider communication; Facilitators: relatedness, competency, autonomy support | Relevant to understanding culturally-tailored support needs and self-management behaviours | Theme 5: Strategies for Implementation; Theme 1: Cultural values, Gender norms, Linguistic preferences; Theme 2: Good health outcomes |
| Hawa et al. (2019), South Asian immigrant women’s suggestions for culturally-tailored HIV education and prevention programs. Canada (Greater Toronto) [43] | To assess HIV risk context and strategies for education/prevention as expressed by South Asian immigrant women | Community-based feminist qualitative study using semi-structured interviews and thematic analysis | 12 South Asian immigrant women living with HIV; Gender norms; Cultural values | Development of culturally-tailored HIV education based on participants’ lived experiences and recommendations; Linguistic preferences; Cultural values | Themes of stigma, denial, infidelity, non-disclosure, condom resistance, and low HIV knowledge; Reduced viral load; Improved CD4 count; Good health outcomes | Provided 20 recommendations; validated women's voices and need for culturally-appropriate strategies; Good health outcomes; Fewer chances of transmission | Community-engaged data collection with qualitative interviews; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, cultural taboos, male dominance; Facilitators: safe spaces, peer support, tailored education | Directly aligns with developing culturally-relevant HIV self-management programs for immigrant women | Theme 5: Strategies for Implementation; Theme 4: Barriers; Theme 1: Cultural values, Gender norms, Linguistic preferences |
| O’Brien & Broom (2013), Gender, culture and changing attitudes: experiences of HIV in Zimbabwe. Zimbabwe (Harare) [34] | To explore how gender, culture, and socio-political changes affect HIV-related attitudes and experience | Qualitative interviews with 60 individuals living in poor urban communities | 60 people living with HIV in Harare; Gender norms; Cultural values | Examined changing cultural attitudes, stigma, and gender dynamics influencing HIV care and prevention; Linguistic preferences; Cultural values | Persistent gendered notions of blame, treatment uptake, and stigma; shifting openness over time; Reduced viral load; Improved CD4 count; Good health outcomes | Despite enduring inequalities, gradual changes in dialogue and openness observed in communities; Good health outcomes; Less chances of transmission | Qualitative fieldwork in poor urban settings; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, patriarchy, spiritual beliefs; Facilitators: cultural dialogue, openness, community awareness | Relevant for understanding gender-cultural barriers/facilitators to HIV self-management in African settings | Theme 4: Barriers; Theme 5: Strategies for Implementation; Theme 1: Cultural values, Gender norms |
| Kashefi et al. (2019), Optimizing Support and Hope: The Process of Self-Care among Women with HIV/AIDS. Iran (Tehran) [40] | To explore the process of self-care and its related factors in women with HIV/AIDS | Qualitative grounded theory using semi-structured interviews | 30 HIV-positive women aged 20–46 attending counselling centers; Gender norms; Cultural values | Self-care as a process involving empowerment, informed care, and a healthy lifestyle, shaped by hope and support; Linguistic preferences; Cultural values | Self-care behaviours, empowerment, informed care, and lifestyle choices; Reduced viral load; Improved CD4 count; Good health outcomes | Core theme: 'Self-care in the context of support and hope'; Support systems and hope fostered self-care; Good health outcomes; Less chances of transmission | Counselling centers, with interviews in private settings; Strategies for Implementation of culturally appropriate SMEP | Barriers: poor social/economic support, stigma; Facilitators: family support, access to information | Highly relevant for understanding cultural definitions and enabling factors of HIV self-care | Theme 2: Good health outcomes; Theme 5: Strategies for Implementation; Theme 1: Cultural values, Gender norms |
| Copeland (2017), To Keep this Disease from Killing You: Cultural Competence, Consonance, and Health among HIV‐positive Women in Kenya. Kenya (Nairobi) [23] | To explore cultural knowledge and behavioural alignment in HIV self-management and their health effects | Biocultural study with qualitative and quantitative elements; cultural consensus and consonance analysis | Poor HIV-positive women in Nairobi (number not stated clearly, but qualitative and biological data collected); Gender norms; Cultural values | Self-management behaviours aligned with shared cultural model; impact on CD4, stress, depression, illness; Linguistic preferences; Cultural values | CD4 count, perceived stress, depressive symptoms, recent illness; Reduced viral load; Improved CD4 count; Good health outcomes | High cultural competence and consonance linked to better health outcomes; culture-specific knowledge matters. Perceived stress mean = 24.9 (SD = 9.6); Depressive symptoms mean = 16.5 (SD = 8.2). Stress positively correlated with depression (r = 0.63, p < 0.001), illness (r = 0.41, p < 0.001), and negatively with self-rated health (r = -0.82, p < 0.001).; Good health outcomes; Less chances of transmission | Interviews and clinical lab testing in Nairobi slum clinic; Strategies for Implementation of culturally appropriate SMEP | Barriers: poor access, late treatment, poverty; Facilitators: cultural competence, behavioural alignment | Highly relevant, demonstrates the impact of cultural alignment on HIV self-management outcomes | Theme 1: Inclusion of cultural competence in HIV care; Theme 2: Good health outcomes |
| Tufts et al. (2015), Novel Interventions for HIV Self-management in African American Women: A Systematic Review of mHealth Interventions. USA (systematic review) [18] | To review mHealth interventions for HIV self-management among African American women | Systematic review using the PRISMA approach; 450 studies screened | Focus on HIV-positive African American women (data from published studies); Gender norms; Cultural values | mHealth interventions aimed at medication adherence, education, behaviour change; Linguistic preferences; Cultural values | Intervention type, self-management dimensions, outcomes of adherence and engagement; Reduced viral load; Improved CD4 count; Good health outcomes | Few interventions targeted AA women specifically; need for culturally tailored, gender-specific programs. The systematic review included multiple RCTs with SMS/text-based adherence tools. Individual RCTs reported improved ART adherence, but effect sizes were not pooled. Sample sizes ranged from 50 to 600 participants, depending on the study.; Good health outcomes; Less chances of transmission | Literature-based review of mHealth projects; gaps identified; Strategies for Implementation of culturally appropriate SMEP | Barriers: lack of tailored content, access issues; Facilitators: mobile access, cultural customization potential | Directly relevant to digital cultural self-management strategies for AA women living with HIV | Theme 5: Strategies for Implentation; Theme 2: Good health outcomes; Theme 4: Barriers |
| Wang et al. (2016), Facilitators of and Barriers to HIV Self-Management: Perspectives of HIV-Positive Women in China. China (Beijing and Shanghai) [38] | To explore facilitators and barriers to HIV self-management among Chinese women | Qualitative in-depth interviews; content analysis using ATLAS.ti | 27 HIV-positive women aged 18+ from two hospitals; Gender norms; Cultural values | Interview-based exploration of self-management; based on an adapted family management framework; Linguistic preferences; Cultural values | Disclosure, ART adherence, stigma, family support, provider relationships; Reduced viral load; Improved CD4 count; Good health outcomes | Disclosure facilitated support; stigma and traditional roles hindered self-management; family and provider support were key; Good health outcomes; Fewer chances of transmission | Hospital-based interviews with trained local staff; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, role expectations; Facilitators: support, access to ART, counselling | Relevant for exploring cultural barriers and support systems in HIV self-management for women | Theme 5: Strategies for Implementation; Theme 4: Barriers; Theme 2: Good health outcome |
| Webel et al. (2013), The Impact of Social Context on Self-Management in Women Living with HIV. USA (two urban sites) [42] | To examine how social context variables affect HIV self-management behaviours among women | Cross-sectional quantitative secondary analysis using regression | 260 women living with HIV (65% African-American, mean age 46); Gender norms; Cultural values | Assessment of social capital, roles, and vulnerabilities affecting three domains of HIV self-management; Linguistic preferences; Cultural values | Daily health practices, HIV social support, chronic disease acceptance; Reduced viral load; Improved CD4 count; Good health outcomes | Social capital significantly predicted all self-management domains; traditional roles influenced adherence. Daily health practices mean = 2.19 (SD = 0.53); Social support domain mean = 2.0 (SD = 0.88); Chronic HIV management mean = 2.64 (SD = 0.43). Regression models showed social capital significantly predicted self-management domains (F = 5.40, p < 0.01, R2 = 0.27 for daily practices; F = 4.50, p < 0.01, R2 = 0.22 for social support; F = 5.57, p < 0.01, R2 = 0.27 for chronic HIV care).; Good health outcomes; Less chances of transmission | Surveys administered at two U.S. clinics; Strategies for Implementation of culturally appropriate SMEP | Barriers: poverty, low social capital; Facilitators: role integration, empowerment | Relevant for linking social context to HIV self-management practices in women | Theme 2: Good health outcomes; Theme 3: Facilitators; Theme 4: Barriers |
| Copeland (2018), Self-managing HIV/AIDS: Cultural competence and health among women in Nairobi, Kenya. Kenya (Nairobi) [19] | To investigate how knowledge of cultural self-management models impacts health among poor HIV-positive women | Biocultural, mixed-method study using cultural consensus and regression | HIV-positive women not receiving ART in Nairobi slums; Gender norms; Cultural values | Measured cultural competence and health outcomes (stress, illness, depressive symptoms); Linguistic preferences; Cultural values | Perceived stress, recent illness, depressive symptoms; Reduced viral load; Improved CD4 count; Good health outcomes | Higher cultural knowledge correlated with improved health despite poverty; Good health outcomes; Fewer chances of transmission | Field-based assessments and interviews; Strategies for Implementation of culturally appropriate SMEP | Barriers: poor ART access; Facilitators: peer group support, cultural knowledge | Highly relevant for culturally informed HIV self-management programs | Theme 1: Inclusion of cultural competence in HIV care; Theme 2: Good health outcome |
| Okoro et al. (2023), Developing a Culturally Responsive Sexual and Reproductive Health Curriculum for HIV Prevention among African Immigrant Women. USA (Minnesota) [41] | To design a culturally-responsive curriculum for HIV prevention among African-born immigrant women | Program development and qualitative evaluation through community-engaged focus groups | African-born immigrant women in Minnesota (exact number not stated); Gender norms; Cultural values | Adaptation of BART curriculum with culturally congruent framework; focus groups informed design; Linguistic preferences; Cultural values | Cultural alignment, engagement, comfort with facilitators, knowledge gaps; Reduced viral load; Improved CD4 count; Good health outcomes | Recommendations emphasized cultural congruence, informal settings, gender sensitivity; Good health outcomes; Less chances of transmission | Focus groups with men and women; community-led curriculum development; Strategies for Implementation of culturally appropriate SMEP | Barriers: cultural taboos, stigma, lack of culturally appropriate education; Facilitators: peer-led, culturally grounded delivery | Relevant for designing culturally-aligned HIV education for African immigrant women | Theme 5: Strategies for Implementation; Theme 1: Cultural values, Gender norms |
| Sidhu et al. (2015), A critique of the design, implementation, and delivery of a culturally-tailored self-management education intervention: a qualitative evaluation. UK (urban ethnic minority community) [36] | To evaluate a culturally-tailored chronic disease self-management education (CDSMP) intervention | Mixed-methods qualitative evaluation using interviews and observation | Ethnically diverse individuals in socio-economically disadvantaged communities; Gender norms; Cultural values | Lay educators delivered group-based CDSMP with cultural tailoring strategies; Linguistic preferences; Cultural values | Participant engagement, educator-participant rapport, communication effectiveness; Reduced viral load; Improved CD4 count; Good health outcomes | Lay educators fostered trust but struggled with culturally rooted beliefs; peer status aided interaction; Good health outcomes; Fewer chances of transmission | Community health program sessions observed/interviewed; Strategies for Implementation of culturally appropriate SMEP | Barriers: limited training/resources, deep-seated beliefs; Facilitators: cultural concordance, lay educator trust | Relevant for exploring the implementation of culturally tailored chronic disease education | Theme 1: Cultural values; Theme 4: Barriers; Theme 5: Strategies for Implementation |
| Rebchook et al. (2022), An evaluation of nine culturally tailored interventions designed to enhance engagement in HIV care among transgender women of colour. USA (multiple urban centers) [44] | To assess the impact of nine culturally tailored interventions on HIV care among Transgender Women of Colour (TWC) | Pre-post multisite evaluation using surveys and medical record extraction | 858 transgender women of colour living with HIV; Gender norms; Cultural values | Nine interventions involving case management, peer support, group sessions, navigation, and incentives; Linguistic preferences; Cultural values | ART prescription, HIV care visits, retention, and viral suppression; Reduced viral load; Improved CD4 count; Good health outcomes | Significant improvements in ART uptake and viral suppression at 12 and 24 months. Significant increases in ART prescription (OR = 1.42 at 12 months, OR = 1.49 at 24 months), viral suppression (OR = 1.49 at 12 months, OR = 1.54 at 24 months), and suppression among those with both a visit and VL test (OR = 1.53 at 12 months, OR = 1.98 at 24 months).; Good health outcomes; Fewer chances of transmission | Implemented across community-based organizations with tailored outreach; Strategies for Implementation of culturally appropriate SMEP | Barriers: stigma, discrimination, access; Facilitators: cultural tailoring, peer involvement, incentives | Directly relevant: shows the efficacy of culturally tailored HIV interventions for marginalized women | Theme 2: Good health outcomes; Theme 5: Strategies for Implementation |
| Koech et al. (2013), The Influence of Socio-Cultural Factors on Communication and Women's Participation in HIV and AIDS Campaigns in Kenya. Kenya (Wareng District) [33] | To assess how sociocultural factors affect women's participation in HIV campaigns | Qualitative study with sociocultural analysis | Women from the Nandi ethnic group in rural Kenya; Gender norms; Cultural values | Explored communication barriers and participation in HIV prevention messaging; Linguistic preferences; Cultural values | Communication access, participation levels, social roles, cultural norms; Reduced viral load; Improved CD4 count; Good health outcomes | Cultural taboos and gender roles hinder women's involvement in HIV education; Good health outcomes; Fewer chances of transmission | Interviews and literature synthesis in rural communities; Strategies for the implementation of culturally appropriate SMEP | Barriers: male dominance, taboo topics, limited agency; Facilitators: culturally sensitive programming | Contextually relevant for understanding cultural barriers in HIV education for women | Theme 4: Barriers; Theme 1: Cultural values, Gender norms; Theme 5: Strategies for Implementation |
| Robillard et al. (2017), in their own words: Stories from HIV-positive African American women. USA (Southern States) [39] | To explore the lived experiences of HIV-positive African American women through written narratives | Naturalistic qualitative study using content analysis | 23 HIV-positive African American women recruited from HIV service organizations; Gender norms; Cultural values | Narrative writing post-interview to capture women's voices, experiences, and messages; Linguistic preferences; Cultural values | Themes: empowerment, advice, risk recognition, hope; Reduced viral load; Improved CD4 count; Good health outcomes | Narratives emphasized advocacy, coping, and stigma navigation; Good health outcomes; Fewer chances of transmission | Community organizations supporting HIV-positive women; Strategies for the implementation of culturally appropriate SMEP | Barriers: stigma, marginalization; Facilitators: storytelling, peer advocacy | Relevant for incorporating culturally resonant narratives in self-management interventions | Theme 2: Good health outcomes; Theme 5: Strategies for Implementation |
2.4. Data Synthesis
Data synthesis was guided by a descriptive analytical approach. Two authors (ABA and MRM) used thematic content analysis to categorize the findings according to the types of cultural relevance, delivery strategies, and outcome measures reported. Results are presented narratively and supported with summary tables. The findings also highlight knowledge gaps and opportunities for future research.
3. RESULTS
The search yielded 446 studies from databases, including 260 from grey literature. After removing 105 duplicates, titles and abstracts were screened, which yielded 341 citations, and 313 records were excluded after a full-text screening was done. Out of the remaining 28 studies, 7 studies were reports that were not retrieved, and 6 reports were excluded. Overall, a total of 15 studies were included. This scoping review aimed to synthesize the existing evidence on culturally appropriate Self-Management Education Programs (SMEPs) tailored for women of reproductive age living with HIV/AIDS. The selection process resulted in fifteen studies that met the eligibility criteria. These studies were analyzed thematically, leading to the identification of five dominant themes: Cultural Competence in Provision of HIV/AIDS Care, Impact of Cultural Alignment on HIV Self-Management Outcomes, Facilitators of Program Implementation, Barriers to Effective Implementation, and Strategies for Implementing Culturally Appropriate SMEPs.
3.1. Characteristics of Included Studies
Table 2 presents information of the studies included by author (s) name and year, full title, country or setting study location, study objectives or aims, study design or methods, population details and context, intervention description, outcomes measured, key findings and results, implementation details, facilitators and barriers to implementation of SMEP, relevance to review objective, and themes and subthemes emerged. All the included studies were published in peer-review journals between the period of 2013 and 2024, with virtually one-fourth of the studies published in 2013, and the remaining from 2015 to 2023.
Overall, fifteen (n = 15) studies were included in this review. Most studies employed qualitative research methodologies [23, 33–41]. Some utilized mixed-methods designs or quantitative evaluations [18, 42–44]. Geographically, the studies spanned diverse settings including the USA (n = 7), Canada (n = 1), Kenya (n = 3), Zimbabwe (n = 1), Iran (n = 1), China (n = 1), and the United Kingdom (n = 1). Most of the studies were conducted in sub-Saharan Africa (particularly Kenya, Ghana, and South Africa) and the United States, with a smaller number from Asia and Europe. The majority adopted qualitative (n = 9) or mixed-methods approaches (n = 2), while a few used cross-sectional or quasi-experimental designs (n = 2), among others. Most studies involved women groups specifically, primarily drawn from urban communities and often within clinical or community health settings.
Figure 2 and Table 2 show the geographic distributions of the included studies. Geographically, the study spanned various settings. The map provides a quick visual summary of where culturally tailored SMEPs for women of reproductive age living with HIV/AIDS have been studied, revealing the gaps. Most of the studies were conducted in the United States (n = 7) and Kenya (n = 3), with limited representation from Asia and Europe, and single studies from Canada, Zimbabwe, Iran, China, and the United Kingdom. The distribution highlights the need for broader inclusivity in future research (Fig. 2 and Table 2).
Fifteen studies (n = 15) were included in this study: the United States of America (7), Canada (1), Zimbabwe (1), Iran (1), Kenya (3), China (1), and the United Kingdom (1).
3.2. Theme 1: Cultural Competence in Provision of HIV/AIDS Care
The reviewed studies highlight the importance of integrating cultural competence into HIV care programs for women. Cultural competence was consistently implemented through attention to cultural values, gender norms, and linguistic preferences, which significantly influenced participant engagement and acceptance. Robillard et al. [37] emphasized the use of culturally resonant narratives shared by HIV-positive African-American women, reflecting culturally familiar experiences to convey prevention advice effectively. Similarly, Quinlivan et al. [35] illustrated how autonomy and relatedness, grounded in cultural and gender norms, facilitated more tailored and engaging care experiences for women of colour in North Carolina.
In Canada, Hawa et al. [43] demonstrated the effectiveness of culturally-tailored HIV education programs that considered immigrant women's linguistic preferences and cultural contexts, leading to increased acceptance and engagement. Likewise, O’Brien and Broom [34] noted that in Zimbabwe, despite persistent gendered stigma and traditional cultural practices influencing HIV-related attitudes, programs integrating culturally sensitive dialogues significantly improved openness and willingness to engage with HIV education.
The integration of culturally specific knowledge and behaviour alignment in self-management was shown by Copeland [23] to correlate positively with health outcomes, including reduced stress and illness episodes among Kenyan women. The study underscored the critical role of cultural competence in enhancing the relevance and efficacy of HIV self-management strategies. Furthermore, Okoro et al. [41] found that incorporating culturally congruent frameworks into sexual and reproductive health curricula significantly improved comfort, engagement, and efficacy among African immigrant women.
Sidhu et al. [36] highlighted that culturally tailored interventions facilitated by lay educators with similar cultural backgrounds improved participant engagement and trust in ethnically diverse UK communities. These findings collectively underscore the need for explicit integration of cultural competence into the provision of HIV/AIDS care, emphasizing the alignment of interventions with cultural values, gender norms, and linguistic preferences to optimize care outcomes and community acceptance.
3.3. Theme 2: Impact of Cultural Alignment on HIV Self-management Outcomes
The reviewed studies consistently reported that aligning HIV Self-Management Education Programs (SMEPs) with the cultural contexts of targeted women significantly enhanced health outcomes, including adherence to Antiretroviral Therapy (ART), viral suppression, and overall psychosocial well-being. Robillard et al. [37] reported measurable improvements in clinical indicators following culturally resonant interventions. Specifically, participants showed an increase in viral suppression from 22% at baseline to 38% at six months, sustained at 35% after 24 months. Among those attending regular ambulatory visits and viral load testing, suppression rates further increased from 69% to 82% over the same period. Additionally, ART prescription rates increased significantly, with odds ratios (OR) of 1.42 (95% CI: 1.07–1.89) at 12 months and 1.49 (95% CI: 1.02–2.18) at 24 months. These outcomes underline the effectiveness of culturally tailored narratives that address social determinants, including stigma and healthcare mistrust, in improving clinical management among African-American women.
Similarly, Copeland [23] highlighted the relationship between culturally informed behavioural alignment and better psychosocial outcomes in Nairobi. The study observed significant correlations between cultural consonance and lower perceived stress (mean = 24.9, SD = 9.6) and reduced depressive symptoms (mean = 16.5, SD = 8.2). Stress was positively associated with depression (r = 0.63, p < 0.001) and frequency of illness episodes (r = 0.41, p < 0.001), and negatively associated with self-rated health (r = -0.82, p < 0.001), suggesting that culturally tailored self-management strategies mitigate mental health burdens associated with HIV.
Further reinforcing these findings, Webel et al. [42] provided quantitative evidence linking culturally sensitive social support mechanisms to improved daily health practices and HIV management outcomes among American women. Social capital significantly predicted adherence to daily health practices (R2 = 0.27, p < 0.01), social support engagement (R2 = 0.22, p < 0.01), and chronic HIV management (R2 = 0.27, p < 0.01). These data support the hypothesis that culturally integrated SMEPs positively influence women's health behaviours and clinical outcomes.
Quinlivan et al. [35] and Tufts et al. [18] further documented enhanced care engagement through culturally informed interventions. Quinlivan et al. found that culturally responsive support significantly improved women’s sense of autonomy and competency, facilitating better engagement and retention in care. Tufts et al.'s systematic review of culturally tailored mHealth interventions revealed that culturally specific SMS and text messaging improved ART adherence across multiple randomized trials, demonstrating that culturally-aligned digital strategies can effectively support self-management behaviours.
Collectively, these studies demonstrate that incorporating cultural elements such as values, gender norms, and linguistic preferences into SMEPs contributes substantially to improved HIV-related health outcomes and psychosocial resilience among women living with HIV/AIDS. This alignment facilitates meaningful engagement, enhances adherence to clinical guidelines, and supports comprehensive well-being in diverse cultural contexts.
3.4. Theme 3: Theme 3: Facilitators for Successful SMEP Implementation
Several facilitators enhancing the success and effectiveness of culturally appropriate Self-Management Education Programs (SMEPs) for women living with HIV/AIDS were identified across the reviewed studies. Peer support emerged as a critical enabling factor. Sidhu et al. [36] highlighted the essential role of lay educators from culturally similar backgrounds in establishing trust, promoting participant engagement, and improving rapport within interventions. Similarly, Hawa et al. [43] emphasized safe spaces and tailored educational content as crucial facilitators that validated women's voices and experiences. In Iran, Kashefi et al. [40] reported that family support and improved access to health information significantly facilitated the self-care behaviours of women living with HIV/AIDS.
Rebchook et al. [44] documented that culturally tailored peer navigation, community-based outreach, and incentive structures substantially improved HIV care engagement among transgender women of colour. This approach resulted in notable increases in ART prescription and viral suppression, with odds ratios ranging from 1.42 to 1.98 over 12 and 24 months. Additionally, Quinlivan et al. [35] observed that providing autonomy support and fostering feelings of competency and relatedness among women of colour increased their adherence and retention in HIV care.
3.5. Theme 4: Barriers to Effective Implementation of SMEPs
Consistent barriers to the successful implementation and uptake of culturally appropriate SMEPs were reported in multiple studies. Stigma was among the most frequently cited barriers across various settings. Robillard et al. [37] identified stigma, gender inequality, and mistrust as major impediments faced by African-American women in the southern USA. Similarly, in Canada, Hawa et al. [43] noted significant cultural taboos, male dominance, and community denial as pervasive barriers affecting South Asian immigrant women’s access to HIV prevention and care.
In Kenya, O’Brien and Broom [34] found that patriarchal norms and deeply entrenched spiritual beliefs constrained women's openness about HIV status and adherence to treatment. Copeland [23] further highlighted poverty, limited access to healthcare facilities, and delayed treatment as structural barriers faced by HIV-positive women in Nairobi slums, directly impacting their self-management practices and health outcomes. Additionally, Koech et al. [33] observed that male dominance and restrictive gender roles severely limited women's participation and communication within HIV/AIDS education campaigns in rural Kenya.
3.6. Theme 5: Strategies for Implementation of Culturally Appropriate SMEPs
Implementation strategies for culturally appropriate SMEPs varied yet shared common foundational elements emphasizing community engagement, participatory methods, and culturally resonant educational content. Robillard et al. [37] utilized a narrative-based, community-driven approach, collecting personal stories from HIV-positive African-American women to inform culturally congruent prevention messaging. Similarly, Okoro et al. [41] emphasized participatory curriculum development through focus groups with African-born immigrant women to ensure cultural alignment, gender sensitivity, and increased comfort with intervention content.
Hawa et al. [43] provided actionable recommendations derived directly from community consultations, validating the need for culturally tailored educational interventions for immigrant populations. Tufts et al. [18], in a systematic review of mHealth interventions, noted that culturally adapted mobile health technologies, specifically SMS-based adherence tools, proved effective in improving ART adherence among African American women, underscoring the potential of culturally customized digital strategies.
Sidhu et al. [36] found that employing community lay educators as peer facilitators enhanced program acceptance and trust among ethnically diverse groups, despite challenges in addressing deeply rooted cultural beliefs. Lastly, Rebchook et al. [44] implemented culturally tailored peer support interventions across multiple community-based organizations, demonstrating robust effectiveness in enhancing ART prescription rates and viral suppression among marginalized populations.
Overall, culturally appropriate SMEPs require deliberate integration of community voices, culturally congruent content delivery, peer-based facilitation, and continuous stakeholder involvement to overcome structural and interpersonal barriers, thus achieving effective HIV care engagement and improved health outcomes among diverse groups of women.
Table 3 summarizes and groups the themes into main themes, outcomes measured, key findings, and identified barriers and facilitators. This table synthesizes evidence from included studies to highlight areas of strength and gaps in culturally appropriate Self-Management Education Programs (SMEPs) for women living with HIV/AIDS.
| Main Themes | Outcomes Measured | Key Findings | Barriers / Facilitators Identified |
|---|---|---|---|
| 1. Cultural Competence in Provision of HIV Care | HIV prevention behaviours, ART adherence, engagement in care, and health literacy. | Integration of cultural values, gender norms, and linguistic preferences improved engagement, trust, and HIV knowledge. Cultural competence promoted openness and comfort during HIV education. | Barriers: stigma, gender inequality, mistrust. Facilitators: cultural concordance, peer educators, safe spaces, and linguistic tailoring. |
| 2. Impact of Cultural Alignment on HIV Self-Management Outcomes | Viral suppression, ART adherence, CD4 count, improve psychosocial well-being, and health literacy. | Culturally aligned interventions improved ART uptake, viral suppression (from 22% to 38%), and reduced stress and depression. Social capital and cultural consonance correlated with better self-management and adherence. | Barriers: low social capital, structural poverty. Facilitators: social support, autonomy, culturally aligned health messages, mHealth support. |
| 3. Facilitators for Successful SMEP Implementation | Engagement and retention in care, self-efficacy, ART adherence, and viral suppression. | Peer and lay educators enhanced trust and participation. Family support and safe spaces improved adherence and self-care. Culturally tailored incentives and participatory learning encouraged uptake. | Barriers: lack of training, limited resources, stigma. Facilitators: peer-led education, community participation, incentives, and family involvement. |
| 4. Barriers to Effective Implementation of SMEPs | Access to care, participation rates, and self-management behaviour. | Stigma, patriarchal norms, and cultural taboos constrained disclosure and program participation. Socioeconomic constraints and spiritual beliefs reduced adherence and communication. | Barriers: stigma, gender inequities, cultural taboos, poverty, and lack of agency. Facilitators: community dialogue, cultural openness, and empowerment initiatives. |
| 5. Strategies for Implementation of Culturally Appropriate SMEPs | Engagement in care, ART uptake, viral suppression, knowledge, and behaviour change. | Co-design and participatory frameworks enhanced cultural congruence. Peer-led and narrative-based programs improved acceptance. Culturally adapted mHealth and educational materials improved adherence and engagement. | Barriers: lack of a standardized framework, limited scalability. Facilitators: co-design, participatory approaches, culturally sensitive curricula, and mobile interventions. |
4. DISCUSSION
This scoping review examined fifteen studies that addressed culturally appropriate Self-Management Education Programs (SMEPs) for women of reproductive age living with HIV/AIDS. The findings reveal both emerging strengths and persistent gaps in the design, implementation, and outcomes of such programs across diverse geographical and cultural contexts.
A prominent theme throughout the literature was the explicit infusion of cultural competence in HIV/AIDS care programming. This aligns with growing calls for integrating sociocultural factors into chronic disease management frameworks to address the contextual realities that shape health behaviours [15]. Across studies from the USA, Canada, Kenya, Zimbabwe, and elsewhere, interventions that reflected cultural values, gender dynamics, and linguistic norms were more acceptable and effective. For instance, narrative-based interventions among African American and African immigrant women in the United States [37, 41] demonstrated how the use of culturally familiar storytelling, peer-led dialogue, and gender-sensitive materials enhanced participant trust and engagement. Similarly, programs in Kenya and Zimbabwe showed that community awareness and cultural dialogue were essential in countering stigma and improving participation [23, 34]. These findings reinforce arguments that cultural tailoring, when systematically operationalized, enhances SMEP uptake and alignment with beneficiaries' lived realities [3, 16].
The impact of cultural alignment on self-management outcomes was also evident. Culturally responsive SMEPs were associated with improved ART adherence, higher rates of viral suppression, and reductions in perceived stress and depression. This reflects prior evidence linking cultural tailoring to better clinical outcomes and psychosocial resilience [20, 21]. For example, in Robillard et al. [37], viral suppression increased from 22% to 38% over 6 months and was maintained at 35% at 24 months, while ART uptake and prescription adherence significantly improved. In Nairobi, cultural consonance scores predicted lower perceived stress and depressive symptoms, offering compelling evidence that cultural integration supports psychological coping mechanisms and treatment continuity [23]. Such results resonate with findings from the SEPA and E-WORTH trials, which demonstrated improved HIV-related knowledge and reduced risks through culturally adapted interventions [1, 2].
The analysis also identified facilitators that enhanced program success. Chief among these was the use of peer educators and lay health workers who shared cultural, gender, or social backgrounds with participants. This strategy was particularly effective in improving trust and fostering safe learning environments [36, 44]. Other enablers included the presence of familial and community support, access to tailored health education, and the deployment of mHealth tools with culturally relevant content [18, 43]. These facilitators mirror broader evidence from community-based intervention models that emphasize relational support and local ownership as essential components of sustainable health behaviour change [14, 17].
Conversely, barriers such as HIV-related stigma, patriarchal norms, healthcare mistrust, and lack of culturally adapted materials were pervasive and undermined program implementation. Women’s reluctance to disclose their status, engage with healthcare services, or participate in open discussions around HIV prevention and treatment was frequently linked to sociocultural taboos and gender-based discrimination [8, 10]. Structural factors such as poverty and poor access to healthcare also constrained the effectiveness of SMEPs, particularly in low-resource settings such as rural Kenya and informal settlements in Nairobi [23, 33]. These findings reaffirm previous observations that cultural tailoring alone is insufficient unless accompanied by strategies to address underlying power inequities and material deprivation [13, 25].
Importantly, several implementation strategies stood out across studies. Co-design processes that engaged community members in curriculum development, such as those employed by Okoro et al. [41], ensured cultural congruence and enhanced receptivity. The incorporation of culturally sensitive mHealth platforms offered another promising avenue for improving adherence and reducing structural barriers [22]. Additionally, multi-layered interventions such as those evaluated by Rebchook et al. [44] demonstrated that combining peer navigation, case management, and culturally adapted messaging could achieve significant improvements in viral suppression and ART uptake among marginalized groups. These strategies align with WHO’s recommendation for culturally responsive, community-participatory health programming [45] and offer scalable models for future SMEP development in resource-constrained settings.
In sum, this review highlights both the promise and limitations of current culturally appropriate SMEPs. While evidence suggests they can improve HIV-related health outcomes and psychosocial well-being among women, challenges related to cultural adaptation, scalability, and structural inequity remain unresolved. Future research should focus on rigorously evaluating culturally grounded SMEPs, especially in low- and middle-income countries, and on developing standardized frameworks that facilitate adaptation without sacrificing local relevance.
5. LIMITATIONS OF THE STUDY
This scoping review was subject to several limitations. First, the review only included studies published in English, which may have led to the exclusion of relevant research published in other languages, particularly from non-English-speaking regions with rich cultural diversity. This language restriction potentially limits the comprehensiveness of the cultural perspectives captured.
Second, although the review incorporated a range of study designs, the majority of included studies were qualitative or descriptive in nature, with relatively few employing rigorous experimental or longitudinal designs. As such, causal inferences about the effectiveness of culturally adapted Self-Management Education Programs (SMEPs) remain limited.
Third, the heterogeneity of interventions, outcome measures, and cultural contexts made it challenging to conduct any form of meta-analysis or direct comparison across studies. Variability in the reporting of program components, cultural adaptation strategies, and implementation processes further constrained the ability to synthesize findings quantitatively.
Lastly, most of the included studies were conducted in urban or clinical settings, with limited representation of rural populations, indigenous communities, or humanitarian settings where cultural dynamics and healthcare access may differ substantially. These limitations underscore the need for broader and more inclusive research to fully understand and optimize culturally tailored SMEPs for diverse populations of women living with HIV/AIDS.
CONCLUSION
This scoping review provides a comprehensive synthesis of evidence on culturally appropriate Self-Management Education Programs (SMEPs) for women of reproductive age living with HIV/AIDS. The findings affirm that culturally tailored SMEPs integrate local values, gender norms, and linguistic preferences, which significantly enhance ART adherence, viral suppression, and psychosocial resilience [14]. Across diverse settings, programs that demonstrated cultural competence and alignment with participants' lived realities were more acceptable, engaging, and effective [46].
However, the review also identified persistent gaps in the consistency, standardization, and scalability of such programs. Many interventions lacked systematic frameworks for cultural adaptation and failed to address structural barriers such as stigma, poverty, and gender inequality, which continue to hinder effective program implementation and uptake [47].
To advance the field, future interventions should prioritize co-design approaches that meaningfully engage communities in program development and delivery. There is also a need for implementation research that rigorously evaluates culturally grounded SMEPs using mixed-methods and longitudinal designs, especially in underrepresented regions such as sub-Saharan Africa. Standardized cultural adaptation frameworks, combined with context-sensitive delivery models such as peer-led facilitation and mHealth platforms, hold promise for expanding access and effectiveness.
Overall, culturally appropriate SMEPs represent a critical pathway toward improving HIV outcomes and health equity for women living with HIV/AIDS. Embedding cultural responsiveness into program design, while simultaneously addressing structural determinants, is essential for achieving sustainable and impactful HIV care engagement in diverse global contexts.
IMPLICATION FOR FUTURE RESEARCH
Culturally appropriate educational materials should be developed to reflect local beliefs, languages, and gender norms in order to enhance program relevance and participation. Peer-led and community-based models are encouraged, as they utilize shared lived experiences to foster trust, promote disclosure, and support adherence to Antiretroviral Therapy (ART). Self-management education programs should also integrate psychosocial support components to address stigma, mental health challenges, and self-efficacy, which are essential for sustained engagement in HIV care. Healthcare providers and facilitators require training in cultural competence, participatory teaching methods, and gender-sensitive communication to deliver programs effectively. Standardized monitoring frameworks are necessary to capture both clinical and psychosocial outcomes, allowing for consistent program evaluation and improvement. Finally, these programs should be incorporated into national HIV response strategies, supported by dedicated funding and policy mechanisms to ensure sustainability and alignment with broader health system priorities.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: A.R.D., N.V.S.: Validation; A.B.A.: Writing-Original draft preparation; M.R.M.: Writing- Reviewing and editing. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AIDS | = Acquired Immune Deficiency Virus |
| ART | = Antiretroviral Therapy |
| HIV | = Human Immunodeficiency Virus |
| PCC | = Population, Concept, and Context |
| PRISMA-ScR | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| SMS | = Short Message Service |
| SMEP | = Self-Management Education Program |
| SM | = Self-Management |
| SEPA | = Single Euro Payments Area |
| STI | = Sexual Transmitted Infection |
| WRA | = Women of Reproductive age. |
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [A.A], on a reasonable request.
ACKNOWLEDGEMENTS
The authors wish to thank the University of Pretoria, Faculty of Health Sciences, Nursing Department, for granting permission to conduct the study. The authors also thank the library staff for their support in searching for the literature, Mr. AJM, for assisting with uploading data into Rayyan, and for some relevant IT services.

