All published articles of this journal are available on ScienceDirect.

Prevalence and Associated Factors of Musculoskeletal Disorders among Garment Workers in Haiphong, Vietnam: A Cross-Sectional Study
Abstract
Introduction
Musculoskeletal disorders (MSDs) are a major occupational health problem worldwide. Garment workers are particularly vulnerable due to repetitive movements, awkward postures, and prolonged static work. In Vietnam, evidence on work-related MSDs in this workforce remains limited.
Aims and Objectives
This study aimed to estimate the prevalence of MSDs and identify factors associated with them among garment workers.
Methods
A descriptive cross-sectional study was conducted among 391 garment workers at Hieu Ha Embroider Print Sew Company Limited in Haiphong, Vietnam, using a structured questionnaire covering socio-demographic characteristics, occupational factors, and the extended Nordic Musculoskeletal Questionnaire (NMQ-E). MSDs were defined as pain or discomfort occurring at least once per month or lasting at least one week in the previous twelve months. Multivariable logistic regression was used to identify factors independently associated with MSDs.
Results
The 12-month prevalence of MSDs was 62.7%. The lower back was the most commonly affected body region (39.9% in the past 12 months). Female workers had significantly higher odds of MSDs than males (aOR = 3.7; 95% CI: 2.3-5.8). Overweight workers were more likely to report MSDs compared with those of normal BMI (aOR = 2.5; 95% CI: 1.1-5.9). Occupational factors were also significant, with cutting workers (aOR = 4.3; 95% CI: 1.7-11.3) and workers with more than 10 years of job seniority (aOR = 2.6; 95% CI: 1.1-6.1) showing increased risk.
Discussion
Female sex, overweight, repetitive sewing-line work, and longer job seniority were associated with an increased risk of MSD symptoms.
Conclusion
MSDs were highly prevalent among garment workers, particularly lower back pain, highlighting the need for further research to inform ergonomic and preventive interventions in the Vietnamese garment industry.
1. INTRODUCTION
Musculoskeletal disorders (MSDs), injuries and pain of muscles, joints, tendons, or nerves, are a major global occupational health problem [1]. In 2020, musculoskeletal disorders (MSDs) affected an estimated 494 million people worldwide, more than doubling since 1990. Projections suggest that the number of cases will increase by 115% by 2050, reaching 1.06 billion, with most regions expected to experience increases of no less than 50% [2]. Low back pain is among the leading causes of disability-adjusted life years globally [3]. Work-related MSDs (WMSDs) arise from repetitive tasks, awkward postures, prolonged static work, forceful exertions, and psychosocial stressors [4]. These conditions have an impact not only on workers’ health, productivity, and quality of life but also lead to high costs for enterprises and society [2, 4-6]. The textile and garment industries are particularly prone to WMSDs: workers perform repetitive, precise motions (e.g., sewing, cutting, pressing), often in fixed stooped postures with minimal rest. A recent systematic review of 15,029 garment workers across Asia and Africa reported a pooled 12-month WMSD prevalence of 65.6%, with low back and neck pain most common [7]. Factors such as long working hours, lack of ergonomic seating, and inadequate exercise have been identified as risks for textile workers [8].
In Vietnam, occupational diseases and their prevention are increasingly becoming a concern. Vietnam’s statutory list of occupational diseases covered by social security includes 35 diseases [9, 10]. Nevertheless, MSDs are not currently included in the list of occupational diseases covered by national compensation. Therefore, in this ergonomic context, conducting more in-depth research on musculoskeletal symptoms among textile workers is important to raise community awareness. According to recent research in Vietnam, MSDs are ubiquitously reported in certain types of labour: seafood processing workers [11], waste collectors [12], and, more recently, nurses [13, 14]. MSDs are frequently reported, often in overall health check-up reports, but have not been specifically investigated in this population [15]. Despite the importance of this issue, epidemiological data on garment workers in Vietnam are limited in terms of geographical coverage, workforce characteristics, and analytical assessment of associated factors. The study by Nguyen Minh Hieu et al., which reported a very high prevalence of MSD symptoms at 91.6% [16], was conducted in a single enterprise and mainly provided descriptive prevalence data, which may not fully reflect the occupational conditions of garment workers in other industrial settings in Vietnam. In addition, variations in production organization, ergonomic conditions, workload, and workforce demographics across factories may influence the occurrence of MSDs. Besides, previous studies have suggested that MSDs among garment workers are associated with both individual and occupational factors, including female gender, increased BMI, prolonged job seniority, repetitive movements, awkward posture, and prolonged sitting [7, 17, 18]. Therefore, further studies in different occupational contexts are needed to provide more representative epidemiological evidence and to identify factors associated with MSDs among garment workers.
Hieu Ha Embroider Print Sew Company Limited, a Hai Phong garment factory with approximately 400 workers, had no formal MSD surveillance data. Therefore, this cross-sectional study was conducted to determine the prevalence of work-related MSDs and to identify socio-demographic and occupational factors associated with MSD symptoms among garment workers at this factory. Understanding these factors is crucial to guide workplace ergonomics and health programs.
2. MATERIALS AND METHODS
2.1. Study Design and Population
A descriptive cross-sectional study was conducted among garment workers at Hieu Ha Embroider Print Sew Company Limited, Hai Phong, Vietnam, from December 2024 to May 2025. Inclusion criteria included workers with at least 12 months of employment who were present during the data collection period. Exclusion criteria included workers who declined participation, were pregnant, or were unable to complete the questionnaire. The sample size was calculated using the single proportion formula:
In which α = 0.05;
 p: sample proportion; d: accepted absolute errors = 0.03. The sample proportion was referred to from the study of Nguyen Minh Hieu et al [16], with the percentage of garment workers who had MSDs being 91.6% (p = 0.916), thereby yielding a minimum sample of 329 workers. All eligible workers were invited, and 391 participants were included in the final analysis. This sample size was sufficiently representative and reliable, and ensured adequate statistical power for analyzing differences.
p: sample proportion; d: accepted absolute errors = 0.03. The sample proportion was referred to from the study of Nguyen Minh Hieu et al [16], with the percentage of garment workers who had MSDs being 91.6% (p = 0.916), thereby yielding a minimum sample of 329 workers. All eligible workers were invited, and 391 participants were included in the final analysis. This sample size was sufficiently representative and reliable, and ensured adequate statistical power for analyzing differences.
2.2. Study Questionnaires
Data were collected using a structured questionnaire comprising two components:
- The first part gathered general information on socio-demographic and occupational characteristics, including sex, age, education, marital status, income, job type, work seniority, weekly working days and hours, body mass index, dominant hand, history of musculoskeletal diseases, and use of pain medication.
- The second part employed the extended Nordic Musculoskeletal Questionnaire (NMQ-E), adapted from the original instrument developed by Kuorinka et al. [19] and later expanded by Dawson et al. [20] to cover multiple body regions. The NMQ-E assessed pain or discomfort across nine major anatomical sites (neck, shoulders, elbows, wrists/hands, upper back, low back, hips/thighs, knees, ankles/feet) and symptom frequency during the previous 12 months. Workers were classified as having MSDs if any symptoms (pain or discomfort) occurred at least once per month or lasted one week or longer in any of the nine body regions. The Vietnamese version of this questionnaire has been adapted to the Vietnamese context by several other studies and has been widely used [14, 21]. This study has referenced and used the Vietnamese versions from those studies.
2.3. Data Collection
The questionnaire was pilot-tested to ensure clarity. After obtaining informed consent, eligible workers were invited to participate and completed the questionnaire after work hours, requiring approximately 15-20 minutes. Completed questionnaires were checked for completeness upon submission. All data were anonymized and securely stored. The study protocol was approved by the Ethics Committee of Hai Phong University of Medicine and Pharmacy, and permission was obtained from factory management.
2.4. Statistical Analysis
Data were double-entered and analyzed with Stata 17.0. Descriptive statistics (means ± SD, frequencies, proportions) summarized participant characteristics and MSDs prevalence by body site. Bivariate associations between potential factors and the presence of any MSDs were tested using chi-square or Fisher’s exact tests. Variables with p < 0.05 in bivariate analysis were entered into a multivariable logistic regression to identify independent factors. Adjusted odds ratios (aOR) with 95% confidence intervals (CI) were calculated; p < 0.05 was considered statistically significant.
3. RESULTS
3.1. Participant Characteristics
Among the 391 respondents, 248 (63.4%) were female. The mean age was 35.4 ± 6.2 years (range: 23-47), and the majority were married (88.8%). Most participants had a vocational education (82.3%), while only 0.5% reported a monthly income exceeding 10 million VND. The mean body mass index (BMI) was 21.1 ± 2.0 kg/m2, with 12.6% classified as overweight (23 - 24.9) or obese (≥ 25). A small proportion of workers reported a history of musculoskeletal diseases (3.8%), prior use of pain medication (2.6%), and left-handedness (4.1%).
3.2. Work Organization Characteristics
Most workers were engaged in sewing tasks (70.6%), and the majority had more than 10 years of job seniority (88.2%). The mean duration of work experience was 7.4 ± 3.4 years, ranging from 1.3 to 18.8 years. Approximately two-thirds of participants (62.2%) worked 40 hours or fewer per week, with a mean weekly working time of 43.2 ± 4.6 hours (range: 40-56 hours). Most workers (72.1%) worked five days or fewer per week, with an average of 5.3 ± 0.5 working days (range: 5-7 days) (Table 1).
| Characteristics | Frequency | Percentage (%) | Mean ± SD (Min - Max) | |
|---|---|---|---|---|
| Job titles | Cutting | 64 | 16.4 | - |
| Sewing | 276 | 70.6 | - | |
| Printing | 16 | 4.1 | - | |
| Finish and quality controls | 35 | 8.9 | - | |
|
Seniority (year) |
≤ 10 years | 345 | 88.2 | 7.4 ± 3.4 (1.3 - 18.8) |
| > 10 years | 46 | 11.8 | ||
| Weekly working hours | ≤ 40 hours | 243 | 62.2 | 43.2 ± 4.6 (40 - 56) |
| > 40 hours | 148 | 37.8 | ||
| Weekly working days | ≤ 5 days | 282 | 72.1 | 5.3 ± 0.5 (5 - 7) |
| > 5 days | 109 | 27.9 | ||
3.3. MSDs Prevalences
3.3.1. Distribution of MSDs by Anatomical Regions
Overall, 62.7% of workers reported MSDs in the previous 12 months. Among the 245 workers with musculoskeletal symptoms, single-site involvement was most common (62%), while multisite symptoms were less frequent. Specifically, involvement of two to five anatomical sites accounted for 35.6% of cases, whereas symptoms affecting more than five sites were rare (2.4%) (Fig. 1).
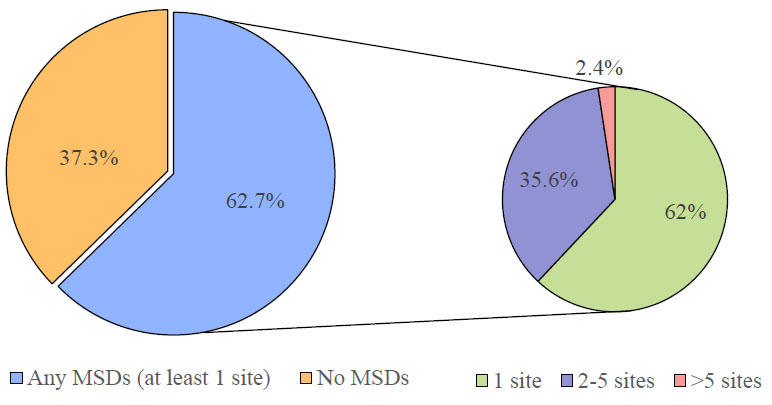
Prevalence of MSDs among workers during the last 12 months (n=391).
Low back pain (LBP) showed the highest prevalence across all time periods. Lifetime prevalence of LBP was 45.6%, and it remained the most common MSD in the previous 12 months (39.9%) and the past 7 days (15.6%). In contrast, hip/thigh disorders consistently had the lowest prevalence, remaining below 5% across all three time intervals (Fig. 2).
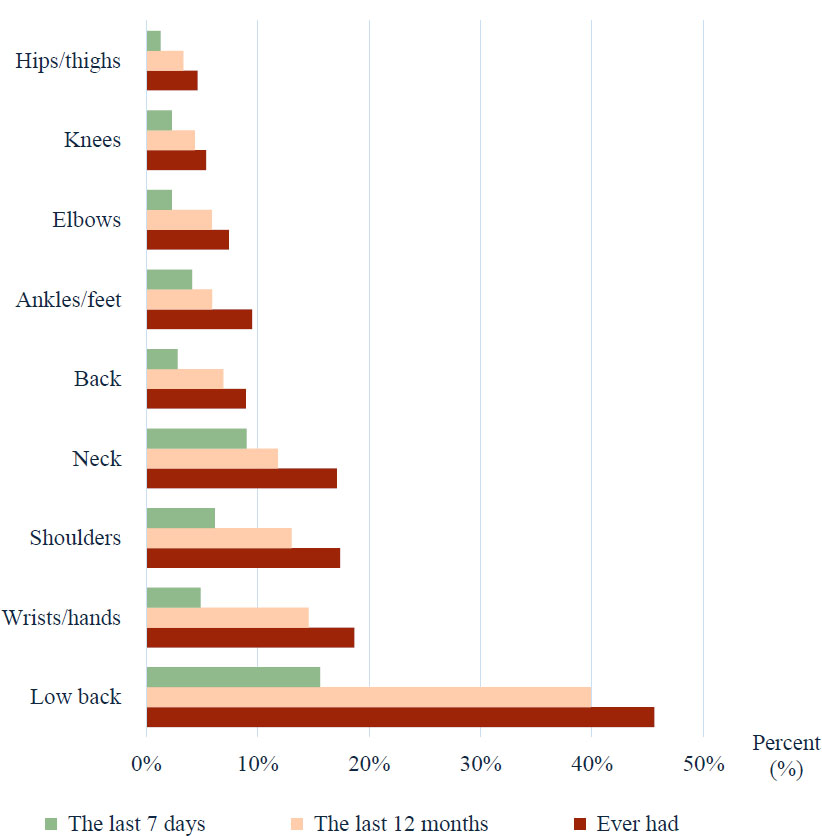
The prevalence of MSDs in body parts during different periods (n=245).
3.3.2. Consequences of MSDs
Figure 3 illustrates the work-related consequences of self-reported MSDs. Reduced work activities were most frequently reported for low back pain (15.4%), followed by wrist/hand disorders (8.7%). Shoulder disorders accounted for the highest proportion of workers prevented from performing normal work (4.1%), while low back pain was the leading cause of health care utilization, with 2.3% of workers reporting visits to health professionals (Fig. 3).
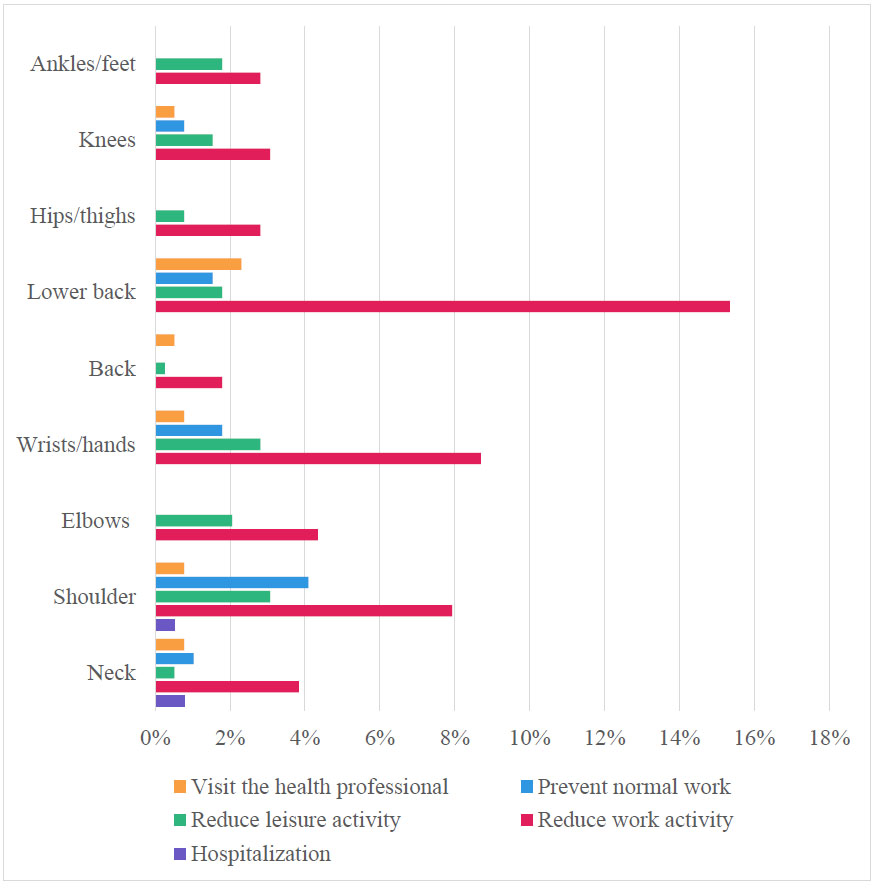
The consequences of MSDs in 9 body regions (n=245).
3.4. Factors associated with MSDs
3.4.1. Bivariate Analysis
Bivariate analysis was first performed using the following variables: gender, age groups, educational levels, marital status, BMI groups, seniority, job titles, working hours, working days, history of musculoskeletal diseases, dominant hand, and painkiller history. The results showed that female workers had a significantly higher prevalence of MSDs than males (74.2% vs. 42.7%, p < 0.001); overweight workers were more likely to report MSDs than those with normal BMI (OR = 2.6 (1.2 - 5.8); p = 0.021); job title and work seniority were significantly associated with MSDs, with higher prevalence observed among cutting, sewing, and printing workers, as well as among workers with more than 10 years of service (p < 0.05) (Table 2).
| Factors | MSDs |
OR 95% CI |
p | ||
|---|---|---|---|---|---|
|
Yes n (%) |
No n (%) |
||||
| Gender | Female | 184 (74.2) | 64 (25.8) | 3.9 (2.4 - 6.1) |
< 0.001* |
| Male | 61 (42.7) | 82 (57.3) | |||
| BMI groups | 18,5 - 22,9 (Normal) | 192 (60.0) | 128 (40.0) | reference | - |
| < 18,5 (Underweight) | 16 (72.7) | 6 (27.3) | 2.2 (0.7 - 4.7) |
0.242*** | |
| 23 - 24.9 (Overweight) | 31 (79.5) | 8 (20.5) | 2.6 (1.2 - 5.8) |
0.021*** | |
| ≥ 25 (Obesity) | 6 (60.0) | 4 (40.0) | 1 (0.3 - 3.6) |
> 0.99*** | |
| Seniority | > 10 years | 38 (82.6) | 8 (17.4) | 3.2 (1.4 - 7) |
0.003* |
| ≤ 10 years | 207 (60) | 138 (40) | |||
| Job titles | Finish and quality controls | 14 (40.0) | 21 (60.0) | reference | - |
| Cutting | 50 (78.1) | 14 (21.9) | 5.4 (2.2 - 13.2) |
< 0.001*** | |
| Sewing | 169 (61.2) | 107 (38.8) | 2.4 (1.2 - 4.8) |
0.019*** | |
| Printing | 12 (75.0) | 4 (25.0) | 4.5 (1.2 - 16.8) |
0.025*** | |
(**): Fisher's Exact Test.
(***): Bivariate logistic regression.
3.4.2. Multivariable Logistic Regression Analysis
Table 3 presents the multivariable logistic regression results. Female gender (aOR = 3.7; 95% CI: 2.3-5.8), overweight status (aOR = 2.5; 95% CI: 1.1-5.9), working in cutting positions (aOR = 4.3; 95% CI: 1.7-11.3), and job seniority exceeding 10 years (aOR = 2.6; 95% CI: 1.1-6.1) were independently associated with MSDs. All associations were statistically significant (p < 0.05) (Table 3).
| Variables | aOR | 95% CI | p |
|---|---|---|---|
| Gender | |||
| Female | 3.7 | 2.3 - 5.8 | <0.001 |
| Male | reference | - | - |
| BMI groups | |||
| Overweight | 2.5 | 1.1 - 5.9 | 0.048 |
| Normal | reference | - | - |
| Working position | |||
| Cutting | 4.3 | 1.7 - 11.3 | 0.003 |
| Sewing | 2.1 | 0.9 - 4.6 | 0.054 |
| Printing | 3.3 | 0.8 - 13.2 | 0.085 |
| Finish and quality controls | reference | - | - |
| Seniority | |||
| > 10 years | 2.6 | 1.1 - 6.1 | 0.027 |
| ≤ 10 years | reference | - | - |
4. DISCUSSION
The present cross-sectional survey of 391 garment workers reveals a high burden of MSDs and identifies key demographic and occupational factors associated with MSDs. In this workforce, 63.4% of employees were female, and the mean age was 35.4 years (SD 6.2). This female predominance mirrors broader industry trends: in Vietnam’s textile and garment sector, roughly 75% of workers are women [22], and similarly, high proportions of women (60-80%) are reported in garment workforces elsewhere [23, 24]. Notably, only 3.8% of participants reported a prior history of MSD, and only 2.6% were using pain medication, suggesting that most musculoskeletal symptoms in this group were newly arising or unmanaged prior to the study.
4.1. Prevalence and Patterns of MSDs
According to a recent analysis of the Global Burden of Disease 2021 data, musculoskeletal disorders remain a major contributor to disability in Asia, accounting for nearly 120 million DALYs in 2021, an increase of 94% compared with 1990. Low back pain was identified as the leading contributor to DALYs among musculoskeletal conditions, followed by osteoarthritis and rheumatoid arthritis. The study also highlighted the substantial impact of occupational and lifestyle-related risk factors, emphasizing the urgent need for targeted prevention, workplace interventions, and rehabilitation strategies across Asian countries [25].
MSDs were widespread among garment workers. Overall, 62.7% of employees reported pain or discomfort in at least one anatomical site over the past 12 months. This high prevalence is consistent with international findings: a recent systematic review and meta-analysis of 15,029 garment workers (across 9 countries) reported a pooled 12-month MSD prevalence of 65.6% [7]. In our study, the distribution of pain sites was uneven. The lower back was by far the most affected region: 39.9% of workers reported lower back pain in the past 12 months (45.6% over the lifetime), and 15.6% reported low back pain in the past 7 days. Other regions had much lower 7-day prevalence (<1%), with only wrist/hand (1.8%), neck (1.6%), and shoulder (1.4%) exceeding 1%. This contrasts with some reports from other settings. For example, Van et al. (2016) found that 89.0% of Cambodian garment workers reported symptoms in the past 7 days, with neck (54.7%) and shoulder (54.4%) most affected [26]. Similarly, a study of Bangladeshi workers reported 77.1% 7-day prevalence, with shoulder (17.9%) and lower back (15.2%) most common [23]. The much lower acute symptom prevalence in our Vietnamese sample (15.6% for low back and <2% for other sites) may reflect differences in work tasks, reporting practices, or recall periods.
The pattern of chronic symptoms (12-month prevalence) in our study also aligns with prior reports. In our study, 62.7% of workers had pain in at least one site in the past year. This is comparable to the 65-92% 12-month prevalence reported in other garment worker studies [7]. For instance, Hieu and Quynh (2018) found that 91.6% of female sewing operators at a Vietnamese garment factory had musculoskeletal pain in at least one site over 12 months [16]. In that study, lower back (44.1%), shoulder (41.1%), and neck (34.2%) were the most common pain sites, with most women reporting pain in only one region [16]. In the present factory, single-site pain was also predominant: among the 245 workers with any MSD, 62.0% had only one painful region. The proportion with multi-site pain (35.6% with pain in 2-5 regions, 2.5% in >5 regions) was substantial but somewhat lower than some reports (for example, Shazzad et al. found that 49.4% of Bangladeshi workers had pain in multiple regions [23]).
Among workers with MSDs, 15.4% reported reduced work capacity due to low back pain, and smaller proportions reported reduced capacity for wrist/hand (8.7%) or shoulder pain (7.9%). Leisure and social activities were less frequently affected (up to 4.1% for shoulder), and only very short work absences (1-7 days) occurred (predominantly for wrist/hand and low back). These impact figures suggest that most MSD episodes were mild to moderate in severity and were largely self-managed rather than medically treated.
4.2. Factors associated with MSDs
The present study identified gender, body mass index (BMI) group, working position, and seniority as statistically significant factors independently associated with MSDs among garment workers. These findings underscore the multifactorial nature of MSDs and highlight the combined influence of biological, ergonomic, and occupational exposure-related determinants.
4.2.1. Gender and MSDs
Gender emerged as one of the strongest independent predictors of MSDs in the multivariable logistic regression model. After adjusting for confounding factors such as working position and seniority, female workers had 3.7 times higher odds of experiencing MSDs compared with male workers (p < 0.001). This finding is consistent with evidence from Ethiopia, where Zele et al. (2021) reported a significantly increased risk of MSDs among female garment workers after multivariable adjustment (adjusted OR = 1.29; p < 0.001) [24]. Similar gender disparities have been widely documented in South and Southeast Asia. For example, Hossain et al. (2018) found a significantly higher prevalence of work-related MSDs among female garment workers in Bangladesh [17], while Van et al. (2016) reported comparable findings in Cambodia [26]. These differences may be attributed to sex-related musculoskeletal characteristics as well as the dual burden faced by many women, who combine physically demanding work with household and caregiving responsibilities. From a policy perspective, gender-sensitive ergonomic interventions, such as task redistribution, improved workstation design, and targeted occupational health education, are essential to reduce MSD risk among female workers.
4.2.2. BMI Group and MSDs
BMI also emerged as a significant factor associated with MSDs. Workers classified as overweight exhibited a substantially higher prevalence of MSDs (79.5%) compared with those with normal BMI (60%), with an odds ratio of approximately 2.5 (p = 0.048). This finding is consistent with biomechanical theories and epidemiological evidence indicating that excess body weight increases mechanical loading on the spine and weight-bearing joints, thereby elevating the risk of musculoskeletal pain and dysfunction. Previous studies among garment workers in Bangladesh have similarly suggested that higher body weight is associated with increased musculoskeletal strain during prolonged static and repetitive tasks [17]. These findings highlight the importance of integrating workplace health promotion programs that include physical activity encouragement, nutritional counseling, and ergonomic training tailored to overweight workers.
4.2.3. Working Position and MSDs
Regarding working positions, the study revealed pronounced differences in MSD risk across occupational roles. Workers engaged in cutting tasks experienced the highest prevalence of MSDs (78.1%) and were more than five times as likely to develop MSDs compared with those in finishing and quality control positions (OR ≈ 5.4; p < 0.001). Sewing machine operators also demonstrated an elevated risk (61.2%; OR ≈ 2.4; p = 0.019), although to a lesser extent than cutting workers. These findings are consistent with research from Cambodia, where Van et al. (2016) reported significant associations between work type and MSD prevalence, particularly among workers exposed to prolonged standing, repetitive movements, and forceful manual tasks [26, 27]. Similar conclusions were drawn in Bangladesh by Hossain et al. (2018) [17]. Cutting tasks typically involve prolonged standing, frequent trunk flexion, and repetitive upper-limb exertion, which may explain the elevated risk. Practical interventions should therefore focus on ergonomic redesign, such as adjustable worktables, anti-fatigue mats, job rotation, and scheduled micro-breaks for stretching and recovery.
4.2.4. Seniority and MSDs
Job seniority was identified as another independent risk factor for MSDs. Workers with more than 10 years of experience had a significantly higher prevalence of MSDs (82.6%) compared with those with 10 years or less (60%), with an odds ratio of approximately 2.6 (p < 0.05). This finding corroborates results from Bangladesh, where longer employment duration was significantly associated with MSD prevalence among garment workers [17]. Furthermore, a study conducted in Tunisia by Rmadi N. et al. (2024) reported that each additional year of job seniority increased the likelihood of developing multisite musculoskeletal symptoms (OR = 1.11; p < 0.001) [28]. This trend is also supported by research in Ethiopia’s textile sector, where longer work experience correlated with increased WMSDs prevalence [29]. The cumulative exposure hypothesis offers a plausible explanation, as prolonged exposure to repetitive motions, awkward postures, and sustained physical demands may progressively impair musculoskeletal structures. Occupational health policies should therefore prioritize senior workers by implementing periodic health screening, ergonomic support, task modification, and flexible work arrangements.
4.2.5. Integrated Interpretation of the Logistic Regression Model
The binary logistic regression model explained approximately 13.2% of the variance in MSD occurrence, a figure typical of occupational health studies involving complex, multifactorial outcomes. The results indicate female sex, overweight BMI, certain working positions, and longer job seniority as statistically significant associated factors for MSDs among garment workers. These findings are consistent with global evidence indicating high MSD prevalence in the garment and textile industries due to repetitive tasks and ergonomic risk factors [7].
These findings suggest that MSD prevention in the garment industry requires a multilevel approach that combines ergonomic redesign of workstations, task rotation for high-risk positions, health promotion strategies targeting modifiable risk factors such as BMI, and targeted surveillance for long-serving and female workers. Addressing these factors simultaneously is likely to yield greater reductions in MSD burden than isolated interventions.
5. STRENGTHS AND LIMITATIONS
This study benefits from a high participation rate and the use of a standardized questionnaire, slightly modified for the Vietnamese context, allowing comparison with published benchmarks. However, it is limited by its cross-sectional design, self-reported outcomes, and lack of multivariate risk modeling. Furthermore, biomechanical factors were not comprehensively assessed in this study and were evaluated solely through self-reported questionnaire data. No physical examinations, ergonomic assessments, or objective exposure measurements, such as posture observation, repetition frequency analysis, or force estimation, were conducted. Future research could explore additional related groups of factors (e.g., psychosocial and biomechanical factors), examine causal links, and evaluate interventions. Nonetheless, the data clearly indicate that MSDs are a current concern among Hieu Ha’s garment workers, necessitating ongoing occupational health attention.
CONCLUSION
Musculoskeletal symptoms are common among garment workers, with lower back pain predominating. Female gender, overweight, repetitive sewing-line work, and longer job seniority can increase MSD symptoms. These results highlight the need for targeted ergonomics and health programs to protect this vital workforce, consistent with Vietnam’s broader emphasis on women’s occupational health.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: H.T.N., H.T.N.: Study conception and design; H.T.N.: Data collection; H.T.N., H.T.N.: Analysis and interpretation of results; H.T.N.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MSDs | = Musculoskeletal disorders |
| NMQ-E | = Extended Nordic Musculoskeletal Questionnaire |
| WMSDs | = Work-related musculoskeletal disorders |
| BMI | = Body mass index |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the research project approval committee of Haiphong University of Medicine and Pharmacy under Decision No. 3052/QD-YDHP dated December 20, 2024.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of our study are available upon request from the corresponding author, Hai T Nguyen, with the following contact information: nthanhhai@hpmu.edu.vn.
FUNDING
This research received no external funding, and the APC was partially supported by Hai Phong University of Medicine and Pharmacy.
ACKNOWLEDGEMENTS
We would like to express our sincere appreciation for the permission and support provided by the Board of Directors of Hieu Ha Embroider Print Sew Company Limited in Haiphong, Vietnam. We are deeply grateful to all workers who generously agreed to participate in this study. We also extend our heartfelt thanks to the students from Hai Phong University of Medicine and Pharmacy for their valuable assistance in data collection and entry. During the preparation of this manuscript, the authors used ChatGPT (OpenAI) for grammatical editing and language refinement. The authors have reviewed and edited the output and take full responsibility for the content of this publication.

