All published articles of this journal are available on ScienceDirect.

Practice Management in Audiology and Speech-Language Therapy: A Global Narrative Review of Practitioner Perspectives on Operational and Leadership Challenges
Abstract
Background
Effective practice management is essential for the delivery, accessibility, and sustainability of audiology and speech-language therapy services. However, growing evidence suggests that practitioners are often underprepared for the administrative, financial, and leadership demands of their roles.
Objectives
This narrative review examines how practitioners across different countries describe their experiences with managing audiology and speech-language therapy practices. The review synthesises peer-reviewed literature that captures the challenges, strategies, and recommendations reported by clinicians working in diverse healthcare contexts.
Methods
A structured narrative review methodology, incorporating systematic search and screening procedures, was adopted. A total of 192 records were identified through database searching, of which 182 remained after duplicate removal. Following title and abstract screening, 37 full-text articles were assessed for eligibility, and 16 studies met the inclusion criteria. Sixteen peer-reviewed publications published between 2000 and April 2025 were identified through systematic database searches. Studies were included if they presented practitioner perspectives on any aspect of practice management. Thematic analysis was used to synthesise the data.
Results
The analysis revealed nine interrelated themes: limited business and financial training; reimbursement complexities; ethical dilemmas; high workload and burnout; barriers to continuing professional development; private practice management challenges; gaps in human resource capacity; insufficient policy engagement; and the importance of interprofessional collaboration and person-centred care. Studies from high-, middle-, and low-income countries highlighted both globally shared and context-specific barriers. Practitioners emphasised the need for embedded business skills training, improved access to continued professional development (CPD), supportive regulatory environments, and clearer guidance from professional bodies.
Discussion
The findings indicate that practice management challenges are systemic rather than isolated, reflecting broader gaps in health workforce preparation and policy support. The recurrence of similar themes across diverse settings highlights the need for integrated training models that combine clinical expertise with leadership, financial, and advocacy competencies to ensure sustainable and equitable service delivery.
Conclusion
The results of the study highlight the global need for integrated, context-sensitive preparation in practice management within health professions education and systems. This review provides actionable insights to inform reforms in training, policy, and organisational support, better equipping practitioners for sustainable, high-quality service delivery.
1. INTRODUCTION
Optimizing the administration and strategic development of clinical services is critical for ensuring the financial viability and therapeutic efficacy of audiology and speech-language therapy practices [1, 2]. These two allied health fields navigate unique systemic challenges due to diverse operational footprints that span independent private clinics, acute care hospitals, schools, and community health settings [3, 4]. Furthermore, the regulatory environments governing these professions vary significantly across different countries, and the landscape of healthcare technology and policy is continuously evolving. These global challenges are mirrored within the South African landscape. Recent findings by Sebothoma et al. [2] indicate that a significant cohort of early-career audiologists is leaving the profession or emigrating, driven by a scarcity of public-sector employment options and a parallel lack of the business acumen required to successfully navigate private practice. These authors assert that the disjunction between clinical training and real-world management demands has resulted in a mismatch between the curriculum and market needs, particularly acute in Low- and Middle-Income Countries (LMICs), where health entrepreneurship is a matter of survival, not choice.
The ability to navigate these complexities through sound practice management is critical for the sustainability and growth of audiology and speech-language therapy services, for supporting practitioners' well-being by mitigating issues such as burnout, and ultimately for optimising client outcomes and satisfaction. The multifaceted nature of practice management in these fields encompasses financial oversight, human resource management, service delivery optimisation, ethical considerations, and the effective integration of technology [2, 5, 6]. A comprehensive understanding of these interdependent elements is essential for successful practice operations. Given the global scope of healthcare, it is also necessary to consider how practice management challenges and solutions may differ across various healthcare systems and cultural contexts [7]. Despite the recognised need for clinical competence, there is growing global awareness that practitioner success also relies on sound business and management acumen [2, 4, 8]. This growing expectation reflects a shift in health professional roles, where clinicians are increasingly required to function not only as service providers but also as managers, leaders, and system navigators within complex healthcare environments. In contexts such as South Africa, where structural inequities intersect with professional challenges, business training remains insufficiently addressed, as evidenced by recent work highlighting the economic vulnerability of audiologists without business training [2].
This lack of practice management competency presents not only a professional development concern but a broader health systems challenge. Deficiencies in financial, administrative, and strategic management skills directly influence workforce sustainability, service access, and the quality of client care, particularly in under-resourced settings [9]. In this regard, inadequate practice management capacity among allied health professionals impairs the health system’s ability to respond effectively to population needs. Globally, allied health workforce shortages remain a persistent concern, particularly in LMICs, where resource constraints and uneven workforce distribution limit service access. Within the World Health Organisation (WHO)’s Health Systems Framework, these challenges are closely linked to weaknesses in the ‘health workforce’ building block, reinforcing the need for training models that integrate both clinical and managerial competencies [10]. This study is conceptually informed by the WHO’s Health Systems Framework, specifically its ‘health workforce’ and ‘service delivery’ building blocks, which emphasise the necessity of well-trained, well-supported practitioners to ensure equitable, efficient, and effective care [10].
Practitioners, as individuals directly engaged in the daily operations and strategic planning of audiology and speech-language therapy services, possess invaluable insights into the practical realities of practice management. Their perspectives can illuminate everyday challenges, effective strategies, and areas for improvement in ways that may not be fully captured by quantitative data or policy documents. A narrative synthesis of these perspectives holds the potential to provide a rich and nuanced understanding of the global landscape of practice management within these specialised fields. This understanding can inform evidence-based improvements in how practices are organised and run, ultimately benefiting practitioners and the clients they serve. Therefore, this narrative review aims to strategically synthesise the existing global peer-reviewed literature that captures the perspectives, experiences, and issues raised by audiologists and speech-language pathologists regarding various aspects of practice management. The intention is to identify key themes, barriers, enablers, and recommendations that emerge from these practitioner viewpoints, contributing to a more comprehensive understanding of the factors influencing the effective management of audiology and speech-language therapy practices worldwide. This study responds to these global and local imperatives by analysing international practitioner perspectives on practice management, illuminating both shared and context-specific challenges, and opportunities for curriculum reform and policy development. The synthesis presented here offers timely insights to inform policy alignment, workforce planning, and curriculum design in support of stronger, more resilient health systems, especially in LMIC contexts.
To address these gaps, this review adopts a structured narrative approach that integrates systematic search principles with interpretive thematic synthesis, enabling both methodological transparency and in-depth exploration of practitioner experiences.
2. METHODS
This study adopts a narrative review methodology, guided by the Scale for the Assessment of Narrative Review Articles (SANRA) framework, to synthesise the global peer-reviewed literature concerning practitioner perspectives on strategic practice management in audiology and speech-language therapy. A narrative review approach is appropriate for this topic due to its exploratory nature and the goal of synthesising diverse perspectives rather than statistically aggregating findings [11]. While narrative in design, this review incorporated systematic search and screening procedures to enhance transparency and reproducibility, thereby reflecting a hybrid methodological approach. This method provides a broad overview of the existing literature and identifies key themes and trends. To ensure rigor and transparency, the narrative review followed a structured approach encompassing literature search, selection, and synthesis.
The literature search involved a systematic exploration of several electronic databases to identify relevant peer-reviewed articles. These databases included PubMed, Scopus, Web of Science, and Google Scholar. Additionally, discipline-specific databases such as CINAHL and PsycINFO were considered due to their coverage of journals relevant to audiology and speech-language pathology. A comprehensive list of keywords and search terms was utilised, incorporating both general practice management terms and specific terms related to audiology and speech-language therapy. Examples of search terms included: “practice management” AND “audiology” OR “speech-language therapy”; “clinic administration” AND “audiology” OR “speech-language pathology”; “private practice” AND “audiology” OR “speech-language therapy”; “school-based SLP management”; “audiology business”; “speech therapy administration”; “practitioner perspectives” AND “audiology” OR “speech-language therapy” AND “management”; “clinician experiences” AND “audiology” OR “speech-language therapy” AND “administration”; “challenges in audiology practice”; “issues in speech therapy management”; “global” OR “international” AND “practice management” AND “audiology” OR “speech-language therapy”; and combinations of management areas (HR, finance, service delivery, etc.) with “audiology” or “speech-language therapy” and terms like “perspectives,” “experiences,” “challenges,” “barriers,” “enablers,” and “recommendations.” Boolean operators (AND, OR) and truncation symbols were employed to optimise the search strategy and ensure comprehensive retrieval of relevant literature. The search strategy strictly focused on peer-reviewed articles, explicitly excluding grey literature such as conference abstracts, reports, and theses unless published in peer-reviewed journals. The final search was conducted in April 2025. The study selection process, depicted in a PRISMA-style flow diagram (Fig. 1), is summarised as follows: 192 records were initially identified through database searching, with 182 remaining after duplicate removal. Following title and abstract screening, 145 records were excluded. Thirty-seven full-text articles were assessed for eligibility, of which 21 were excluded for not meeting inclusion criteria (e.g., lack of practitioner perspective, focus on clinical interventions only). A total of 16 studies were included in the final qualitative synthesis.
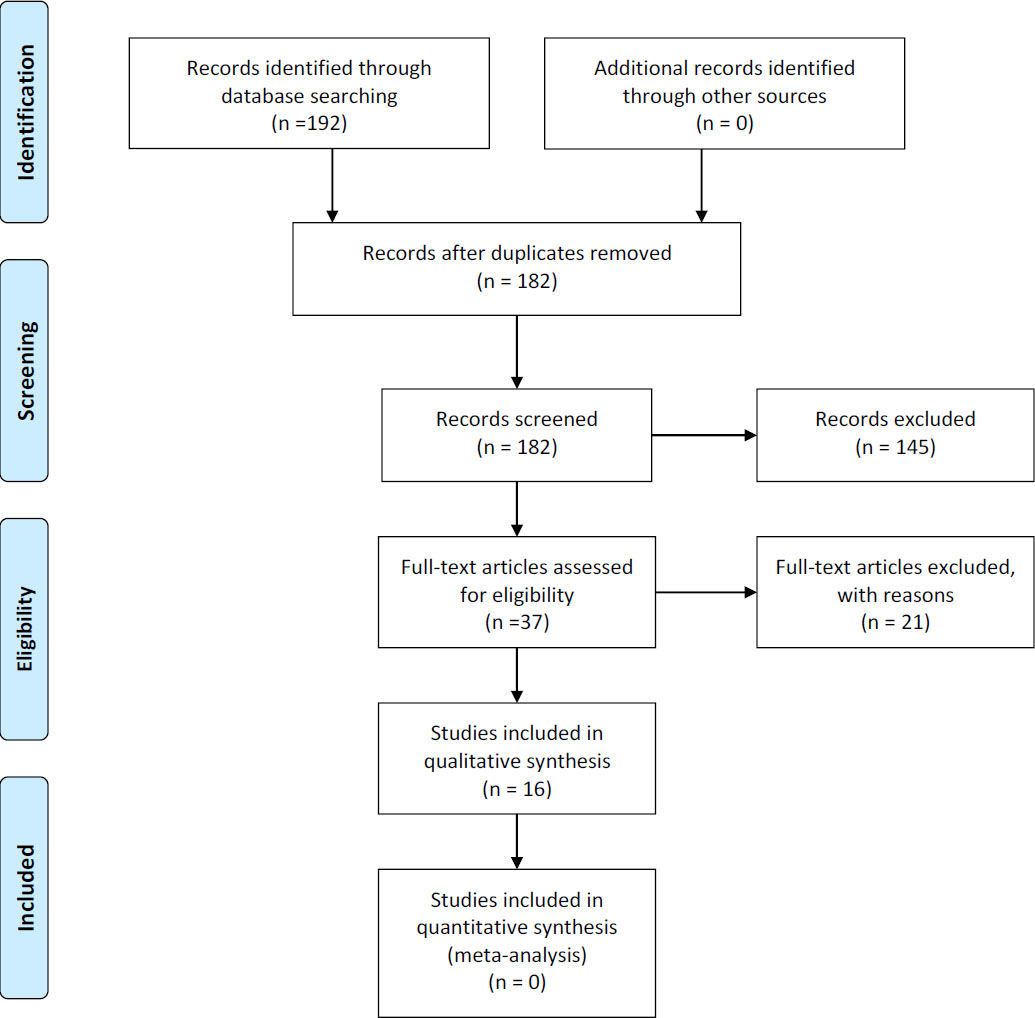
PRISMA-style flow diagram depicting the study selection process.
The inclusion criteria for this review were peer-reviewed publications in scholarly journals published between 2000 and April 2025 that explicitly focused on, or provided significant insights into, the perspectives, experiences, and issues related to practice management as perceived by audiologists and/or speech-language pathologists. Publications addressing practice management in any setting (e.g., private practice, hospitals, schools, community clinics, telehealth) with a global or international focus, representing diverse geographic regions and healthcare systems, and published in English were considered for inclusion. The restriction to English-language publications was based on feasibility and resource constraints; however, this may have resulted in the underrepresentation of non-Anglophone perspectives, particularly from LMICs. Exclusion criteria encompassed non-peer-reviewed publications, studies solely focused on clinical interventions or diagnostic procedures without addressing practice management, articles primarily discussing patient perspectives without significant practitioner input on management issues, studies focused on the management of other healthcare professions unless providing highly relevant comparative insights, and articles not accessible through institutional subscriptions or open access.
The study selection process involved a systematic screening of identified articles. Initially, titles and abstracts were screened based on the inclusion and exclusion criteria. Subsequently, full-text articles of those passing the initial screening were retrieved and assessed against the criteria. Any disagreements regarding article inclusion were resolved through discussion. Finally, the reference lists of included articles were manually searched to identify additional potentially relevant studies.
Data extraction from the 16 included studies was conducted using a standardised data extraction form, based directly on the evidence table (Table 1). The following data points were extracted for each study: Citation (Author(s), year, title, journal), Country/Region, Study Design, Population (Type of practitioners involved, number, demographics), Practice Setting, Management Area(s) (Human Resource, finance, service delivery, tech, policy, ethics, client management, etc.), Key Themes (Summarised practitioner perspectives, experiences, and issues raised), Barriers or Enablers, Recommendations, and Relevance to Global Insights. The data extraction process was performed to ensure accuracy and consistency across the included studies.
| Citation | Country/Region | Study Design | Population | Practice Setting | Management Area(s) | Key Themes | Barriers or Enablers | Recommendations | Relevance to Global Insights |
|---|---|---|---|---|---|---|---|---|---|
| Eakin et al (2022) [20] | Australia | Prospective cohort inter-rater agreement study | 50 children aged 0–16 years with middle ear and hearing concerns | Paediatric primary contact clinic at a public hospital | Diagnosis and management of paediatric hearing concerns | High agreement on diagnosis, substantial agreement on management, disagreements on timing of Ear, Nose, and Throat (ENT) review and discharge criteria | Enabler: Objective testing, established pathway, and audiologist experience. Barrier: ENT review based solely on written information. | Further research with larger samples and in-person ENT assessment. Investigate re-referral rates and accelerated pathways. Explore applications in remote areas. | Supports audiology-led primary contact models for improved access and efficiency in paediatric ENT care globally. Highlights considerations for implementation in different healthcare systems. |
| Granberg & Skagerstrand (2022) [21] | Sweden | Feasibility study (post-only design, reflections, focus group) | 4 licensed audiologists (25 adult audiologic rehabilitation patient interviews) | Audiological clinic (umbrella clinic with three subunits) | Audiologic rehabilitation, person-centred care, clinical implementation of assessment tools | Promoted person-centred care, deeper information gathering, and enhanced patient participation. Rehabilitation plans remained largely the same. | Barriers: Unfamiliarity with using all info, managing emotional responses, lack of referral routines, time limitations, and lack of organisational focus on person-centred care. Enablers: ICF-based tool, sharing tool outline, structured reflections, pre-implementation education, collegial discussions. | Consider time implications; provide additional training (psychological, lifestyle factors, referrals); foster a person-centred culture; implement structured reflections; consider ICF principles; and improve documentation. | Relevance for the global audiology community in enhancing person-centred approaches to rehabilitation. Identifies common barriers and enablers for implementing such tools. |
| Byrne et al. (2012) [22] | United States | Perspective piece | Population at risk for hearing loss across various settings | Clinical audiology practices, community events, and public health campaigns | Awareness and education, intervention programmes, risk assessment, hearing protection, public health campaigns, monitoring outcomes, advocacy | Crucial role of audiologists in hearing loss prevention beyond occupational settings. Unique qualifications to educate and implement interventions. Importance of shaping public knowledge and behaviours. | Implicit enablers: Audiologist's education, tools, opportunity, and strategic position. Potential barrier: Perception that prevention is solely industrial audiology. | Audiologists should take a more active role in all aspects of prevention. Educate on noise measurement and hearing protection. Minimise risks at community events. Shape public behaviours. Promote surveillance and prevention services. | Highly relevant globally, as noise-induced hearing loss is a significant public health issue. Recommendations applicable across different countries and healthcare systems. |
| Bennett et al. (2020) [6] | Australia | Concept mapping | GPs (n=8), adults with hearing loss (n=22), professionals working with GPs (n=5) | Primary care (General Practice) | Management of age-related hearing loss | Six key concepts describing the GP's role: determine-diagnose-discuss, ask-assess-act, know-refer-coordinate, inform-advise-partner, educate-strategise-encourage, reassure-support-empower. | Explored perceived barriers and facilitators to hearing loss identification and management in primary care. | The GP role is multifaceted and requires partnership. Enlisting practice nurses, managers, and audiologists could help. Incorporation of routine hearing screening programmes. | Highlights the crucial role of primary care physicians in the early detection and management of age-related hearing loss globally. Recommendations relevant to primary care systems in other countries. |
| Barath & Ross (2024a) [17] | South Africa | Descriptive qualitative (semi-structured online interviews) | 11 young audiologists (23-26 years) in the private sector | Private sector audiology practices | Continuing Professional Development (CPD) | Five key themes aligned with andragogy: self-concept, adult learning experience, readiness to learn, orientation to learning, and internal motivation. | Enablers: Personal responsibility, informal learning, desire to stay updated, relevant CPD content, perceived skill improvement, and interprofessional CPD. | CPD planning should consider audiologists' experiences. Integrate insights to foster higher compliance. Tailor programmes using andragogy. Encourage peer interaction and interprofessional activities. | Highlights the importance of understanding healthcare professionals' perspectives on CPD globally. Findings on andragogy are relevant to designing effective programmes internationally. |
| Hlayisi et al. (2024) [7] | Multiple (South Africa, India, Nigeria, Brazil, Tunisia, Bhutan, Thailand, Malaysia, Sri Lanka, Nepal) | Not specified | Audiologists and potentially other stakeholders in hearing healthcare | Various audiology practice settings | Global professionalisation of audiology, historical evolution of practice | Historical development of audiology practice, global professionalisation, and influence of context on best practice. | Not explicitly detailed. | Emphasis on context-specific best practices in audiology. Consideration of resources, culture, and individual needs. | Highlights the need for culturally competent, contextually appropriate audiology services worldwide, especially in resource-limited settings. |
| Kleih et al. (2016) [23] | Germany | Pilot feasibility study | 5 participants with post-stroke aphasia (motor) | Rehabilitation clinic | Aphasia rehabilitation, BCI technology, communication tools | Potential of BCI for communication and neuronal plasticity in aphasia rehabilitation. Feasibility of the visual P300 speller with adjustments. | Barriers: Heterogeneous stroke symptoms, initial inability to use standard BCI, attention deficits, finding target letters, and potential high workload. Enablers: Paradigm adjustments (cardboard cover, increased display time), experimenter support, eventual independent use. | Further investigation with a larger sample, paradigm adjustments, a control group, attention monitoring, increased training sessions, and encouraging pronunciation. | Contributes to research on BCI for neurorehabilitation, highlighting user-centred design and potential for individuals with communication and cognitive challenges. |
| Barath & Ross (2024b) [18] | South Africa | Descriptive qualitative (semi-structured online interviews) | 11 audiologists in the private sector | Private sector audiology practices | Continuing Professional Development (CPD) | Personal barriers (lack of motivation, relevant topics), financial barriers (cost, location, fees, connectivity), structural barriers (lack of information, timing). | Barriers: Personal (lack of motivation, relevance), financial (cost, location, fees, connectivity), Structural (lack of info, timing). | Undertake needs analysis, provide relevant and affordable CPD, improve monitoring and accessibility, ensure balance of clinical and ethical content, and improve information dissemination. | Provides insights into CPD challenges faced by audiologists in a developing country, likely resonating with other healthcare professionals in similar settings globally. Offers practical strategies for improvement. |
| Nickless et al. (2023) [19] | Australia | Qualitative (semi-structured interviews) | 20 independent speech-language pathologists with experience accessing public funding | Australian independent (private) speech-language pathology practices | Public funding models for children and young persons with communication and swallowing needs | Accessibility of funding, time burden, incongruence with evidence-based practice, trust between stakeholders, and consequences of funding models (inconsistencies, workforce impacts). | Barriers: Model complexity, socioeconomic factors, gatekeeper inconsistencies, bureaucratic delays, funding limitations, and a lack of trust. Enablers: Knowledgeable gatekeepers, NDIS potential, multidisciplinary models. | Future research on equitable access, consumer experiences, alignment with evidence, and performance measures. Advocacy for vulnerable populations and improved gatekeeper education. | Challenges regarding equitable access, alignment of funding with evidence, and system complexity are likely relevant to other countries with mixed healthcare systems. |
| Goulios & Patuzzi (2008) [24] | 62 countries (global survey) | Survey | Major audiology organisations | Various audiology practice settings globally | Audiology education and practice, scope of practice, and education levels | A wide range of professionals in hearing healthcare, the need for more audiologists, variation in scope of practice and education levels, and categorisation of countries based on resources. | Challenges in educating audiologists and providing hearing healthcare services globally. | Propose cost-effective and sustainable education models. | Provides a global perspective on audiology education and practice, highlighting disparities and common needs across different regions. |
| Foxcroft (2001) [5] | South Africa | Quantitative survey (cross-sectional) | 199 speech-language therapists and audiologists in private practice | Private clinical settings | Business management practices | Lack of business management knowledge; awareness not translating into practice | Limited expertise in business management; absence of formal training | Implement targeted training and education in business management for private practitioners | Highlights the universal need for business management skills among private practitioners |
| Breytenbach et al. (2015) [25] | South Africa | Descriptive survey | 147 audiologists | Public and private sectors | Practice management tasks, including legal, ethical, marketing, and accounting | Significant gaps between existing and required knowledge in practice management | Insufficient training in key management areas | Enhance practice management training to bridge knowledge gaps | Emphasises the critical need for comprehensive management training in audiology |
| Traynor & Taylor (2025) [1] | United States (applicable globally) | Professional textbook | Audiologists and healthcare professionals | Various healthcare settings | Strategic practice management, business operations | Integration of business strategies into healthcare practice | Lack of business acumen among healthcare professionals | Incorporate business training into healthcare education | Provides a comprehensive framework for integrating business practices in healthcare |
| Traynor (2006) [27] | United States | Professional article | Audiologists | Audiology clinics | Business fundamentals in audiology | Importance of business knowledge for audiologists | Traditional focus on clinical skills over business skills | Emphasise business education in audiology training programmes | Highlights the necessity of business skills in audiology practice |
| Alanazi (2017) [26] | Saudi Arabia | Cross-sectional mixed methods study | 23 audiologists and 37 speech-language pathologists | Hospitals | Professional practice, education, and policy | Need for development in education and practice standards | Limited educational programmes; lack of national guidelines | Develop national databases, clinical guidelines, and policies | Underlines the importance of standardised education and practice guidelines |
| Sebothoma et al. (2025) [2] | South Africa | Perspective article | South African audiologists | Various | Curriculum development, business skills in audiology | The necessity of business skills for audiologists' survival | Current curricula lacking in business training | Revise curricula to include business and entrepreneurial skills | Stresses the global need for business competencies in audiology education |
Key: BCI – Brain Computer Interface; CPD - Continuing Professional Development; ENT – Ear, Nose and Throat; GP - General Practitioner; ICF – International Classification of Functioning, Disability and Health; NDIS - National Disability Insurance Scheme.
Data synthesis and analysis involved two primary approaches. First, the extracted data were organised and presented in a comprehensive evidence table (Table 1) to provide an overview of the characteristics of the included studies. Second, a thematic analysis was conducted inductively to synthesise qualitative data on practitioners' perspectives, experiences, and issues. Guided by Braun and Clarke’s [12] six-step framework, this involved familiarisation with the data, generation of initial codes, searching for themes, reviewing themes, defining and naming themes, and producing a clear, organised report of the findings. Coding was conducted manually and verified independently by a second coder. Thematic saturation was operationally defined as the point at which no new codes or themes emerged from successive analysis of included studies. Saturation was determined iteratively during coding, with both coders confirming that additional articles did not yield novel conceptual insights, consistent with established qualitative synthesis approaches [13].
Given the narrative review design and the heterogeneity of included sources (including surveys, conceptual papers, and textbook contributions), direct participant quotations were not captured, if and where available, and were not included; instead, findings were synthesised at the level of reported themes and author-interpreted practitioner perspectives to maintain analytical consistency.
To ensure methodological rigor, this narrative review employed several quality assurance strategies, including systematic documentation of the search and selection process, critical appraisal of included studies for relevance and credibility, and reflexive consideration of potential researcher biases [14, 15]. A formal quality appraisal was conducted using an adapted Critical Appraisal Skills Programme (CASP) approach for qualitative and mixed-method studies, focusing on clarity of aims, methodological appropriateness, data collection, analysis rigor, and relevance to the review objectives. These steps enhanced the transparency, validity, and reproducibility of the findings. As the study is based on publicly available literature, formal ethical approval was not required. Nonetheless, ethical integrity was upheld through comprehensive citation, objective data handling, and efforts to incorporate diverse perspectives while acknowledging limitations in the existing evidence base [16].
3. RESULTS AND DISCUSSION
The results of this narrative review are structured to provide a comprehensive overview of the included studies and the key themes that emerged from the analysis of practitioner perspectives on practice management in audiology and speech-language therapy globally.
3.1. Description of Included Studies
A total of 16 peer-reviewed publications met the inclusion criteria for this narrative review. These studies exhibited a variety of methodological approaches, geographic contexts, and foci within practice management. These included empirical studies, academic dissertations, professional perspectives, and textbook contributions reflecting a broad understanding of management in audiology and speech-language pathology. A detailed evidence table (Table 1) is presented to ensure transparency and allow readers to interrogate individual study characteristics; however, key patterns in study design, geography, and focus are summarised in the text to support narrative synthesis and readability.
3.2. Study Design Profile
As shown in Table 1, the included studies spanned a range of designs. Overall, the dataset included approximately five qualitative studies, four survey-based studies, two mixed-methods studies, and a combination of feasibility, cohort, concept-mapping, and perspective-based contributions, reflecting a diverse methodological landscape. Three studies employed descriptive qualitative research designs using semi-structured interviews [17-19]. One study utilised a prospective cohort inter-rater agreement design [20], while another was a feasibility study employing a post-only design [21]. Concept mapping techniques were used in one study [6]. One article presented a perspective on the role of audiologists in hearing loss prevention [22], with Hlayisi et al. [7] presenting perspectives from South Africa, India, Nigeria, Brazil, Tunisia, Bhutan, Thailand, Malaysia, Sri Lanka, and Nepal, while Sebothoma et al. [2] provided perspectives from South Africa on curriculum development and business skills in audiology. A pilot feasibility study was conducted in one instance, and a global survey was used in two others [23, 24]. Additionally, two studies used survey designs to evaluate knowledge gaps and business practices in South Africa [5, 25]. One study used a cross-sectional, mixed-methods approach to map professional needs in Saudi Arabia [26]. One textbook provided a comprehensive overview of strategic practice management [1], while another article presented a synthesis of business fundamentals in audiology [27]. This diversity in study design suggests a multifaceted approach to investigating practice management within these professions.
3.3. Geographic Focus Profile
The geographic focus of the included studies varied, providing insights from different regions around the world. Collectively, the studies represented high-, middle-, and low-income country contexts, with notable contributions from South Africa (n=5) and Australia (n=3), and spanning Europe, the Middle East, Asia, and multi-country LMIC contexts. Some of the studies originated in Australia [6, 19, 20], with studies on diagnostic agreement, age-related hearing loss management, and public funding models. Sweden contributed a study on person-centred audiological rehabilitation [21]. South Africa was represented by five studies, including research on continuing professional development among audiologists in private practice, business skill gaps, curriculum responsiveness, and business practices in private settings [2, 5, 17, 18, 25]. A study involving multiple countries within Africa, Asia, and South America provided a broader perspective on audiology practice [7]. Germany was the location for a pilot study on aphasia rehabilitation [23]. The United States served as the implicit context for a perspective piece on hearing loss prevention [22]. Two United States-based publications offered comprehensive insights into strategic practice management and the basics of audiology business [1, 27]. A global survey offered an international overview of audiology education and practice. Saudi Arabia was included through a study examining practice infrastructure and education [26]. The variation in geographic focus highlights the potential influence of different healthcare systems, regulatory frameworks, and cultural contexts on practice management in audiology and speech-language therapy.
3.4. Practice Analysis Focus Profile
An examination of the primary practice management areas investigated across the included studies revealed several key areas of focus. One study examined agreement in diagnosis and management between audiologists and Ear, Nose, and Throat (ENT) specialists [20]. Person-centred audiological rehabilitation was the focus of another [21]. Hearing loss prevention was examined from an audiological practice perspective. The role of general practitioners in managing age-related hearing loss was investigated in one study. Continued Professional Development (CPD) for audiologists in private practice was a central theme in two studies. Best practices in audiology from an international standpoint were discussed. Aphasia rehabilitation using brain-computer interface technology was explored. Public funding models for speech-language pathology services were examined. A global survey provided an international perspective on audiology education and practice. Additional practice areas included strategic business planning, financial management, reimbursement complexities, human resource management, marketing, ethical dilemmas, and curriculum responsiveness. These were discussed in studies from South Africa, Germany, Saudi Arabia, and the United States, highlighting gaps in training, support, and policy. The distribution of research across these various practice analysis foci highlights the diverse range of considerations relevant to the effective management of audiology and speech-language therapy services.
3.5. Thematic Analysis Findings
The thematic analysis of the 16 included studies revealed nine key themes reflecting the experiences, challenges, and recommendations of audiologists and speech-language pathologists worldwide regarding practice management. These themes offer nuanced insights into the strategic, financial, and operational aspects of clinical management, with contextual variation across practice settings and countries.
3.5.1. Theme 1: Financial Management and Reimbursement Complexities
Financial management and reimbursement complexities emerged as the most consistently reported challenge across studies. Practitioners identified difficulty navigating funding models, limited financial literacy, and the lack of structured training in financial planning and sustainability [2, 5, 25]. These concerns extended beyond billing to broader issues like budgeting, managing overheads, and ensuring long-term viability. Practitioners' perspectives suggest that navigating these systems can be time-consuming and frustrating, potentially diverting resources from direct client care. Foxcroft [5] found that while many South African practitioners were aware of the importance of business management, few applied this knowledge in practice, largely due to a lack of formal training and support. Breytenbach et al. [25] similarly reported significant gaps in financial knowledge and business administration skills among South African audiologists, highlighting a mismatch between academic preparation and professional demands.
Reimbursement complexities were especially prevalent, with practitioners citing burdensome and inconsistent public funding systems. For example, independent practitioners in Australia described administrative inefficiencies that impeded service delivery [19]. Similarly, South African audiologists reported being underprepared to handle the business aspects of private practice due to inadequate undergraduate preparation [2]. In Saudi Arabia, Alanazi [26] identified similar challenges in reimbursement and funding models, particularly in public-sector service delivery, highlighting the global nature of these issues. These experiences echo findings from the U.S. context, where business training is still peripheral despite its importance [1, 27]. Traynor and Taylor [1] further argue that strategic financial planning and operational literacy are no longer optional competencies in audiology and speech-language therapy, but central to service sustainability, particularly in a market-driven or hybrid public-private funding environment. This theme strongly suggests the need for formal integration of financial management modules into audiology and speech-language therapy curricula and for professional associations to provide ongoing business support tools. The systemic nature of reimbursement and financial management challenges, spanning high-, middle-, and low-income countries, demonstrates that these are not isolated practice issues, but rather health systems concerns that impact service equity, professional viability, and healthcare access. Failure to address this gap may impact practitioner viability and service accessibility, particularly in LMICs.
3.5.2. Theme 2: Ethical Dilemmas in Practice
Ethical dilemmas were highlighted across both the private and public sectors. Issues included managing conflicts of interest, especially in settings where practitioner income is tied to service volume; supervision of less qualified support personnel; and maintaining confidentiality in digital environments [2, 18, 25]. These challenges highlight the need for continuous professional ethics training. Breytenbach et al. [25] identified critical knowledge gaps among South African audiologists in managing the ethical and legal aspects of practice, particularly in supervision, documentation, and professional boundaries, indicating that these concerns are not isolated incidents but recurring systemic issues.
Importantly, the growing use of technology has introduced new ethical considerations, particularly regarding data privacy and informed consent in telepractice [3, 26]. Alanazi [26] found that audiologists and speech-language pathologists in Saudi Arabia expressed concern about a lack of clear ethical guidelines governing digital interactions, a concern further complicated by inconsistent national regulations, an issue echoed in other LMICs. This highlights the growing need for practitioners to be trained in technology-mediated ethical reasoning.
The discussion underscores the need for robust ethical guidelines and real-time decision-making frameworks, particularly in under-regulated or evolving policy environments. Such frameworks are crucial in contexts where practitioners must independently interpret ethical grey areas, especially in rural, private, or digital-first practices. Embedding case-based ethical decision-making into training may enhance practitioners' readiness to address these complexities. Developing context-sensitive ethics modules, co-informed by clinical experience and emerging practice scenarios (e.g., tele-audiology, hybrid supervision models), could prepare practitioners to navigate evolving professional environments more effectively.
3.5.3. Theme 3: Workload and Burnout
Substantial caseloads, escalating administrative burdens, and unrealistic expectations are frequently linked to high workloads and systemic burnout [2, 23], creating a cascading effect that severely reduces job satisfaction and drives workforce attrition. The impact of burnout is not limited to individual health but extends to compromised care quality and organisational efficiency [28]. These observations echo wider concerns in global health systems about clinician sustainability and highlight the need for policy-level responses, including more realistic caseload expectations and structured mental health support for practitioners [3, 29]. Sebothoma et al. [2] also noted that early-career audiologists in South Africa face compounded burnout risks, not only due to high patient loads but also limited administrative infrastructure, a lack of mentorship, and inadequate preparation in workflow and systems management. The pressure of balancing clinical and managerial duties without adequate training further exacerbates stress levels.
Although caseload pressures are common in both public and private settings, the burden may be more pronounced in under-resourced environments where clinicians take on multiple roles, clinical, administrative, and operational, simultaneously [5, 25]. This multitasking without support can lead to rapid professional fatigue and workforce attrition. Additionally, integrating time and workload management skills into undergraduate training and CPD can serve as protective measures against burnout. Proactively embedding stress management, administrative efficiency training, and work-life balance strategies into early-career development pathways may strengthen practitioners' resilience. These competencies are especially critical in LMICs, where professional support systems are limited, and clinician burnout threatens the continuity of care and system stability.
3.5.4. Theme 4: Adoption and Implementation of Technology
Technology adoption surfaced as a double-edged theme. Innovations such as Brain-Computer Interfaces (BCIs), electronic health records, and telepractice platforms offer viable pathways to optimize clinical access and therapeutic efficacy; however, widespread adoption remains constrained by steep operational learning curves, financial limitations, and inadequate institutional training in core digital competencies [1, 23]. Crucially, this technological transition directly intersects with broader fiscal and bioethical frameworks. In South Africa, for instance, technology adoption is hindered by infrastructure constraints and costs [30]. Globally, as Traynor and Taylor [1] suggest, digital literacy must be seen as a core competency. They emphasise that the rapid digitalisation of healthcare requires not just technical knowledge but a strategic understanding of how to use technology to improve workflows, data management, and client engagement. Alanazi [26] reported similar implementation challenges in Saudi Arabia, where clinicians acknowledged the potential of telepractice but cited poor institutional support, limited policy clarity, and inadequate training as key barriers to effective use. These barriers led to inconsistent uptake of technology-enhanced care despite growing clinician interest. Additionally, ethical and data security concerns, particularly regarding client confidentiality on virtual platforms, continue to affect practitioner confidence and technology adoption. These intersecting challenges underline the need for integrated, context-responsive frameworks that combine infrastructure support, professional training, and clear ethical guidelines. Notably, none of the included studies provided robust cost-effectiveness data or economic evaluations of technology implementation, particularly in LMIC settings. This represents a critical evidence gap, as decisions regarding digital adoption are often constrained by resource limitations. Future research should prioritise cost-benefit and implementation analyses to guide contextually appropriate technology integration.
Addressing these gaps requires curriculum updates, institutional investment in infrastructure, and policy support to ensure equitable technology integration. Digital skills must be taught not in isolation but alongside administrative and clinical training to ensure practitioners are fully prepared to function in hybrid, tech-enhanced healthcare environments. Without these structural supports, technology risks becoming an added burden rather than a lever for service innovation.
3.5.5. Theme 5: Interprofessional Collaboration and Communication
Effective interprofessional collaboration was described as essential to improving client outcomes [2, 6, 17, 19, 20]. High diagnostic agreement between audiologists and ENT specialists (e.g., in Australian paediatric care) illustrates how collaborative pathways can streamline service delivery and reduce unnecessary referrals [20]. The emphasis on interprofessional collaboration highlights the growing recognition of the importance of a team-based approach to healthcare [31]. Practitioners in audiology and speech-language therapy recognise that working effectively with other professionals can lead to better client outcomes.
Beyond clinical benefits, interprofessional collaboration is associated with enhanced service efficiency, minimized delays within care pathways, and elevated professional satisfaction [1]. Consequently, evidence suggests that the long-term sustainability of modern healthcare systems increasingly depends on developing these collaborative competencies, bridging clinical teams with administrative and fiscal domains. This reflects a broader movement toward integrated models of care, particularly in health systems that are attempting to use limited resources more efficiently while improving patient outcomes. However, barriers such as professional silos, unclear role boundaries, and time constraints persist. In some contexts, as noted by Sebothoma et al. [2], hierarchical healthcare structures and unclear referral protocols limit audiologists' and speech-language therapists' ability to function as equal partners in multidisciplinary teams. The findings emphasise that interprofessional education during pre-service training, along with workplace models that facilitate shared care planning, are essential strategies for enhancing collaboration and ultimately, quality of care [17].
To promote sustainable interdisciplinary engagement, collaboration should be embedded not just in clinical instruction but also in management training, enabling practitioners to navigate team dynamics, advocate for their roles, and contribute meaningfully to shared service goals. Institutional policies must also support collaborative practice through joint CPD programmes and structures that reward cooperative care models.
3.5.6. Theme 6: Private Practice Management
Private practice management emerged as a theme encompassing both opportunities and vulnerabilities [2, 7]. Practitioners described difficulties in marketing services, hiring staff, navigating billing systems, and securing ongoing professional development. In South Africa, the compounded impact of language-based exclusion in hiring, lack of CPD access, and high startup costs made private practice largely inaccessible to new graduates [2]. Foxcroft [5] found that although many South African clinicians recognized the value of management skills, few applied them in practice, largely due to insufficient training. In both LMICs and high-income countries (HICs), findings indicate that managing a private practice requires a hybrid skill set that blends clinical excellence with entrepreneurial competence. Curricular responsiveness and mentorship programmes are needed to close this readiness gap. Alanazi [26] similarly reported that in Saudi Arabia, clinicians working outside major hospitals faced challenges accessing professional development, navigating bureaucratic systems, and managing independently, challenges that mirror those found in other middle-income countries. Taken together, these studies suggest that the challenges of private practice are not limited to a single country or region, but are linked to broader gaps in professional training, support structures, and regulatory guidance.
The findings further highlight a systemic neglect of practice management training in curricula, particularly acute in LMICs [2, 3, 5, 21, 25, 26]. This aligns directly with the curriculum responsiveness concerns raised by Sebothoma et al. [2], reinforcing the disconnect between academic preparation and the real-world demands of private practice. The South African study by Sebothoma et al. [2] reinforces this gap, emphasising how early-career professionals are often unprepared to navigate private practice, despite high demand for audiological services. Traynor and Taylor [1] argue that private practice readiness should be viewed as a strategic outcome of allied health training rather than an optional career pathway. Their work highlights the need for structured mentorship, administrative toolkits, and simulation-based financial planning modules to support emerging professionals in transitioning from clinical learners to practice owners.
Addressing this mismatch requires a curriculum that integrates essential business skills, a need echoed across multiple countries in this review. Without intentional capacity-building for private practitioners, many systems risk losing skilled clinicians who are otherwise willing to serve but lack the operational support to sustain independent practice.
3.5.7. Theme 7: Human Resource Management
Human Resource (HR) management, particularly as it relates to CPD, supervision, and team leadership, was a recurring theme [2, 17, 18, 25]. Retaining skilled staff and providing appropriate mentorship to early-career professionals were flagged as ongoing challenges. Breytenbach et al. [25] noted specific deficits in audiologists’ management knowledge in South Africa, including HR practices. These findings indicate the need for intervention at two levels: integrating leadership and supervision frameworks into training programmes and providing targeted CPD opportunities in HR management for practice owners and senior clinicians.
Foxcroft [5] earlier identified that private practitioners often lacked the confidence and knowledge to manage human resources effectively, particularly in areas such as recruitment, performance evaluation, and conflict management in small-team environments. Despite some awareness of these responsibilities, the application of HR management principles remained inconsistent, largely due to the absence of formal training or mentorship.
Alanazi [26] added to this by highlighting that in Saudi Arabia, speech-language pathologists and audiologists working in hospital systems often lacked autonomy in HR-related decisions, while those in peripheral or private settings were expected to manage staff without adequate leadership preparation. These findings point to a global mismatch between expectations and preparation in HR competencies. Traynor and Taylor [1] argue that HR management is a cornerstone of effective practice leadership and should be introduced as a core theme in both undergraduate training and early-career mentorship programmes. Their framework emphasises succession planning, retention strategies, team communication, and the ability to manage support staff and students, skills that are transferable across public and private sectors.
These findings suggest that HR training must go beyond basic supervisory duties. Developing broader HR competencies among practitioners, such as workload delegation, conflict resolution, and team motivation, may strengthen the sustainability of practices and contribute to healthier workplace environments. This is particularly important in LMIC contexts where professional isolation and burnout are compounded by staffing instability and high turnover.
3.5.8. Theme 8: Policy and Advocacy
Several studies called for stronger professional engagement with policy development and advocacy [1, 2, 26]. Practitioners highlighted how healthcare regulations, scope-of-practice restrictions, and inconsistent government support shaped their capacity to manage practices effectively. Alanazi [26] reported gaps in Saudi Arabia's national infrastructure and policy, echoing calls for context-relevant guidelines and professional regulation. Globally, there’s a need to empower practitioners not only as service providers but as policy influencers. Associations should support advocacy training and involve clinicians in policy consultations to bridge this gap.
Foxcroft [5] and Breytenbach et al. [25] both emphasised that in South Africa, policy constraints, particularly those affecting private practice regulation, reimbursement protocols, and recognition of services, pose real limitations on entrepreneurial development and professional autonomy. These constraints are rarely addressed in formal training, leaving clinicians ill-equipped to navigate or challenge policy systems that affect their daily operations. Sebothoma et al. [2] further highlighted how newly qualified audiologists in LMICs often struggle to find their place in broader health policy conversations, due to limited exposure to health systems governance, advocacy tools, or stakeholder negotiation skills during training. As a result, their voices are frequently absent in decisions that directly affect service access and professional scope. Traynor and Taylor [1] argue that policy literacy should be an essential component of health professional education, framing it as both a leadership and sustainability skill. They recommend integrating advocacy modules into professional curricula and fostering partnerships among clinical, academic, and regulatory bodies to enable clinicians to shape the systems in which they operate.
To enable meaningful change, professional associations must play a more proactive role in mobilising practitioners, facilitating policy dialogues, and building collective capacity for regulatory engagement, particularly in settings where practitioner advocacy is underdeveloped or structurally marginalised. Lessons can be drawn from other allied health fields, such as nursing and public health, where structured advocacy training programmes and professional lobbying mechanisms have successfully influenced workforce policy and service delivery reforms. Without deliberate attention to advocacy and policy engagement, practice management improvements risk being undermined by stagnant, outdated, or misaligned regulatory frameworks.
3.5.9. Theme 9: Client Management and Engagement
Client management emerged as a critical domain intersecting with all other themes. Strategies to build trust, ensure informed consent, and enhance adherence to treatment plans were central concerns. The reviewed literature emphasised the shift towards person-centred care as both a philosophical and strategic imperative in modern practice [2, 21, 23]. This approach demands communication competence, cultural responsiveness, and participatory goal-setting, of which should be embedded in both training and clinical protocols. Person-centredness is not simply an ideal; it is a measurable determinant of rehabilitation success [32, 33]. The focus on person-centred care reflects a shift towards a more holistic understanding of patient needs and the importance of involving patients in their rehabilitation journey.
Granberg and Skagerstrand [21] emphasised the value of using structured communication tools such as the International Classification of Functioning (ICF)-based interview guide to strengthen client-practitioner dialogue. Their findings suggest that structured, yet flexible communication frameworks can help uncover environmental and psychosocial barriers to rehabilitation, making intervention more relevant and personalised. Hlayisi et al. [7] also noted that in multilingual and multicultural contexts such as South Africa, effective client management requires linguistic responsiveness and cultural humility. Without these, misunderstandings may compromise trust and adherence. These insights underline the need for training programmes to include both language-access strategies and cultural competence training, not just as add-ons but as central components of client care. Alanazi [26] reported similar concerns in Saudi Arabia, where patients often come from diverse cultural backgrounds and healthcare systems lack standardised protocols for patient engagement. In such settings, clinicians reported the need for tools to facilitate collaborative goal setting and shared decision-making, especially in audiology, where treatment often requires long-term behavioural and lifestyle adjustments. In addition to improving clinical outcomes, person-centred approaches also have implications for service efficiency and resource optimisation, as aligned goals often lead to better adherence and reduced attrition from care pathways. Embedding these approaches into practice management protocols can thus support both ethical care and operational success.
3.6. Regional Contextualisation of Findings
While this review adopts a global lens, a relatively strong representation of South African studies was noted across several themes. This reflects both the availability of contextually relevant research and the pronounced practice management challenges documented within LMIC settings. Importantly, these studies were not intended to disproportionately weight findings, but rather to illustrate how systemic constraints, such as limited infrastructure, regulatory complexity, and workforce shortages, manifest in specific contexts. Similar patterns, however, were observed across other LMIC and even high-income settings, suggesting that while the intensity of challenges may vary, their underlying nature is globally shared. This reinforces the importance of interpreting findings through both global and context-specific lenses, rather than attributing them to any single regional experience.
Overall, the findings of this narrative review highlight several interrelated dimensions of practice management as experienced by audiologists and speech-language pathologists globally. The prominence of themes such as financial and reimbursement complexities, gaps in business and administrative training, barriers to continuing professional development, the critical importance of interprofessional collaboration, and the increasing emphasis on person-centred client engagement reflects the evolving demands placed on professionals operating at the intersection of clinical care and health system administration. Emerging developments such as artificial intelligence-assisted diagnostics and evolving telehealth reimbursement policies are likely to further reshape practice management demands, requiring practitioners to develop adaptive competencies in digital governance, data interpretation, and technology-enabled service delivery.
These themes resonate with broader challenges in healthcare management and workforce development [34], but they also surface profession-specific issues that uniquely impact audiology and speech-language therapy. These include the underrepresentation of practice management in pre-service curricula, limited infrastructure to support private practice sustainability, ethical tensions in digitally mediated service delivery, and misalignment between service demand and training outputs. Importantly, many of these challenges map directly onto health system building blocks, particularly ‘health workforce,’ ‘service delivery,’ and ‘leadership and governance,’ as defined by the World Health Organisation’s Health Systems Framework. This reinforces the relevance of these findings beyond professional silos, pointing to their systemic significance. Professional bodies such as the South African Speech Language and Hearing Association (SASLHA), the South African Association of Audiologists (SAAA), and the American Speech-Language-Hearing Association (ASHA) have recognised the gravity of these challenges and continue to invest in guidance and CPD on practice management. However, the persistence of gaps in practitioner preparedness suggests that such initiatives must be more widely integrated into formal training and policy frameworks.
Despite regional differences, the findings suggest a set of globally shared concerns. From Australia to Germany, South Africa to Saudi Arabia, and the United States, practitioners consistently face similar pressures, underdeveloped business and leadership competencies, uncoordinated policy environments, and inadequate support for practice sustainability. The recurrence of these themes across diverse geopolitical and economic contexts confirms that practice management challenges are not isolated to individual practitioners or countries, but instead reflect structural weaknesses in how health systems train, regulate, and support allied health professionals. Addressing these systemic gaps requires coordinated, multisectoral responses. Partnerships between health faculties, business schools, and professional associations may provide scalable opportunities to embed operational, leadership, and policy advocacy skills into the training pipeline without compromising core clinical content. Tailored CPD modules, simulation-based business planning, and structured mentorship programmes could bridge the gap between classroom and clinic. Professional associations must also play a proactive role in regulatory advocacy, ensuring that practitioners are equipped not only to function within existing systems but to reform them where necessary.
While commonalities exist, the intensity and nature of challenges vary by context. For example, reimbursement hurdles may be more pronounced in countries with fragmented insurance systems, while private practice barriers may be more acute in LMICs due to limited capital access and regulatory complexity. Similarly, CPD constraints differ across settings depending on digital infrastructure, workforce distribution, and institutional support. This highlights the need for comparative regional research that accounts for policy, economic, and training contexts in shaping practice management experiences. Such research can inform more context-sensitive reform initiatives that reflect both global principles and local realities.
This narrative review has several limitations. The selection of studies was based on peer-reviewed, English-language literature available at the time of the review, potentially introducing selection and language bias. The restriction to English-language publications and the 2000–2025 publication window may have led to the underrepresentation of relevant studies from non-Anglophone regions and of earlier foundational work, particularly in LMIC contexts where local dissemination channels differ. The narrative synthesis methodology does not involve statistical aggregation, which may limit the generalisability of findings. The diversity in study designs, focus areas, and geographic coverage also limits comparability. Furthermore, while practitioner perspectives offer invaluable insights, they may be shaped by context-specific challenges or disciplinary lenses, and the absence of client or policymaker viewpoints is acknowledged. Nonetheless, the review offers a critical synthesis of global practitioner perspectives on practice management and contributes a timely evidence base for health system leaders, educators, and professional bodies seeking to reform how allied health services are organised, managed, and sustained. The insights presented here may inform future research and practical initiatives aimed at strengthening the preparedness and sustainability of the audiology and speech-language therapy workforce.
CONCLUSION
This narrative review synthesised the global peer-reviewed literature on practitioners' perspectives on strategic practice management in audiology and speech-language therapy. Following a structured, PRISMA-informed selection process (n = 192 identified; n = 182 screened; n = 37 full-text assessed; n = 16 included), the analysis uncovered nine interrelated themes reflecting core challenges and emerging opportunities in managing clinical practices. These included persistent difficulties with financial management and reimbursement processes, ethical complexities, workload-related burnout, uneven technology adoption, human resource limitations, barriers to continuing professional development, and underdeveloped policies. Additionally, themes of interprofessional collaboration and person-centred client engagement highlight the evolving scope of practice in these professions.
What emerges is a shared global concern: audiologists and speech-language pathologists are increasingly expected to demonstrate not only clinical proficiency but also business acumen, leadership, and policy literacy, yet current training and support structures often leave them underprepared for these responsibilities. This is particularly evident in LMICs, where structural inequities, resource constraints, and limited access to CPD exacerbate these challenges. Future research should prioritise a mixed-methods, multi-stakeholder design incorporating practitioner, client, and policymaker perspectives to develop a more comprehensive and system-responsive understanding of practice management across contexts. At the same time, the literature highlights practitioner resilience, a willingness to adapt, and the growing recognition of the value of multidisciplinary approaches. In health systems terms, these gaps reflect a misalignment between professional education, service delivery demands, and the health workforce’s role in achieving equitable access and quality of care. As emphasised in the WHO’s Health Systems Framework, strengthening the 'health workforce' and 'service delivery' building blocks requires investment in the managerial capacity of allied health professionals.
Based on these findings, several actionable recommendations are proposed. First, for practitioners, the development of robust business, administrative, and leadership skills must be prioritised. This includes financial literacy, ethical decision-making in complex settings, and strategies for managing workload and burnout. Practitioners should also proactively seek out CPD opportunities, mentorship networks, and interprofessional collaboration platforms to strengthen both practice and advocacy capabilities. Second, for professional organisations (e.g., SASLHA, SAAA, ASHA, AAA), the role of providing accessible, contextually relevant resources remains vital. These bodies should champion best practices in areas such as financial sustainability, technology integration, and ethical care. Moreover, they must intensify advocacy efforts to address systemic barriers, such as opaque reimbursement frameworks and uneven access to CPD, while facilitating global knowledge exchange and peer learning. Third, for educational institutions, curricula must be redesigned to embed comprehensive training in practice management. This includes not only foundational business and HR skills but also applied knowledge in billing systems, marketing, digital practice platforms, and interprofessional teamwork. Innovative models, such as partnerships between health sciences faculties and business schools, can offer scalable solutions to bridge this curricular gap. Fourth, for policymakers and healthcare administrators, a more responsive regulatory and funding environment is essential. Simplifying funding pathways, enabling interdisciplinary care models, ensuring equitable access to CPD, and recognising the specific needs of private and community-based practices will help align health systems with the real-world demands professionals face. Policy efforts to build and retain a resilient allied health workforce must also incorporate practice management competencies as a core element of professional development and service sustainability strategies.
In conclusion, this review highlights not only a professional training concern, but a broader health systems issue: the absence of integrated, strategic practice management competencies compromises service quality, equity, and workforce retention. Importantly, the consistency of findings across the 16 included studies suggests that these challenges are systemic rather than contextually isolated, reinforcing the need for coordinated global and context-specific responses. Embedding these competencies at all levels, education, regulation, and policy, is essential to bridge the gap between clinical excellence and operational sustainability. Future work should also focus on translating the identified themes and recommendations into practical outputs, such as competency-based curricula, simulation-based training modules, and adaptable practice management toolkits for use in allied-health education and CPD programmes. The themes and recommendations outlined in this paper provide a strong foundation for transformative policy and curricular reform, ensuring that practitioners are not only clinically capable but also strategically equipped to lead, innovate, and thrive within evolving healthcare systems. Lastly, further research is needed to generate context-specific evidence on cost-effectiveness, technology integration, and policy implementation, particularly within LMICs where data remain limited. Comparative and longitudinal designs may also help to evaluate the impact of practice management training interventions on workforce retention and service outcomes.
DECLARATIONS
Contribution to the field: This study contributes to the global discourse on health workforce development by illuminating persistent gaps in practice management training for audiologists and speech-language therapists. Through a thematic synthesis of practitioner perspectives across diverse geographic and health system contexts, the review presents compelling evidence for the integration of business, leadership, and policy engagement skills into pre-service curricula and continuing professional development. These findings offer valuable guidance for educators, regulatory bodies, and policymakers seeking to strengthen professional preparedness, enhance service delivery sustainability, and align training with the operational realities of modern healthcare systems.
AUTHOR’S CONTRIBUTIONS
This is a sole-authored review in which the author conceptualised the study, conducted the research, analysed the data, and wrote the manuscript.
LIST OF ABBREVIATIONS
| ASHA | = American Speech-Language-Hearing Association |
| SAAA | = South African Association of Audiologists |
| BCIs | = Brain-Computer Interfaces |
| CPD | = Continuing Professional Development |
| ENT | = Ear, Nose, and Throat |
| HICs | = High-Income Countries |
| ICF | = International Classification of Functioning Disability and Health |
| LMICs | = Low-and Middle-Income Countries |
| SASLHA | = South African Speech Language and Hearing Association |
| WHO | = World Health Organisation |
ACKNOWLEDGEMENTS
Declared none.

