All published articles of this journal are available on ScienceDirect.

The Burden of Low Birth Weight among Children under Five in Indonesia: A Systematic Analysis of the Global Burden of Disease Study 2021
Authors Info & Affiliations
Abstract
Introduction
Low Birth Weight (LBW) is a global health issue, including in Indonesia. LBW contributes to the loss of healthy life opportunities among children under five. This study aims to assess the burden and potential loss of healthy life opportunities among children under five due to LBW in Indonesia.
Methods
The study used a systematic analysis of the Global Burden of Disease (GBD) 2021 to analyze the burden of disease due to LBW in Indonesia.
Results
The burden of disease among children under five in Indonesia has decreased compared to the previous year. However, it remains high and concentrated in eastern Indonesia. The burden of LBW is attributed to Years of Life Lost (YLLs) rather than Years Lived with Disability (YLDs), accounting for 99.11%. Infants under 28 days have higher Disability-Adjusted Life Years (DALYs) than other age groups, with 863,365 DALYs per 100,000 children under five (95% UI = 691,784.16–1,055,370.99), and boys have higher DALYs than girls. Most of the DALYs associated with LBW are caused by neonatal disorders, with a proportion of 94.27%. Nationally, LBW accounts for 69.68% of neonatal disorders. Nearly three million years of healthy life opportunities were lost due to LBW in 2021.
Discussion
Low Birth Weight (LBW) is the leading contributor to DALYs among Indonesian children under five, with the highest burden in central and eastern regions, where healthcare access and service quality remain uneven.
Conclusion
LBW remains a significant issue in Indonesia. Many programs have been established to address this problem; however, they have not been implemented optimally and have yet to effectively resolve the issue. Developing and perfecting health programs with multisector collaboration should be prioritized to reduce the burden of LBW in Indonesia.
1. INTRODUCTION
Low Birth Weight (LBW) is one of the most significant global health issues, particularly in low- and middle-income countries. According to UNICEF data, approximately 14.7% of babies are born with a birth weight of less than 2,500 grams each year [1]. Despite global efforts, progress in reducing LBW prevalence remains slow, especially in low-resource settings [1].
The causes of LBW are diverse, including preterm birth, maternal malnutrition during pregnancy, inadequate prenatal care, low maternal knowledge levels, and environmental factors [2-5]. The high prevalence of LBW is a significant concern due to its impact on infant health, both in the short and long term. LBW contributes to increased risks of neonatal complications, impaired growth and development, and a higher likelihood of chronic diseases later in life, placing a substantial burden on health systems [3, 6, 7].
In Indonesia, the prevalence of LBW reached 6.1% in 2023, showing minimal improvement from 6.2% in 2018 [8, 9]. LBW contributes to the loss of healthy life opportunities among children under five due to premature death and disability, amounting to 13,458.19 years per 100,000 children under five [6]. It reflects ongoing challenges in maternal and child health services, indicating that LBW prevention remains a significant public health priority.
The Global Burden of Disease (GBD) approach is used to provide an overview and compare health progress while finding the primary causes of health loss that could potentially be prevented, including those stemming from childhood malnutrition [6]. It utilizes Disability-Adjusted Life Years (DALYs), a metric that reflects both premature mortality and disability. Using this approach allows a deeper understanding of the magnitude and distribution of LBW-related health loss.
Given the persistent burden of LBW in Indonesia, this study aims to analyze GBD 2021 data to estimate the health loss attributable to LBW among children under five and to examine regional disparities. Findings from this analysis are expected to inform policies and interventions to strengthen maternal and child health programs in Indonesia.
2. METHODS
2.1. Data Sources
This study used estimates of Disability-Adjusted Life Years (DALYs), Years of Life Lost (YLLs), and Years Lived with Disability (YLDs) attributable to Low Birth Weight (LBW) from the Global Burden of Disease (GBD) 2021 study produced by the Institute for Health Metrics and Evaluation (IHME). The Indonesian estimates draw on multiple data sources incorporated within the GBD modeling framework, including the Indonesia Family Life Survey (IFLS), SUSENAS, RISKESDAS, and the National Household Health Survey (SKRT).
GBD provides nationally and provincially aggregated estimates and does not include individual-level data. GBD estimates disease burden using standardized modeling procedures, and reports point estimates along with 95% Uncertainty Intervals (UI).
Data were extracted directly from the IHME GBD Compare and GBD results tools, which provide downloadable estimates for DALYs, YLLs, and YLDs by age group, sex, location, and year. Inclusion criteria were all LBW-attributable DALYs, YLLs, and YLDs for children under five in Indonesia. Estimates unrelated to LBW, from populations aged >5 years, or outside Indonesia, were excluded.
2.2. Data Analysis
This study used the systematic review of the Global Burden of Disease (GBD) 2021 to analyze the burden of disease risked by LBW among children under five in Indonesia. Data were analyzed descriptively to assess temporal trends, age and sex patterns, and regional variations in LBW-related DALYs, YLLs, and YLDs. Results are presented as rates per 100,000 population with 95% Uncertainty Intervals (UI).
3. RESULTS
3.1. Trend of Burden of Disease Among Children Under Five
The ranking of DALYs risk factors for children under five in Indonesia in 1990 and 2021 (Fig. 1). All risk factors for children under five experienced a decline during the period 1990–2021. In 1990, the largest DALY risk factor was wasting, with a DALY rate of 36,906.92 per 100,000 children under five (95% UI = 10,984.5–50,732.41). However, by 2021, the leading DALY risk factor for children under five had shifted to LBW, despite a significant reduction of 57.03% with DALYs 13,458.19 per 100,000 children under five (95% UI = 11,653.16–17,685.86).
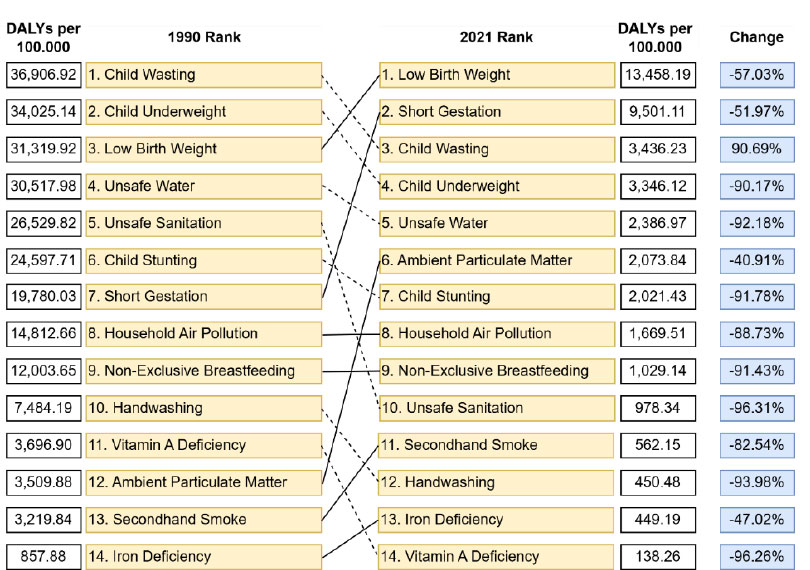
Ranking of DALYs risk factors for children under five in Indonesia in 1990 and 2021.
3.2. The Burden of LBW
While the burden of risk factors in Indonesian children under five has decreased compared to previous years, disparities persist. These disparities are clear in the higher concentration of regions with high DALYs due to LBW in central and eastern Indonesia (Fig. 2). Several provinces in the eastern regions, such as Maluku, Sulawesi, and Nusa Tenggara, face a significantly higher burden of LBW. In contrast, provinces in other regions, such as Java-Bali, experience relatively lower burdens of LBW.
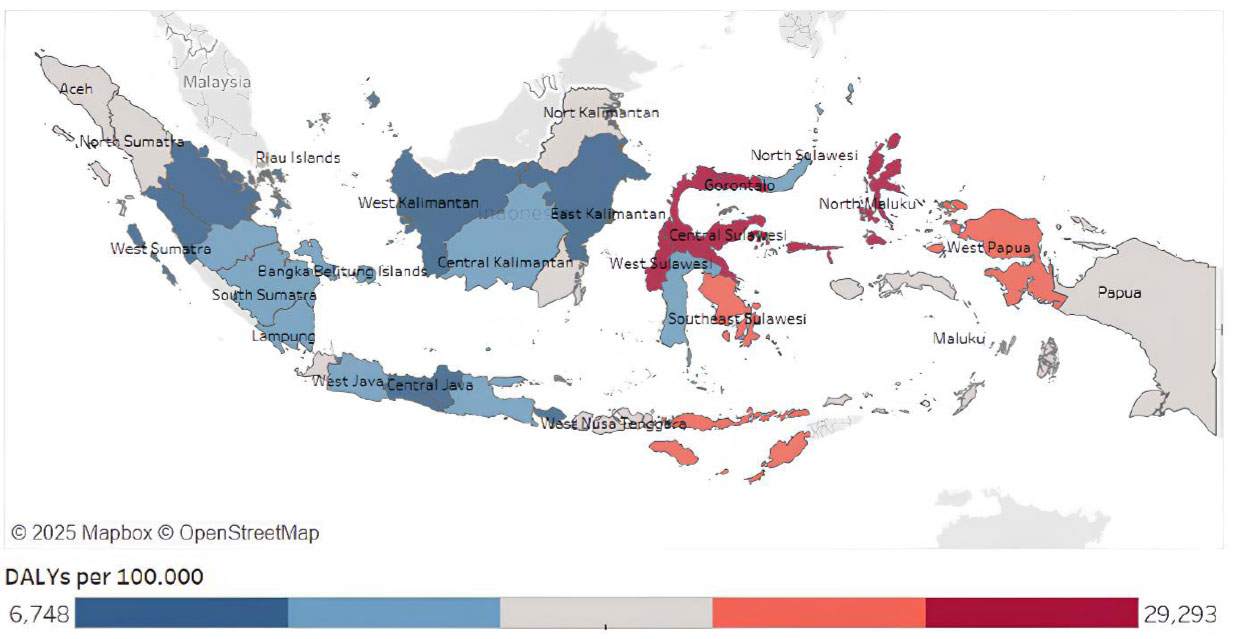
Distribution of burden of LBW among children under five in Indonesia in 2021.
Figure 3 illustrates the DALYs related to Low Birth Weight (LBW) by age group and sex among children under five in Indonesia in 2021. Infants under 28 days old have significantly higher DALYs compared to other age groups, with a DALY rate of 863,365 per 100,000 children under five (95% UI = 691,784.16–1,055,370.99) (Fig. 3). Among the age groups, boys have higher DALYs than girls, both in the under 28 days group, the under 1 year group, and the under 5 years group.
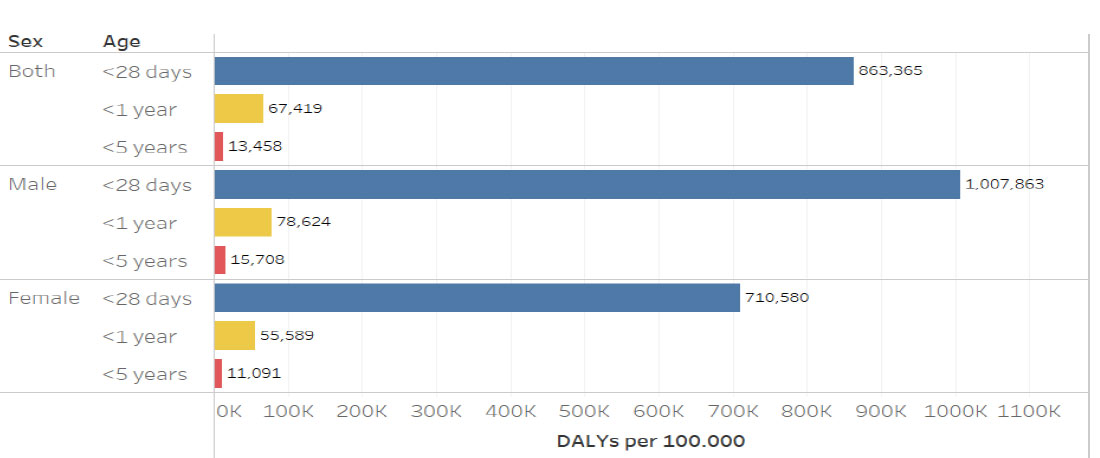
DALYs related to LBW by age and sex among children under five in Indonesia in 2021.
The burden related to LBW is viewed through the indicators of Years of Life Lost (YLLs) and Years Lived with Disability (YLDs). The burden due to LBW is more dominant in YLLs compared to. LBW accounts for 529,397 YLLs per 100,000 children under five, or 99.11% of the DALYs due to LBW, and accounts for 4,748 YLDs per 100,000 children under five, or 0.89% of the DALYs due to LBW (Fig. 4). It means that LBW conditions tend to cause premature death more often than long-term disability. Children with LBW are more vulnerable to fatal diseases and have a higher risk of death. Therefore, the loss of healthy life opportunities among children with a history of LBW is primarily due to the contribution of LBW to premature death, rather than long-term disability.

The proportion of YLLs and YLDs due to low birth weight (LBW) among children under five in Indonesia in 2021.
3.3. Specific Causes Related to LBW and Attributable Risk Factors of LBW
Figure 5 shows the proportion of causes of DALYs related to LBW among children under five in Indonesia in 2021. The majority of DALYs related to LBW are caused by neonatal disorders, contributing 94.27% to the total burden. Other diseases contributing to the LBW-related burden include respiratory infections and Tuberculosis (TB) at 3.60%, enteric infections at 1.54%, and other infectious diseases at 0.59%.
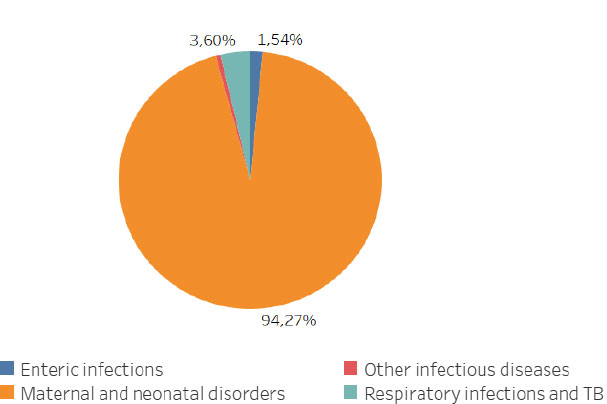
Specific causes of DALYs related to low birth weight (LBW) among children under five in Indonesia in 2021.
Figure 6 presents the attributable risk factors illustrating the potential loss of healthy life opportunities related To Low Birth Weight (LBW) among children under five in Indonesia in 2021. Nationally, 69.68% of neonatal disorders are attributable to LBW. Nearly 3 million years of healthy life were lost due to neonatal disorders attributable to LBW. Additionally, LBW also contributes to respiratory infections and digestive tract infections, with contributions of 10.63% and 4.77%, respectively, leading to the loss of 105,774 and 45,383 years of healthy life (Fig. 6).
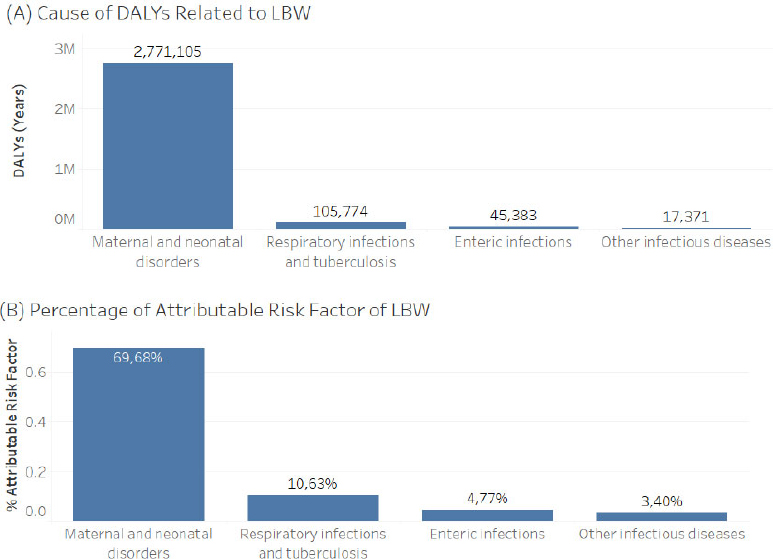
Attributable risk factor of LBW among children under five in Indonesia in 2021. (A) DALY in years. (B) percentage of attributable risk factors.
4. DISCUSSION
The burden of LBW in Indonesia is highest in the central and eastern provinces, which aligns with longstanding disparities in healthcare access, geographic constraints, and socioeconomic disadvantages in these regions [9]. High-quality maternal and neonatal services remain concentrated in major urban centers, while remote, rural, and island areas face limited facility availability and substantial transportation barriers [10]. These structural challenges are reflected in lower utilization of hospital and preventive services in eastern Indonesia, driven in part by lower educational attainment and higher poverty levels that reduce care seeking and access to essential maternal and child health services [11-13]. These findings highlight the need to expand the availability and quality of maternal and neonatal health services in underserved provinces as a policy priority.
Significant disparities in advanced neonatal care capacity contribute to the unequal burden of LBW across regions. Hospitals with NICU and PICU services are predominantly located in western Indonesia, leaving many central and eastern provinces with limited capacity to manage severe LBW complications [14]. This shortage forces families to travel long distances for care, causing treatment delays and increasing indirect costs. Although national health insurance reduces direct medical expenses, geographic and non-medical barriers remain substantial. Evidence from eastern Indonesia shows that, despite financial protection for primary care, utilization of higher-level maternal and neonatal services remains low due to structural constraints rather than medical costs [15]. These gaps in NICU/PICU availability likely contribute to higher LBW-related DALYs in eastern regions.
Regional disparities in neonatal care utilization further reinforce these patterns. Only 47.9% of infants nationwide received complete neonatal visits, ranging from 58.5% in Java–Bali to 23.8% in Papua [16]. Completeness of neonatal care is strongly influenced by delivery attendant, maternal education, place of delivery, parity, and ANC adequacy, with delivery attendant being the most influential factor [16]. These low follow-up care levels may contribute to the higher burden of LBW and neonatal disorders in eastern Indonesia.
DALYs related to LBW are much higher in the neonatal group (<28 days). Mortality risk among LBW infants is particularly elevated during the early neonatal period, as shown in Makassar, where mortality among LBW infants under 28 days reached 30.2% [17]. Meanwhile, a similar study in Ethiopia showed an infant mortality rate of 28.1% for LBW infants under 28 days of age (95% CI = 25.0-31.54) [18]. Beyond mortality, LBW contributes to long-term disability, including cognitive and behavioral impairments, ADHD, autism spectrum disorders, cerebral palsy, sensory impairments, and chronic lung disease [19]. LBW infants also have immature immune systems, increasing susceptibility to pneumonia and other respiratory infections that may lead to serious complications [3, 20].
Among the various causes of DALYs in LBW infants, neonatal disorders account for the largest share in Indonesia [6]. This is consistent with findings in India, where neonatal disorders account for the largest proportion of DALYs related to LBW [21]. As 69,68% of neonatal disorders are attributable to LBW, showing that nearly three-quarters of neonatal disorder cases in Indonesia are caused by LBW. Therefore, reducing LBW prevalence is essential for lowering neonatal morbidity and mortality, as neonatal disorders remain the primary driver of health loss among Indonesian children [6, 22, 23].
Addressing LBW in Indonesia could significantly reduce the disease burden from premature death and long-term disability, potentially saving nearly 3 million years of healthy life. Therefore, several intervention programs have already been implemented in Indonesia, such as Antenatal Care (ANC) services, provision of iron tablets, neonatal care services, and Universal Health Coverage (UHC). In ANC services, monitoring of growth and development, early detection of abnormalities or diseases, and maternal health services are conducted [24]. Numerous studies have shown that inadequate ANC is strongly associated with LBW incidence [4, 25-27]. Mothers with fewer than four ANC visits were 3.69 times more likely to deliver LBW infants than those with adequate ANC visits [28]. However, K4 coverage (four ANC visits) remains at 68.1%, still below the national target of 85% [9].
In addition to ANC, the iron supplement (TTD) for adolescent girls and pregnant women is also a preventive measure for LBW by preventing anemia in pregnant women. Anemia during pregnancy significantly increases LBW risk (OR = 3.42; 95% CI = 1.85–6.34) [29-33]. Pregnant women who did not consume TTD as recommended had a 1.25 times (95% CI = 1.08-1.46) higher risk of delivering LBW babies compared to those adhering to recommendations [32]. Postnatal care also plays a critical role: neonatal mortality was 4.4 times higher among infants without complete KN1 visits compared to those receiving appropriate care [34]. Despite these programs, coverage of ANC, TTD, and KN1 remains low in several central and eastern regions and has yet to meet 2021 national targets, although UHC enrollment reached 98.56% in 2024 [9, 35].
Low utilization of maternal and child health services is influenced not only by system-level barriers but also by individual and community-level factors. Poor knowledge, cultural beliefs, limited awareness, and inadequate family support contribute to low uptake of essential services [36-38]. To enhance all program coverage, multisector collaboration is essential, such as collaborating with schools to enhance program coverage by incorporating compliance TTD consumption as an additional evaluation criterion for students and collaborating with the Ministry of Social Affairs to make child and maternal health programs a prerequisite for social aid. In addition, community health initiatives such as empowering community leaders to educate the importance of ANC and motivating families to support child and maternal health are also necessary.
5. LIMITATIONS
This study provides an overview of the burden of disease of LBW among children under five in Indonesia. However, several limitations in this research should be considered to provide a more comprehensive understanding of the findings and their implications. First, the GBD database provides aggregate estimates only at the provincial level, which may mask important variations at district or city levels where child health challenges may differ. Second, the accuracy of GBD estimates depends on the availability and quality of underlying data sources, including surveys and vital registration systems, which vary across regions and may affect the precision of the burden estimates. Third, the GBD framework does not fully account for contextual factors such as program implementation, socioeconomic dynamics, and environmental changes that influence LBW trends, potentially limiting the interpretability of the findings. Finally, because this study focuses solely on Indonesia at the provincial level, future research may extend the analysis to smaller administrative units or conduct comparative studies across countries using additional data sources to address these limitations.
CONCLUSION
LBW is a risk factor for the highest burden of disease among children under five in Indonesia. The burden of disease related to LBW is higher in eastern Indonesia, related to unequal access to health services. The age group under 28 days has the highest burden of LBW, and boys have higher DALYs than girls. LBW contributes to a greater burden of disease in premature death than prolonged disability, and neonatal disorders are the main cause. Programs and policies have been formed and implemented by the Indonesian government, but the implementation has not met the targets that have been set, so it has not been able to solve the issue. Cross-sectoral collaboration must improve the program to address LBW. Developing and perfecting health programs with multisector collaboration should be prioritized to reduce the burden of LBW.
SIGNIFICANCE FOR PUBLIC HEALTH
This study highlights the significant public health impact of Low Birth Weight (LBW) in Indonesia, particularly its contribution to neonatal mortality and long-term health risks. Quantifying the burden of disease, it underscores the urgent need for targeted interventions to reduce LBW and improve child health outcomes. Strengthening maternal care, enhancing prenatal care, and strengthening healthcare infrastructure can lead to significant reductions in the burden of disease and loss of healthy life opportunities due to LBW. Moreover, the study underscores the importance of multisectoral collaboration in developing comprehensive policies and programs to tackle LBW effectively. Prioritizing these strategies can help mitigate LBW’s impact, ultimately improving survival rates and promoting healthier futures for children.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: I.R.F.E.: Responsible for the analysis and interpretation of the results; M.M., I.T., W.S., and B.S.W.: Drafted the manuscript; T.S.: Reviewed and edited the draft. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| ANC | = Antenatal Care |
| DALYs | = Disability-Adjusted Life Years |
| GBD | = Global Burden of Disease |
| IHME | = Institute for Health Metrics and Evaluation |
| KN1 | = First neonatal visit |
| LBW | = Low birth weight |
| SKI | = Indonesian Health Survey |
| TTD | = Iron Supplement |
| UI | = Uncertainty Intervals |
| YLDs | = Years Lived with Disability |
| YLLs | = Years of Life Lost |
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
The authors would like to extend their gratitude to all parties who have contributed to this research, including IHME as the owner of the data. The authors also gratefully acknowledge VSK for organizing the boot camp and providing valuable mentoring, which significantly contributed to improving manuscript writing.

