All published articles of this journal are available on ScienceDirect.

Assessment of Hygiene Behavior and Associated Factors Among School Children in Shey Bench, Southwest, Ethiopia. An Institutional Based-Cross Sectional Study
Abstract
Introduction:
In underdeveloped countries, such as Ethiopia, the impact of disease burden caused by inadequate, contaminated water and a lack of sanitation is a huge burden. Water and sanitation-related infections are still a high-risk habit among primary school-aged children. As a reason, the objective was to analyze hygiene behavior and associated factors among school children in Shey Bench, Southwest Ethiopia, during the 2018/19 school year.
Methods:
An institutional-based descriptive cross-sectional study was done in 2019 to collect data from 770 primary school students in grades 5th through 8th from January 1 to 30, 2019. Data were entered into Epi data 4.2 and then analyzed in SPSS V. 21.0. Multivariate logistic regression analysis was used to identify independent factors of hygienic behavior.
Results:
In this study area, 34.1 percent of school students have good hygiene behavior. Being female students (AOR=2.68), Urban residency (AOR=1.86), having poor hand-washing knowledge (AOR=0.148), lack of availability of hand-washing facility (AOR=0.541), separate toilet for male and female (AOR=2.11), no read and write father's educational status (AOR=0.314) and presence of clubs in the school (AOR=1.75) were all significantly associated with hygienic behavior
Conclusion:
In general, there is a poor hygiene. Urban residency, no read and write father's educational status, existence of sanitation club in schools, having separate toilets for boys and girls, having hand washing available in the facility, and having poor knowledge of hand washing were all substantially associated to hygienic behavior.
1. INRODUCTION
The impact of disease burden owing to inadequate, unclean water and lack of sanitation is a complex issue, as is unhygienic behavior [1]. Hygiene and sanitation in schools are critical to allow children to learn more about hygiene, which will provide immediate and long-term health advantages [2]. Diseases related to inadequate water facilities, sanitation, intestinal parasite infectors and hygiene are a large burden in developing countries [3, 4]. Every year, more than 10 million children worldwide die as a result of an unhygienic cause that impacts daily life, child health, and the well-being of their mothers. Children in low-income nations die from diarrheal infections at a rate of about 4,500 per day [5]. Schools and daycare centers have repeatedly been implicated to be involved in the spread of infectious diseases, both among the children themselves and among their families and communities [6, 7]. Numerous school communities have a high prevalence of infections caused by insufficient water supply, sanitation, and hygiene, as well as child malnutrition and other underlying health issues [8]. In poor countries, promoting sanitary behaviors has been identified as a public health intervention that has the potential to reduce diarrheal diseases, absenteeism, and respiratory infections [9]. Particularly, a school-based hygiene promotion intervention may have a positive impact on hygiene behavior in students' homes and families [10].
Hygiene behavior is a multifaceted phenomenon that can be explained as the result of an interaction of numerous factors. Children are at risk from contaminated water, a lack of adequate sanitation, disease vectors, lack of safe waste disposal, and degraded environments [11]. Personal hygiene is a major cause of childhood deaths, illnesses, and impairments, particularly in developing countries, due to acute respiratory diseases, diarrheal diseases, physical trauma, poisoning, insect-borne diseases, and pregnancy infections [12].
Ethiopia has made significant strides in increasing the adoption of improved hygiene and sanitation. The promotion of improved sanitation facilities and safe hygiene practices in schools is critical, and it should ideally go hand in hand with community/household initiatives [13].
Schools are the most essential places for children to learn and alter their behavior. Childhood is the ideal period for children to learn good behavior. Children's knowledge, attitudes, and beliefs are heavily influenced by what they are taught, whether at home or school. Therefore, the aim of this study was to assess hygienic behavior and associated factors among schoolchildren in the Shey Bench, South-West Ethiopia.
2. MATERIALS AND METHODS
2.1. Study Area and Period
The study was conducted at Shey-Bench from January 1 to 30, 2019. Shey Bench is located in southern Ethiopia, approximately 561 kilometers from Addis Ababa. According to the 2007 population and housing census, the total population of the Shey Bench was 652531, with 323348 males and 329183 females. The majority of the population lives in rural areas, with only 11.53% living in cities. In the area, there are 13 schools, which accommodate around 18,357 students in the 2018/19 academic year.
2.3. Source of Population and Population under Study
The source population comprised all children of primary school-going age in Shey Bench.
The study population consisted of grade five to eight pupils attending school in the district, as they are the most mature and senior in primary school to respond with the required information without any difficulties.
2.4. Inclusion Criteria and Exclusion Criteria
2.5. Sample Size Determination
To determine the sample size, a single population formula was used. n= (Za/2)2 p (1-P) / d2.
Za/2= 95% CI= 1.96. P=prevalence of knowledge of hand washing =0.65 [14], d2=margin of precision= 0.05, n= (1.96)2 *0.65(1-0.65) / (0.05)2= 349.58.
Using the assumption of design effect as 2, n=349.59*2 = 700 by considering 10% nonresponse rate, n= sample size=770.
2.6. Variables
The outcome, i.e., dependent variable was hygiene behavior, while predictors/independent variables were age, sex, knowledge of hygeine, membership, mother's educational status, father's educational status, parent's occupational status, household enabling facilities, water handling knowledge, and latrine utilization.
2.7. Operational Definitions
2.7.1. Hygiene Behavior
It provided a composite score for students who answered yes to at least 9 questions related to the practice of water handling, latrine utilization, and hand washing, and classified them as having positive hygiene behavior [2].
2.7.2. Water Handling
Students who answered usually or yes to at least 3 water handling practice questions were classified as having proper water handling practice [2].
2.7.3. Latrine Utilization
Students who answered in latrine/always to at least 2 questions requesting the practice/skill of latrine utilization were classified as having proper latrine usage [2].
2.7.4. Hand Washing
Students who answered yes/always to at least 4 questions requesting information about the practice/skill of hand-washing were classified as having good hand-washing behavior [2].
2.8. Data Quality Control
One week before the day of actual data collection, the questionnaires for data collection were pretested on 5% of the sample size in locations other than the study area. Following the pretest, the instrument was changed in accordance with the study's objectives. The quality of the data was controlled during data collection by the immediate supervisor of the data collectors and the collection technique, as well as by daily reviewing the obtained data. Any ambiguity in the items was immediately evaluated by the supervisors and addressed by the main investigators following the day of the data collection. The data were cleaned, entered into Epi-data, and cross-tabulated.
2.9. Sampling Procedure
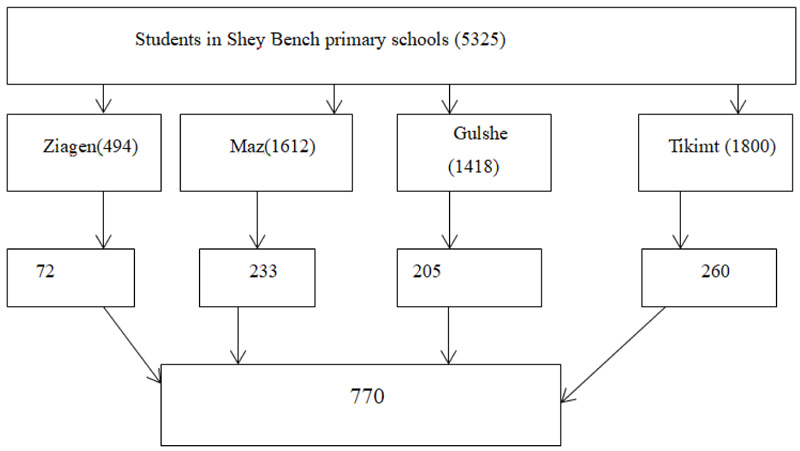
A multi-stage probability sampling procedure was used to select participating students. The study's target participants were students in the second cycle of each selected primary school in the specified woreda. A multistage simple random selection approach was utilized to choose students in the school. The district educational office picked four primary schools by lottery from 13 lists of primary schools with a second cycle, i.e., grades five to eight. Schoolchildren were chosen at random from the students' roaster list of selected schools depending on the proportion of grade five to eight students in each school. The goal of selecting students from grades five to eight was due to their maturity and seniority in elementary school (Fig. 1).
2.10. Data Collection Procedure
A structured questionnaire was used to collect data from the participants through face-to-face interviews and an observational checklist. The observational checklist was used to record variables, such as handwashing facility, presence and type of toilet in the school, anal cleaning materials on the floor, latrine smell, fecal materials on the floor or not, open defecation around the school, presence of hand-washing materials in the school, and the like. The questionnaire was initially drafted in English and translated to Amharic. A pre-test was given to 5% (60) of participants at Wacha primary school prior to the actual data collection time. The aim of the pre-test was to assess the suitability of the questionnaire with regards to duration, language appropriateness, content validity, and question comprehensibility.
Four teachers who were school coordinators in the setting were recruited to facilitate and guide the data collection process. For those data collectors, a day of training was given by the principal investigator on the overall questionnaires whenever they came across difficulties in completing the questionnaire. Students who answered “yes” to all knowledge questions were classified as having adequate knowledge of hygiene behaviour. The questionnaire included questions that determined whether the schoolchildren believe that hygiene behaviours (hand-washing, use and cleaning of the toilet, handling drinking water) can actually help in disease prevention. The observational study was used to collect data from the participants.
2.11. Data Processing and Analysis
The data gathered through face-to-face interviews and the observational checklist were analyzed together. The acquired data was cleaned, coded, and entered into the SPSS software before the actual analysis began. The Statistical Package for Social Sciences (SPSS) version 20 was used to enter and analyze the data, and a descriptive summary with frequencies, graphs, percentages, proportions, and cross tabs was utilized to present the results. The frequency and percentage of independent and dependent variables were calculated using descriptive statistical analysis. The VIF test value of the variables ranged from 2.13 to 9.87, and the entrance test value ranged from 0.10. The Hosmer-Lemeshow test was found to be non-significant, which had a p-value of 0.341 and an R-square value of 72.4%.
The degree of relationship between dependent and independent factors was determined using the odds ratio (OR) and confidence interval (CI). Bivariate analysis was used to examine the effects of numerous factors on the outcome variable. The statistical significance level was chosen at 0.2. Multivariate logistic regression was also performed to control the confounding impact, and factors with P-values less than 0.05 were considered statistically significant.
3. RESULTS
3.1. Socio-demographic Characteristics
A total of 739 schoolchildren participated in the study with a response rate of 96%. 396 (53.6%) of the participants were female, with an average age of 14.5 years (SD=2.5) in the study. According to the current year of study, 356 (48.2%), 293 (39.6%), and 90 (12.2%) of the participants were in grades six, seven, and eight, respectively.
3.2. Predisposing Factors
The majority of the participants, 642 (86.9%), demonstrated good hygiene knowledge, according to the comprehensive knowledge test. It was divided into three categories: handwashing, water handling, and latrine use, with 258 (34.9%), 377 (51%), and 446 (60.4%), respectively. The majority of participants (634, or 85.8%) knew how to safeguard drinking water and food against pest contamination, whereas the rest did not (Table 1).
3.3. Enabling Factors
606 (82%) of the total participants had a toilet at home, whereas the remaining individuals did not. According to study participants' toilet usage, 309 (51.0%), 159 (26.2%), and 138 (22.8%) had used the toilet always, usually, and sometimes, respectively. 685 people (92.7%) reported having access to a toilet at home and at school. The majority of respondents indicated there were separate toilet rooms for males and females at school. The most common types of latrines in schools were traditional toilets (309, or 64.0%), modified traditional latrines (168, or 34.9%), and VIP latrines (0.9%).
When it comes to access to drinking water, 487 (65.9%) of the study participants said they had it at any time (morning, mid-day, and afternoon). The majority of participants (648, or 87.7%) were aware that dirty water causes health concerns, while the remaining participants were not. Drinking water was handled in the following ways by survey participants: 153 (20.7%) used normal water; 315 (42.6%) boiling; 112 (15.25%) by adding chlorine; 131 (17.7%) by filtering with material; and 28 (3.8%) in other ways. The majority of participants, 488 (66.0%), collected water using a narrow-neck pot, while the remainder collected using a wide-neck pot. 355 (48.0%) adult females, 230 (31.1%) females aged 6-12 years, 119 (16.1%) adult males, and 35 (4.7%) males aged 6-12 years were responsible for collecting water from the source or pipe (Table 2).
| Characteristics | Frequency | Percent |
|---|---|---|
| Knowledge about latrine utilization Good Poor |
446 293 |
60.4 39.6 |
| Knowledge about water handling Good Poor |
377 362 |
51.0 49.0 |
| Knowledge about hand washing Good Poor |
481 258 |
65.1 34.9 |
| Do you take shower once in a week Yes no |
550 189 |
74.4 25.6 |
| Do you daily brush your teeth before bed and morning Yes No |
571 168 |
77.3 22.7 |
| Have you ever cut your finger once in a week Yes No |
585 154 |
79.2 20.8 |
| Do you daily wash your genitals after the toilet Yes No |
585 154 |
79.2 20.8 |
| Do you daily change washed clothes Yes No |
544 195 |
73.6 26.4 |
| Characteristics | Frequency | Percent |
|---|---|---|
| Accessibility of latrine Yes No |
585 154 |
79.2 20.8 |
| Separate facilities for boys and girls Yes No |
530 209 |
71.7 28.3 |
| Waste disposal site at school Yes No |
620 119 |
83.9 16.1 |
| Availability of drinking water at any time Yes No |
487 252 |
65.9 34.1 |
| Main source of drinking water Private pipe water Common pipe Groundwater From river |
392 264 70 13 |
53.0 35.7 9.5 1.8 |
| Availability of anal cleaning material Yes No |
411 328 |
55.6 44.4 |
| Faces outside the latrine structure Yes No |
495 244 |
67.0 33.0 |
| Open defecation happened around school Yes No |
438 301 |
59.3 40.7 |
| Availability of washing facility Yes No |
154 564 |
20.8 76.3 |
| Availability of hand washing materials (soap and ash) Yes No |
480 259 |
65.0 35.0 |
3.4. Motivational Factors
The participants used a school toilet for a variety of reasons. The toilets were reported to be separate for the boys and girls. Cleanliness, privacy, and security were listed as crucial factors to consider when using the toilet. In addition, 412 (55.8%) participants reported needing a driving force to use the toilet facilities, 106 (14.3%) reported self-initiated toilet usage, 75 (10.1%) reported peer pressure, and 12 (16.4%) reported teacher influence. handwashing has been emphasized to be associated witha driving force like terror, comfort, and nurture. When the individuals cleaned their hands, peer pressure, conformity, and the desire to avoid disease were all elements they considered. With respect to the location of the handwashing facility from the toilet, 452 (61.2%) and 287 (38.8%), respectively, reported it to be next to the latrine and within walking distance.
3.5. Hygienic Behavior of Participants
Regarding the hygienic behavior of the participants, out of the total participants, 487 (65.9%) had poor hygienic behavior and 252 (34.1%) had good hygienic behavior (Table 3).
| Characteristics | Hygienic Behavior Outcome | |
|---|---|---|
| Good | Poor | |
| Paternal educational status Unable to read and write Primary school Secondary school College and above |
126(56.3%) 188(65.7%) 103(83.6%) 70(71.4%) |
98(43.7%) 98(34.3%) 21(16.4%) 35 (28.6%) |
| Maternal educational status Cannot read and write Primary Secondary College and above |
112(39%) 105(35.9%) 21(20.2%) 14(25%) |
175(61%) 187(64.1%) 83(79.8%) 42(75%) |
| Family occupation Farmer Merchant Government employee |
133(37.6%) 77(50%) 42(20.7%) |
221(62.4%) 77(50%) 161(79.3%) |
| Presence of hygienic club in the school (Yes) No |
147(29.3%) 105(44.1%) |
354(70.7%) 133(55.9%) |
| Membership in hygiene club Yes No |
168(34.4%) 84(33.5%) |
320(65.6%) 167(66.5%) |
| Role model in school Yes No |
147(32.5%) 105(36.6%) |
305(67.5%) 182(63.4%) |
| Characteristics | HB | P | AOR | 95% CI | |
|---|---|---|---|---|---|
| good | poor | ||||
| Gender Male(reference) Female |
196(54.4%) 307(74.9%) |
164(45.6%) 103(25.1%) |
0.00 | 2.68 | 1.9 - 3.83* |
| Academic years Grade five -six Grade seven -eight |
249(68.6%) 254(62.4%) |
114(31.4%) 153(37.6%) |
0.852 | 1 1.056 |
0.596-1.872 |
| Residence Urban Rural (reference) |
296(73.4%) 207(56.4%) |
107(26.6%) 160(43.6%) |
0.00 | 2.657 | 1.863-3.790* |
| Maternal education: no read and write Primary school Secondary school College and above(reference) |
112(39%) 105(35.9%) 21(20.2%) 14(25%) |
175(61%) 187(64.1%) 83(79.8%) 42(75%) |
0.02 0.02 0.46 |
3.528 3.617 1.556 1 |
1.2- 10.78* 1.2- 11.06* 0.48- 5.03 |
| Paternal education: no read and write Primary school Secondary school College and above(reference) |
126(56.3%) 188(65.7%) 103(83.6%) 70(71.4%) |
98(43.7%) 98(34.3%) 21(16.4%) 35 (28.6%) |
0.400 0.177 0.396 |
0.314 1.501 0.787 |
0.159-1. 619 0.833-2.705 0.04-0.19 |
| Sanitation club in the school: Yes No (reference) |
147(29.3%) 105(44.1%) |
354(70.7%) 133(55.9%) |
0.234 | 1 .319 1 |
0.213 -3.479 |
| Membership in hygiene club Yes No (reference) |
168(34.4%) 84(33.5%) |
320(65.6%) 167(66.5%) |
0.489 | 1.154 1 |
0.769- 1730 |
| Separate toilet for male and female Yes No (reference) |
339(62.7%) 149(72.0%) |
202(37.3%) 58(28.0%) |
0.00 | 2.107 1 |
1.412-3.145* |
| Availability of hand washing facility No Yes (reference) |
87(53.4%) 401(68.5%) |
76(46.6%) 184(31.5%) |
0.02 | 0.541 | 0.33 -0.89* |
| Knowledge about hand washing Good Poor |
317(70.3%) 52(20.35) |
134(29.7%) 206(79.8%) |
0.00 | 1 0.148 |
0.08-0.274* |
3.6. Determinants of Hygienic Behavior
Gender of students, fathers' educational status, maternal education status, the academic year of students, membership in a club, presence of a hygiene club in the school, the residence of students, presence of a separate toilet in the school, availability of handwashing facility, and having good knowledge of handwashing, were all variables with a p-value less than 0.2 in bivariate analysis. Multivariate analysis was a possibility for these variables. Thus, using multivariate analysis, variables, such as students’ gender, fathers' educational status, maternal education status, academic year, presence of hygiene club in school, the residence of students, presence of a separated toilet in school, and having good knowledge of handwashing were found to be significantly associated with hygiene behavior (Table 4).
4. DISCUSSION
The sanitary behavior of school-aged children is influenced by a range of sophisticated and interconnected components that are difficult to detect. To acquire a better understanding of the factors that influence cleanliness practices, researchers in this study related important hygiene behaviors to school-based outcome variables [13].
Knowledge is one of the factors considered in the causal pathway to conduct [1, 10]. This study evaluated hand washing (65.1%), water handling (51%), and toilet usage (60.4%) practices of second-cycle school children. According to research conducted in Tigray's Mereb region, 71.1%, 68.8%, and 53.2% of the same target population, respectively, knew how to wash their hands, handle water, and use the toilet [15]. The findings of this study, however, were lower than one conducted in Bangalore, where the percentage was 88.3% in 2017 [16]. This discrepancy could be attributable to the characteristics of the study participants, the physical facility, or the study's scope (Table 4).
Students' knowledge was measured in this study, and those with good knowledge had a larger proportion of positive hygienic behavior. In this study, having a good knowledge of hand-washing was favorably associated with hygienic behavior (P = 0.00). It is similar to a research conducted in Mereb, Tigray, in 2014. However, it contrasts with a KAP hand-washing study conducted on Hosanna town schoolchildren in 2018 [14]. This difference could be owing to the existence of WASH in adjacent Hosanna Town, as well as the nature of participants and hand washing facilities (Table 4).
According to the findings, the proportion of hygiene-enabling facilities was found to be significant in hygienic behavior. When it comes to enabling factors, having a separate toilet for male and female students is strongly linked to hygienic behavior. This is in line with the findings of a study conducted in Sub-Saharan Africa [17]. It is a fact that students may be encouraged to avoid feces because of the dirt and odor. Alternatively, teachers and parents may instruct students on how to build good hand washing, water handling, and toilet habits through daily activities (Table 4).
In this study, the motivational elements were evaluated based on factors that influence hygienic behavior. 53.6% of female students and 46.4% of male students reported using hygienic behavior at a key time. Female students were shown to be more likely to engage in hygienic activities than male students. The authors agree with the research conducted in Hong Kong in 2017 and Sharjah, the United Arab Emirates, which found that women are more likely than men to wash their hands [3, 17]. This could be a result of women traditionally being more involved than men in meal preparation, housekeeping, and laundry. According to a study conducted in Korea, females are more likely than males to adopt hygienic behavior [3, 18] (Table 4).
This finding demonstrated that belonging to a hygiene and sanitation club has a positive impact on sanitary behavior. However, a 2017 study in Addis Ababa, Ethiopia, found belonging to a hygiene and sanitation club to have a negative impact on the sanitary behavior [19]. This disparity could be due to a time difference, a private school's failure to develop a club in their school, or the breadth of studies (Table 4).
4.1. Strength and Limitation of the Study
One of the great things about this study is that, unlike some other studies, it has used both self-administered and observational data collection methodologies. Furthermore, this study's prospective specialty lies in the specific (sex-based, behavior-based, and skill-based) and general examination of school activities. However, there are certain limitations to this research. Due to resource constraints, the study was unable to discover enabling elements that may have contributed to the students' cleanliness behavior. Understanding the elements that drive hygiene behavior is a difficult task that requires a lot of time and money.
CONCLUSION
Overall, just 34.1% of the children in the chosen primary school engaged in hygienic conduct, according to the findings of this study. Urban residence, the presence of sanitation clubs in schools, having separate toilets for boys and girls, having handwashing facility and high awareness of handwashing, were all strongly associated with unhygienic behavior.
The authors recommend the education offices of Shey-bench Woreda and Bench-Sheko zone educational bureau to implement school sanitation clubs in order to empower the students to enjoy the clubs. Health improvement personnel should focus their efforts on the health risks of drinking water with dirty hands, not washing hands after eating and after defecation at critical times, and incorrect hand-washing procedures. Thestudents should be taught, by using an emerging curriculum on hygienic behavior, about the importance of hand-washing, latrine utilization, and water handling.Moreover, further studies that combine different methodological approaches should be conducted to quantify the influence of enabling factors on the hygiene behavior of students and to understand further motivation/supportive issues and hygienic enabling factors.
AUTHORS’ CONTRIBUTIONS
The study's concept and design, as well as the data analysis and paper writing were done by SS. MB and WA assisted with data analysis, manuscript drafting, and overall research paper advice, as well as data interpretation and manuscript preparation. The final version of the manuscript has been read and approved by all the authors.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Mizan-Tepi University Ethical Review Committee granted the ethical clearance with the reference number C/AC/R/D /01/849/2018.
HUMAN AND ANIMAL RIGHTS
There were no animals utilized in this study. All human research operations were carried out in line with the ethical requirements of the institutional and national committees in charge of human experimentation, as well as the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was obtained from the parents/guardians of under 18 years of parents. A consent letter was included with the questionnaire to guarantee that the participants' rights, privacy, and confidentiality were protected.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
Data will be made available upon the request by the corresponding author [M.B].
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to Mizan-Tepi University, College of Health Sciences, for the support to conduct the research paper. Secondly, they would like to express their deepest gratitude to their colleagues for their endless support and constructive comments throughout the research development. Finally, they acknowledge the Mizan-Tepi University librarian, internet center coordinator, and Bench-Sheko Zonal Educational Health Bureau for their support and assistance in getting important materials to develop this research paper.

